CH 6 Lower limbs pt 2
1/152
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
153 Terms
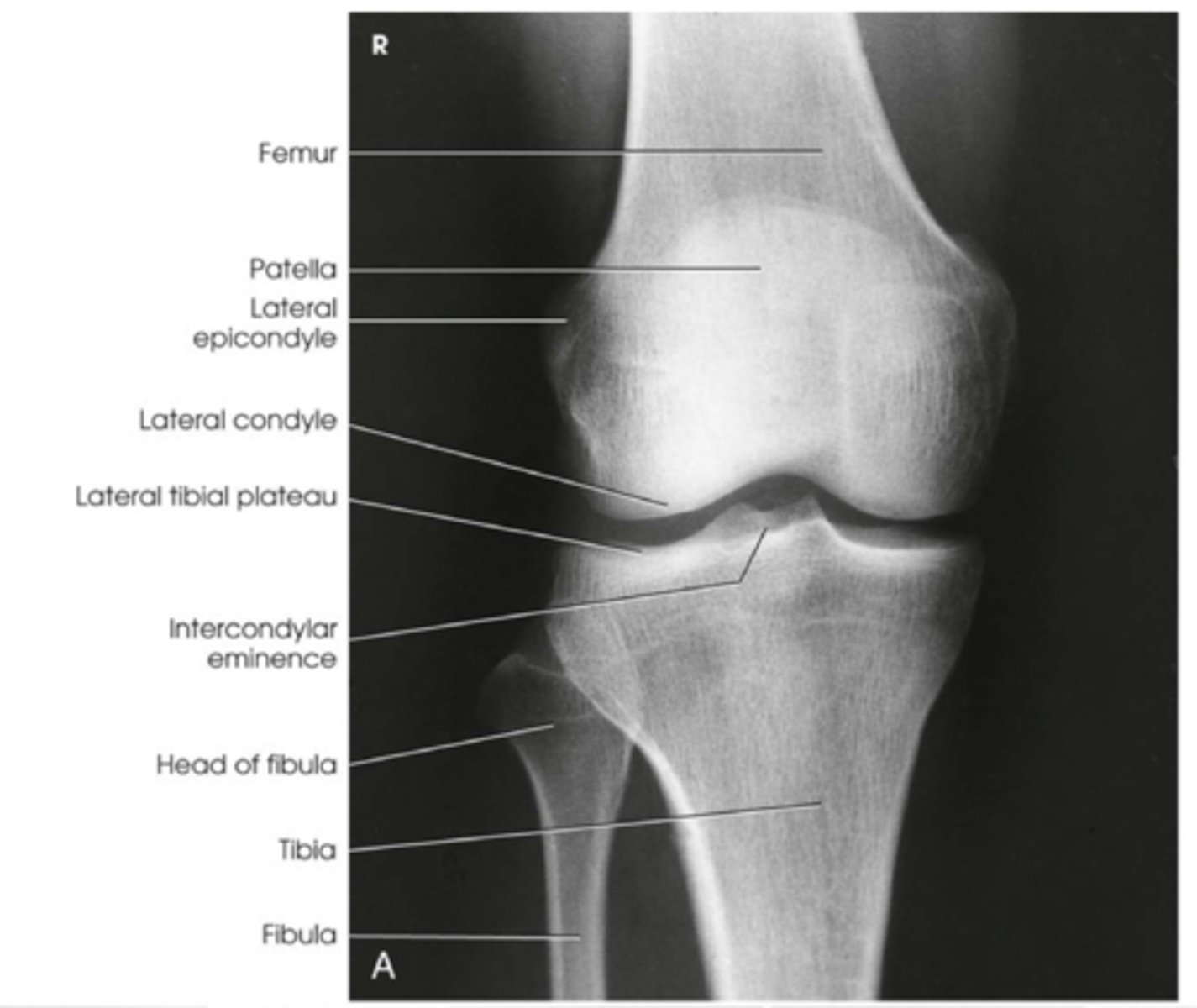
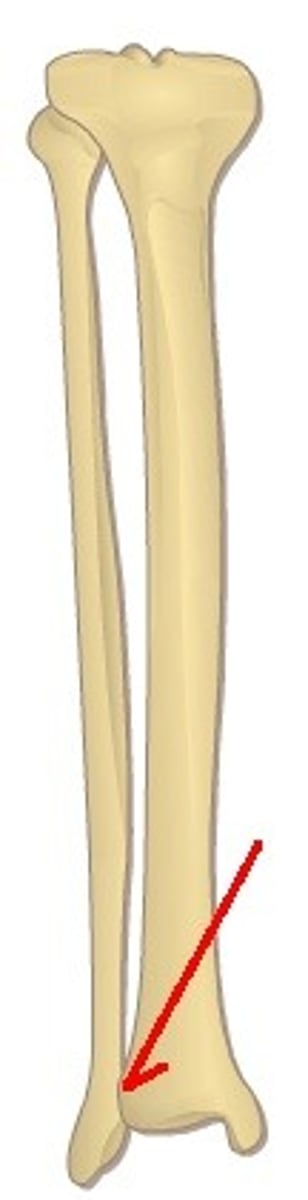
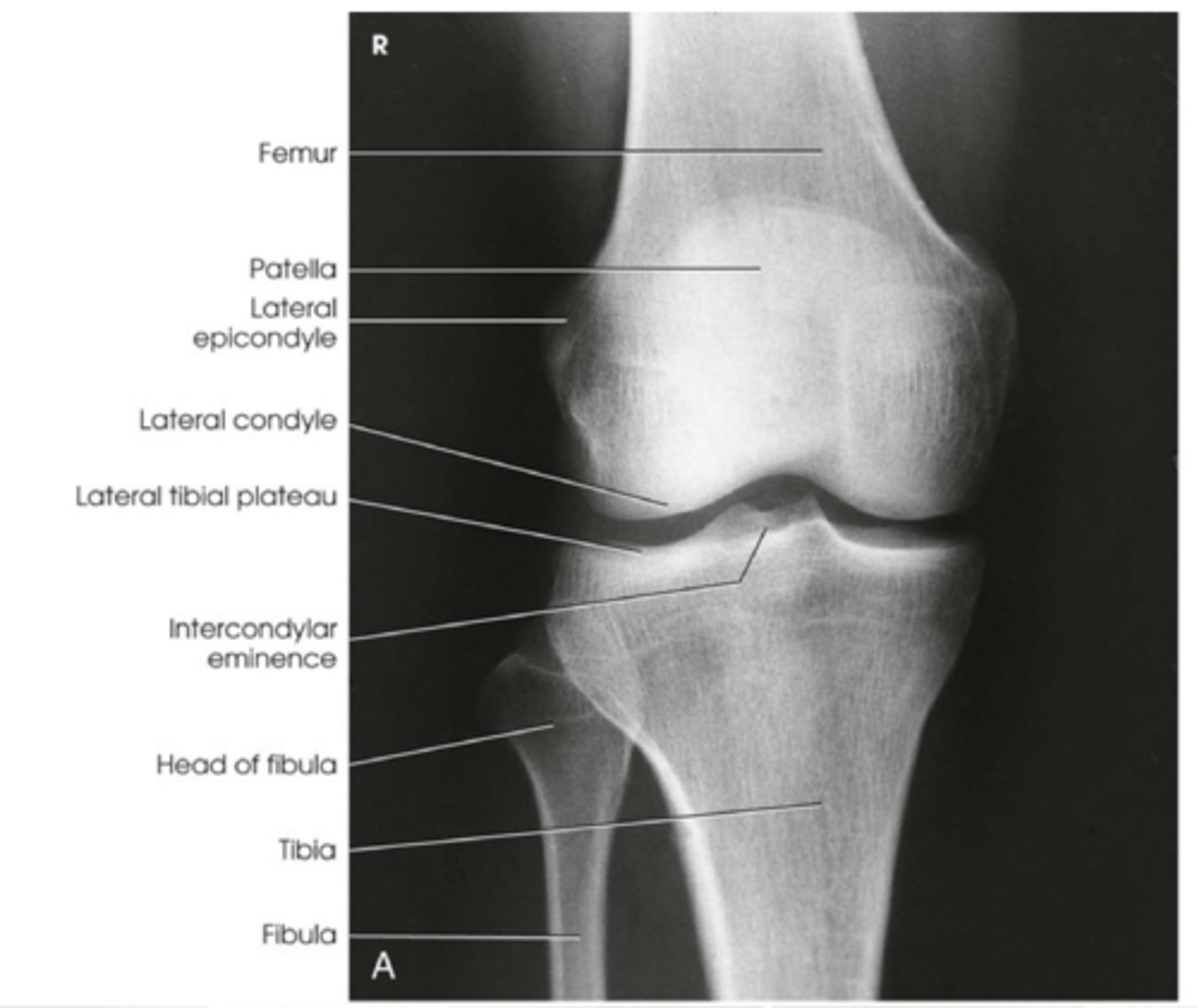
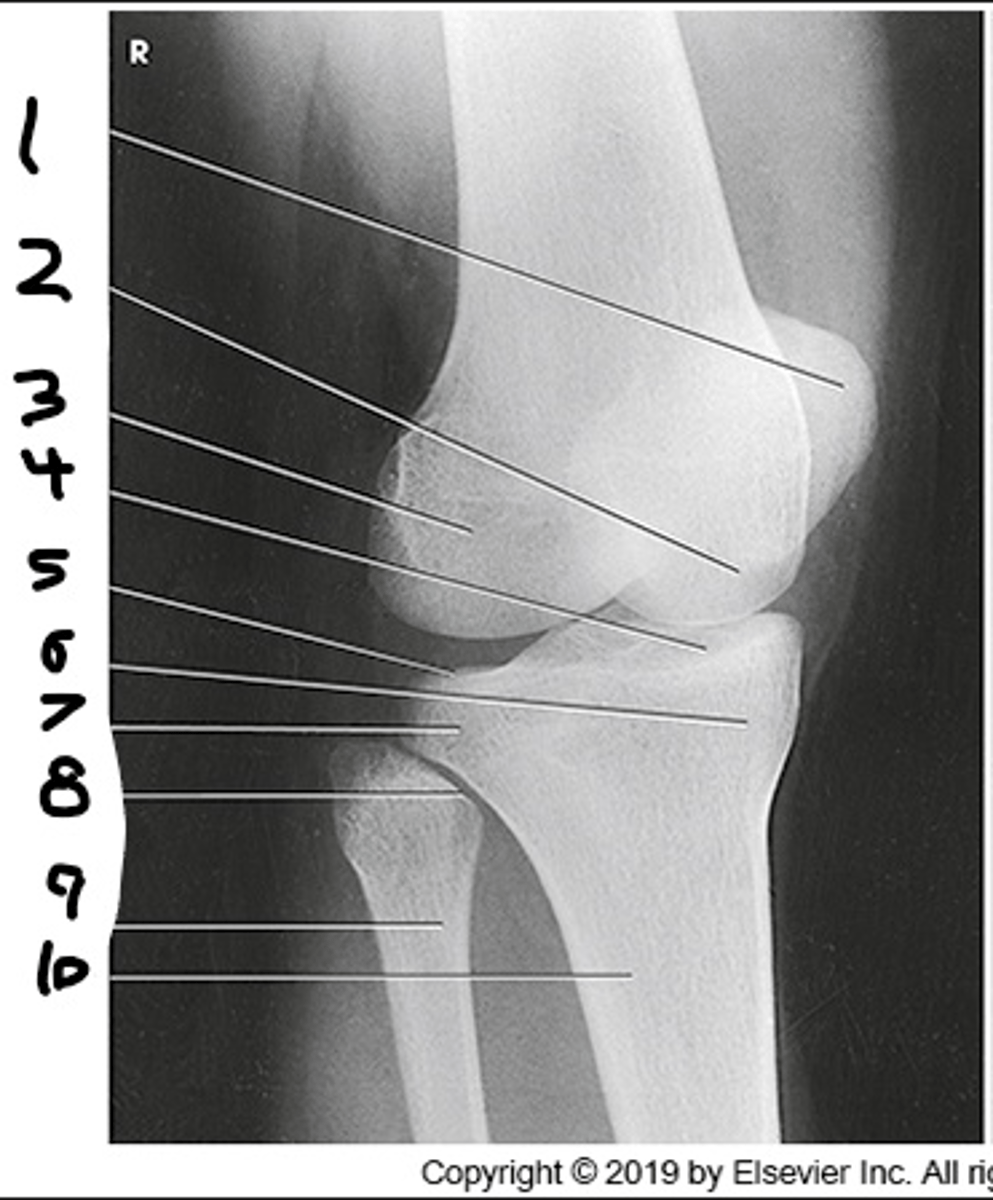
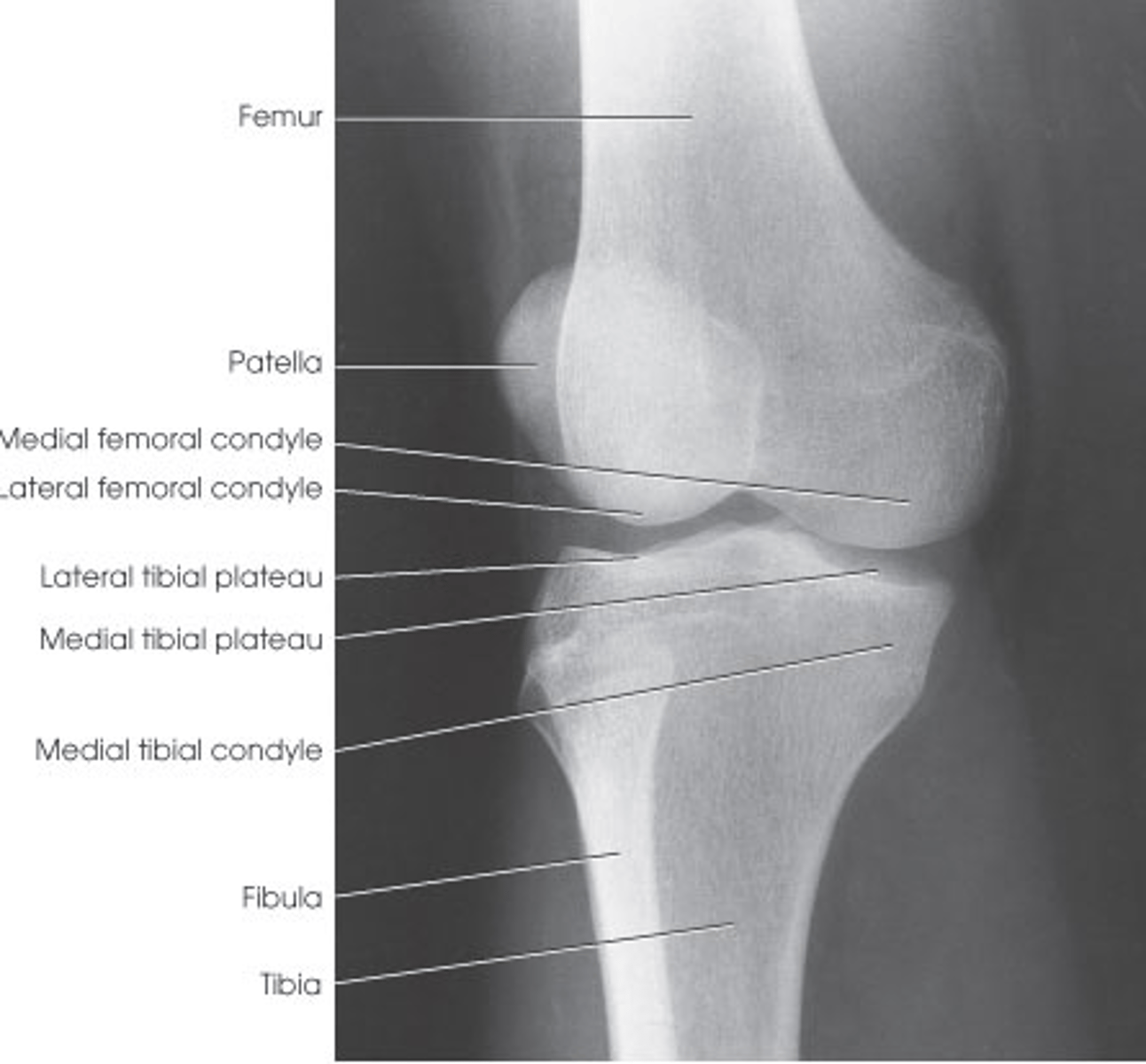
Tibia is made up of?
