Surg Med - Wound Care - Exam 2
1/61
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
62 Terms
Inflammatory Wound Healing
Days 1-6
Chemoattractant release
Phagocytosis
Removal of foreign bodies and bacteria
Proliferative Wound Healing
Days 4-21
Fibroblast proliferation
Provisional ECM synthesis
Granulation tissue formation
Re-epithelialization
Remodeling Wound Healing
3 weeks to 2 years
Type I collagen accumulation
Crosslinking of collagen
Scar tissue formation
Increase in tensile strength
Optimizing Scar Quality
Tension reduction
Layered closure
Moist wound environment
Avoid infection and ischemia
Use appropriate dressings and sun protection
Optimize nutrition and systemic health
Massage after healing (remodeling phase)
Optimal Healing - Necessities
Well vascularized wound bed
Free of devitalized tissue
Minimal bacterial burden
Controlled exudate, moist environment
Healthy granulation tissue
Wound Dressings
Eliminate dead space
Control exudate
Prevent bacterial growth
Ensure proper fluid balance
Demonstrate cost-efficiency
Manageable for the patient/support staff
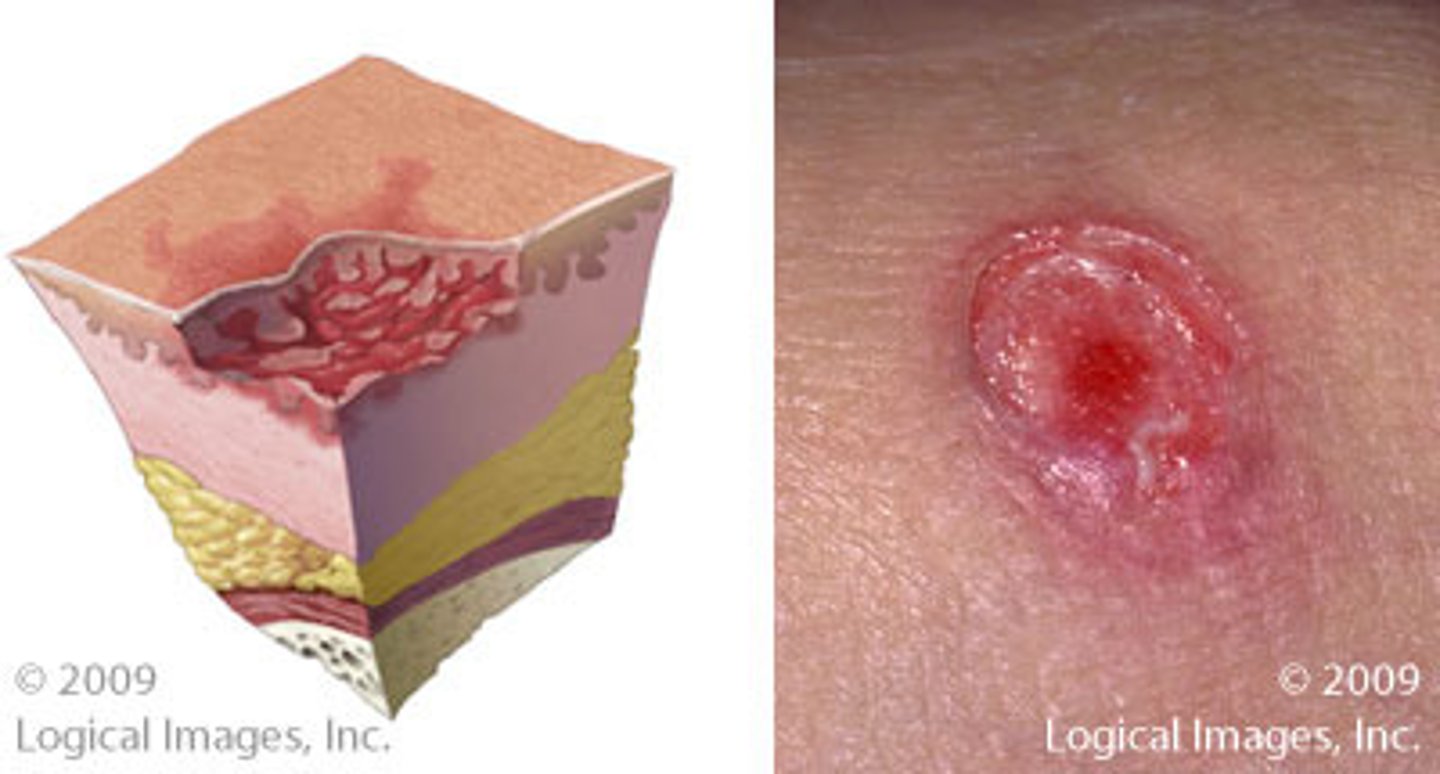
Partial Thickness Wound
Loss of epidermis +/- some dermis
Stage 2 pressure ulcer, blister, skin tear
No slough – heal through epithelialization rather than granulation tissue
Less scarring
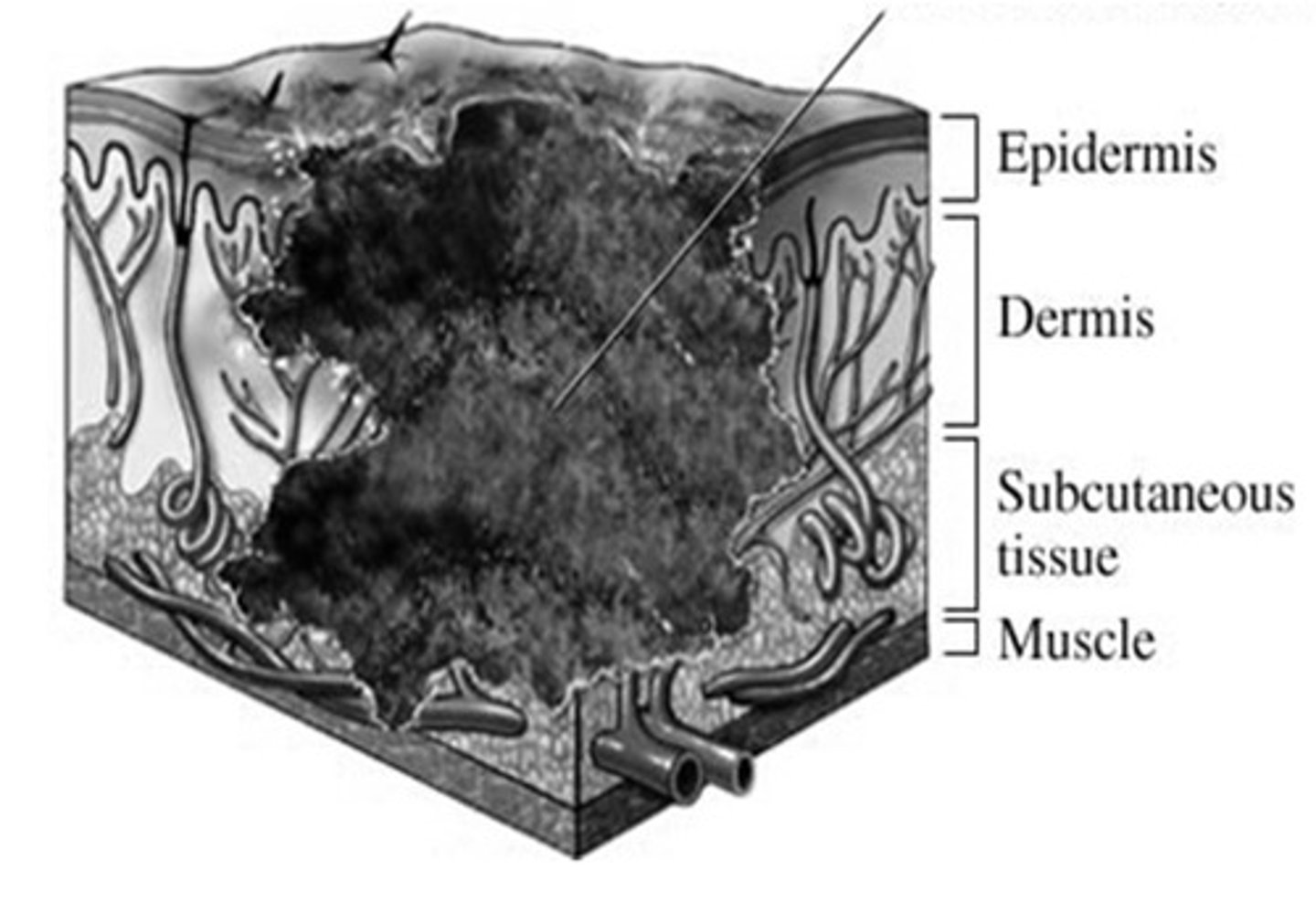
Full Thickness Wound
Loss of epidermis, dermis, and subcutaneous tissue and/or deeper
Requires granulation/contraction
Higher infection risk
Often needs advanced closure/grafting
Local Factors - Impaired Wound Healing
Infection/Debris/Foreign Body
Tension
Mechanical stress/pressure
Ischemia
Necrotic tissue
Systemic Factors - Impaired Wound Healing
Diabetes
Smoking/nicotine
Malnutrition
Steroids/Immunosuppression
Obesity
Vascular Disease
Renal failure
PostOp Wound Care - Assessment
Is the wound intact?
