Rest of Clinical Skills Material
1/137
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
138 Terms
used to evacuate gastric contents, may be used for feeding
Nasogastric
(nasoduodenal, nasojejunal) intended for feeding
Nasoenteric
usually placed endoscopically, nose to common bile duct
Nasobiliary tubes
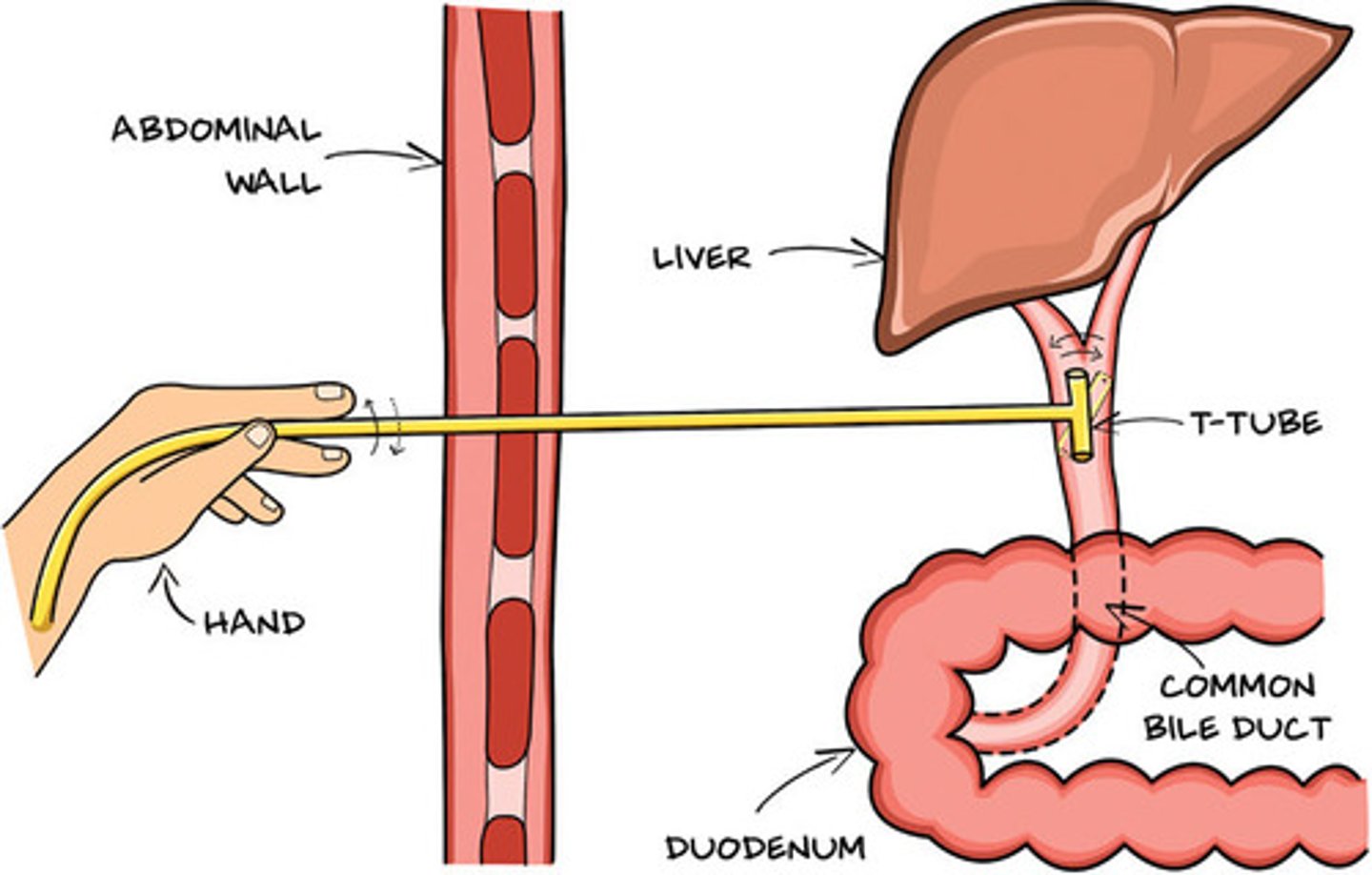
placed endoscopically within the common bile duct for the purpose of drainage, allows for gravity drainage out skin
