Opthalmic Infammatory and Dry Eye Conditions
1/9
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
10 Terms
Describe self-care measures for blepharitis and hordeolum/stye (inflammation of the eyelid conditions)
Blepharitis
Washing eyelids everyday with baby shampoo
Washing hair and eyebrows with an antibacterial soap to reduce bacterial growth
Warm compass
Wet clean washcloth with warm water and wring it out before use
Close eyes and put washcloth on eye for 1 minute
Can rewet wash cloth and do this again at a few minutes at a time
Benefit: loosens flakes, calms itching.burning, keeping oil gland open and functioning right reducing dry eyes symptom
Doctor:
antibiotic pills or ointments
Lubricating eye drops, steroid eye drops, and antibiotic eye drops
Chalazia
Warm compress:
Soak a clean washcloth in hot water and hold it to your eyelid for 10–15 minutes at a time, 3–5 times a day. Keep the cloth warm by soaking it in hot water often. For a chalazion, this warm compress helps the clogged oil gland to open and drain. You can help the gland clear itself by gently massaging around the area with your clean finger.
Antibiotics or Steroid Shots:
The PCP/ophthalmologist may prescribe an antibiotic for an infected stye. If the chalazion is very swollen, the ophthalmologist may give a steroid shot (cortisone) to reduce the swelling.
Surgery to drain the area
If the stye or chalazion affects vision or does not go away, it may need to be drained. This surgery is usually done in the doctor’s office using local anesthesia.
If a stye or chalazion keeps coming back time after time, an ophthalmologist may biopsy it. This is where a tiny piece of tissue is removed and studied. This helps the ophthalmologist check to see if there is a more serious eye problem.
Distinguish between the causes, defining features, and treatments for the three types of conjunctivitis
Infection or inflammation of white part of eye or the tissue on top (conjunctiva)
Bacterial conjunctivitis
Thick, mucus, sticky discharge that might have some yellow or green color
In the morning, lid are going to be matted shut and stuck shut with material
Duration: 5-7 days, immune system is self-limiting (mostly clear on own)
Presents only in one eye usually, but might spread to the other because it is contagious by touch
Treatment
immune system is self-limiting (mostly clear on own)
Antibacterial eye drops; some OTCs but not strong enough
Prescription are strong tho - shorten by a few days
Viral conjunctivitis
Watery discharge and weepy eyes with small amount of mucus
Swelling
Last 7-14 days
Virus can start in one eye and spread to other; spread acts similar to bacterial
Treatment
No antiviral meds that can help with this, so has to letting it clear on own
In some cases, in the doctor’s office there can be treatment done with Betadine which will kill active viruses on surface to quicken its course
Doctors may also prescribe steroids after the infection to bring down the inflammation on the cornea from some viral infections
Allergic conjunctivitis
A little weeping, not really any discharge; just reddening like the others
Red and itchy; bilateral
Seasonal allergies or animal allergies
Treatment
Antihistamines eye drop (OTC and prescription)
Contact lenses with antihistamines (Acuvue)
Ophthalmic Antihistamines and Ophthalmologic antihistamines/ Mast cell stabilizer -OTC
Non-prescription
Agents:
Pheniramine maleate
Antazoline phosphate
Effective alone, but most OTC products also include a decongestant
Common combinations:
Pheniramine + naphazoline
Antazoline + naphazoline
Belong to different antihistamine classes, but both:
Act as H₁-receptor antagonists
Indications:
Rapid relief of symptoms from:
Seasonal conjunctivitis
Atopic conjunctivitis
Combination therapy (antihistamine + decongestant):
More effective than either agent alone
FDA classification:
Considered less than effective due to limited clinical efficacy data

RX-Ophthalmic Antihistamines and Ophthalmologic antihistamines/ Mast cell stabilizer
Mechanism of Action:
Strong H₁-receptor antagonist → prevents acute histamine-mediated symptoms
Stabilizes mast cells → inhibits degranulation and release of histamine and other inflammatory mediators
Inhibits eosinophils → reduces late-phase allergic response
Advantages:
Relief within minutes
Effects last up to 12 hours with a single dose
No vasoconstrictor
No risk of vasoconstrictor overuse or rebound redness
Seek help
Pain, discomfort, long duration
If wear contact lenses- see doctor
Dry Eye Disease (DED) ManagementNonpharmacologic Therapy (Lifestyle Modifications)
Goal: Stabilize the tear film and decrease evaporation.