Drainage?
Erythema?
Pain out of proportion?
Fever?
Fluctuance?
Necrosis?
PostOp Wound Care - Dressing
Keep clean
Moist, but not macerated
Avoid unnecessary dressing changes
24-48 hours
Immediate postop dressing often left intact _______
Wound Dehiscence
Partial or complete disruption of any or all layers of the operative wound
Wound Dehiscence Local Factors
Inadequate closure - easiest modifiable factor
Fascial layers are strength layers!
Increased pressure
Deficient wound healing
Anything that disrupts healing - i.e., seromas, hematomas,
5-8d
wound dehiscence most commonly occurs _______ post-op (when the strength of the healing tissue is at a minimum)
Venous Stasis Ulcer
Caused by chronic venous hypertension and inflammation
Appearance: shallow, irregular ulcer with moderate to heavy exudate, warm, painful, pruritic

Venous Stasis Ulcer - Associations
hemosiderin staining
stasis dermatitis
"champagne leg"
lipodermatosclerosis
Venous Stasis Pathophys
Valve failure → venous reflex → tissue congestion + hypoxia
Leads to inflammation and ulceration
Worsened by protein-rich fluid buildup and trauma
Venous Stasis Ulcer Tx
Control Edema
Use dressings that wick moisture away from the wound and break down wound debris
Pneumatic (lymphedema) compression pumps
Investigate for infection
Optimize comorbid conditions
weight-bearing
diabetic ulcers are most common on _________ surfaces
Diabetic Ulcers
may be small at the surface but have large subcutaneous dead space and possible bone involvement
Higher risk for osteomyelitis, thus, amputation
X-ray – not positive in early disease
Follow up with MRI or CT if wound has been present >4 weeks
WG1
superficial ulcer
WG2
deep structure involvement WITHOUT infection
WG3
deep structure involvement with infection: abscess, osteomyelitis
WG3/4
deep structure invovlement/abscess/osteomyelitis and eschar
Diabetic Ulcer Tx
Blood sugar control is essential (120-140 mg/dL)
Debride callus
Often complicated by small vessels disease
First 4 weeks are critical
Actively reassess during this time – don’t delay care
Consider hyperbaric O2 therapy for Wagner grade 3-4
Total Contact Cast → Gold Standard for offloading DFUs
Stage 1 Decubitus Ulcer
Non-blanching erythema of intact skin
Edema
Lightly Pigmented
Deeply Pigmented
Transparent film for protection
Stage 2 Decubitus Ulcer
Partial-thickness skin loss exposing the dermis
Semi-occlusive (transparent film) or occlusive dressing (hydrocolloid or hydrogel) so that any necrotic tissue that is present is digested by enzymes normally present in wound base
Stage 3 Decubitus Ulcer
Full-thickness skin loss
Wet-to-Dry dressings for light debridement; generally require debridement and possibly treatment of infection; necrotic tissue promotes bacterial growth and impairs wound healing
Stage 4 Decubitus Ulcer
Full-thickness skin loss w/ exposed or palpable fascia, muscle, tendon, ligament, cartilage, or bone
Wet-to-Dry dressings for light debridement; generally require debridement and possibly treatment of infection; necrotic tissue promotes bacterial growth and impairs wound healing
Deep Tissue Injury
Intact or Non-Intact skin with persistent non-blanchable deep red or purple discoloration or bruising
Unstageable Decubitus Ulcer
Full-thickness skin and tissue loss, but damage cannot be confirmed due to slough or eschar
Decubitus Ulcer Tx
Reduce Pressure, but prevent new injury
Control infection
Improve nutritional status
General principles - debridement and dressings/wound packing
PM&R referral
Film Dressings
Dry to minimally exudative wounds
Allows oxygen in, moisture out, and visual inspection of wound
Tegaderm
Hydrocolloids
For low to moderate exudate
Occlusive, retains moisture, promotes autolytic debridement
Hydrogels
Used on dry/dessicated wound to add moisture to wound bed
Options: No additives, Silver impregnated, Collagen impregnated
Alginates
Reacts with wound exudate and forms a hydrophilic gel → can cause maceration due to heavy drainage
Stimulate macrophage activity +/- silver for antimicrobial properties
Can be a very soft dressing choice for tender wounds
minimal exudate
do not use alginates with wounds that have what?