T-tubes
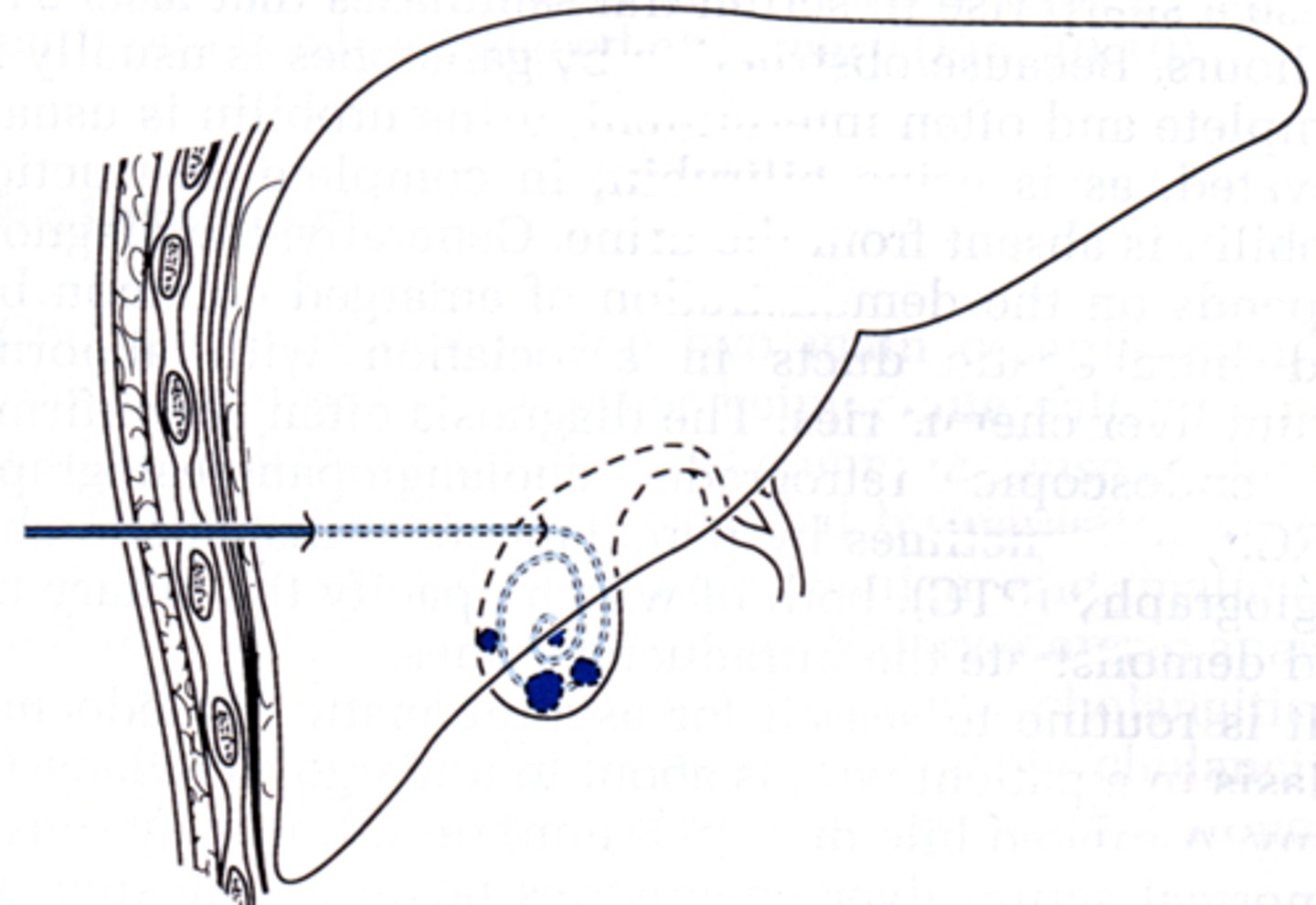
needle is threaded percutaneously into the gallbladder and used to decompress the organ, thus releasing pressure and relieving symptoms, gravity drainage
Placed by Interventional Radiology
Percutaneous Cholecystostomy
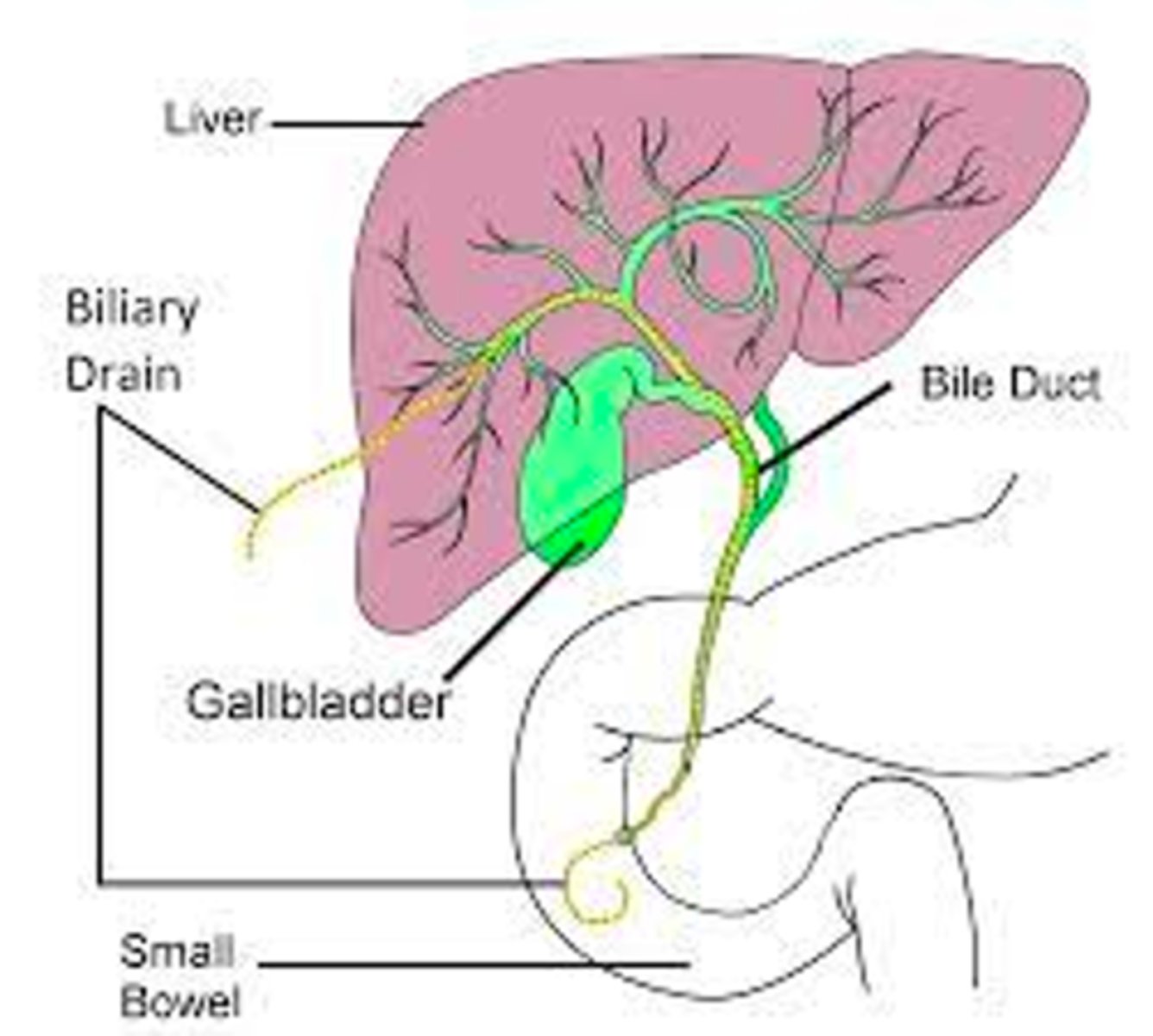
a minimally invasive, image-guided procedure (using X-ray or ultrasound) that