Abdominal Abnormalities (Ch. 62-63)
1/57
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
58 Terms
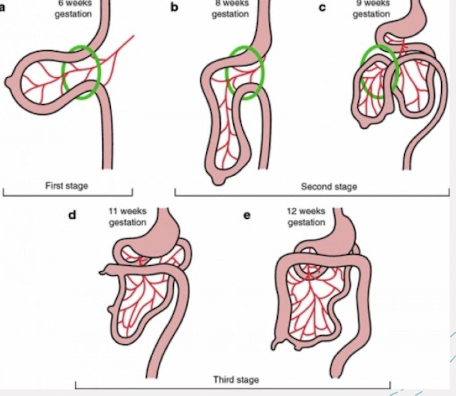
embryology review
physiologic midgut herniation occurs between 8-12 weeks gestation
some of the bowel temporarily migrates into the base of the umbilical cord
around 12 weeks gestation, bowel rotates and returns back into the abdominal cavity
if this process (normal development of abdominal wall) does not occur correctly, abdominal organs may remain at the base of the umbilical cord, leading to abdominal wall abnormalities
how to image abdominal wall
image the cord insertion site
note presence/absence of defects
what is the relation of cord to defect?
MC abdominal wall defects:
omphalocele
umbilical hernia
gastroschisis
in presence of abdominal wall defects, look for other abnormalities
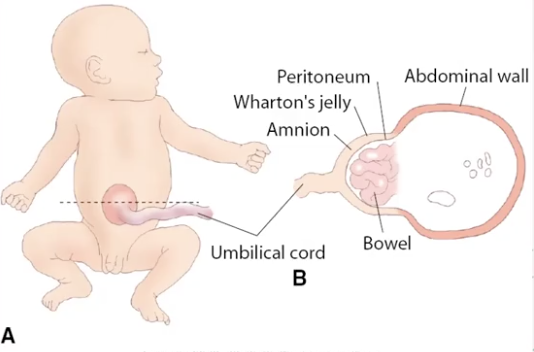
omphalocele
during 8-12th weeks of development, fetal bowel normally migrates into umbilical cord from abdominal cavity
bowl-containing omphalocele occurs when bowel loops fail to return to abdomen
intra-abdominal structures herniate into the base of the umbilical cord
herniation is covered by membrane that consists of amnion and peritoneum
cord goes through the omphalocele
AFP is within normal limits (may be slightly elevated)
omphalocele: bowel-containing vs liver-containing
bowel-containing
intestines fail to return
higher risk of associated chromosomal abnormalities and other anomalies
variable amount of bowel (only) in the herniation
liver-containing
defect affects the abdominal wall closure (closure of muscles, fascia, and skin)
herniation includes fetal liver and sometimes variable amount of bowel
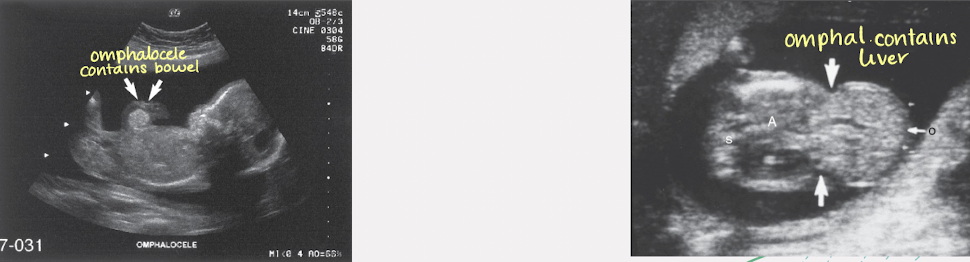
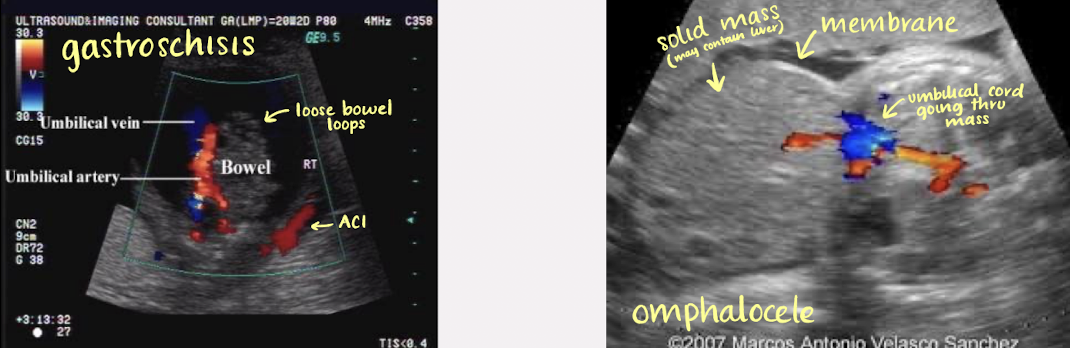
SONO: omphalocele
abdominal wall mass should be continuous with umbilical cord
Doppler to demonstrate intrahepatic umbilical vein coursing through defect
membranous sac should be identified covering contents
document size; increased AC
identify contents of membranous sac
bowel only; liver in and out of sac
hydramnios is common

pathology?
omphalocele
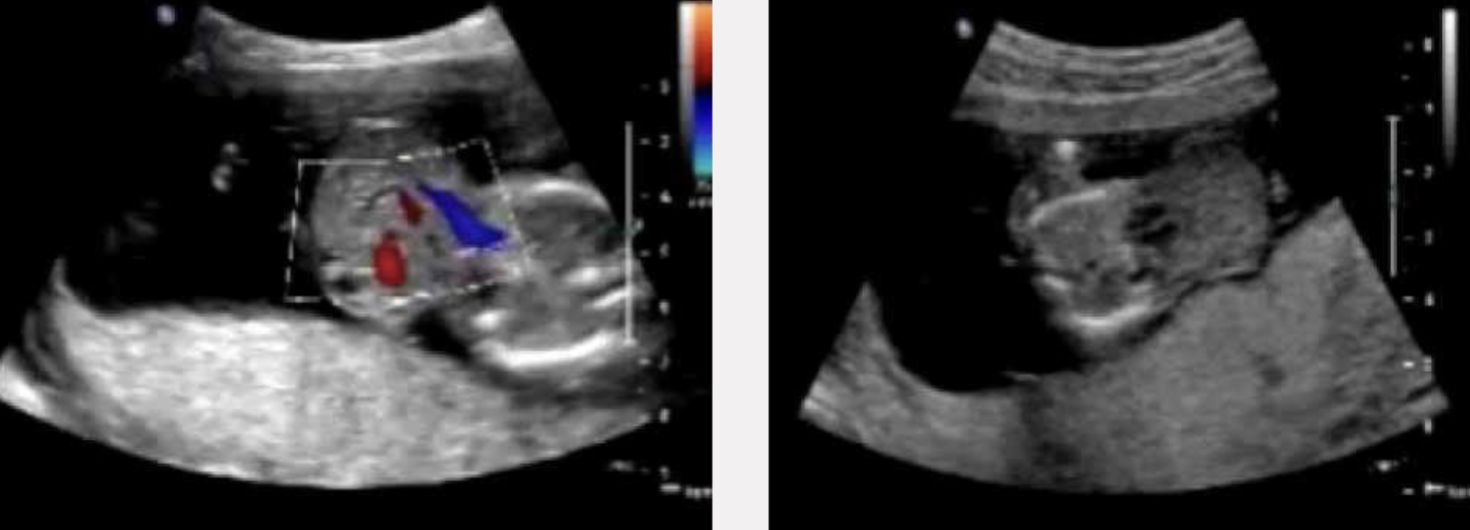
pathology?