Environmental Controls: Avoid dry, dusty, or windy places. Reposition workstations away from direct heating and air conditioning vents. Use humidifiers to add ambient moisture.
Eye protection
Behavioral Changes: Avoid prolonged viewing of computer screens (which lowers blink rate). Wear eye protection (sunglasses or goggles) in windy outdoor environments.
Lid Hygiene: Utilize warm compresses and lid scrubs to improve lid function and provide anti-inflammatory benefits.
Adjuncts: Consider dietary omega-3 or flaxseed oil to support lid health.
Dry Eye Disease (DED) Management
Pharmacologic Therapy: Ocular Lubricants
Artificial tears vary primarily by viscosity, which dictates their clinical role and side-effect profile.
Low-Viscosity Drops:
Less contact time on the eye and higher susceptibility to tear dilution.
Used for mild cases of dry eye.
High-Viscosity Drops & Gels:
Prolonged ocular contact time and greater resistance to tear dilution.
Used for moderate-to-severe dry eye.
Gels offer an advantage over ointments because they do not disturb vision as significantly and are better tolerated.
Nonmedicated Ointments (e.g., Petrolatum):
Mainstay for minor ophthalmic disorders.
Reserved for severe cases or bedtime use due to their strong tendency to cause blurred vision
⚠ Clinical Pearl (Preservative-Free Formulations):
Formulations without preservatives are significantly less likely to irritate the ocular surface. However, because they lack antimicrobial protection, patients must be strictly counseled to discard nonpreserved products immediately after being opened.
Allergic Conjunctivitis & Ocular Decongestants
Nonprescription allergy drops frequently utilize decongestants (vasoconstrictors), antihistamines, or astringents.
Therapeutic Categories & Products
Decongestant-Only Drops: Naphazoline, Tetrahydrozoline, Oxymetazoline, Phenylephrine.