places a thin tube (catheter) through the skin and into the liver to relieve bile duct blockages from liver to duodenum
Internal & External Drain
Placed by Interventional Radiology
Percutaneous Biliary Drain
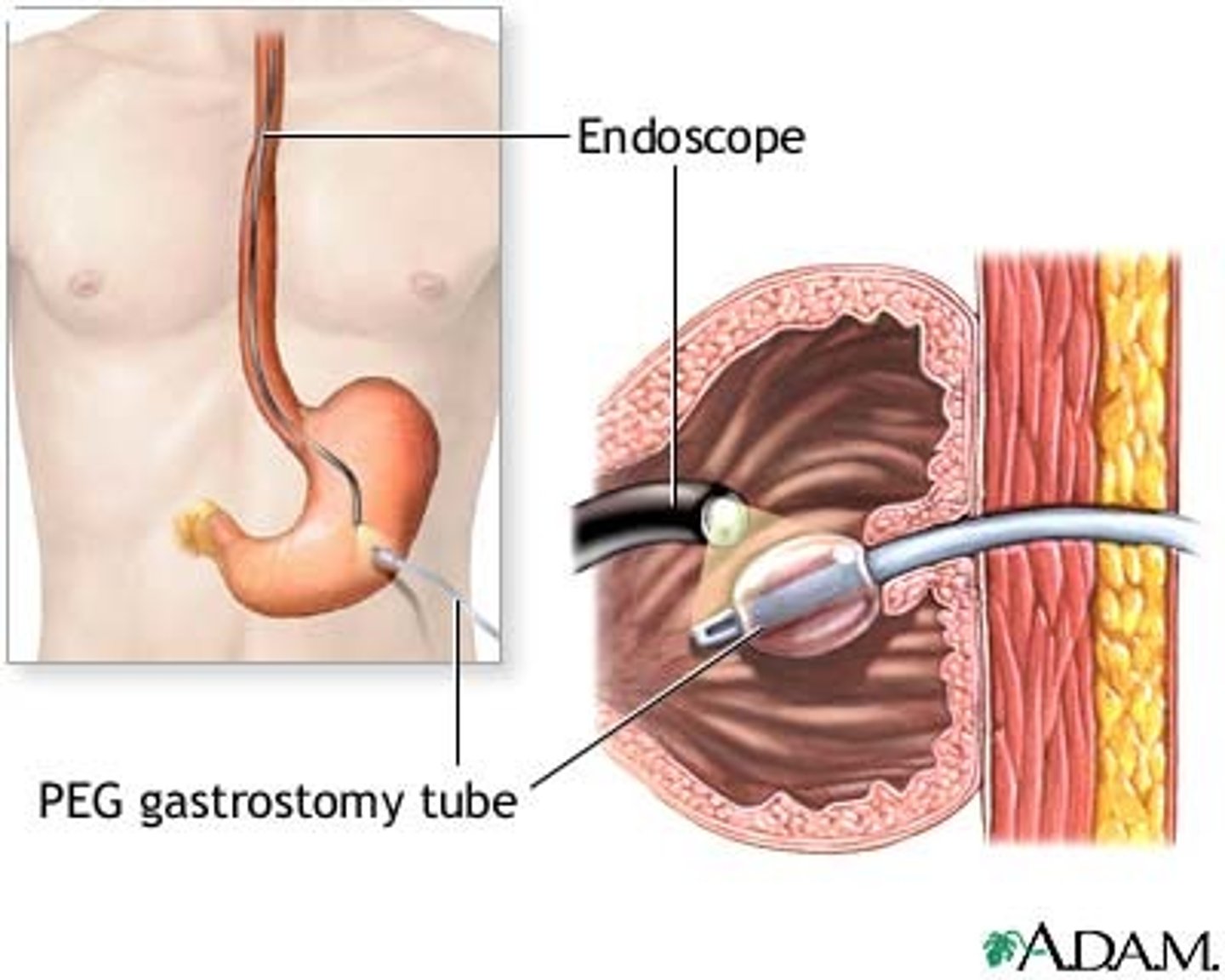
can be placed by surgery, by endoscopy, by radiology
Gastrostomy
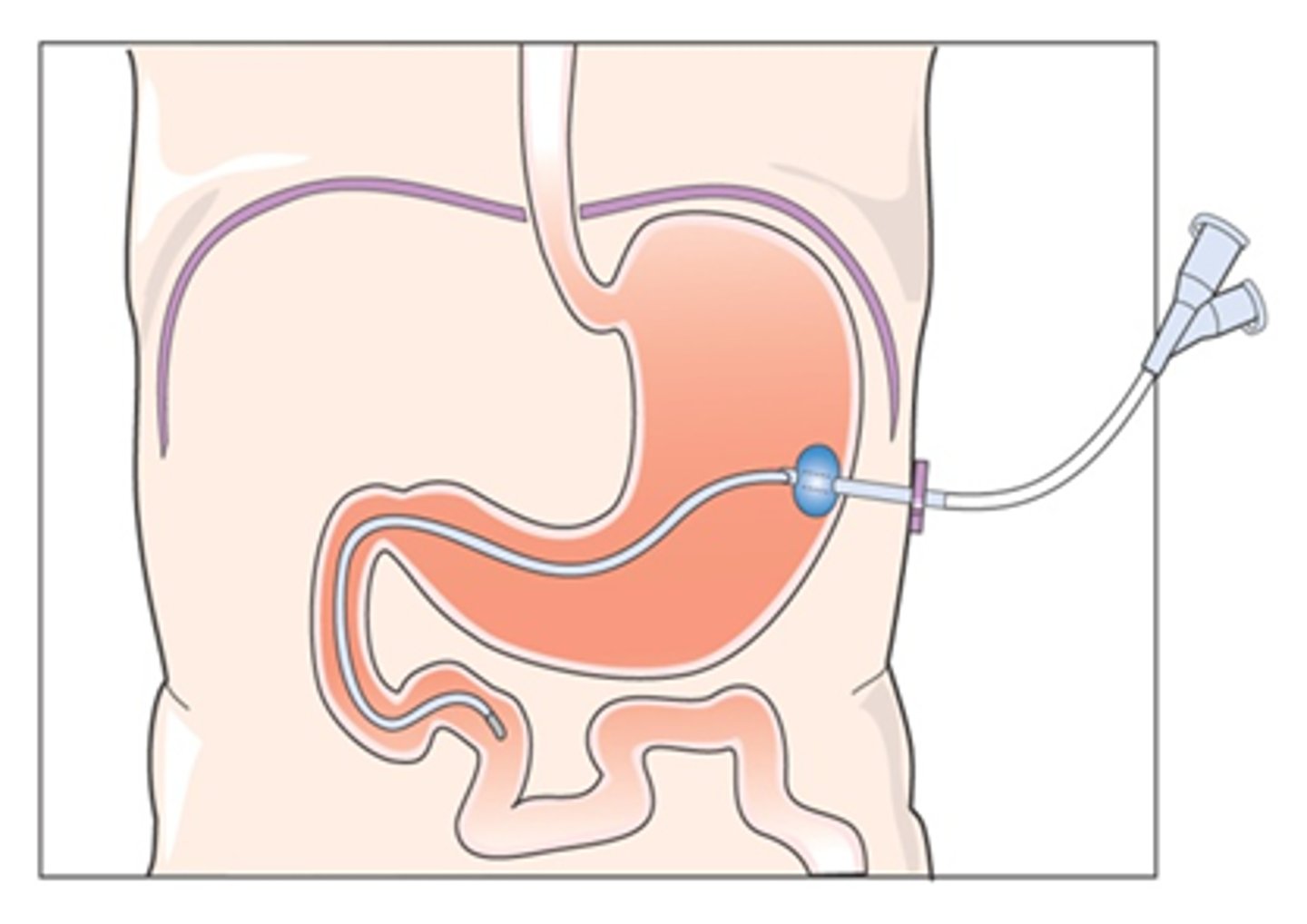
can be placed surgically or endoscopically, long term nutrition
Jejunostomy
•placed for pneumothorax, hemothorax, effusion.
•Often initially set to suction -20 mmHg
•May also have water seal to prevent air from entering pleural space
•Allows drainage of air / fluid
Chest tubes
short term tube for breathing
Endotracheal tubes
long term tube for breathing
Tracheostomy tubes
creation of an artificial opening into the kidney, drain urine directly from kidney, placed by IR
Nephrostomy
a procedure that places a thin, flexible tube through the skin (percutaneously) on the back, through the kidney, down the ureter, and into the bladder to drain urine, often bypassing blockage (stricture), placed by IR
can drain urine internally and externally (cap external portion/nephrostomy portion if patient is doing well)
Nephroureterostomy
how do you know if a patient has a nephrostomy or nephroureterostomy?