the body(shaft) and two extremities
What are the two large processes that make up the medial and lateral aspects of the proximal tibia
medial and lateral condyles
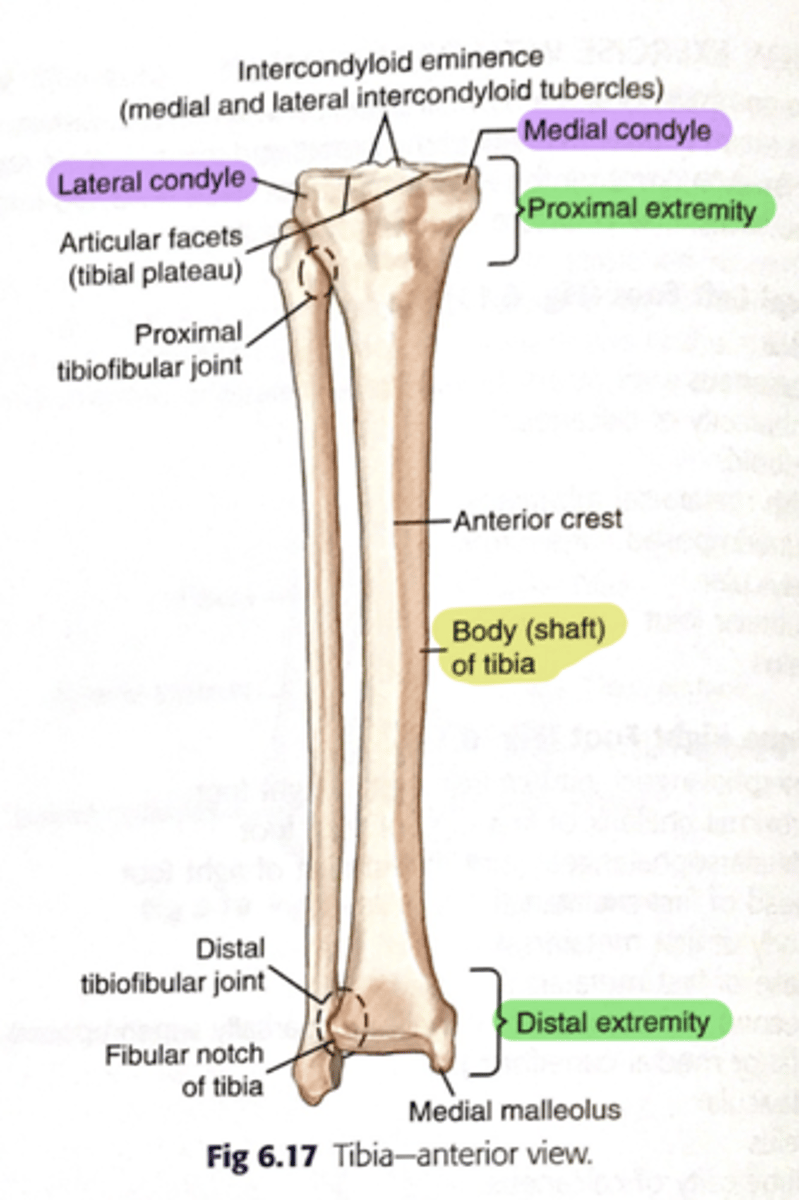
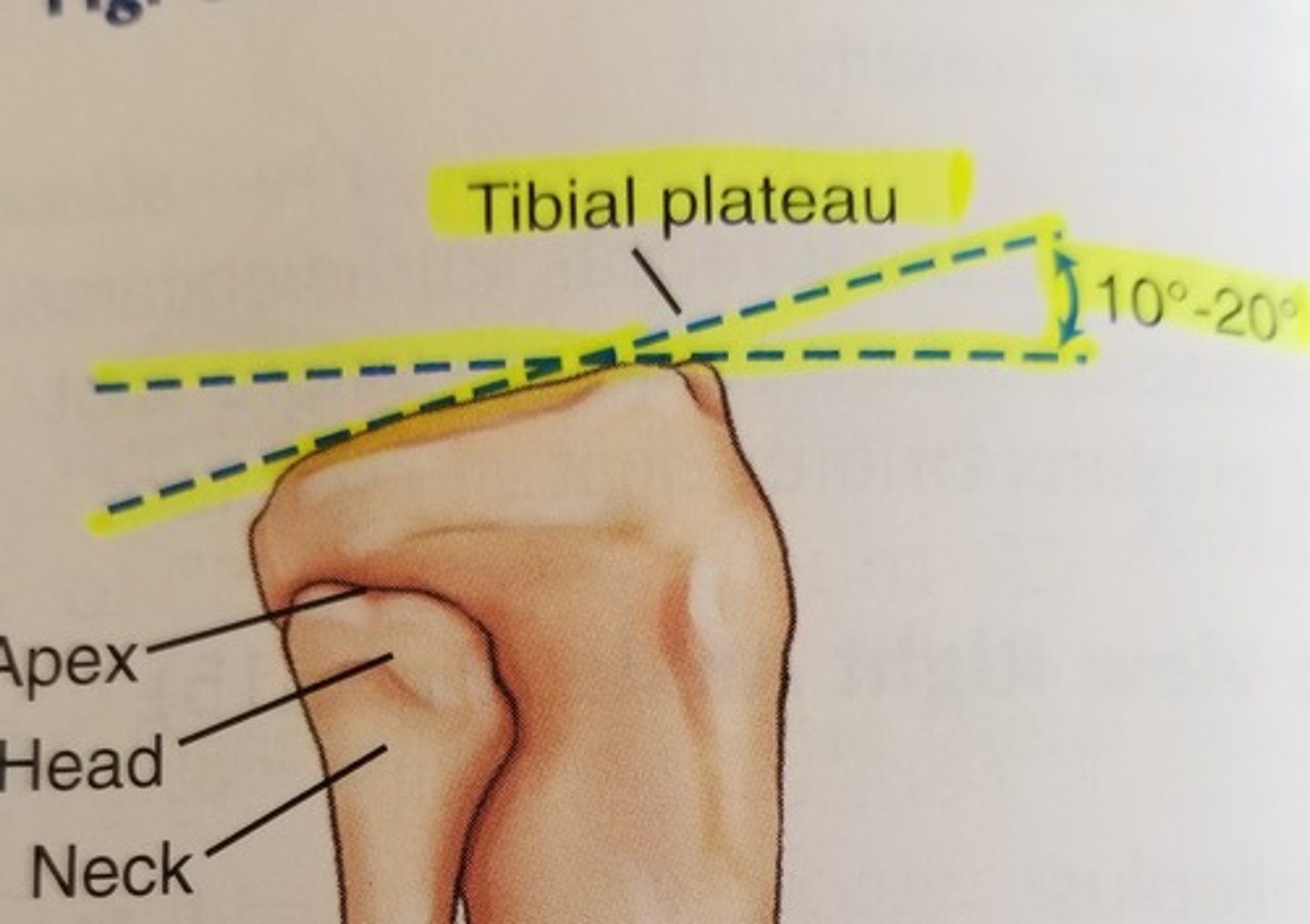
what is the name for the articular facets of the tibia?
tibial plateau
The tibial plateau slope _____________
posteriorly from 10 to 20 degrees
Why do we need to angle the CR for the AP Knee?
tabletop parallel to the tibial plateau and essential in demonstrating an open joint space depending on body size
tibial tuberosity separates from the body of tibia
this condition is called?
osgood-schlatter

anterior crest (border) is known as?
the shin or shin bone

The _________ is the weight-bearing bone of the lower leg
tibia
What is the name of the large prominence located on the midanterior surface of the proximal tibia that serves as a distal attachment for the patellar tendon?
tibial tuberosity

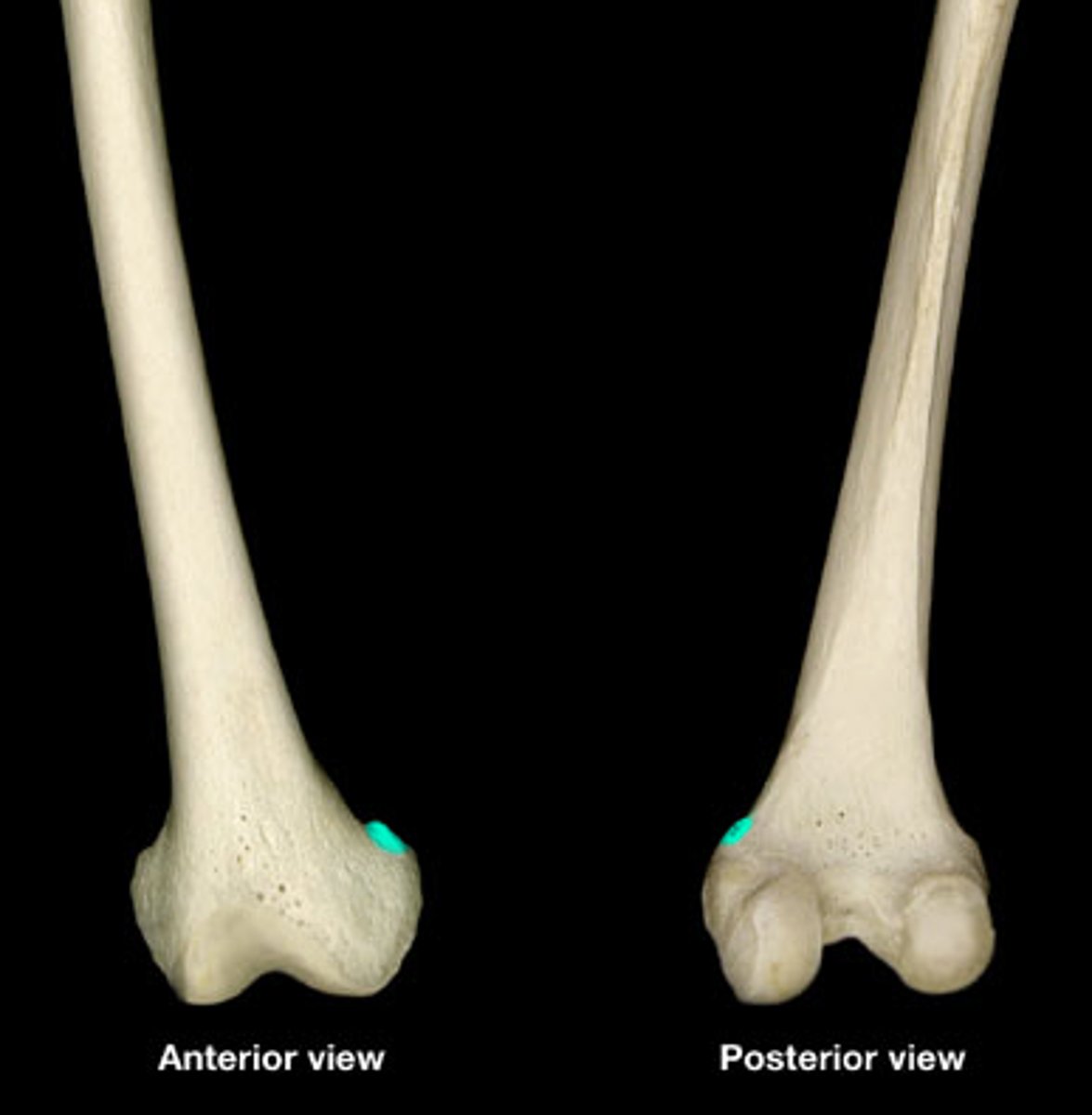
What is the name of the small prominence located on the posterolateral aspect of the medial condyle of the femur that is an identifying landmark to determine possible rotation of a lateral knee?
adductor tubercle
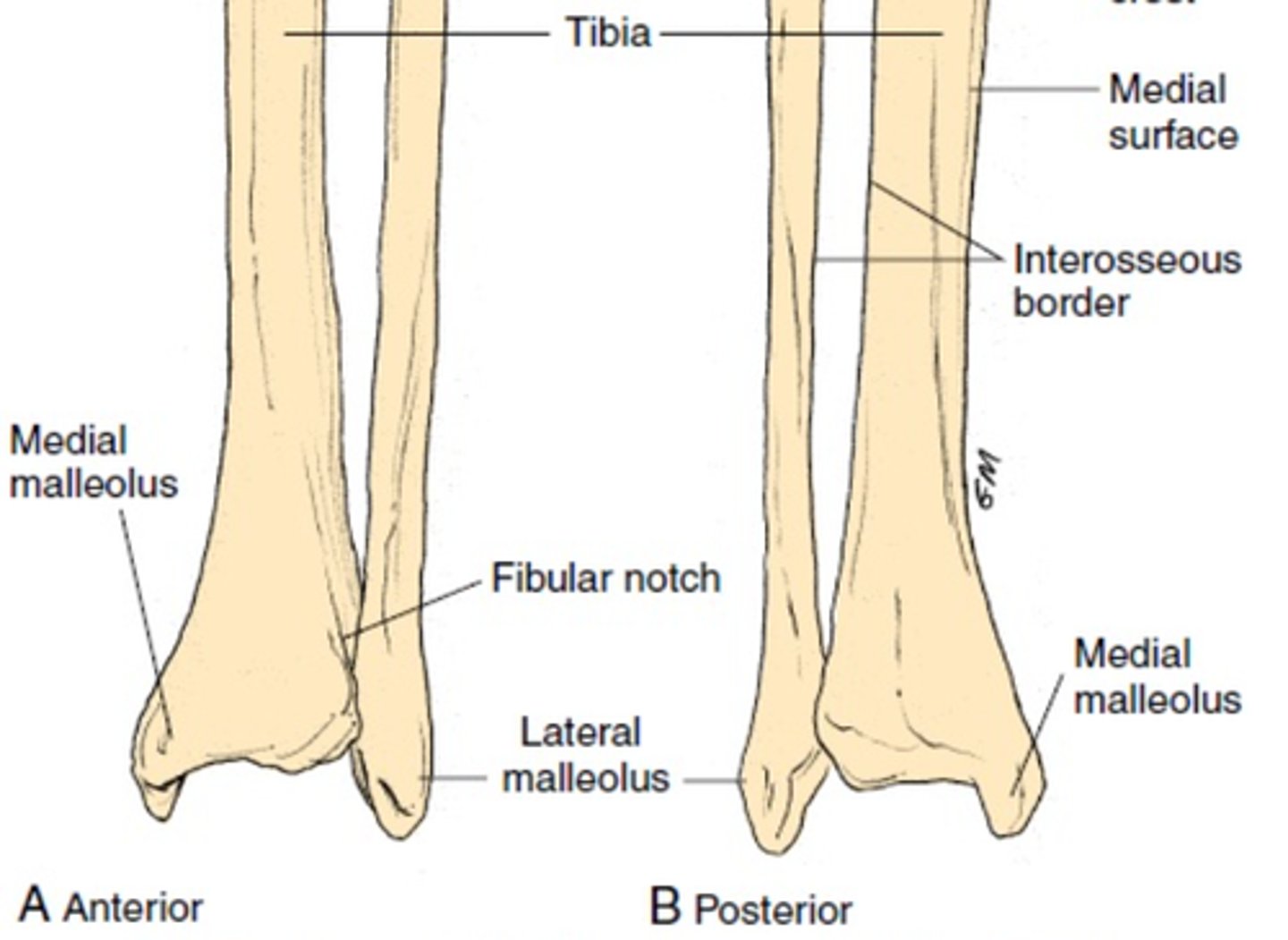
A small, triangular depression located on the tibia that helps form the distal tibiofibular joint is called
fibular notch
the articular facets of the proximal tibia are referred to as the ______
tibial plateau
The articular facets slope ________ degrees posteriorly in relation to the long axis of the tibia
10 to 20 degrees
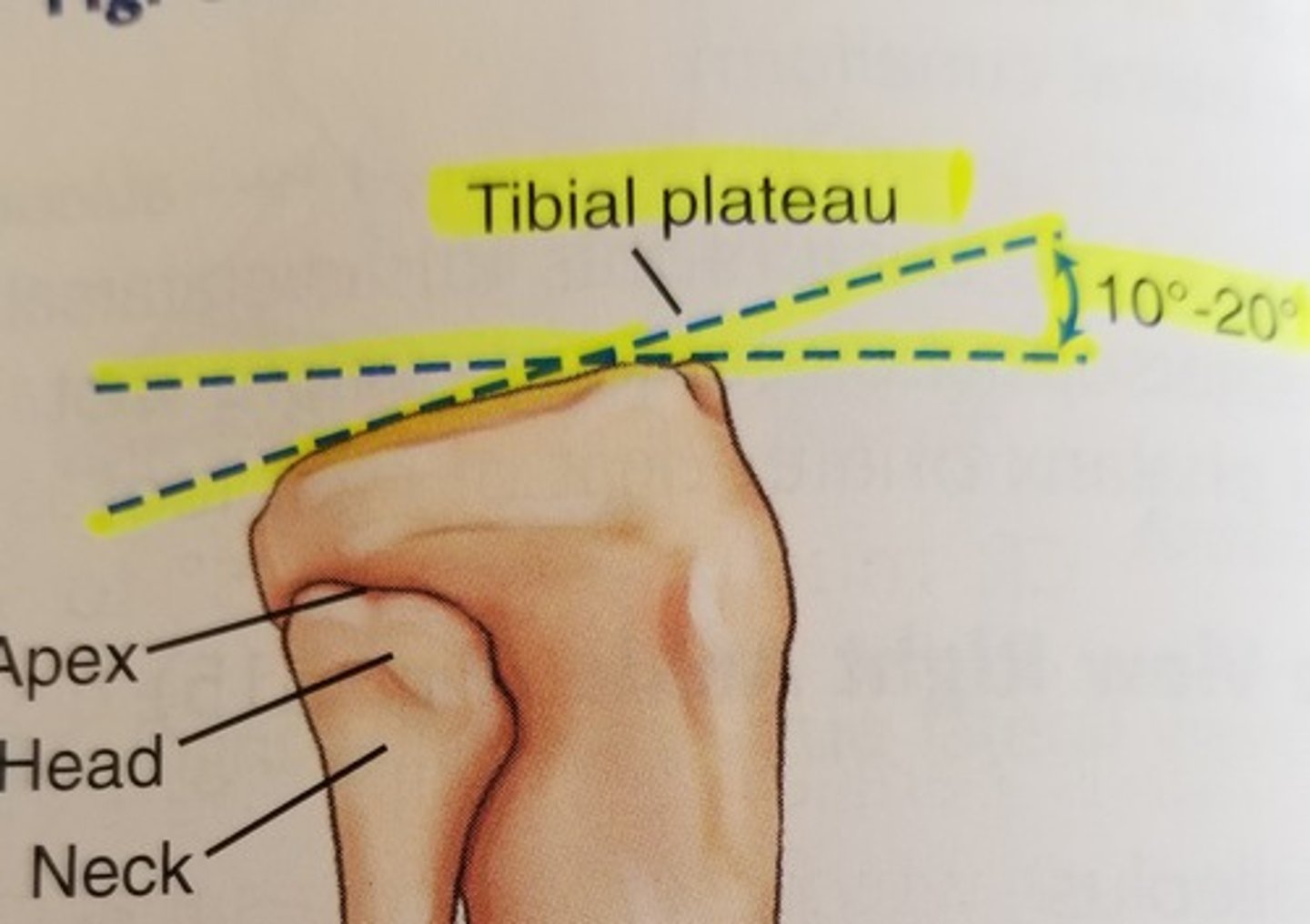
the most proximal aspect of the fibula is ________
apex or styloid process

the extreme distal end of the fibula is the _______
lateral malleolus

What is the name of the largest sesamoid bone in the body?