Antihistamine / Mast Cell Stabilizer: Ketotifen 0.025% (e.g., Zaditor, Alaway).
Antihistamine / Decongestant Combos: Pheniramine maleate + Naphazoline HCl (e.g., Naphcon A, Opcon-A).
Decongestant / Astringent Combos: Naphazoline + Zinc sulfate (e.g., Clear Eyes ACR). Zinc sulfate acts as an astringent to soothe surface irritation.
Critical Safety Warnings & Rationale
Risk Factor | Clinical Consequence & Mechanism | Patient Counseling / Action |
Rebound Hyperemia (Medicamentosa) | Excessive or long-term use causes severe rebound redness/congestion. Can appear within days, or as quickly as 8 hours. | Limit use to a maximum of 72 hours (3 days). Naphazoline/tetrahydrozoline have a lower risk than oxymetazoline/phenylephrine. |
Narrow-Angle Glaucoma | Decongestants can cause mild papillary dilation (mydriasis). In narrow angles, this can physically block fluid outflow and precipitate an acute angle-closure glaucoma crisis. | Strictly contraindicated. Patients with narrow anterior chamber angles must be counseled against using these products. |
Systemic Disease Risks | Systemic absorption of alpha-agonists can trigger adverse cardiovascular and endocrine events. | Use with extreme caution in patients with systemic hypertension, arteriosclerosis, cardiovascular disease, diabetes, or hyperthyroidism. |
Pregnancy | Potential for systemic vasoconstriction. | Pregnant women should use ocular decongestants sparingly, if at all. |
Pediatric Toxicity | Accidental oral ingestion of these solutions can cause severe coronary emergencies and death. | Keep strictly out of reach of children. Monitor use closely if therapy is indicated for a child. |
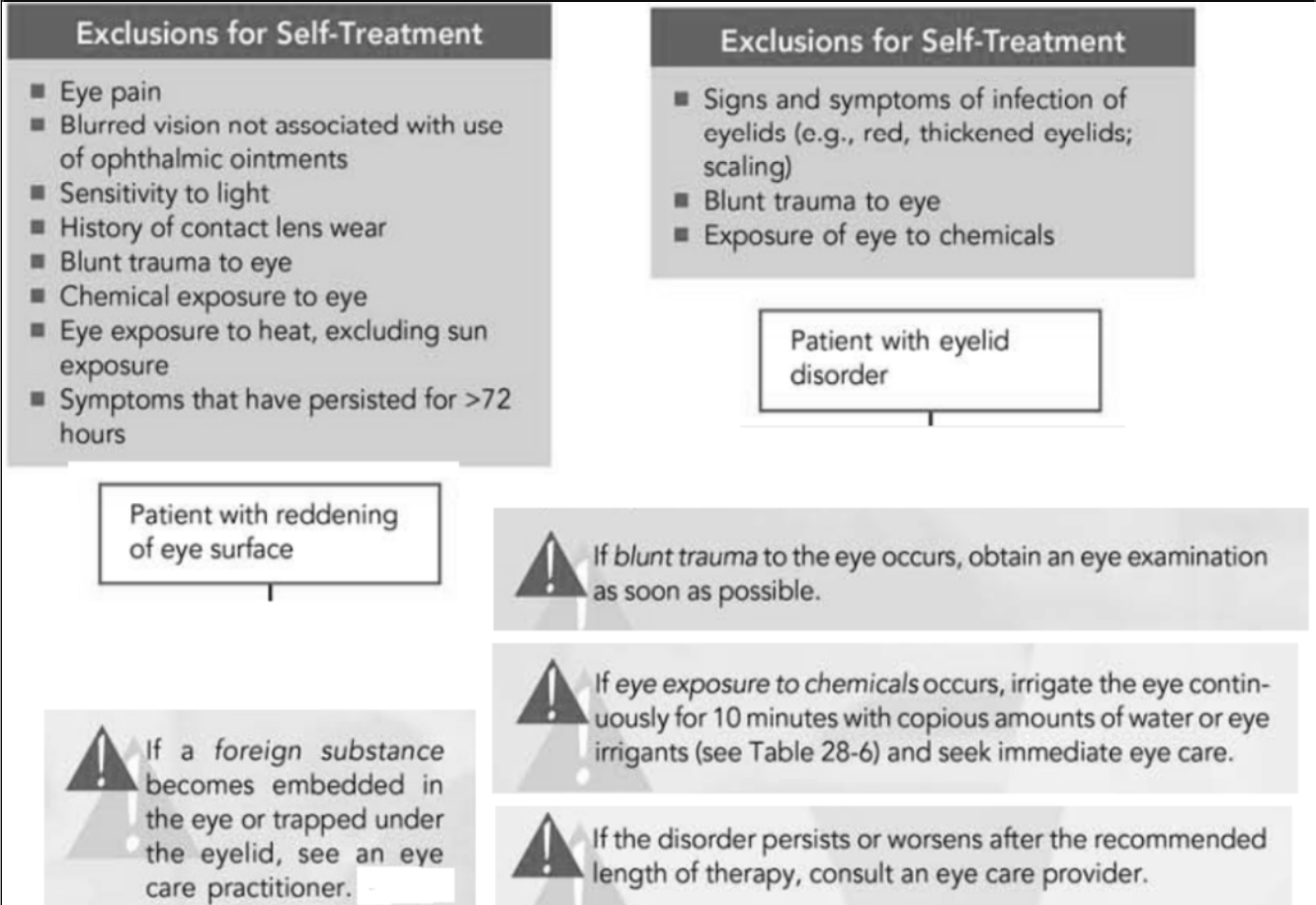
Recognize exclusions for self-treatment of common eye conditions presenting at a community pharmacy