imaging
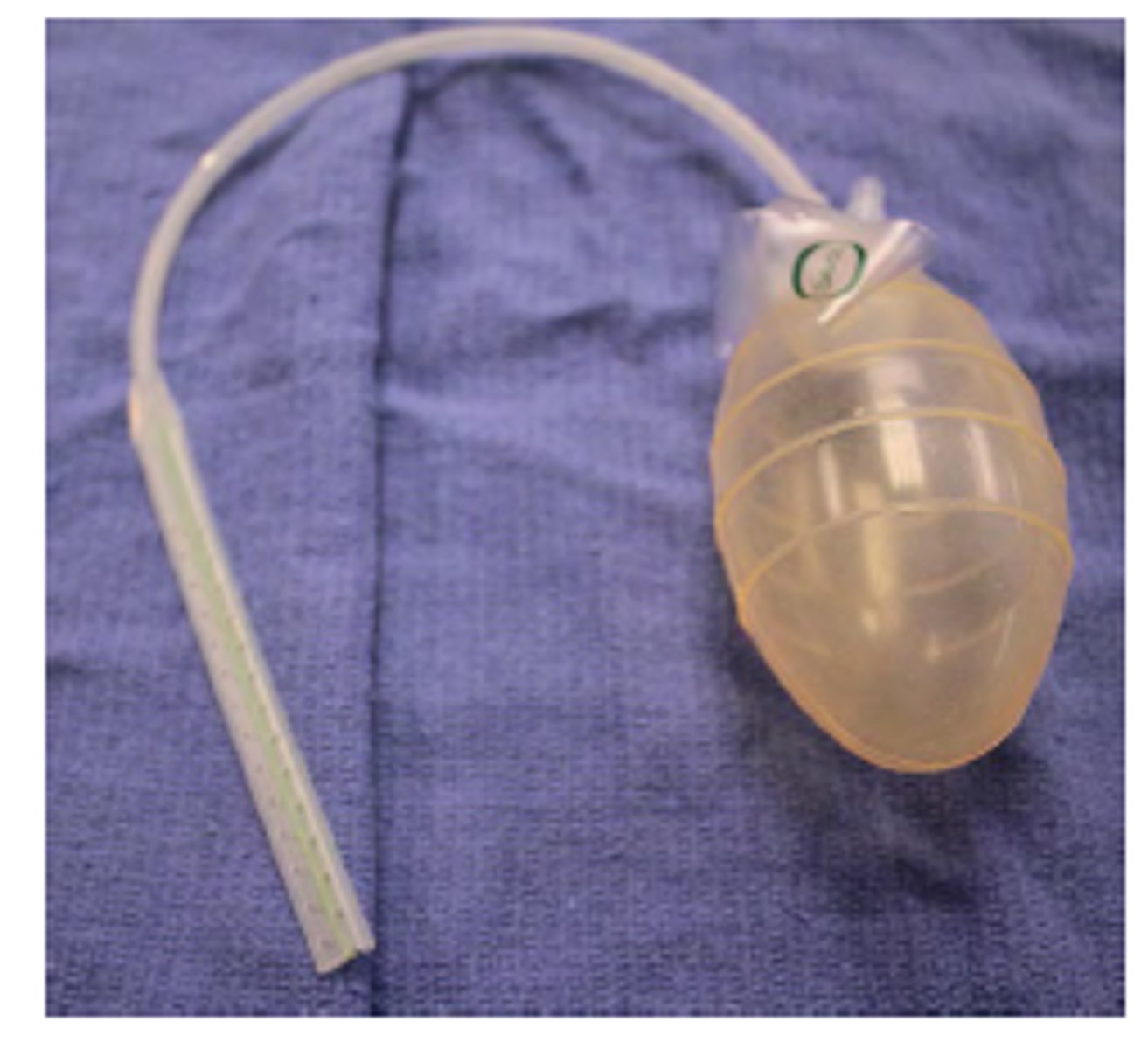
hollow bulb-like device used to collect drainage, pop open valve and squeeze then replace cap to generate vaccuum
need flushed frequently
Jackson Pratt (JP) Drain
aka Grenade Bulb Drain

a closed drainage system in which a soft drain is attached to a springlike suction device, hold more volume than JP, empty fluid and compress it down to initiate vacuum
Hemovac Drain
very large, placed to continuous suctions for when drainage is expected to be thick
Sump Suction Drains
this type of tube is not flushed or encouraged with vacuum
passive (used in very specific scenarios)
soft, flexible, latex or silicone tube used in surgery to passively remove fluids from a wound or surgical site
maintain a pathway for fluid flow
Passive tubes (Penrose)
orders for surgical drains
•Flushing
•Stripping the drain - when there is fibrous material in the drain
•Output
•Closed suction (correct method), wall suction, or to gravity (foley)
pinch proximal drain and pull down on drain to remove fibrous build up
stripping a drain
ways drains are sunctioned
closed suction
wall suction
gravity
when is a drain removed?