patella

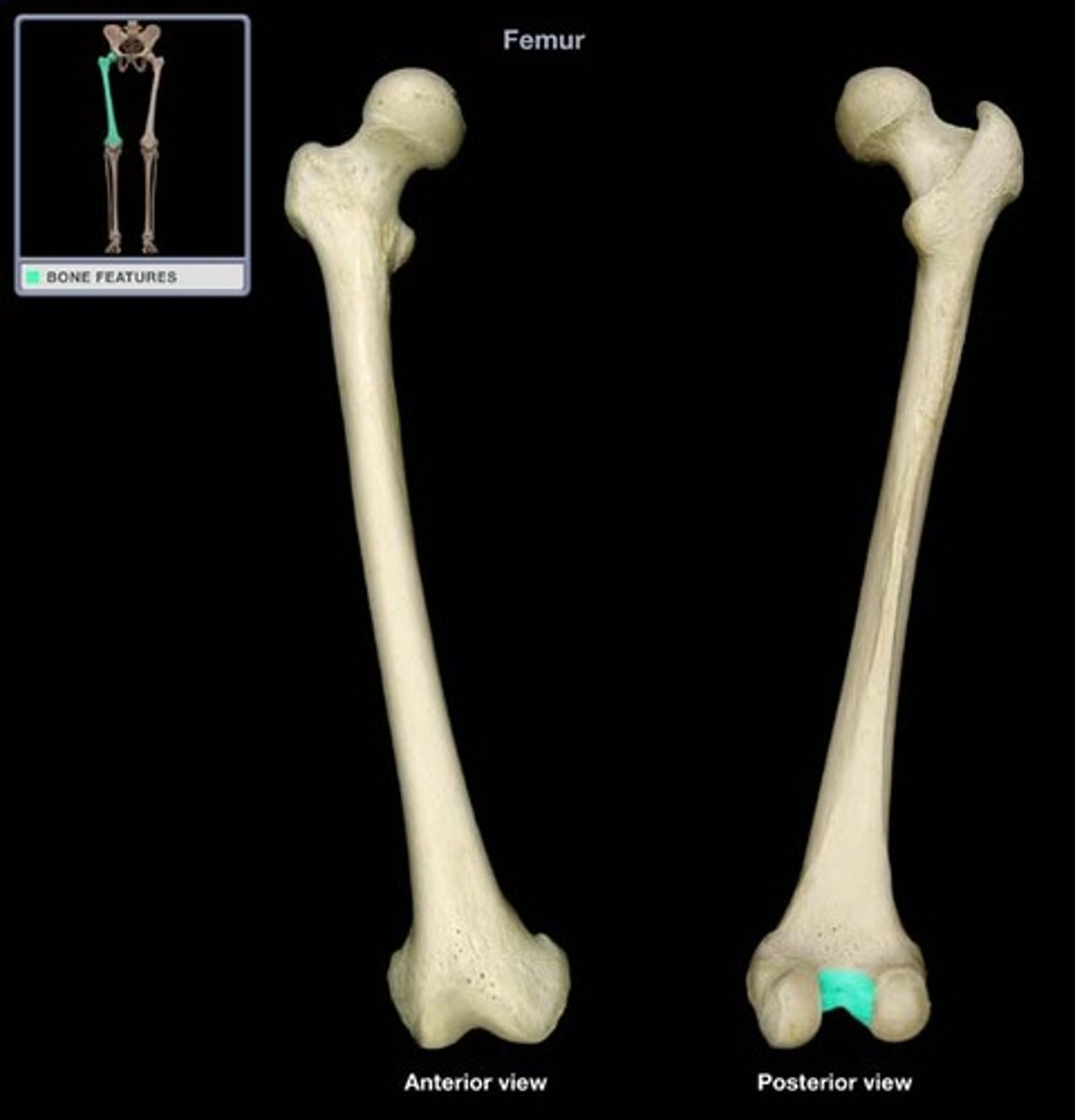
What are the two other names for the patellar surface of the femur?
intercondylar sulcus
trochlear groove
What is the name of the depression located on the posterior aspect of the distal femur?
intercondylar fossa or notch
Why must the CR be angled 5 to 7 degrees cephalad for a lateral knee position?
because the medial condyle extends lower or more distally than the lateral condyle of the femur
The slightly raised area located on the posterolateral aspect of the medial femoral condyle is called the________
adductor tubercle
What are the two palpable bony landmarks found on the distal femur?
medial epicondyle
lateral epicondyle
the general region of the posterior knee is called the _________
popliteal region
True/False
A 20 degree flexion of the knee is forces the patella firmly against the patellar surface of the femur.
false
True/False
The patella acts as a picot to increase the leverage of a large muscle found on the anterior thigh.
true
True/False
The posterior surface of the patella is normally rough.
false
For which large muscle does the patella serve as a pivot to increase the leverage?
quadriceps femoris muscle
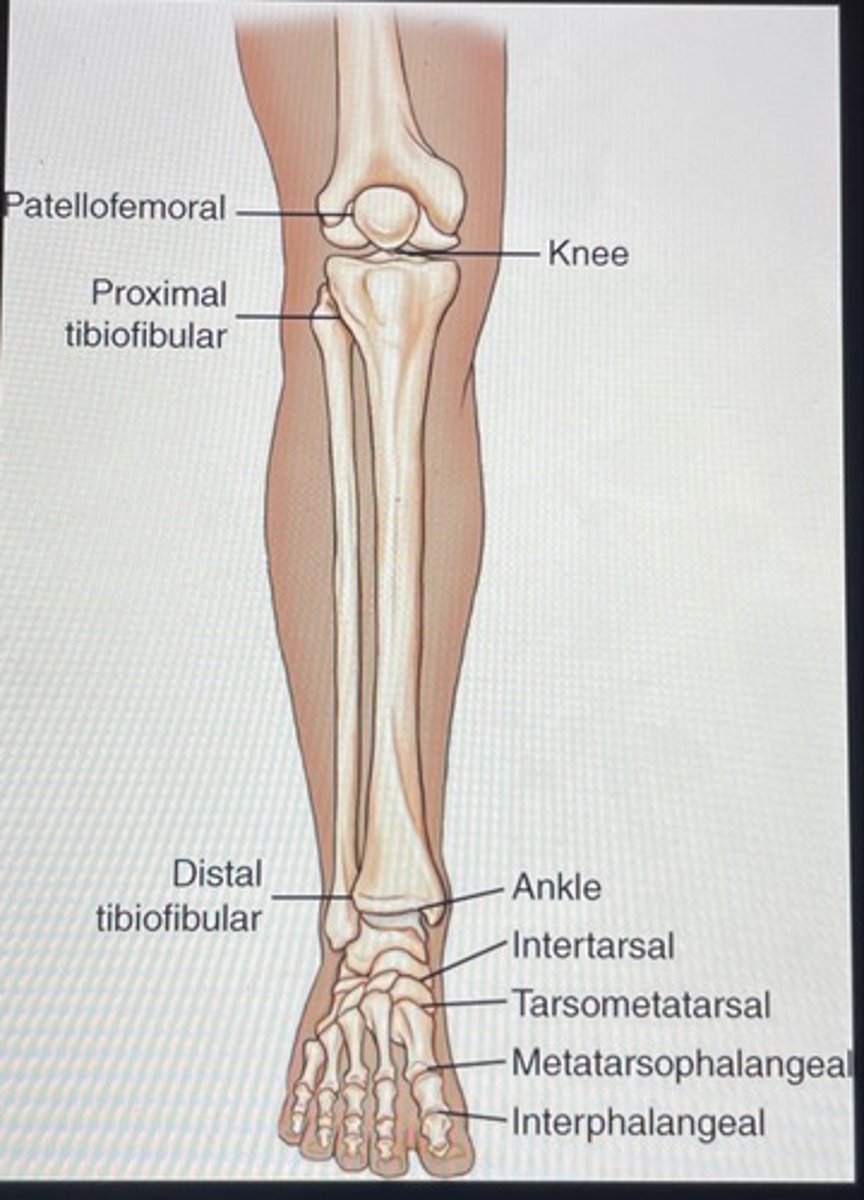
List the correct terms for the following joints:
A. Between the patella and distal femur
B. Between the two condyles of the femur and tibia
A. patellofemoral
B. femorotibial
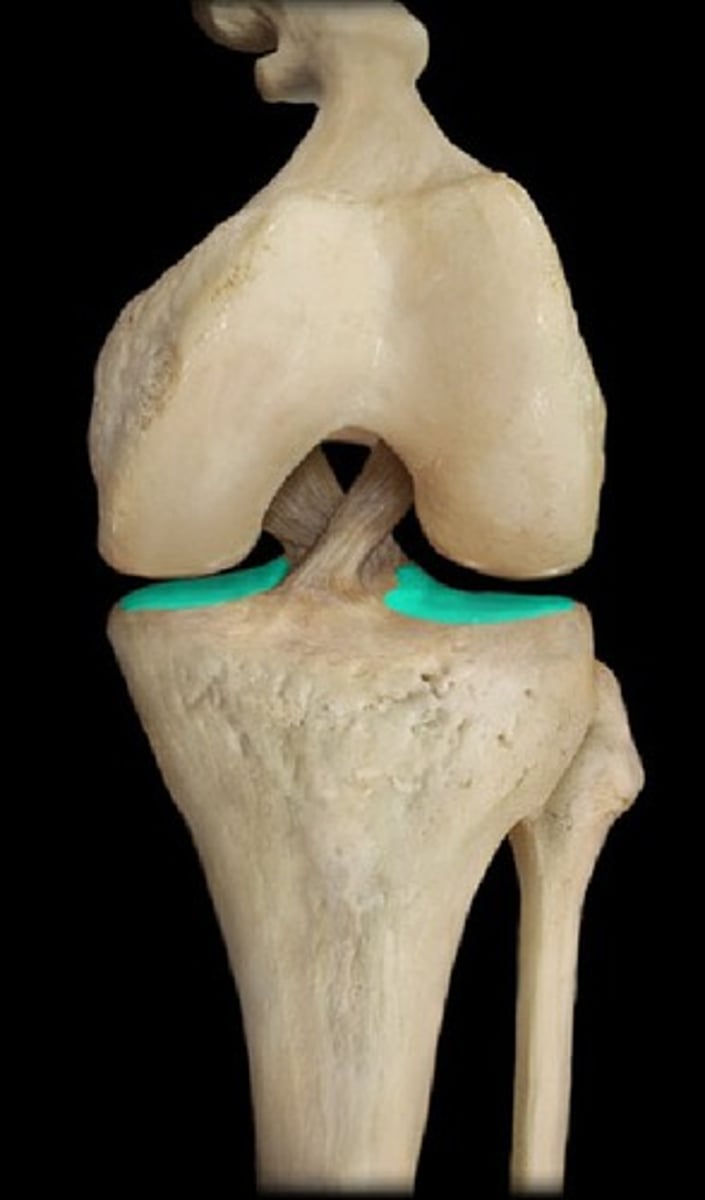
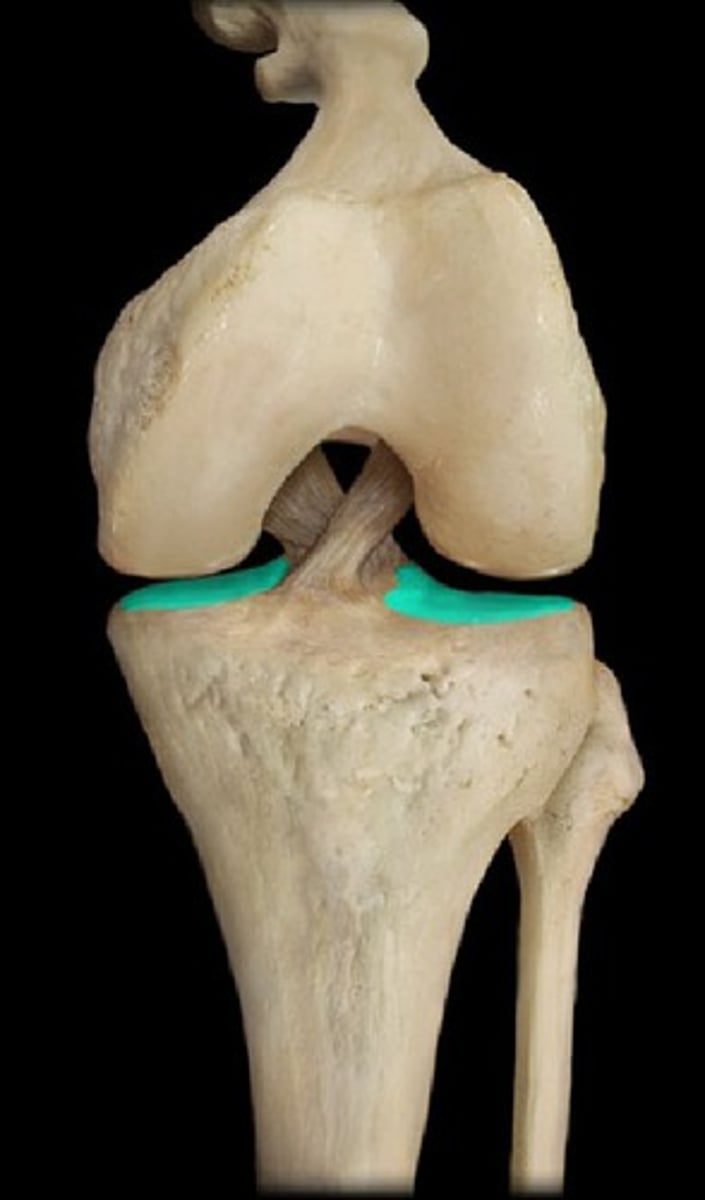
What are the four major ligaments of the knee?