omphalocele
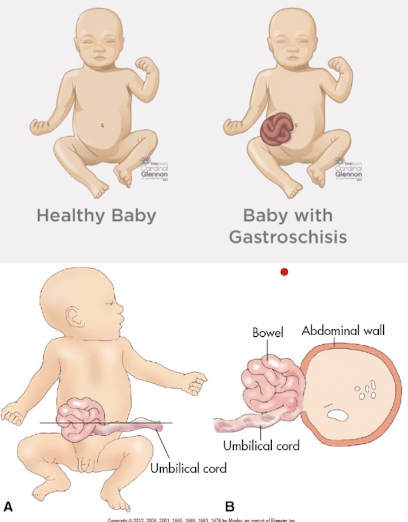
gastroschisis
periumbilical opening in abdominal wall
allows for protrusion of bowel through the defect
herniation of bowel and, infrequently, stomach and genitourinary organs (rarely the stomach)
defect is nearly always to the right of the umbilical cord
umbilical cord insertion is normal
no skin or membrane covering the defect or herniated contents
AFP levels are significantly higher compared to omphalocele
why are AFP levels higher in gastroschisis?
because it does not have a membrane to cover the internal organs of fetus—organs are exposed
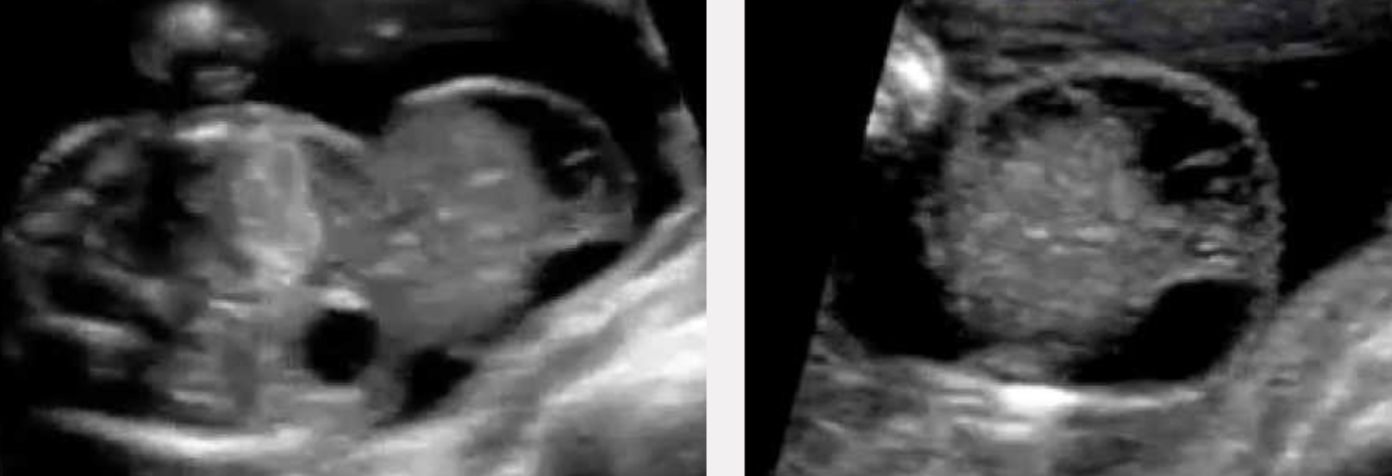
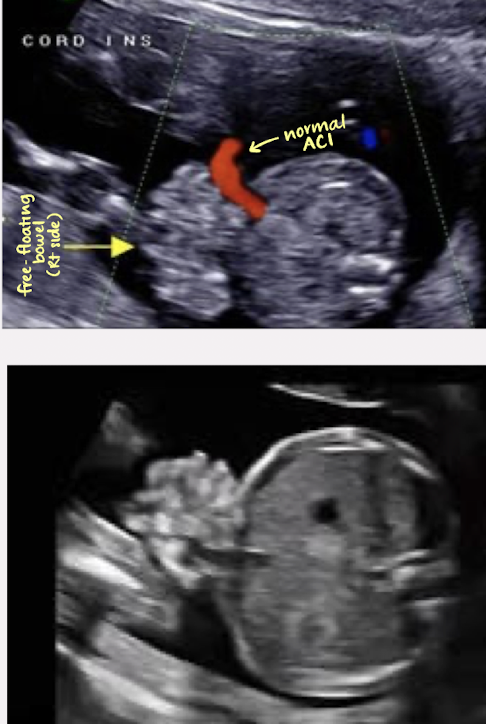
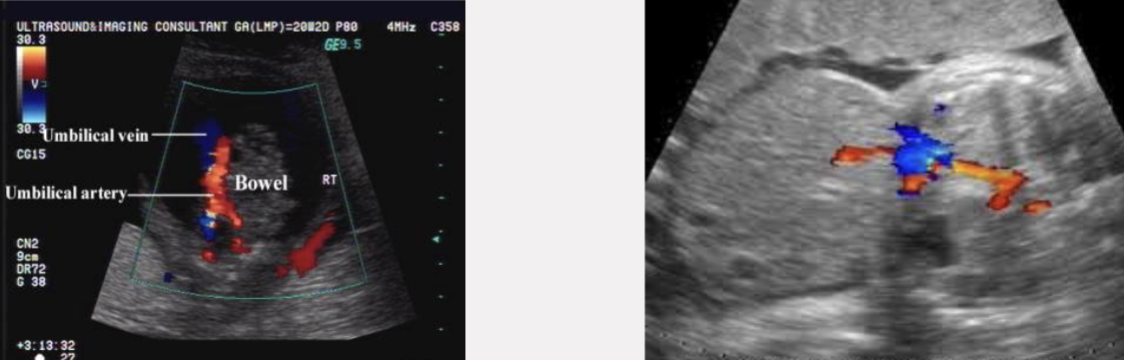
SONO: gastroschisis
right paraumbilical defect of abdominal wall
rarely a left-side defect
normal fetal cord insertion
free-floating herniated bowel
other organs may be involved
herniated bowel may be dilated or thick-walled; may be obstructed

pathology?