- decreased output over time
- confirmed volume depleted on imaging
orders for Immediate Post Op Care
vital signs, fluids, pain management, drain care, medications (including pain management), labs, imaging
for inpatients, post op check every ______ hours
4-6
Position in bed & mobilization post op
turning, upright position, stockings, allowing for drainage, knee & heel support for comfort
post op DVT prophylaxis
medication, stockings, movement
•Within _____ after surgical wound is closed by primary intention space fills with inflammatory exudate, epidermal cells begin to divide and migrate across wound surface, by ___ hours deeper structures are sealed off from external environment. Sterile dressing offer protection at this time.
hours; 48
wound care requires aseptic technique for a minimum of ___ hours
24
Remove dry dressings in _____ days, if wet remove _____
3-4, earlier
Vacuum dressings need to be replaced in ________hours, pain management at dressing changes
24-72 hours
Sutures and staples often remain in place for _____ days depending on location and healing
5-14
Adhesives will fall off in time, avoid ______.
lotion
Need to get Dermabond off?
Acetone, Vaseline, or triple antibiotic ointment will work
cause of surgical wound dehiscencec
Many causes including sutures being too tight, or infection
_______________ from wound is a sign of acute fascial dehiscence.
Spontaneous discharge of serous fluid
what to do if Dehiscence of abdominal fascia and evisceration
Cover organs with sterile towels soaked in saline solution, OR immediately
Parenteral opioids
morphine, meperidine, hydromorphone, etc
Nonopioid parenteral analgesics
NSAIDS
Oral analgesics
acetaminophen with codeine, hydrocodone with acetaminophen, oxycodone with acetaminophen
Release of catecholamines and other stress hormones by postoperative pain causes vasospasm and hypertension, which may in turn lead to complications such as
stroke, myocardial infarction, and bleeding
The patient may be reluctant to breathe deeply, promoting
atelectasis
ways to prevent post op atelectasis
•Smoking cessation 8 weeks preop
•Incentive spirometry, coughing
•Adequate pain management
•Early mobilization
T/F post op fever is always a sign of complication
False
High Temperature about _____ may initiate investigation
38.3° C
Postop pulmonary edema is caused by_______________
high hydrostatic pressures
In the absence of deranged cardiac function or fluid overload, the development of pulmonary edema should be regarded as evidence for ______.
sepsis
Early postoperative respiratory failure develops most commonly in patients with
major operations, severe trauma, and preexisting lung disease
Late postoperative respiratory failure (develops beyond 48 hours post op) is usually triggered by:
pulmonary embolism, abdominal distension, or opioid overdose
respiratory failure:
_____ bpm
tidal volume < _____
PCO2 > ________
PO2 < _______
____ cardiac output
25-30
4ml/kg
45mmHg
60mmHg
low
what may cause need for increased post-op fluids?
extra needs resulting from systemic factors (fever, burns, loss during surgery), loss from drains, tissue edema / ileus (third space losses).
maintenance fluids calculation
weight in kg x 30 in 24 hours period
rule of thumb: 2000 - 2500 ml of 5% dextrose in normal saline or lactated ringer solution daily
(no potassium in first 24 hours)
•After operations on the stomach and upper intestine, propulsive activity can be disorganized for ____ days.
3-4
Anemic patients with recurrent, IgA deficiency, severe allergic reactions benefit from _______ RBCs
washed
•Indicated for massive blood loss with pronounced hypovolemia
Whole blood 450-500 mL of donor blood, RBC, plasma, clotting factors, anticoagulant
Indicated for patients experiencing recurrent febrile nonhemolytic transfusion reactions to RBC or platelets or prophylactically in patients with long term transufion needs
Leukocyte-Reduced Red Blood Cells
•indicated for patients who are at risk for transfusion associated graft versus host disease.
Irradiated Red Blood Cells
Indicated for management of active bleeding in thrombocytopenic patients. Or for patients with platelet dysfunction
Platelets
Good for patients with deficiencies of multiple clotting factors. Albumin, and fibrinogen
FFP
ndicated for the correction of hypofibrinogenemia in dilutional coagulopathy and the hypofibrinogenemia/dysfibrinogenemias of liver disease and DIC.
Cryoprecipitate
are indicated in severely neutropenic patients with bacterial sepsis who have not responded to optimum antibiotic therapy after 48-72 hours
Granulocyte Transfusions
autosomal dominants Disruption of intracellular calcium metabolism
Tachycardia, cyanosis, muscle rigidity.