Fibular (lateral) collateral
tibial (medial) collateral
anterior cruciate
posterior cruciate
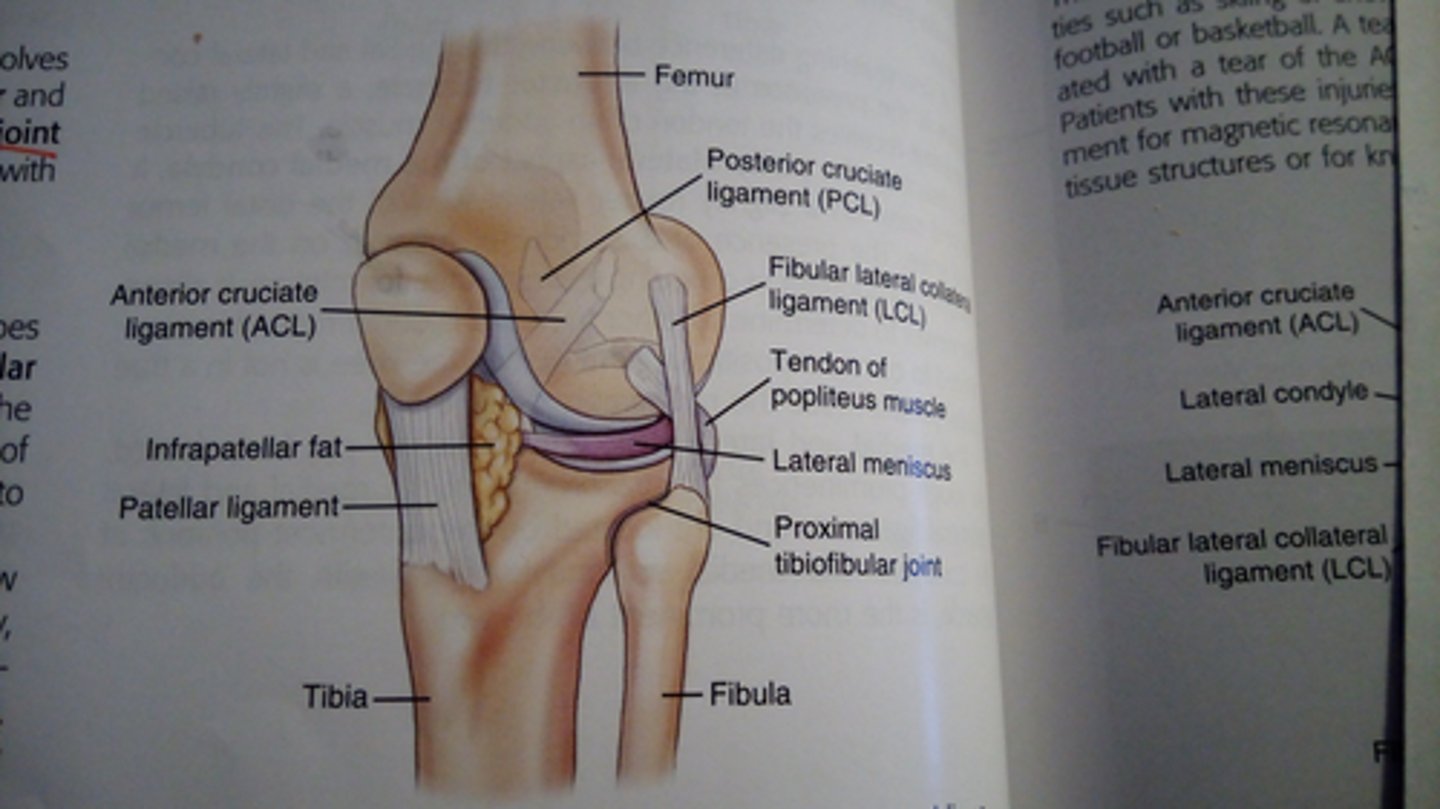
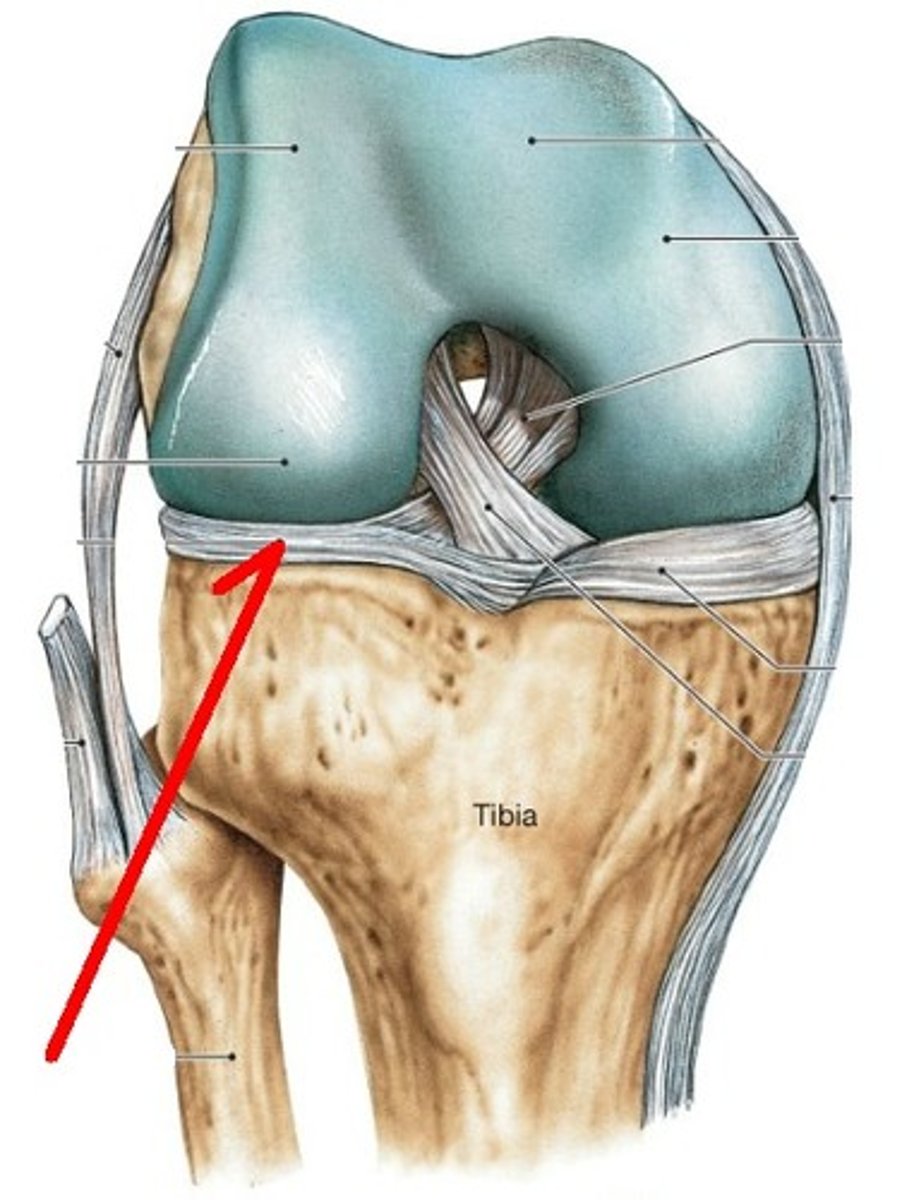
The crescent shaped fibrocartilage disks that act as shock absorbers in the knee joint are called__________
medial and lateral menisci
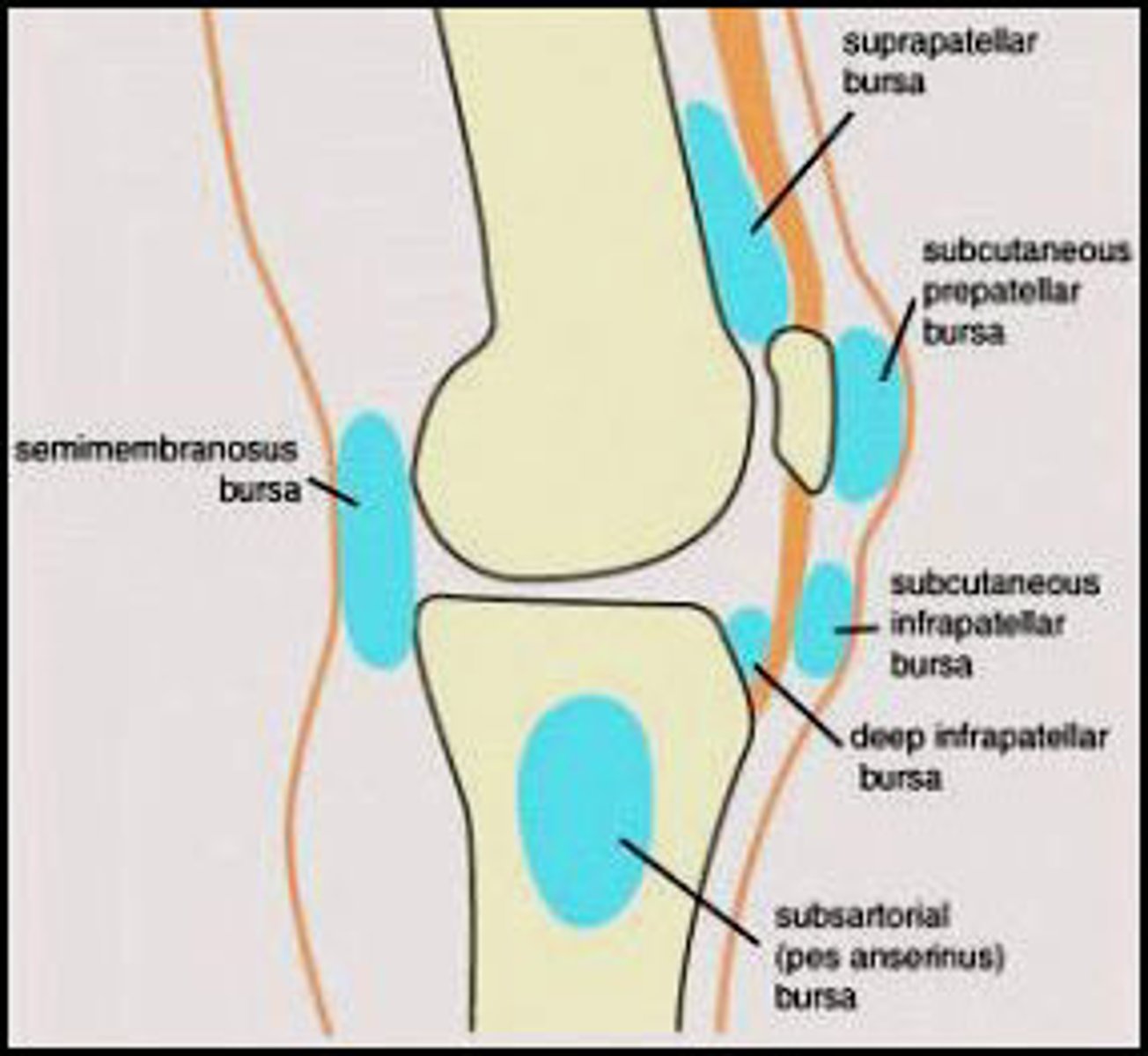
List the two bursae found in the knee joint
suprapatellar bursa
infrapatellar bursa
What is the joint classification for the ankle joint?
saddle (sellar)
dorsiflexion and plantar flexion only
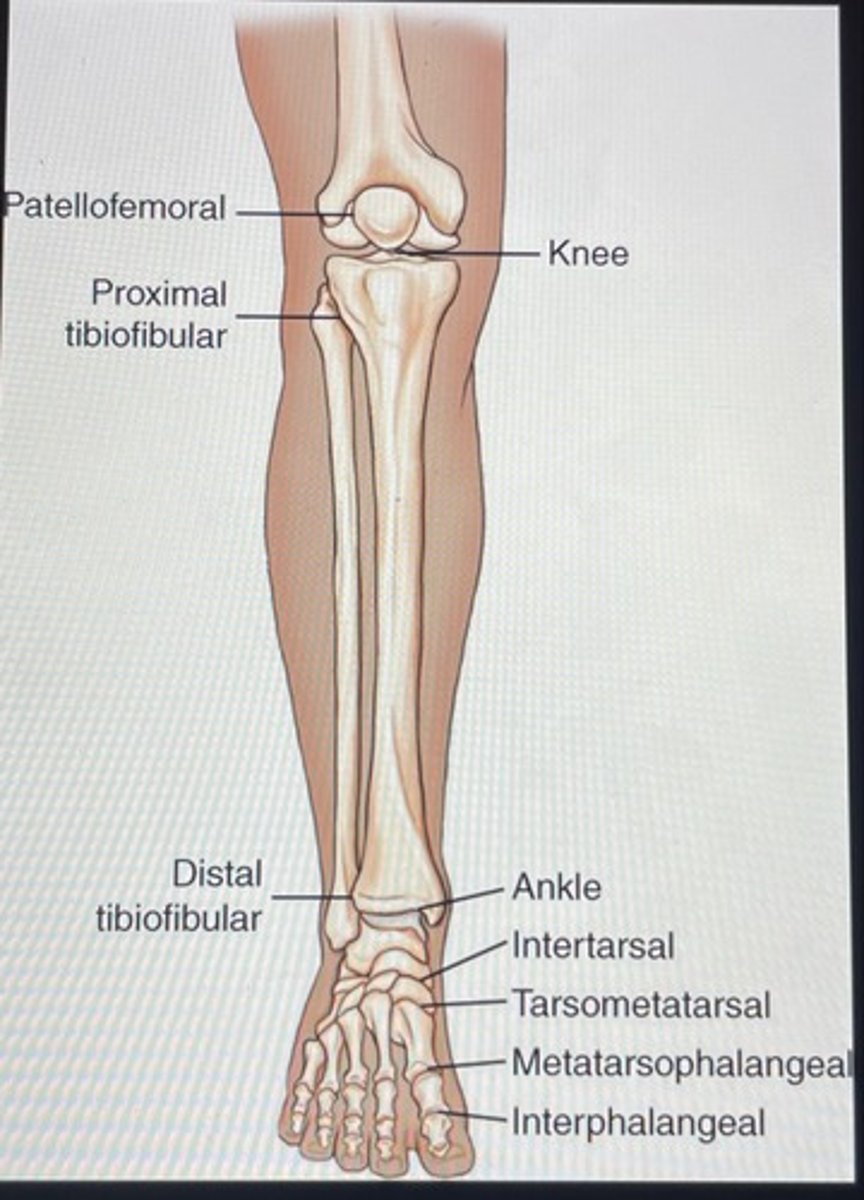
What is the joint classification for the patellofemoral?
saddle (sellar)
considered a saddle type because of its shape and relationship of patella to anterior, distal femur
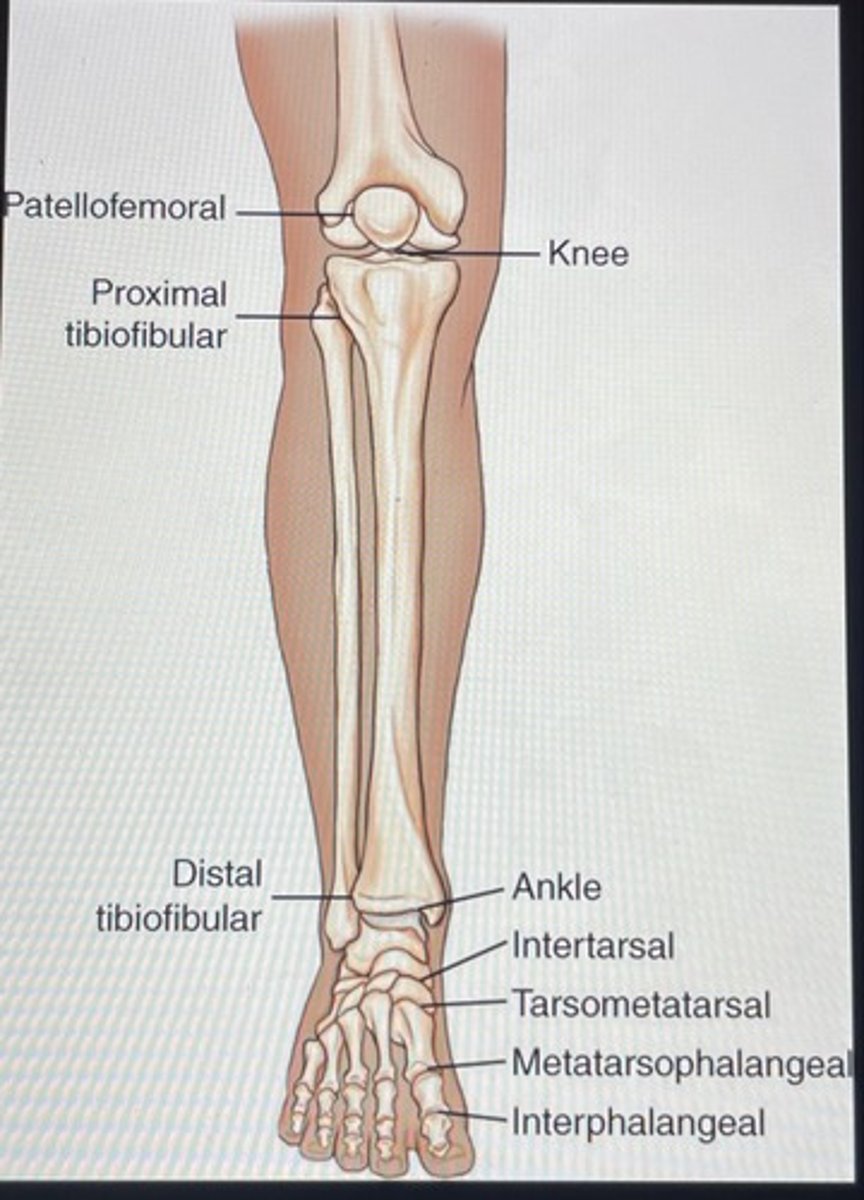
What is the joint classification for the proximal tibiofibular?
plane (gliding)
limited gliding movement between lateral condyle and head of fibula
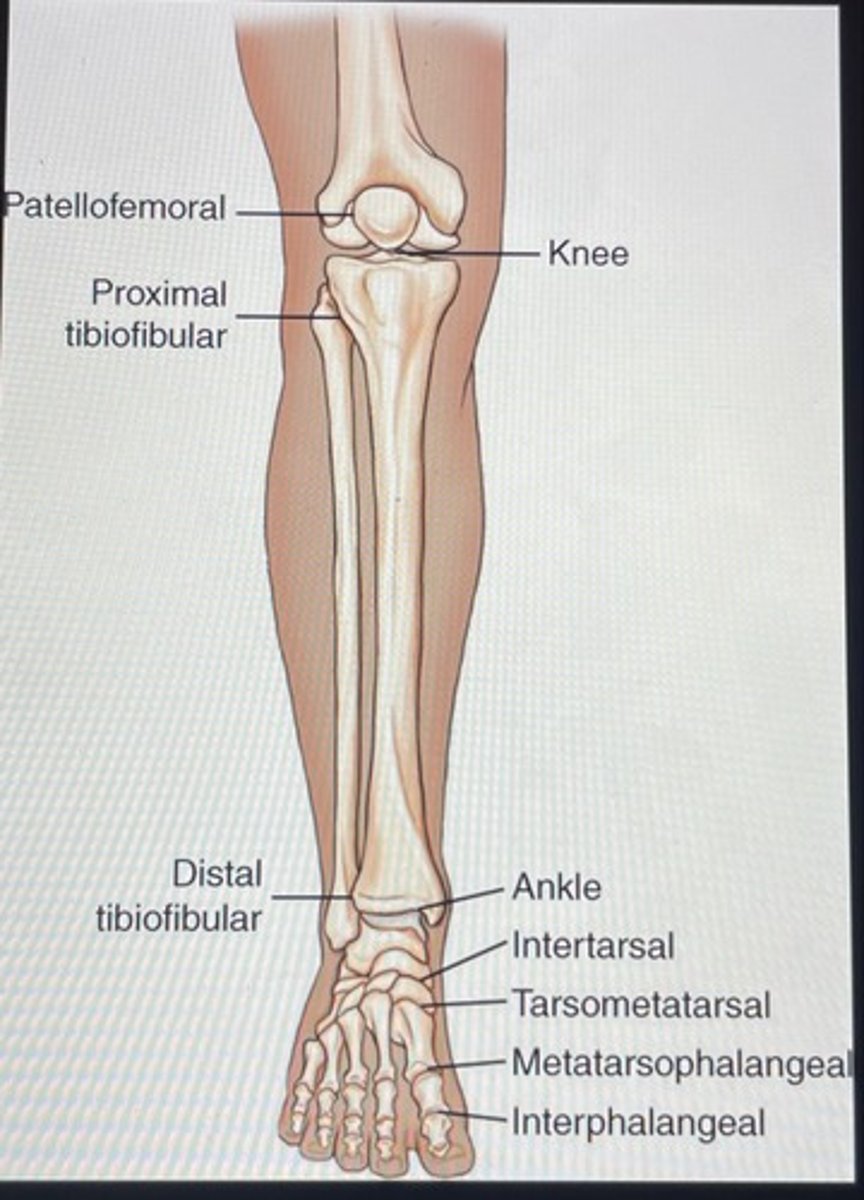
What is the joint classification for the tarsometatarsal?
plane (gliding)
What is the joint classification for the knee joint (femorotibial)?
bicondylar
flexion and extension and some gliding and rotational movements when knee is partially flexed
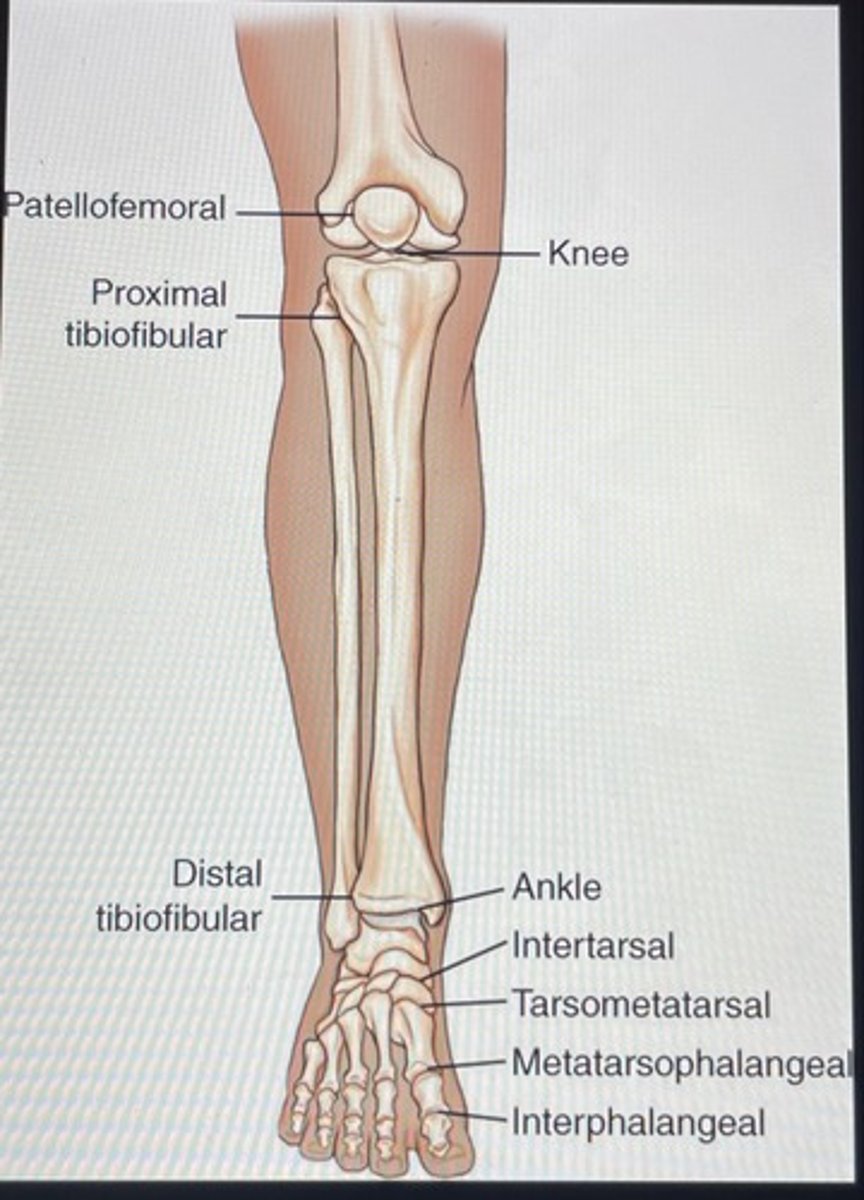
What is the joint classification for the distal tibiofibular?
amphiarthrodial (syndesmosis type)
slightly movable
What is the common term for chondromalacia patellae?