gastroschisis
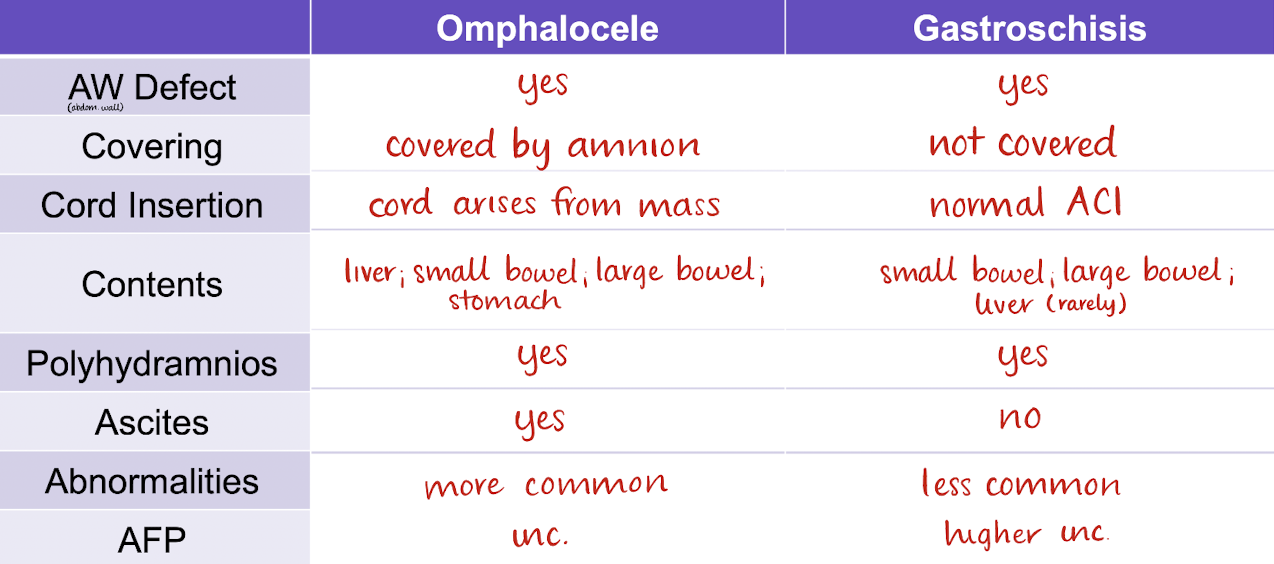
omphalocele vs gastroschisis summary chart
which is omphalocele? which is gastroschisis?
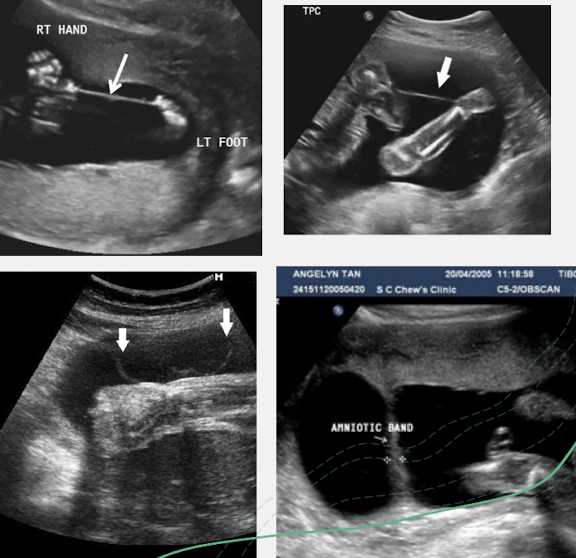
amniotic band syndrome (ABS)
rupture of amnion → entrapment or entanglement of fetal parts by “sticky” chorion
early entrapment → severe craniofacial defects and internal malformations
late entrapment → amputations or limb restrictions
increased AFP
associated abdominal wall anomalies
gastroschisis; omphalocele
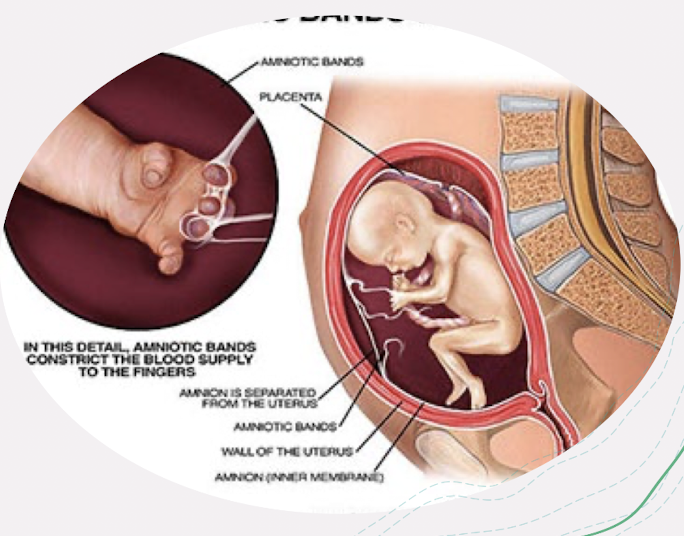
SONO: amniotic band syndrome (ABS)
echogenic bands within amniotic cavity
follow band from uterine wall to fetal attachment
if bands are small, may not be able to visualize
any missing extremities or facial deformities should raise suspicion of ABS
document normal appearance of extremities and fetal contour
help to rule out ABS
limb-body wall complex
aka body stalk anomaly, or short umbilical cord syndrome
extends as sheet from margin of cord
rare malformation caused by failure of closure of ventral body wall
involves: limb or spinal defects, wall defects, thoracic/abdominal defects, craniofacial defects, scoliosis
left-sided body wall defects 3x more common than right-sided defects
prognosis: fatal
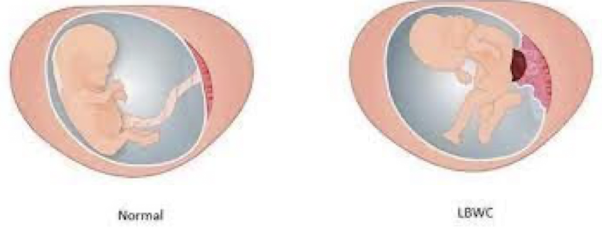
SONO: limb-body wall complex
large ventral wall defect of abdomen and thorax (usually left-sided)
eviscerated organs form a complex mass entangled with membranes
cranial anomalies
limb defects
short umbilical cord
fetus is inseparable from placenta (fetus is right on top of it)

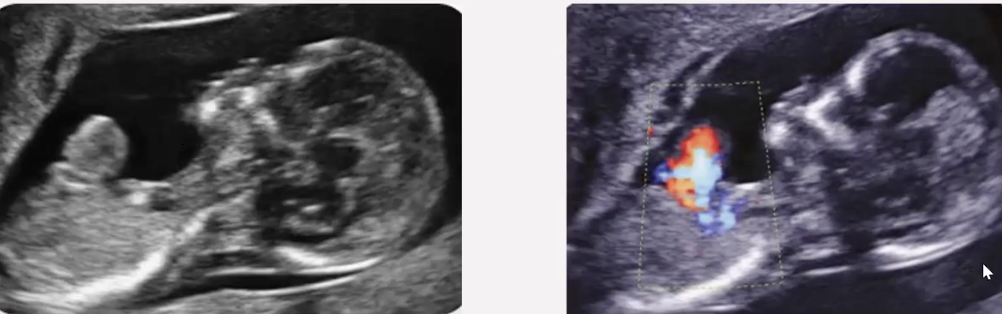
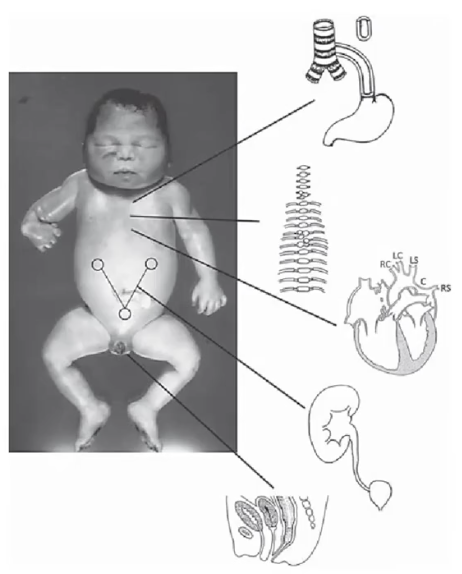
pentalogy of Cantrell
rare syndrome causing defects involving 5 abnormalities:
anterior diaphragmatic hernia
high omphalocele (primary finding)
intracardiac defect
ectopia cordis (cleft defect in lower sternum)
defect of diaphragmatic pericardium