•Body temperature may rise 1-2 degrees every 5 minutes, may not present for up to 36 hours after exposure to triggering agent
malignant hyperthermia
cyanosis, symptoms of hypoxemia that does not improve with supplemental oxygen, discoloration of blood (dark red, chocolate, or brownish to blue) that does not resolve upon oxygenation
Methemoglobinemia
what is the treatment for malignant hyperthermia
dantrolene
causes of Methemoglobinemia
•An infant fed formula made with well water that was not tested for methemoglobin levels
•A member of the military who is administered malarial prophylaxis.
•An individual undergoing endoscopy or bronchoscopy who is treated with a topical anesthetic agent prior to the procedure
what is the treatment for methemoglobinemia?
methylene blue
what are the indications for doing a trauma-oriented eye exam?
- potential eye injury
- suspected scratch or abrasion
- suspected FB
- acute visual disturbance
what are the contraindications to performing a trauma-oriented eye exam?
- ruptured globe
- eyelid laceration (vertical)
if FB is not removed in timely manner, this complication may result
infection or ocular necrosis
when should you suspect ruptured globe?
high velocity injury
what should you do if you suspect a ruptured globe?
- NO topical agents on eye
- cover both eyes with Fox shield
- immediate referral to ophthalmologist
what should you do if someone comes in for a caustic splash exposure to the eye?
- begin flushing with lactated ringers (manually or Morgan lens) immediately and exam later
- check pH PRN until neutral
duration of flushing caustic splash exposure
mild irritant?
most other?
penetrating corrosive?
5 minutes
20 minutes
60 minutes
contact lens users are at high risk for ________ infections
pseudomonas
what are the complications to doing a trauma eye exam?
- increased pain
- N/V
- photophobia
what imaging is preferred for the eye?
plain films/CT
what is a topical anesthetic that can be used for the eye?
proparacaine 0.5%
what devices/tools can be used to remove a foreign body from the eye?
- eye or corneal spud
- 25 gauge needle
- flush
- moistened cotton swab
anesthesia is necessary!
the application of dye to the surface of the eye via eye drops or a strip applicator
with black or cobalt blue light, can help you see FB or abrasion
fluorescein staining
after applying fluorescein stain, its important to
inspect lower eyelid while patient looks up, upper eye lid by everting, and sweep the recesses of the upper conjunctival fornices
patient positioning during trumatic eye exam
patient presses head on forehead strap and chin rest, anchor clinician hand against pt face
from which direction does clinician approach patient eye?
from side and inferiorly (minimizes anxiety and blinking)
removal of rust ring
corneal bur
after removing FB
flush generously
check visual acuity
indicates corneal penetration injury with oozing aqueous humor
"dark waterfall"
seidel sign
T/F topical anesthetics are prescribed for pain relief after an eye injury
F; the anesthetic prolongs epithelial healing
Oral agents are a better choice (opiods/nsaids)
if removing FB with a needle, the bevel shuld face
up
functions as lubricant in eye
bacitracin, ciprofloxacin
ophthalmic antibiotic ointments
easier to apply than ointment, enhance patient compliance, sulfacetamide, ofloxacin
ophthalmic solutions
T/F opthalmic steorids are a good joice post eye FB removal
false; delays healing
A patient presents with an alkali chemical splash to the eye. What is the first priority in management?
A) Instill topical anesthetic before assessment
B) Flush the eye with lactated Ringer’s or normal saline
C) Perform a fluorescein stain to assess for corneal defects
D) Administer IV antibiotics
B
Which of the following findings suggests a penetrating corneal injury requiring immediate ophthalmology referral?
A) Fluorescein staining revealing a linear corneal abrasion
B) A positive Seidel sign
C) Conjunctival injection and tearing
D) Pain relieved by topical anesthetics
B
What is the purpose of using fluorescein dye during an eye trauma exam?
A) To check for corneal abrasions or epithelial defects
B) To test for increased intraocular pressure
C) To assess pupillary reactivity
D) To measure anterior chamber depth
A
An IV access into one of the major blood vessels.
central line
types of central lines
venous catheter in jugular, subclavian, femoral vein
peripheral inserted central catheter (PICC)
implanted ports (IR)
pulmonary artery catheter
plasmapheresis catheter
IVC filter
catheter whose tip is located in the SVC, RA, or IVC
central venous access
locations of CVA insertion
jugular, subclavian, femoral, brachial
PICC is most commonly inserted into
basilic vein
u/s guided
fever complications thatn central line
ideal for community-based parenteral anti-infective therapy
can remain in place for months
PICC line
placed by IR or surgery, common in chemo, place for long periods of time
implanted port