Runner's knee
Which imaginary plane should be placed parallel to the IR for an AP projection of the knee?
Interepicondylar line
Which joint space should be open or almost open for a well-positioned AP oblique knee projection with medial rotation?
Proximal tibiofibular joint
What is another term for the intercondyloid eminence?
Tibial spine
What is the name of the deep depression found on the posterior aspect of the distal femur?
Intercondylar fossa
A line drawn across the most distal aspect of the medial and lateral femoral condyles would be _________ degrees from being a right angle (90°) to the long axis of the femur.
5 - 7 degrees
The upper, or superior, portion of the patella is called the ______________.
Base (superior border)
Which two ligaments of the knee joint help stabilize the knee from the anterior and posterior perspective?
Anterior cruciate ligament (ACL) and Posterior cruciate ligament (PCL)
Helps stabilize the knee joint by preventing anterior and posterior movement within the knee joint.
Which structures serve as shock absorbers within the knee joint?
Medial and lateral menisci
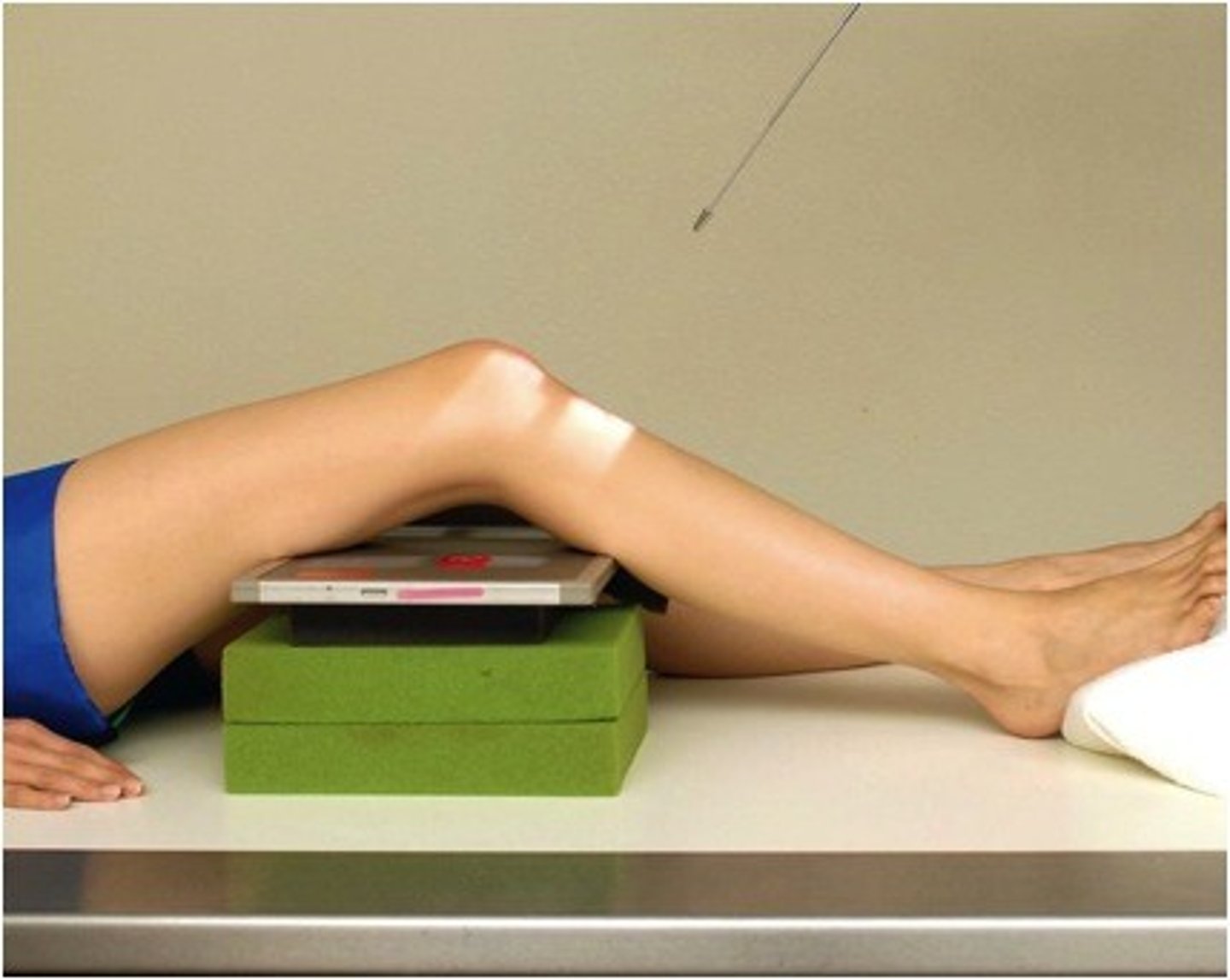
How much knee flexion is required for the horizontal beam lateral patella projection?
5-10 degrees
A radiograph of an AP knee shows that the joint spaces are not equally open and the proximal fibula is completely superimposed over the tibia.
Which specific positioning error leads to this radiographic outcome?
The specific positioning error leading to this radiographic outcome is the position of the knee. For an AP knee projection the leg must be rotated internally 3-5 degrees or until interepicondylar line is parallel to the IR. This will open up the joint spaces. Medial half of the fibular head should be superimposed by the tibia but not completely.
A radiograph of an AP knee projection demonstrates that the femorotibial joint space is not open at all. The patient is young and has no history of degenerative disease.
What type of positioning modification may improve the outcome of this projection?
Avoid angulation of the CR. Align CR parallel to the articular facets (tibial plateau) and directed ½ inch distal to the apex of patella.
A radiograph of an AP oblique with medial rotation of the knee to demonstrate the proximal fibula shows that there is total superimposition of the proximal tibia and the fibula.
What must be modified to correct this projection?
Align and center leg and knee to CR and to the midline of the table or IR. Leg must be rotated internally 45 degrees (interepicondylar line should be 45 degrees to plane of IR).
A radiograph of an AP and lateral tibia and fibula shows that the ankle joint is not included on the AP projection, but the knee and ankle are included on the lateral projection.
What should the technologist do in this situation?
In an AP projection of tibia and fibula both the ankle and knee joints must be included. The technologist has to repeat AP projection to include the ankle joint.
A radiograph of a lateral patella shows that the patella is drawn tightly against the intercondylar sulcus.
Which positioning modification should be performed to improve the quality of the image during the repeat exposure?
Rotate the body and leg until the knee is in a true lateral position. Ensure that the knee is flexed 5-10 degrees.
What condition may cause the tibial tuberosity to be pulled away from the tibial shaft?
Osgood-schlatter disease
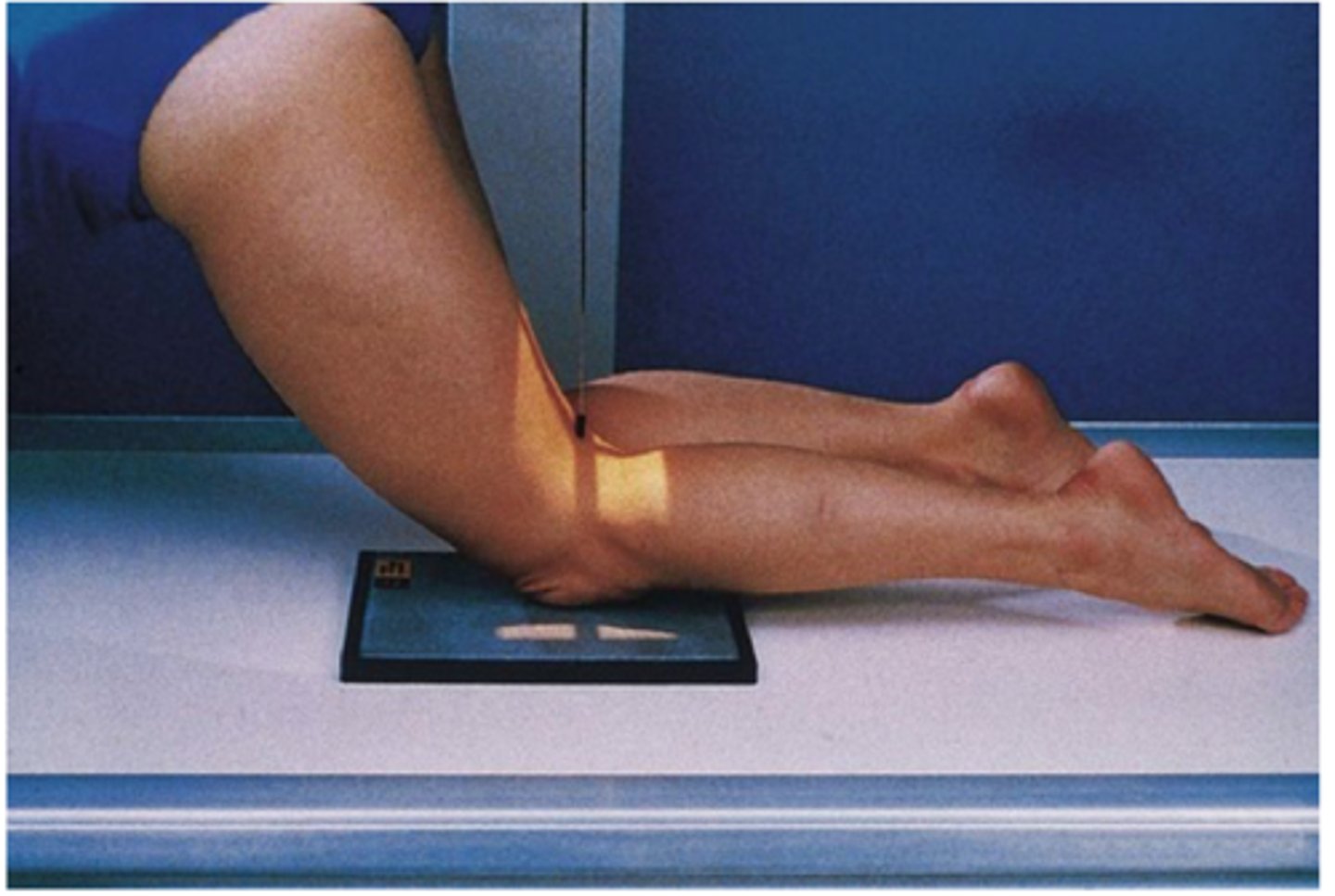
What is the major disadvantage of the Settegast method?
The major disadvantage of this method is that acute knee flexion tightens the quadriceps and draws the patella into the intercondylar sulcus reducing the diagnostic value of this projection.
What is the central ray for an AP projection of the knee?
CR parallel to the articular facets (tibial plateau) and directed ½ inch distal to apex of the patella.
Which basic projection of the knee best demonstrated the proximal fibula free of superimposition?
AP oblique projection - medial rotation
For an AP oblique projection of the knee, the ____ rotation best visualizes the lateral condyle of the tibia and the head and neck of the fibula.
45 degrees
What is the recommended central-ray placement for a lateral knee position on a tall, slender male patient with a narrow pelvis (without support of the lower leg)?
CR angulation 5 degrees
How much flexion is recommended for a lateral projection of the knee to best demonstrate the patellofemoral joint space?
20-30 degrees
Which positioning error(s) is/are present if the distal borders of the femoral condyles are not superimposed on a radiograph of a lateral knee on average-sized knee? (more than one answer is possible)
Over rotation of the lateral knee, incorrect angle of CR, or incorrect flexion of the knee.
What is the best modality to examine ligament injuries of the knee?
Magnetic resonance imaging (MRI)
What type of CR angle is required for superoinferior sitting tangential method for the patella (HOBBS modification)?
No CR angle, CR must be perpendicular to the IR.
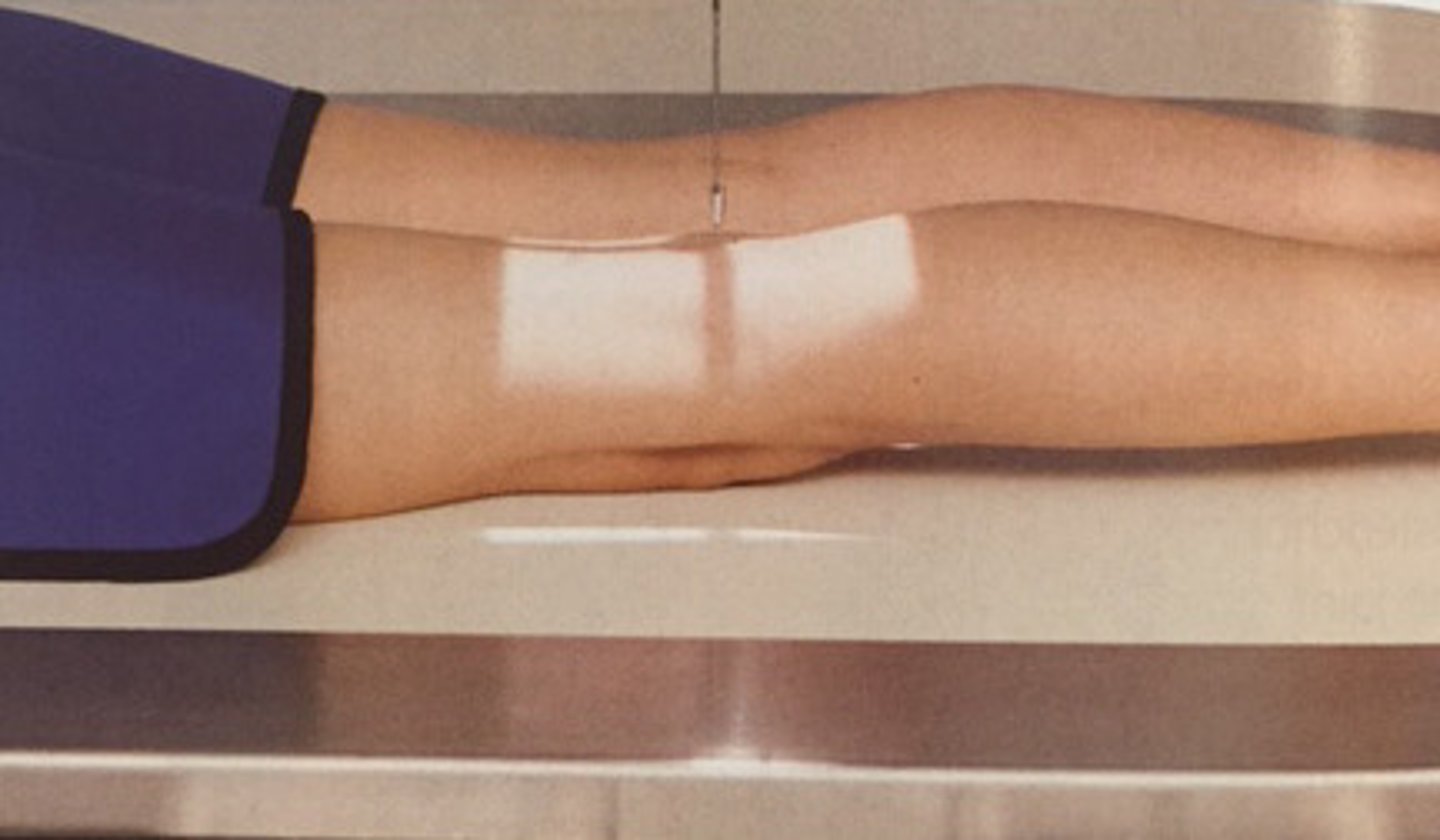
How to position patient during an AP projection of the lower leg (tibia and fibula)?
-pt in supine position
-leg extended
-pelvis, knee, and leg in true AP with no rotation
-dorsiflex foot to 90 degrees to lower leg
-both ankle and knee joints are 1-2 inches

What is the alternative follow-up examination routine for the AP and Lateral projection of lower leg (tibia and fibula)?
To include only the joint that is nearest the site of injury and to place the joint a minimum of 2 inches from end of IR.
For initial examinations, it is important especially when the injury site is in the distal leg, to include the proximal tibiofibular joint area because it is common to have a second fracture at this site.
What is the CR for the AP projection lower leg (tibia and fibula)?