prognosis: very poor
associated with various defects

ectopia cordis
exposed heart outside chest wall through cleft sternum
most dramatic finding is presence of heart outside thoracic cavity
anomalies most frequently associated with ectopia cordis:
omphalocele
cardiovascular malformations
craniofacial defects
Beckwith-Wiedemann Syndrome
rare syndrome results in a grossly large fetus
characterized by:
macroglossia
omphalocele
embryonic tumors
visceromegaly
macrosomia
associated with hepatic, renal, and adrenal tumors; also ear creases
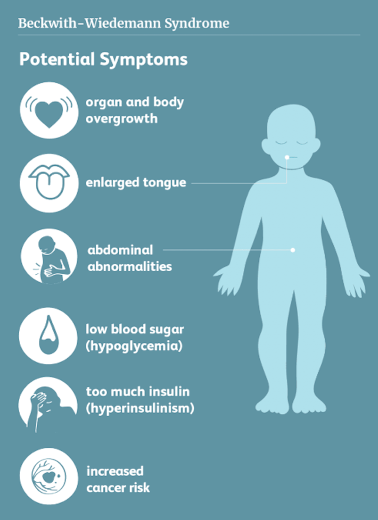
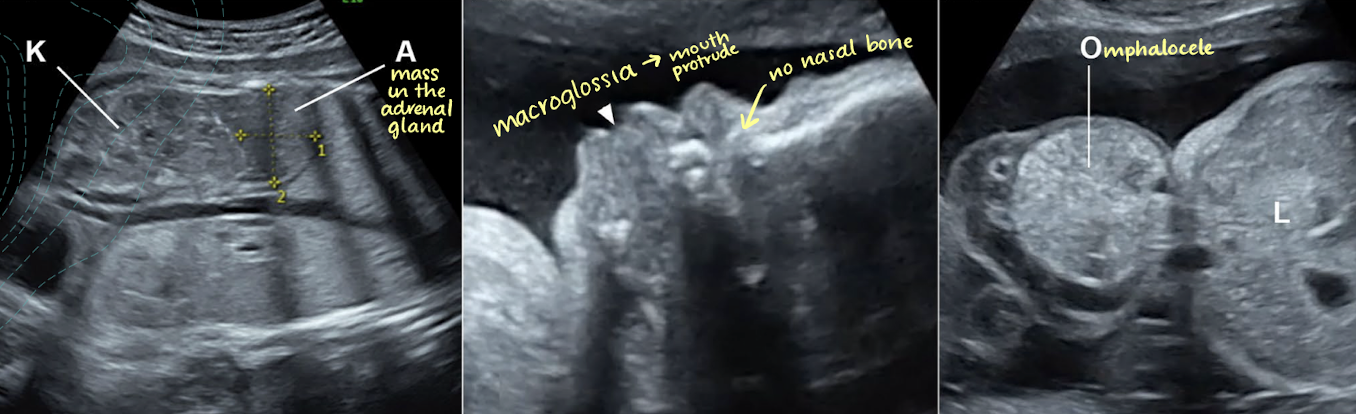
SONO: Beckwith-Wiedemann Syndrome
large for dates fetus with enlarged kidneys, omphalocele, and macroglossia on 2nd trimester US
may have an enlarged spleen, liver, and adrenal glands
bladder exstrophy
defect in lower abdominal wall and anterior wall of urinary bladder
caused by incomplete closure of inferior part of abdominal wall
causes bladder to protrude outside abdomen
defects of the urethra, bladder
may be mild or severe (accompanied by omphalocele, inguinal hernia, undescended testes, anal problems)
SONO: bladder exstrophy
absence of fluid-filled bladder in pelvis
lower abdominal bulge
cord insertion is normal or low
kidneys and AFI usually normal

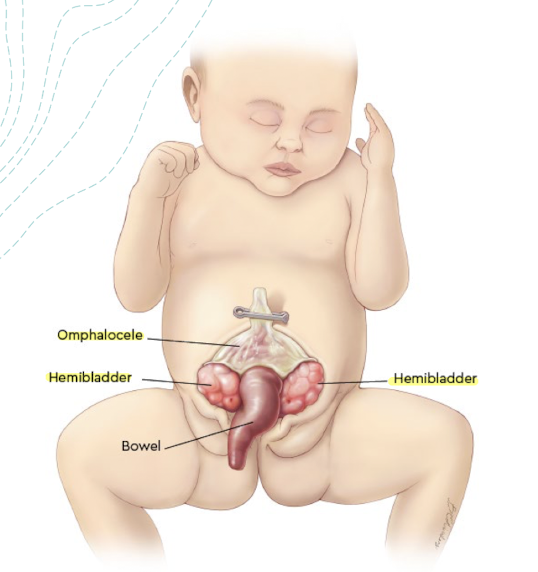
cloacal exstrophy
more rare, complex, and more extreme
condition occurs early in development that involves the primitive gut and persistent cloaca
defects urethra, bladder, and bowel are present
results in:
exstrophy of the bladder (with 2 hemibladders separated by muscosa)
omphalocele (upper part of defect)
lower abdominal wall defect
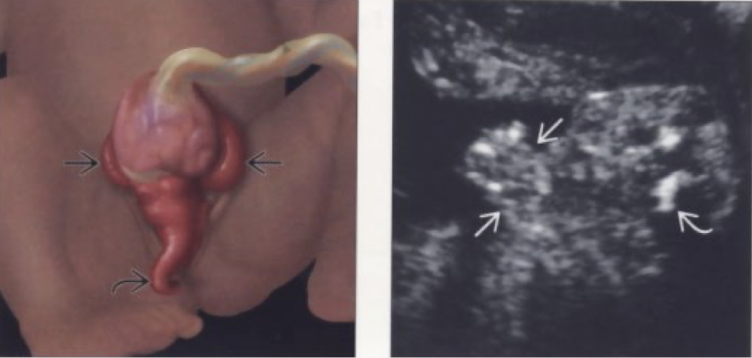
SONO: cloacal exstrophy
absence of normal bladder
lower abdominal defect
herniation of bowel between halves of bladder
omphalocele
liver (hepatobiliary abnormality)