Foams
For moderate to high exudate
Gentle on surrounding skin
Absorptive dressings/powders
For heavy to copious drainage/significant exudate
Also, when dressing change frequency must be reduced
Nonadherent Gauze
Minimize trauma during removal
Lightly exudative wound
topical abx
Not universally recommended for all wounds – overuse can be harmful
Can be used for:
Mild local wound infxns (superficial abrasions, minor lacs)
Prevention of infection in clean, superficial wounds
Colonized wounds at risk for infection, especially in high-risk patients (e.g., diabetics)
Contaminated surgical wounds or wounds healing by secondary intention
Bacitracin
Gram positive (especially staph)
Sufficient for most minor wounds
Neomycin
Gram negative
Common allergen - delayed hypersensitivity reactions
Polymyxin B
Gram negative
Often combined with bacitracin/neomycin
Mupirocin
MRSA, Gram positive
Good for infected/colonized wounds
Silver Sulfadiazine
Broad spectrum (esp burns)
Use limited to burns and high-risk wounds
enzyme debriding agents
Topical medications that chemically break down necrotic or devitalized tissue to help clean a wound bed
enzyme debriding agents - purpose
Remove nonviable tissue
Reduce bacterial burden
Promote granulation tissue formation
Support progression toward healing
Collagenase
Breaks down collagen in necrotic tissue
Selectively digests devitalized tissue
Preserved more healthy tissue than sharp debridement
Enzyme Debriding Agents - Indications
Chronic wounds with necrotic tissue
Pressure injuries
Diabetic ulcers
Patients who are poor surgical candidates
Patients unable to tolerate sharp debridement
maggot therapy
Form of biodebridement using live, sterile larvae to clean, non-healing wounds
Helps when sharp debridement is CI
CI with exposed blood vessels/bleeding risk or pyoderma gangrenosum
Growth Factors
Biologically active proteins that stimulate cell migration, proliferation, and tissue regeneration
Helps "jump start" healing cascade in a stalled wound
Clean, non-infected wounds (infxn inhibits effectiveness)
Patients with good offloading, perfusion, and glucose control
Regranex
Platelet Derived Growth Factor (PDGF)
Used for diabetic foot ulcers, full thickness, lower extremity
Apply daily, requires moist wound bed
Apligraf, Dermagraft
Contain multiple growth factors via bioengineered skin substitutes
Used for chronic venous ulcers, diabetic foot ulcers
Costly, used in refractory cases
Platelet-Rich Plasma (PRP)
Autologous platelets
Off-label use in wound and surgical healing
Still being studied; mixed results
Bioengineered Skin Substitutes
Bottom layer (dermal) is made of a fibrous protein material (collagen) from cows and a substance made from shark cartilage
Top layer (epidermal) is made of silicone
Allows blood vessels and other cells to grow a new layer of skin while the collagen is absorbed into the body
Silicone layer helps close the wound and prevent fluid loss
Negative Pressure Wound Therapy
Applies continuous negative pressure (commonly ~125 mmHg) to the wound bed
Promotes granulation tissue formation and angiogenesis
Removes exudate and decreases wound/periwound edema
Assists with wound contraction and may decrease wound healing time
Hyperbaric Oxygen Therapy
Patient lies in hyperbaric chamber set at 2.0-2.4 ATMS and 100% O2 concentration for approx 2 hours
First 20 minutes spent bringing the patient to desired pressure (2x atmospheric pressure)
Two 5 min normal air breaks
Usually requires daily treatment for at least 20 treatments
Electrical Stimulation
Mimics natural bio-electric system of healing
Chronic wounds with stalled healing despite standards of care
CI in malignancy, osteomyelitis, presence of electrical implants, over carotid sinus, or pregnant uterus
Electrical Stimulation - MOA
Increased blood flow and tissue perfusion
Stimulation of fibroblast and epithelial cell migration
Promotion of angiogenesis
Inhibition of bacterial growth
Enhanced collagen synthesis and granulation tissue formation