CR perpendicular to the IR, directed to midpoint of lower leg
How to position the pt during a lateral-mediolateral projection of the lower leg (Tibia and fibula)
leg in true lateral position (plane of patella perpendicular to IR)
both ankle and knee joints 1-2 inches from ends of IR
if limbs are too long, place lower leg diagonally on IR
What is the CR for a lateral-mediolateral projection of the lower leg (Tibia and fibula)
CR perpendicular to IR, directed to midpoint of lower leg
What anatomy is demonstrated for both an AP and Lateral lower leg projections?
entire tibia and fibula
include ankle and knee joints
What can the technician do if patient cannot be turned during a lateral projection of the lower leg?
horizontal beam (cross-table) lateral
image can be taken cross-table with IR placed on edge between lower legs
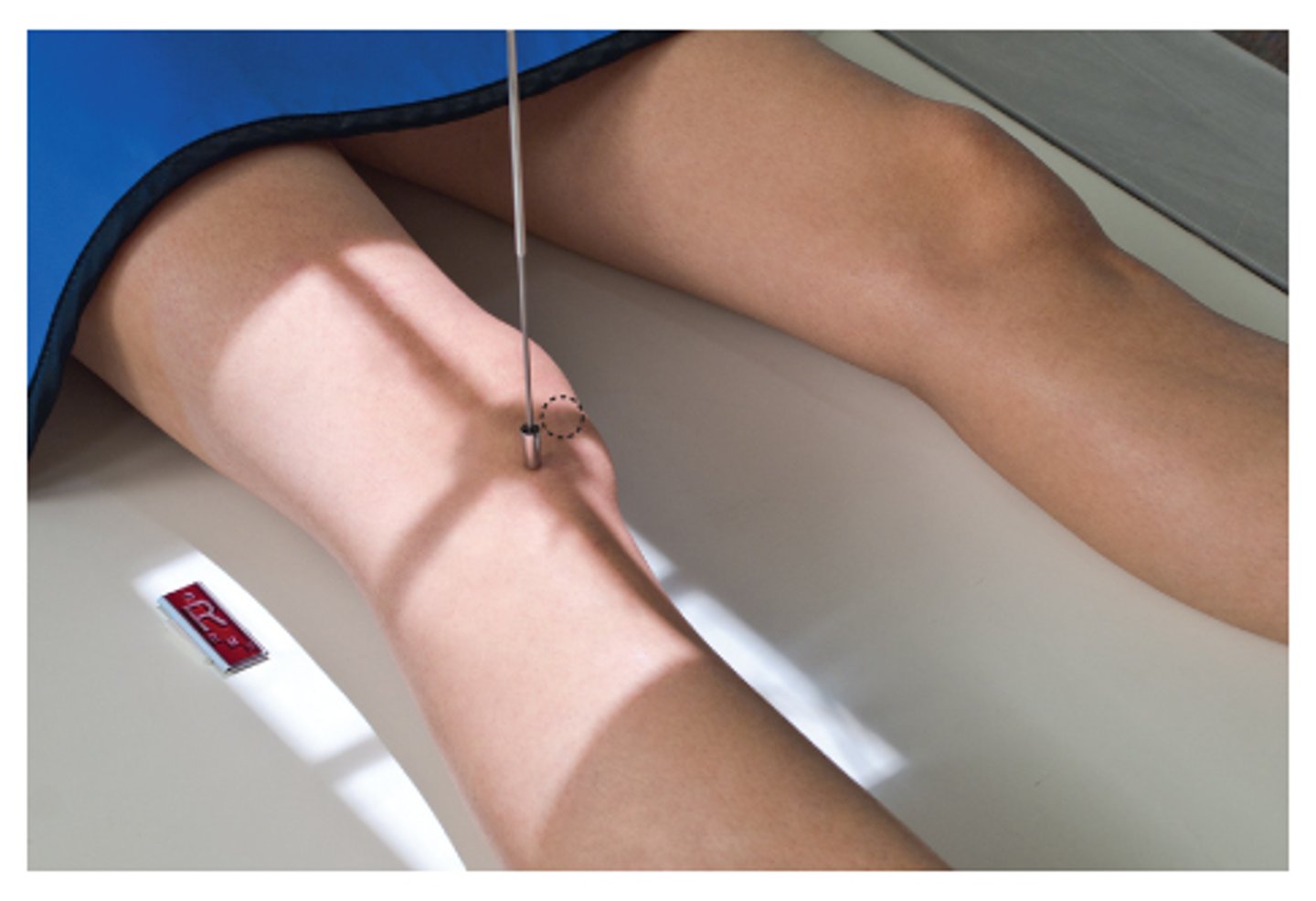
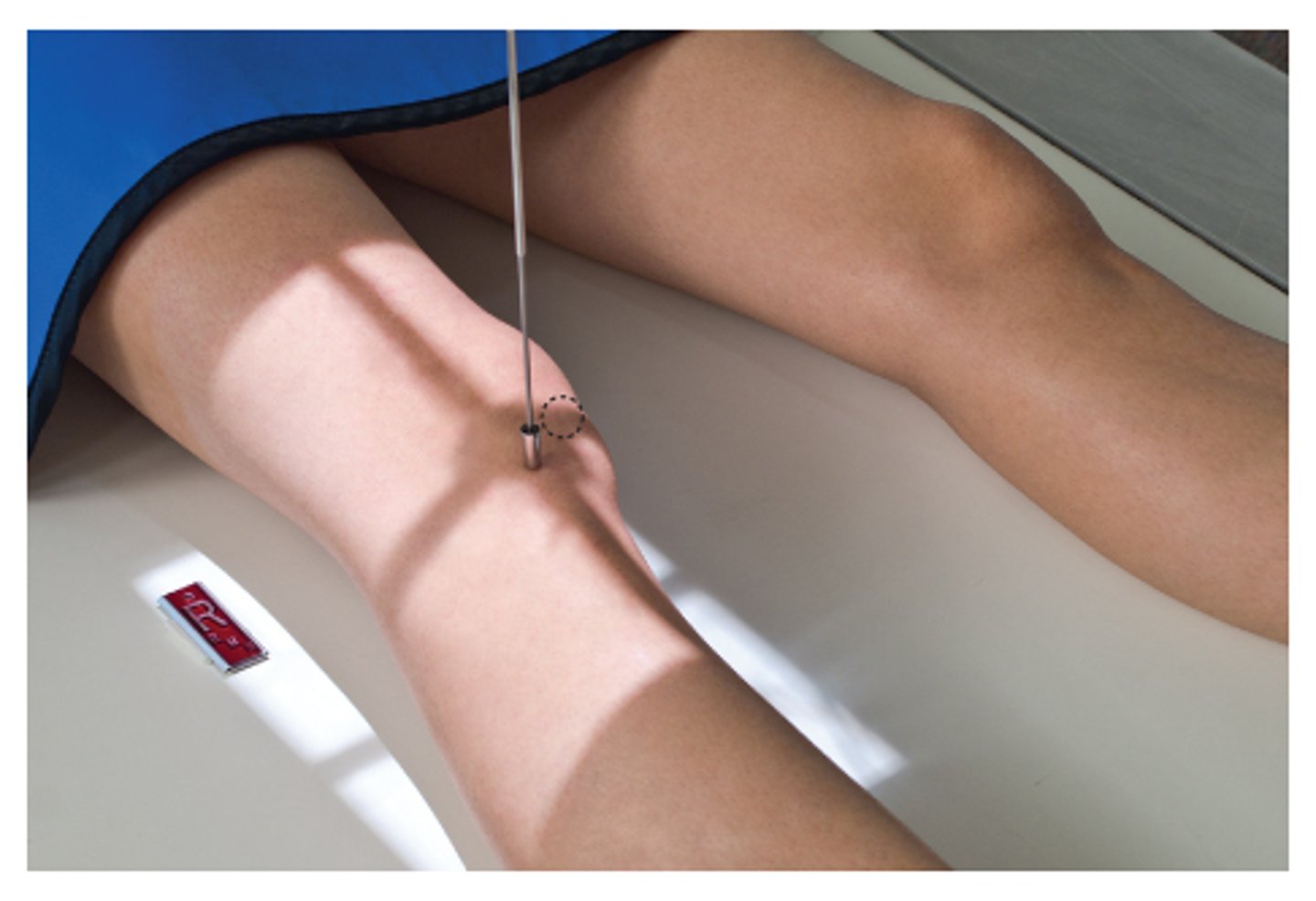
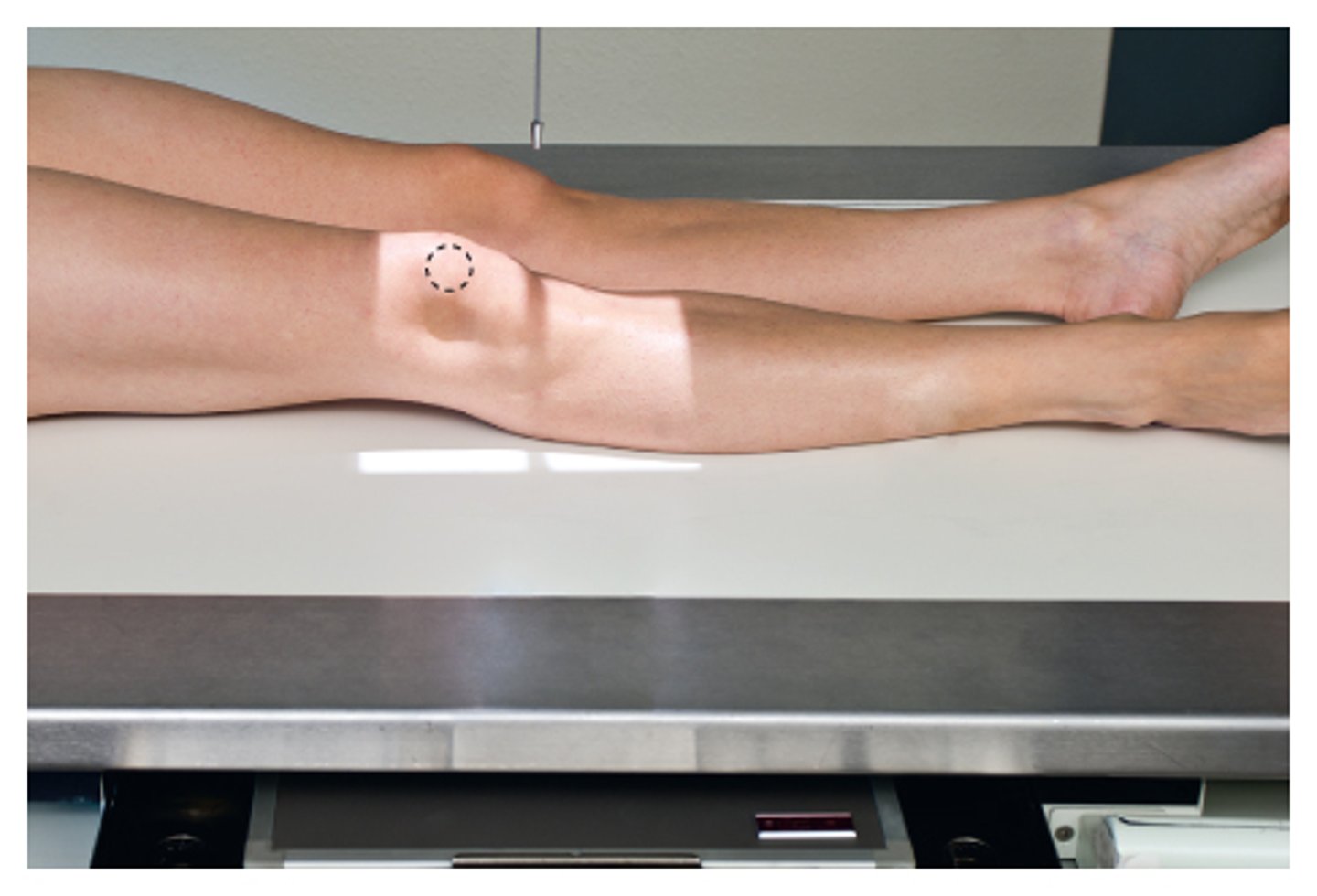
How to position patient for an AP knee?
rotate leg internally 3-5 degrees for true AP
interepicondylar line is parallel to plane of IR
Where is CR directed for AP knee?
Align CR parallel to articular facets (tibial plateau) for average size pts
direct CR 1/2 inch distal to apex of patella
How to determine that CR is parallel to the articular facets for AP knee?
<19cm = 5 degrees caudad
19-24cm = no angle
>24cm = 5 degrees cephalad
What anatomy is demonstrated for AP knee?
distal femur and proximal tibia and fibula
femorotibial joint space open
articular facets of tibia seen on end
How to position patient for an AP oblique (medial rotation) knee?
rotate entire leg internally 45 degrees (interepicondylar 45 degrees to plane of IR)
Where is CR directed for AP oblique (medial rotation) knee?
angle CR 0 degrees on average patient
midpoint of knee at a level 1/2 inch distal to apex of patella
What is demonstrated in the AP oblique (medial rotation) knee?
distal femur and proximal tibia/fibula
patella superimposing the medial femoral condyle
lateral condyles of the femur and tibia
medial and lateral knee joint spaces appear unequal
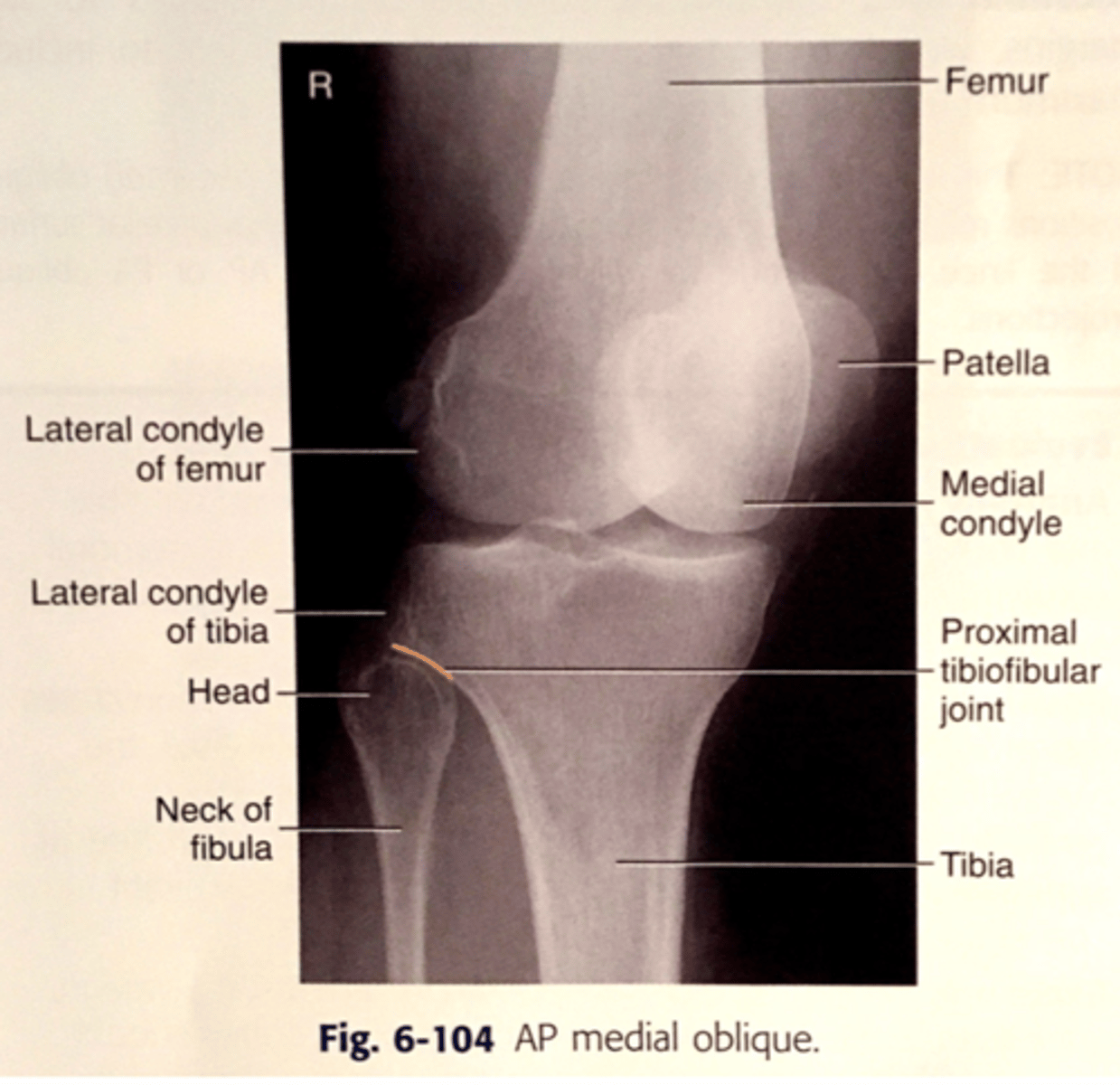
What is visualized for an AP oblique (medial rotation) knee?
head and neck of the fibula are visualized without superimposition
half of patella should be seen free of superimposition by the femur
How to position pt for an AP oblique (lateral rotation) knee?
rotate entire leg externally 45 degrees (interepicondylar 45 degrees to plane of IR)
Where to direct CR for an AP oblique (lateral rotation) knee?
angle CR 0 degrees on average pt
direct CR midpoint of knee at level 1/2 inch distal to apex of patella
Anatomy demonstrated for AP oblique (lateral rotation) knee?
distal femur and proximal tubua/fibula
patella superimposing the lateral femoral condyle
medial condyles of femur and tibia
What visualized for AP oblique (lateral rotation) knee?