rarely affected by isolated hepatic lesions
if lesions seen, cysts and hemangiomas are MC
fetal liver tumors are uncommon
hemangioendothelioma is MC if one is found
liver enlarges in fetuses with Rh-immune disease in response to increased hematopoiesis
SONO: liver (hepatobiliary abnormalities)
most fetal liver tumors appear as solid masses, sometimes with cystic components; may be calcified
liver calcification may be observed as isolated echogenic focus
is usually a benign finding
if multiple calcifications seen within liver, other organs such as brain and spleen may be affected
spleen (hepatobiliary abnormalities)
asplenia
absence of spleen
accompanied abnormal positions of liver, GB, and stomach
polysplenia
more than one spleen
associated with situs inversus
GB is typically absent
splenomegaly
usually associated with Rh-immine disease
GB (hepatobiliary abnormalities)
cholelithiasis
uncommon in fetus; usually resolve in utero or childhood
choledochal cyst
dilation of CBD
presents as cystic mass adjacent to GB
biliary atresia
absence of GB
may be associated with polysplenia

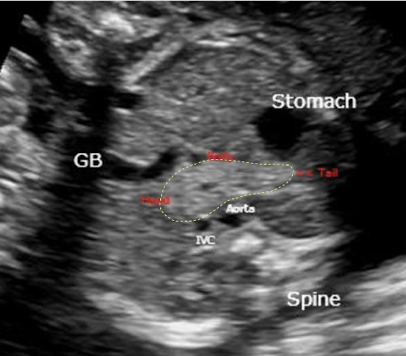
pancreas (hepatobiliary abnormalities)
fetal pancreatic anomalies are rare
pancreatic cysts are uncommon
when present, will appear as midline cystic mass
GI tract abnormalities tips
check bowel diameter
bowel dilation not evident until 20w
polyhydramnios commonly with obstruction
why? b/c fetus can’t swallow normally due to obstruction
lack of stomach: possible “upstream abnormality”
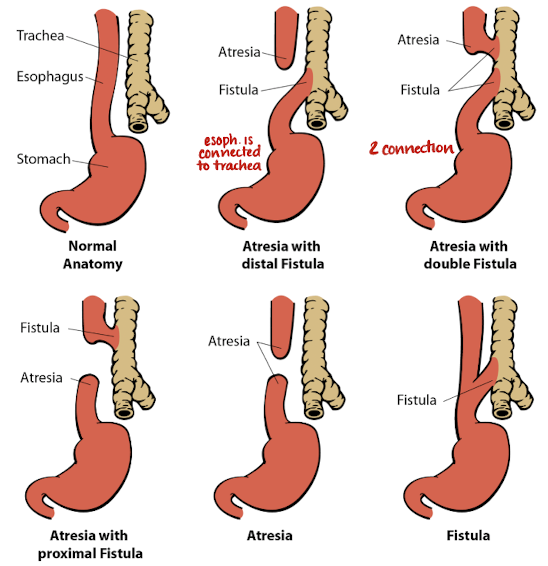
esophageal atresia (GI tract abnormality)
congenital absence/blockage of esophagus
esophagus fails to develop as a continuous passage
trachea and esophagus don’t separate → fistula
often occurs with tracheoesophageal fistula
associated with trisomy 18, 21
often occurs with VACTERL syndrome
what is VACTERL syndrome?
V: vertebral defects
A: anal atresia
C: cardiac anomalies
TE: tracheoesophageal fistula
R: renal anomalies
L: limb defects
SONO: esophageal atresia (GI tract abnormality)
stomach not visualized
polyhydramnios
IUGR appearance (sometimes)
not always seen prenatally because TE fistula results in normal size stomach and normal AFI
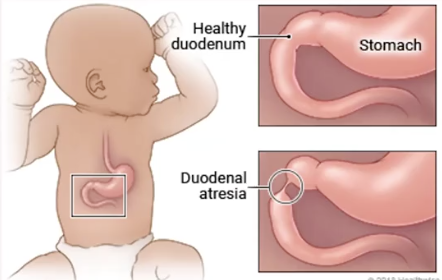
duodenal atresia (GI tract abnormality)
constricted duodenum located distal to ampulla of Vater
dilation of duodenum due to stenosis/atresia
amniotic fluid enters stomach and upper duodenum (dilation of both)
MC bowel obstruction in fetus
unknown cause
associated with T21 and cardiac anomalies
prognosis: excellent (if isolated)
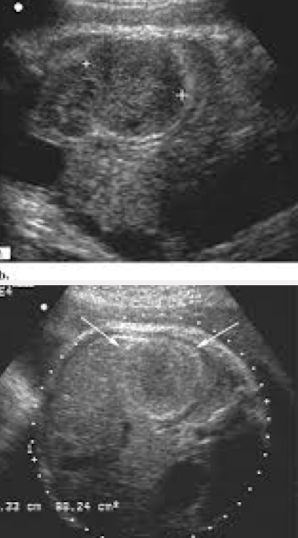
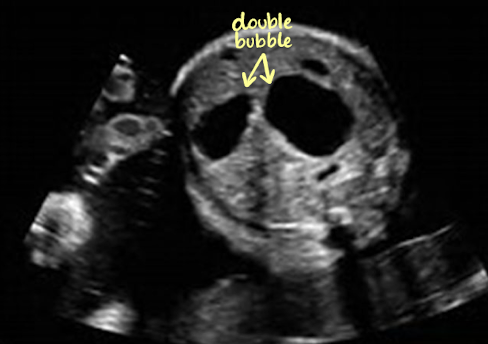
SONO: duodenal atresia (GI tract abnormality)
double bubble sign
dilated stomach and duodenum
polyhydramnios
AC will be large
small bowel atresia/obstruction (GI tract abnormality)
congenital narrowing or obstruction of small bowel
MC in proximal jejunum or distal ileum
general rule: the more distal the obstruction, the less severe the polyhydramnios
causes of fetal small-bowel obstruction

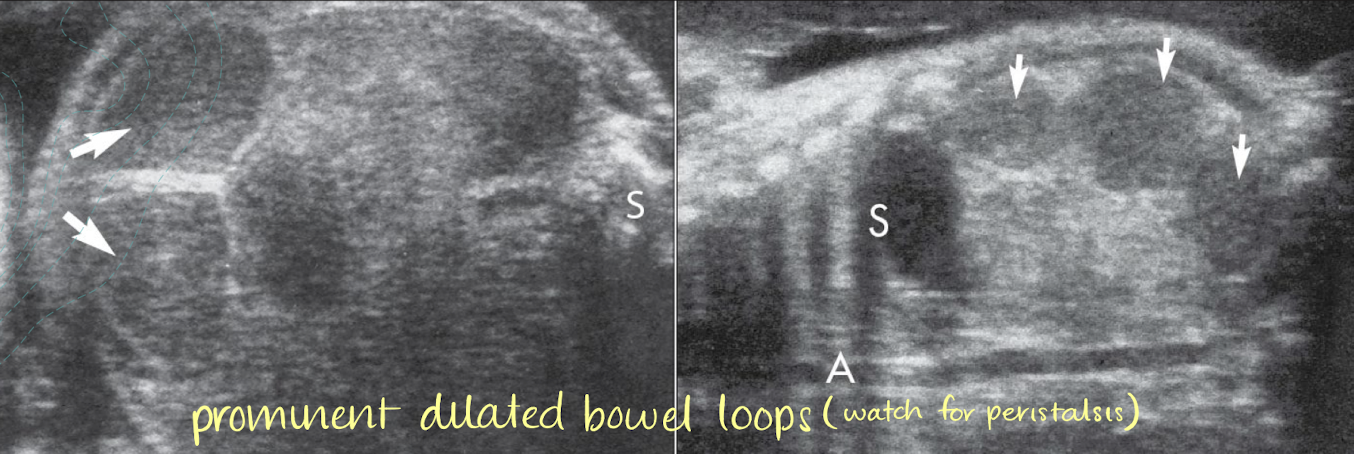
SONO: small bowel atresia/obstruction (GI tract abnormality)
dilated loops of bowel (cystic dilation)
persistently full stomach and dilated bowel loops
absence of peristalsis
pay attention to whether or not there’s movement
hydramnios

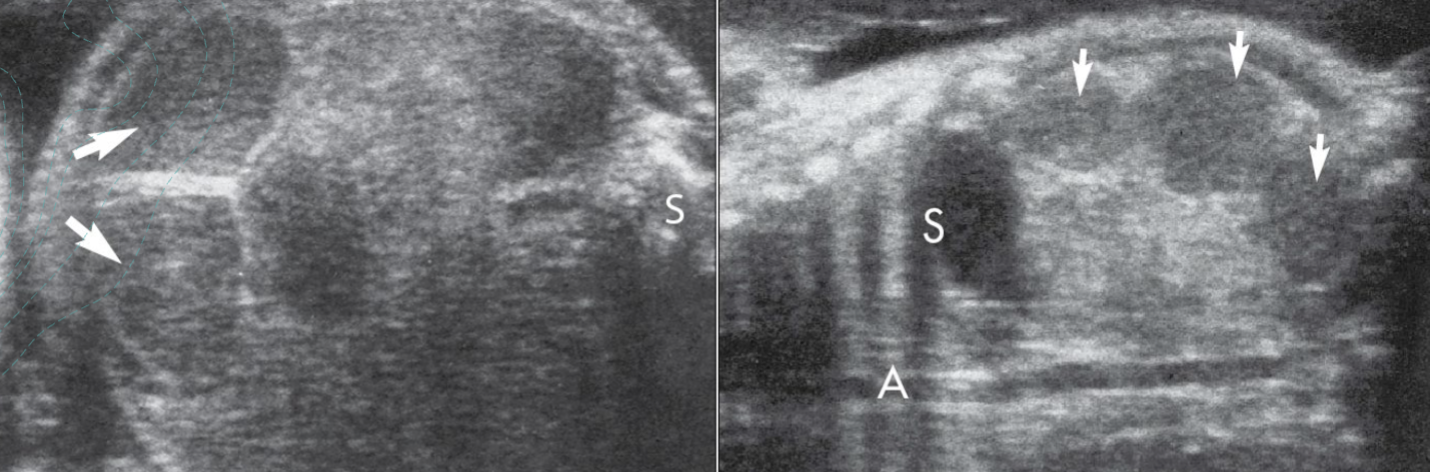
what do you see? pathology?