proximal fibula superimposed by the proximal tibia
medial condyles of the femur and tibia seen in profile
half of patella should be free of superimposition by the femur
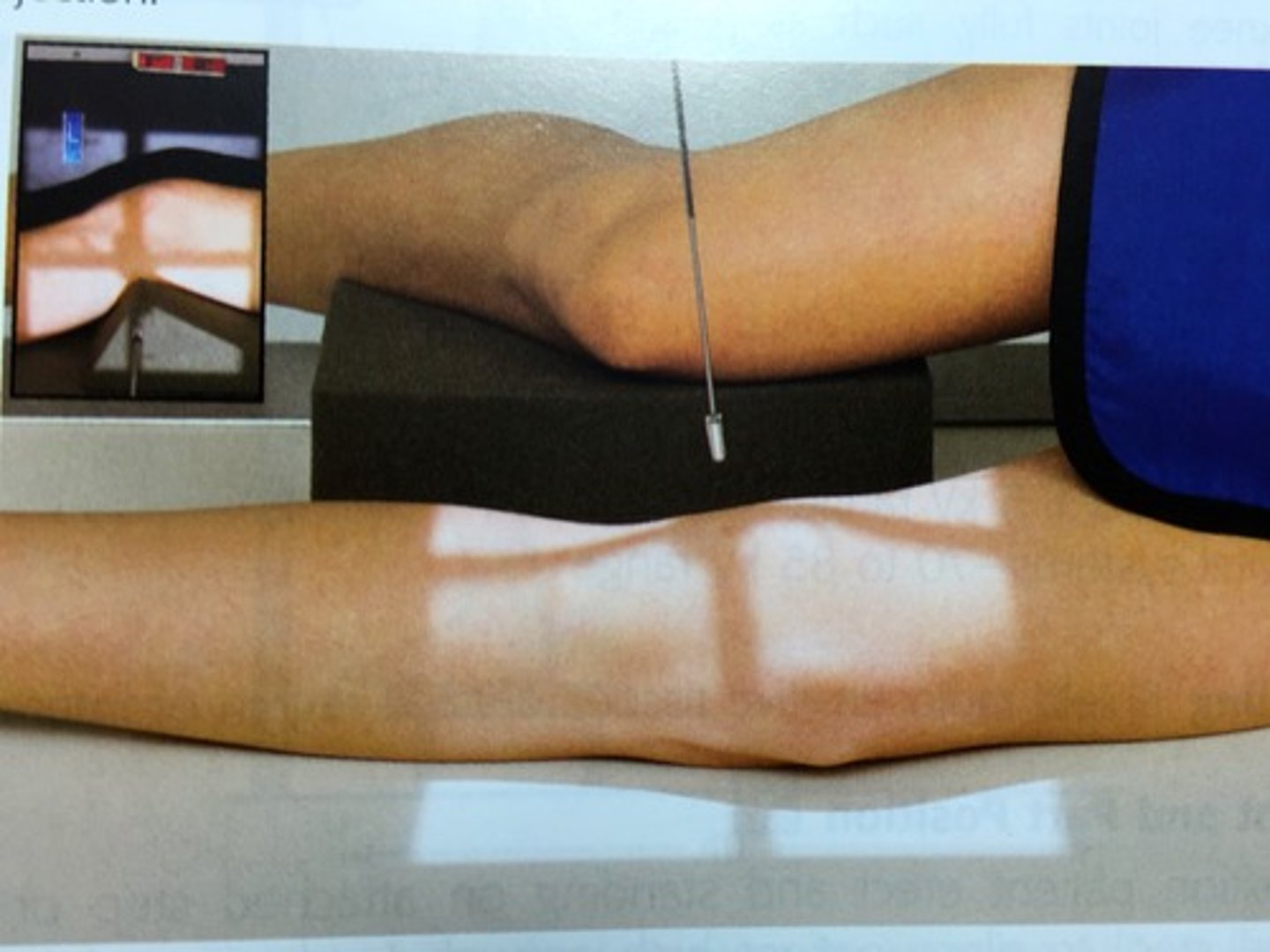
How is the pt positioned for a lateral-mediolateral knee?
rotate body and leg until knee is in true lateral position (femoral condyles directly superimposed and plane of patella perpendicular to IR)
flex knee 20-30 degrees for lateral recumbent projection
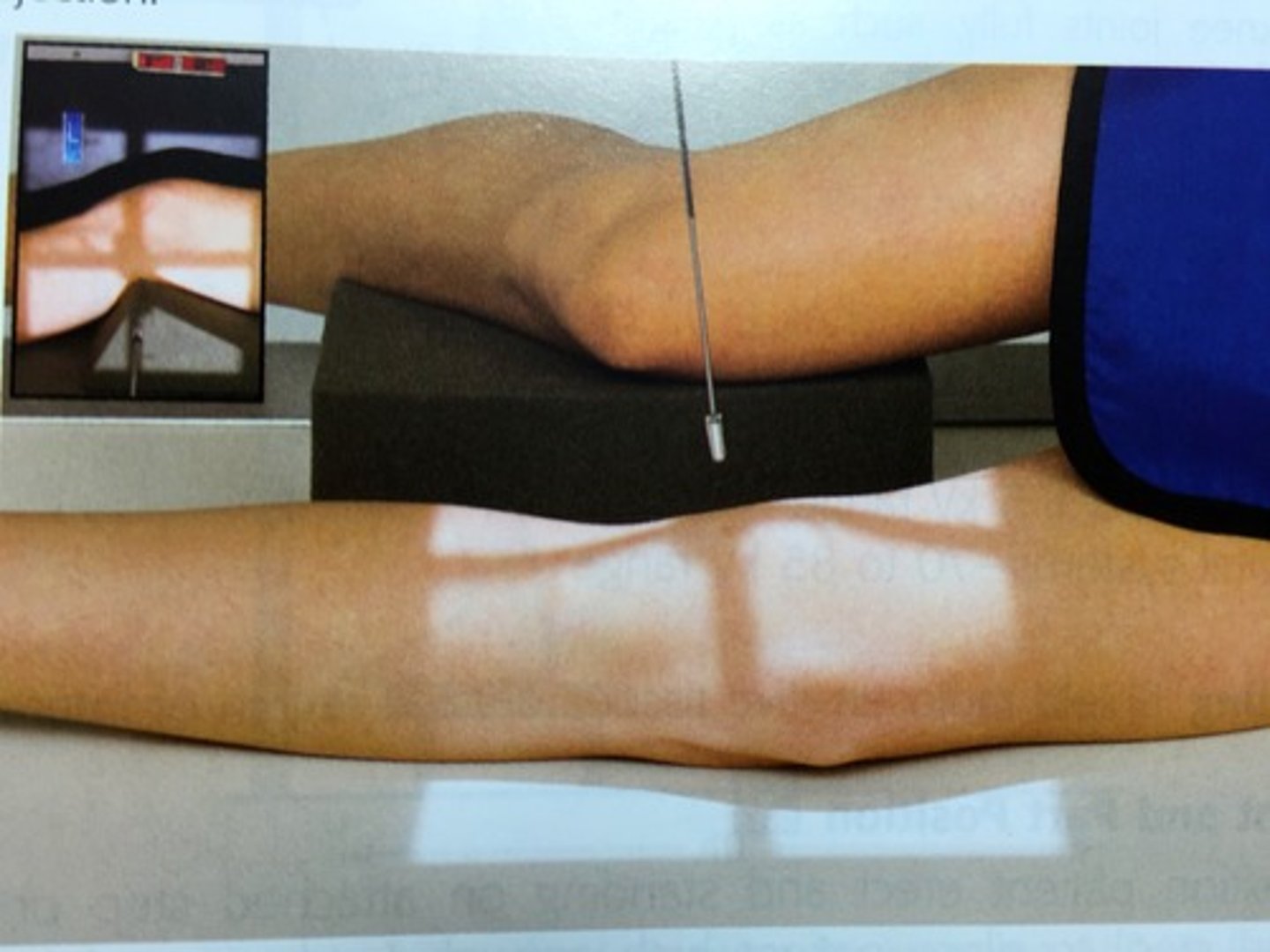
Where is CR directed for lateral-mediolateral knee?
angle CR 5-7 degrees cephalad for lateral recumbent projection
direct CR to 1 inch distal to medial epicondyle
What are two ways that the lateral-mediolateral knee projection can be taken?
lateral recumbent postion
horizontal beam projection (when pt is unable to flex the knee)
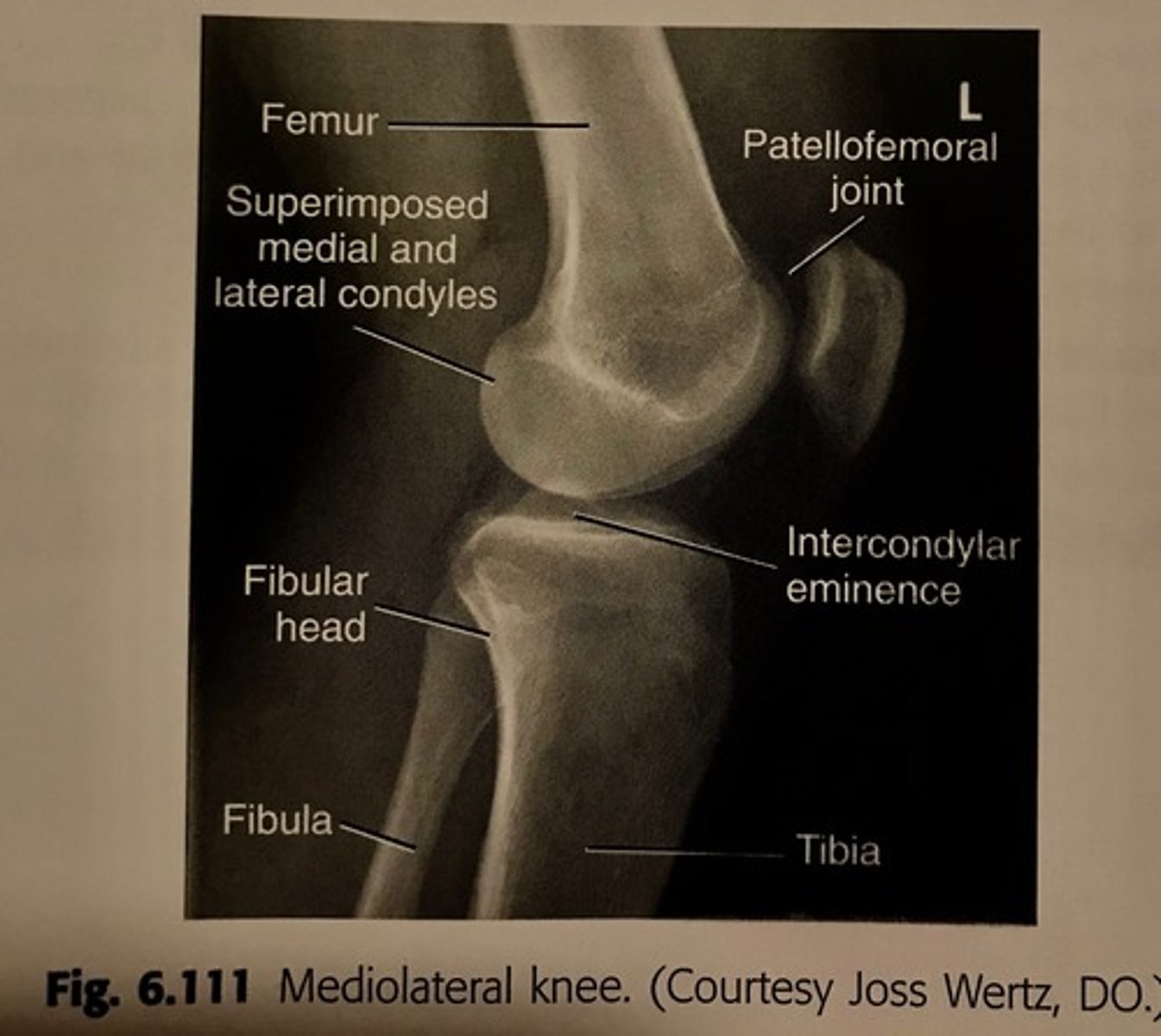
What anatomy is demonstrated for lateral-mediolateral knee?
distal femur
proximal tibia/fibula
patellofemoral and knee joints should be open
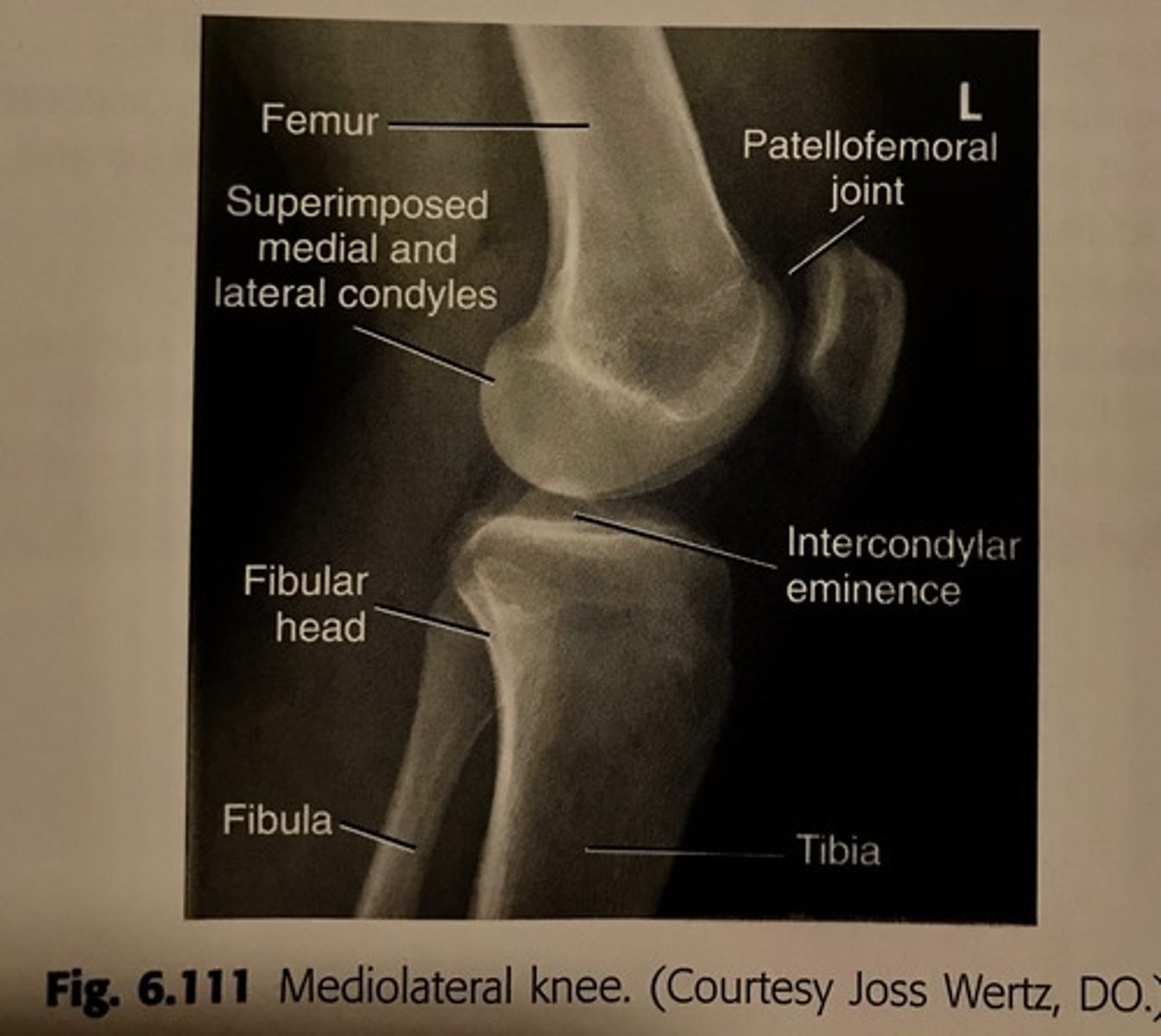
What is visualized in the lateral-mediolateral knee?
true lateral position of knee demonstrates posterior borders of the femoral condyles directly superimposed
patella should be seen in profile with patellofemoral joint space open
the 5-10 degrees cephalad angle of CR should result in direct superimposition of distal borders of the condyles
What is the CR angulation for a short pt with a wide pelvis for a lateral-mediolateral knee?
7-10 degrees
What is the CR angulation for a tall, male pt with a narrow pelvis for a lateral-mediolateral knee?