small bowel atresia/obstruction
anorectal atresia (GI tract abnormality)
complex disorder of bowel and genitourinary tract
imperforate anus (membrane covers anus, prohibiting expulsion of meconium—meconium cant get out)
maybe associated with VACTERL or caudal regression
poor prognosis
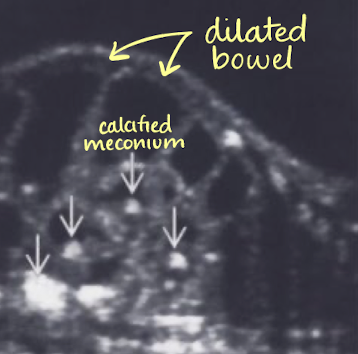
SONO: anorectal atresia (GI tract abnormality)
fluid-filled, dilated colon
calcified meconium
normal AFI
can be decreased if renal problems are present
meconium peritonitis
fetus has sterile chemical peritonitis secondary to in utero bowel perforation
hydramnios present in 65% of fetuses
SONO: meconium peritonitis
calcifications seen on peritoneal surfaces or in scrotum via processus vaginalis
ascitic fluid may be echogenic
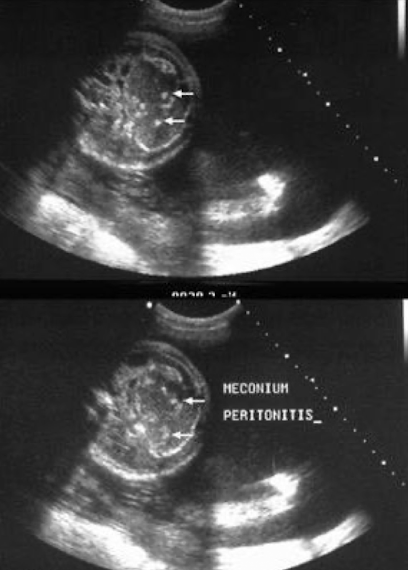
pathology?
meconium peritonitis
meconium ileus
small-bowel disorder with thick meconium in distal ileum
ileum dilates because of impacted meconium
most infants with this have cystic fibrosis
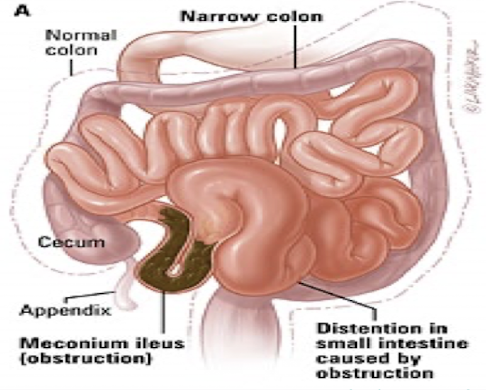
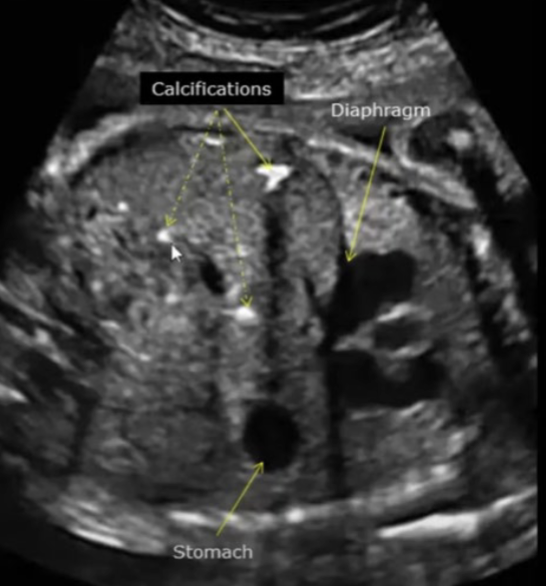
SONO: meconium ileus
usually apparent in 3rd trimester
dilation of small bowel
echogenic bowel
calcifications may be present
hyperechoic bowel
echogenicity similar to bone
typically compared to iliac crest
grade 1: mildly echogenic and typically diffuse
grade 2: moderately echogenic and typically focal
grade 3: very echogenic, similar to that of bone structures
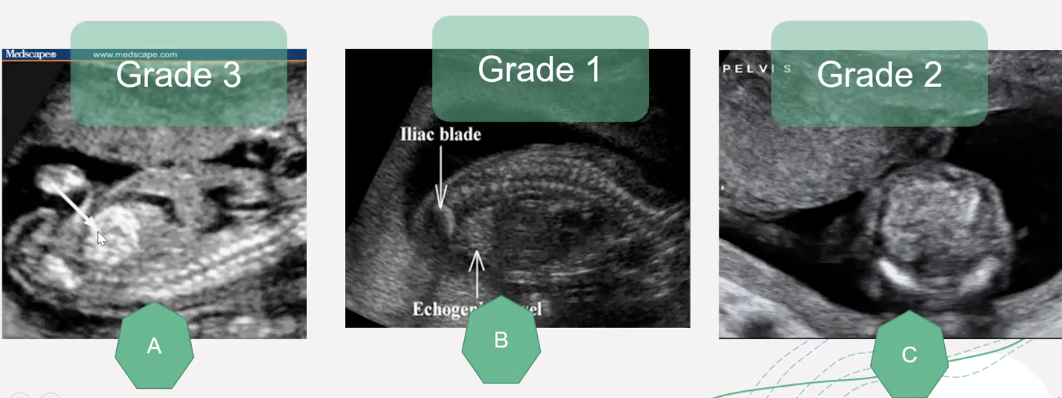
SONO: hyperechoic bowel
usually apparent in the 3rd trimester
dilation of small bowel
echogenic bowel
calcifications may be present
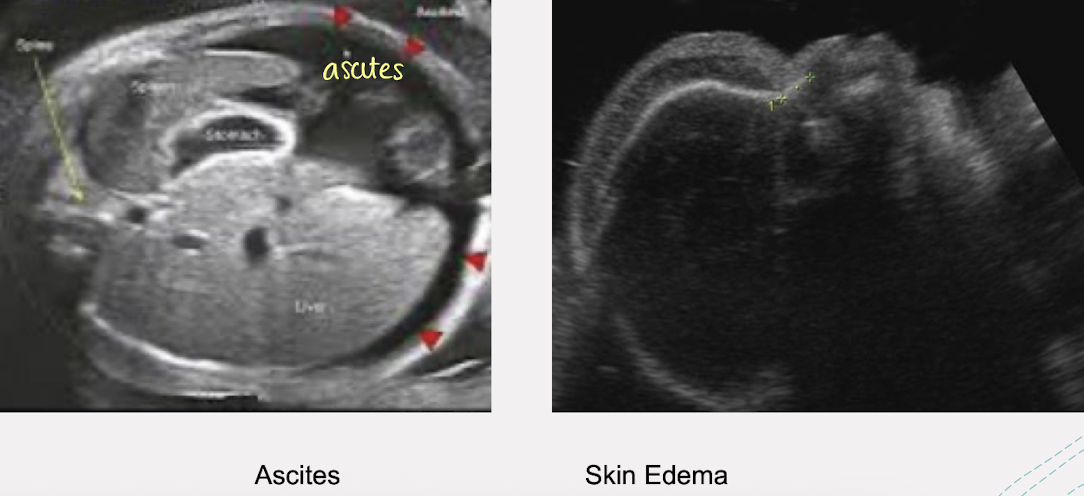
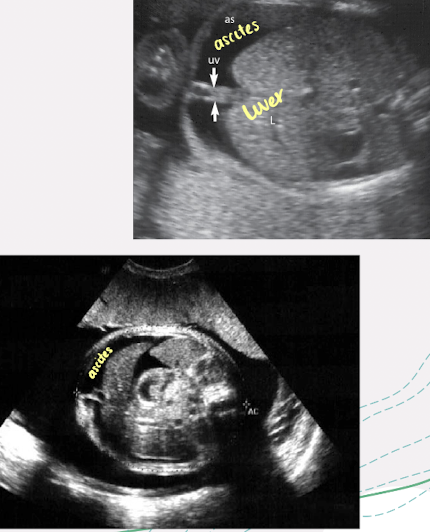
ascites
true ascites in fetal abdomen always abnormal
other conditions that may cause ascites to develop include bowel perforation or urinary ascites secondary to bladder rupture
SONO: ascites
fluid collects between 2 leaves of unfused omentum → cyst-like appearance in abdomen
ascitic fluid may be echogenic
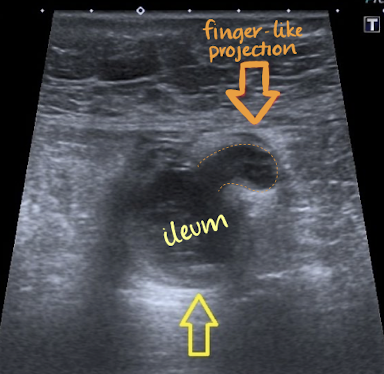
Meckel’s diverticulum
remnant of proximal part of yolk stalk that fails to degenerate and disappear during early fetal period
MC malformation of midgut
it is usually a small finger-like sac, about 5cm long, that projects from border of ileum
hydrops fetalis
life-threatening, severe condition
abnormal fluid builds up in two or more fetal compartments (e.g. abdomen, lungs, heart), causing total body swelling
usually diagnosed via prenatal ultrasound and treated by addressing the underlying cause
prognosis: poor
often fatal, with about 50% survival rate for live-born babies
high mortality rate before or shortly after birth
tx: in-utero interventions like…
blood transfusions
draining fluids
early delivery
causes of hydrops fetalis
non-immune hydrops (NIHF): MC type, caused by heart/lung problems, genetic abnormalities, or infections like Parvovirus B19
immune hydrops: occurs due to Rh blood incompatibility between mother and fetus, though this is less common due to RhoGAM treatments
S/S of hydrops fetalis
severe swelling
severe anemia
jaundice
heart failure
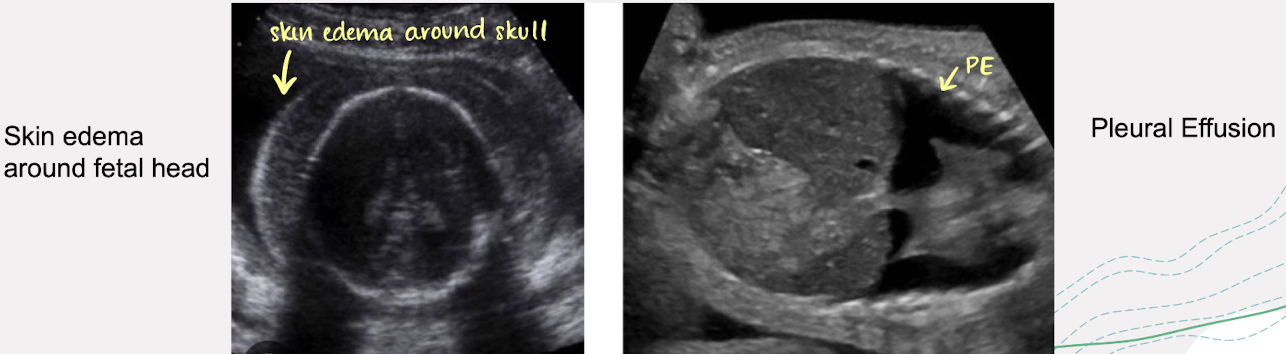
SONO: hydrops fetalis
fluid in abdomen (ascites)
around the lungs (pleural effusion)
around the heart (pericardial effusion)
polyhydramnios
fetal anasarca
rare, severe, often fatal form of hydrops fetalis
characterized by massive, subcutaneous edema (fluid accumulation) in fetus
end-stage condition featuring total body swelling, skin thickening, and often visceral effusions
intense. widespread swelling throughout the body—including head, limbs, torso
typically measuring more than 5mm in tissue thickness
associated with non-immune or immune hydrops fetalis (e.g. erythroblastosis fetalis)
prognosis: often indicated imminent fetal death
causes of fetal anasarca
driven by underlying factors such as…
severe fetal cardiovascular impairment
chromosomal abnormalities
infections
metabolic conditions
SONO: fetal anasarca
in severe cases, this condition can cause serious complications such as
polyhydramnios
placental edema