5 degrees
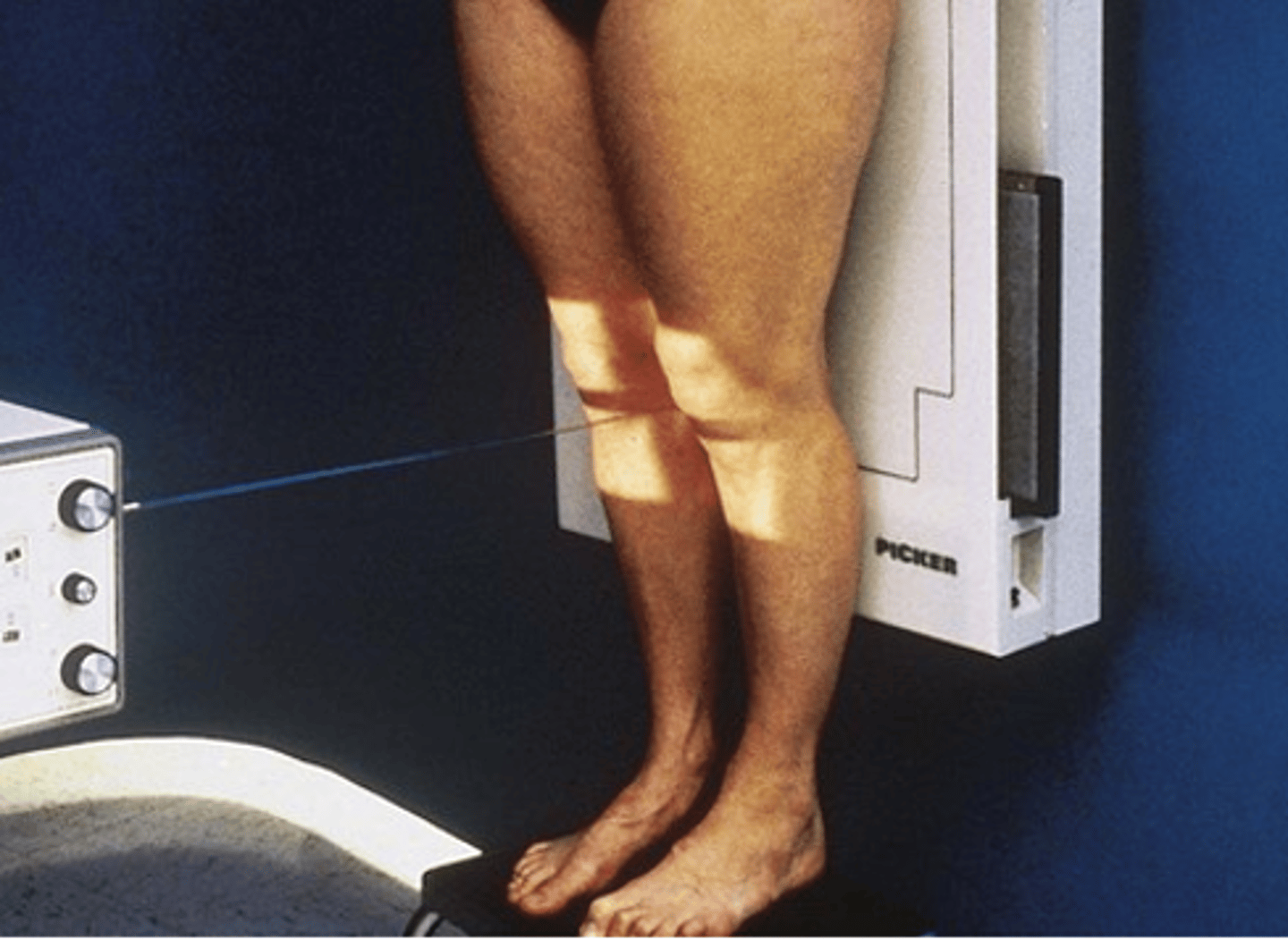
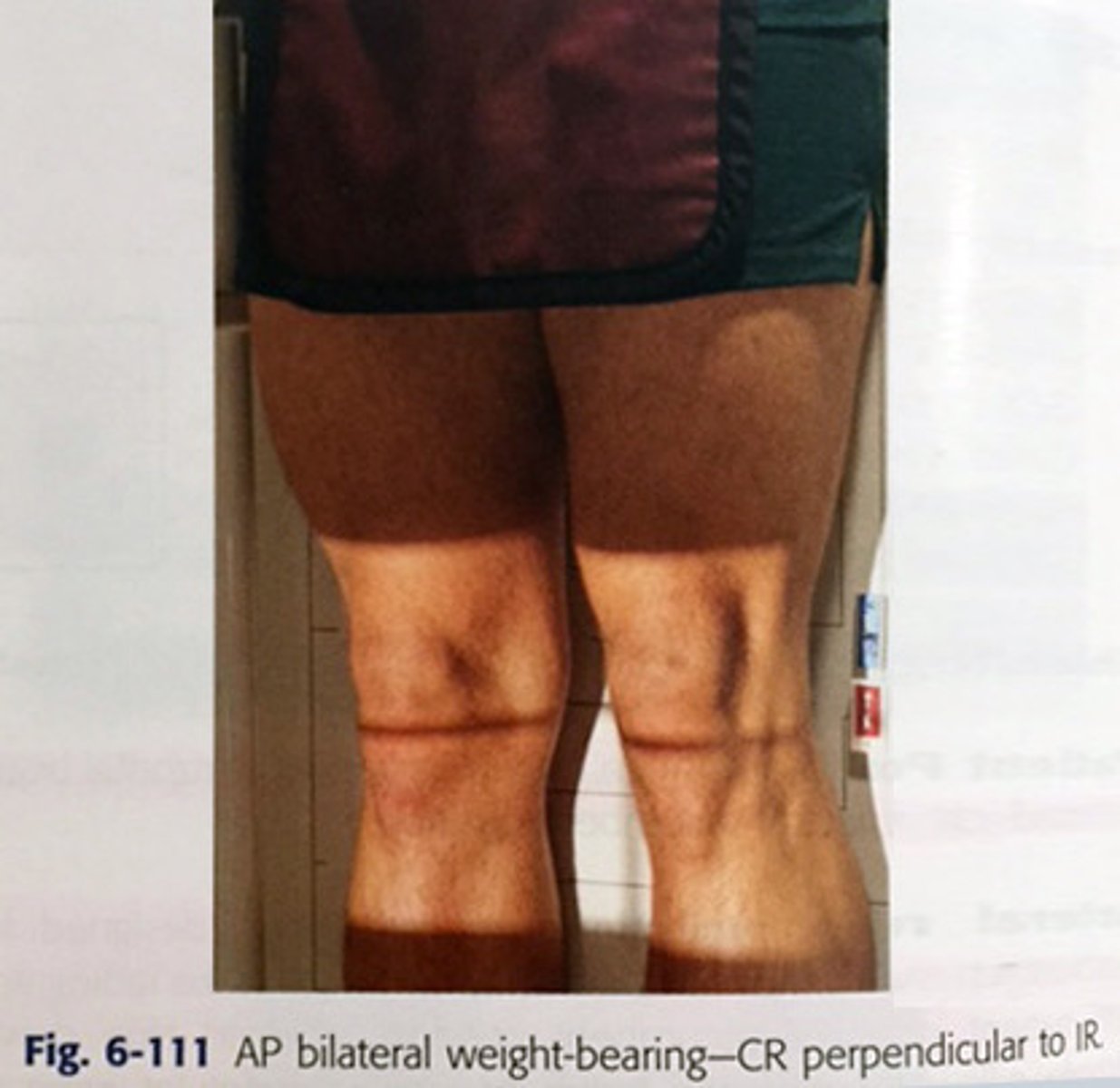
What is the purpose of the AP weight-bearing bilateral knee?
femorotibial joint spaces of the knees demonstrated for possible cartilage degenration or other knee joint pathologies
How to position pt for an AP weight-bearing bilateral knee?
pt standing
feet straight ahead with weight evenly distributed on both feet
align and center bilateral legs and knees to CR
Where is CR directed for an AP weight-bearing bilateral knee?
CR perpendicular to IR
5-10 degrees caudad on thin pt
directed to midpoint between knee joints at a level 1/2 inch below apex of patella
What is the alternative projection for an AP weight-bearing bilateral knee?
alternative PA
pt facing the table, knees flexed 20 degrees
CR 10 degrees caudad to level of knee joints
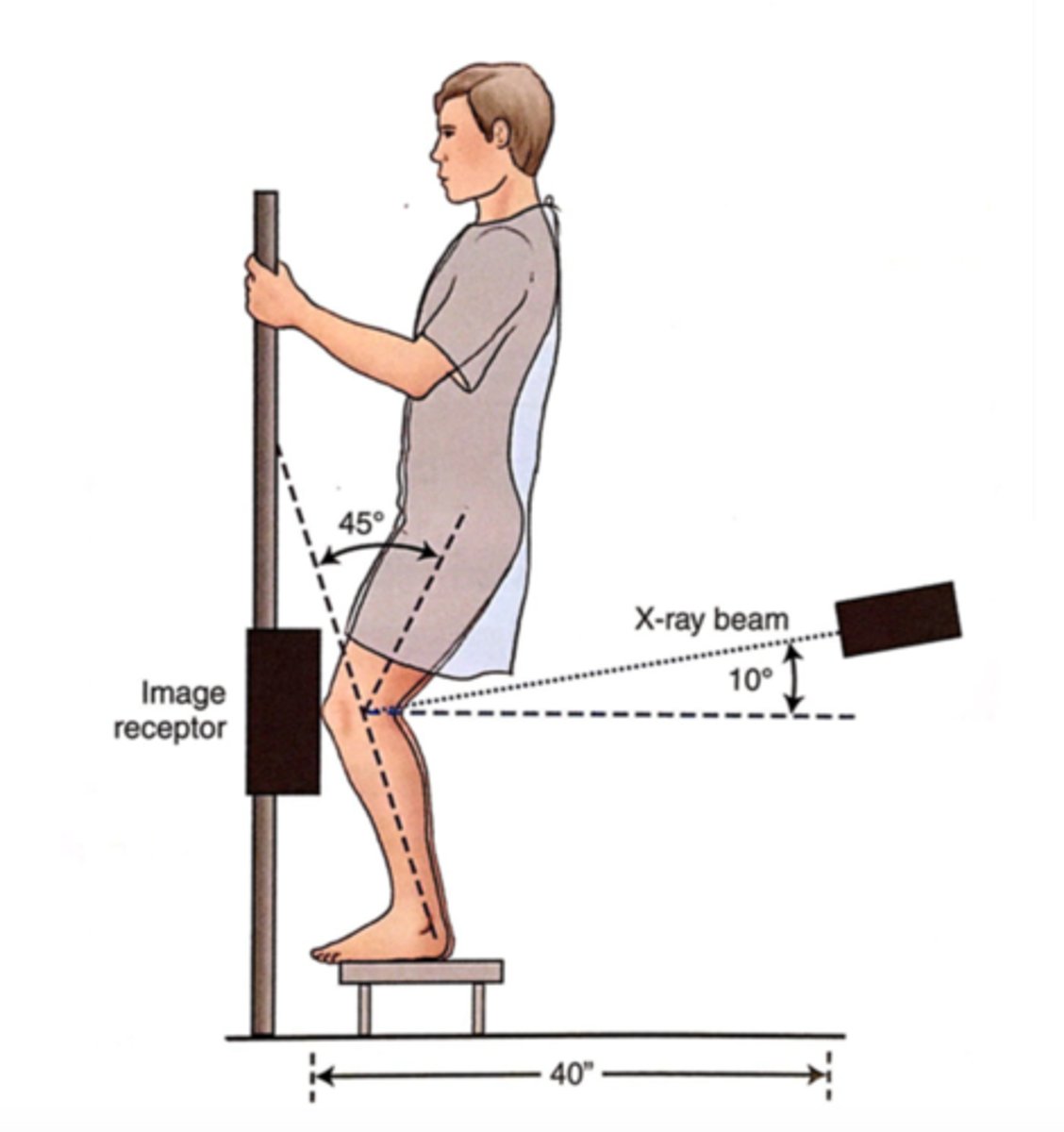
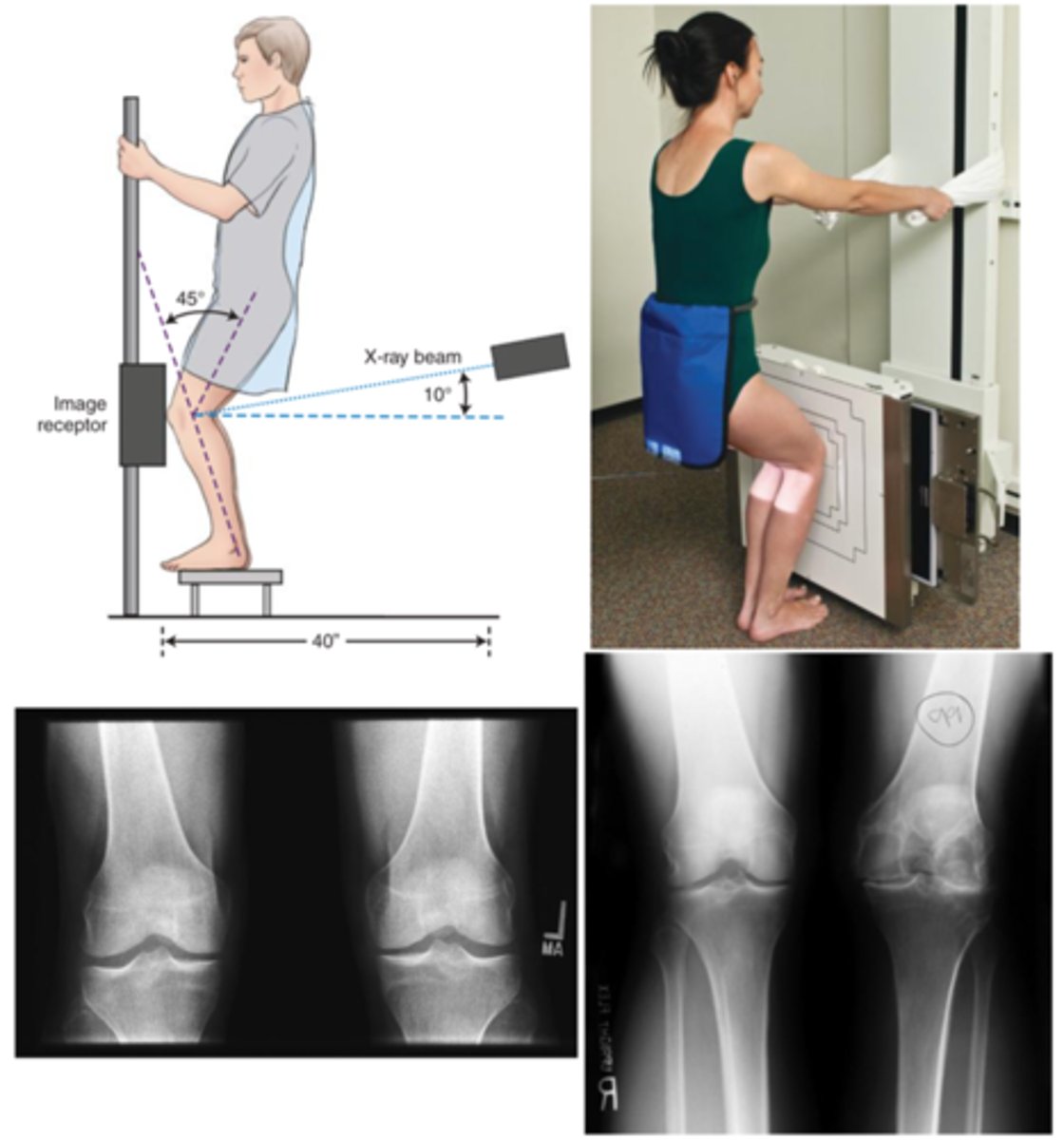
What is the Rosenberg method?
PA axial weight-bearing bilateral knee projection knee

How is pt positioned for the Rosenberg method?
Pt erect
provide step stool for some pt so they are high enough for CR to be 10 degrees caudad
feet straight ahead and weight evenly distributed
knee flexed 45 degrees
What anatomy is demonstrated for the Rosenberg method?
distal femur
proximal tibia/fibula
femorotibial joint space
intercondylar fossa
Where is CR directed for the Rosenberg method?
CR angled 10 degrees caudad
centered directly to midpoint between knee joints at level 1/2 inch below apex of patella

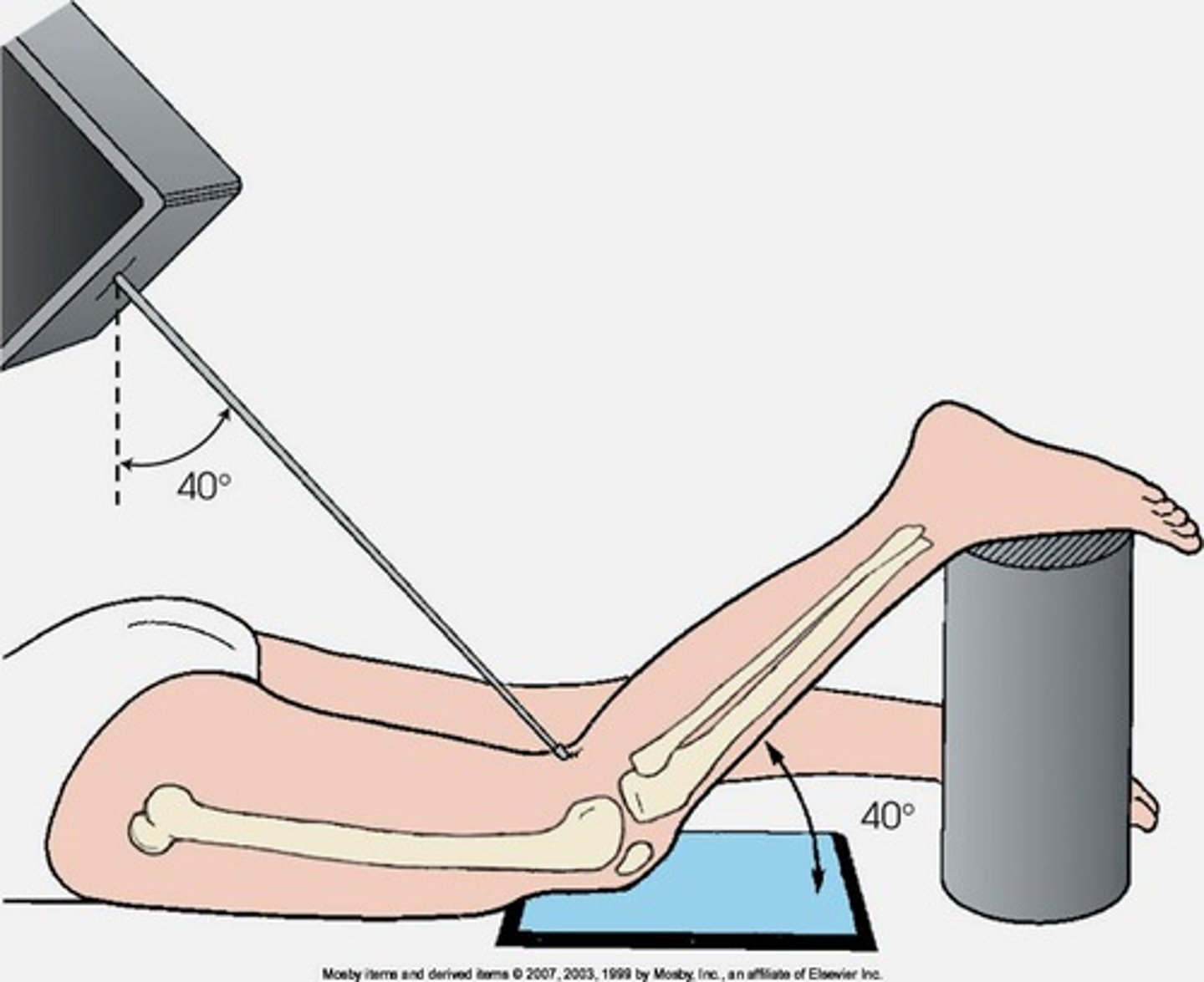
Which methods are used for the projections of the intercondylar fossa?
camp coventry method
holmblad method (and variations)
beclere method
what is the camp coventry method?
projection for the intercondylar fossa in profile
pt in prone position and knee flexed 40-50 degrees
CR perpendicular to lower leg 40-50 degrees caudad
What is the Holmblad method?
projection for the intercondylar fossa in profile
pt kneeling, leaned forward 20-30 degrees degrees
CR perpendicular to IR and lower leg, direct CR to midpopliteal crease
What is the Beclere method?
AP axial projection knee of intercondylar fossa in profile
flex knee 40-45 degrees , and position support under IR as needed to place IR against posterior thigh and lower leg
CR directed perpendicular to lower leg approx. 40-45 degrees cephalad
direct CR 1/2 inch distal to apex of patella
How to position pt for the PA patella and patellofemoral joint?
pt in prone position, legs extended
true PA: align interepicondylar line parallel to plane of IR (requires about 5 degrees internal rotation of anterior knee)