13. Poly Cystic Ovary Syndrome
1/26
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
27 Terms
What is PCOS?
A variable disorder that is marked especially by amenorrhea, hirsutism, obesity, infertility, and ovarian enlargement and is usually initiated by an elevated level of luteinizing hormone, androgen, or estrogen which results in an abnormal cycle of gonadotropin release by the pituitary gland —abbreviation PCOS — called also polycystic ovary disease, polycystic ovary syndrome, Stein-Leventhal syndrome
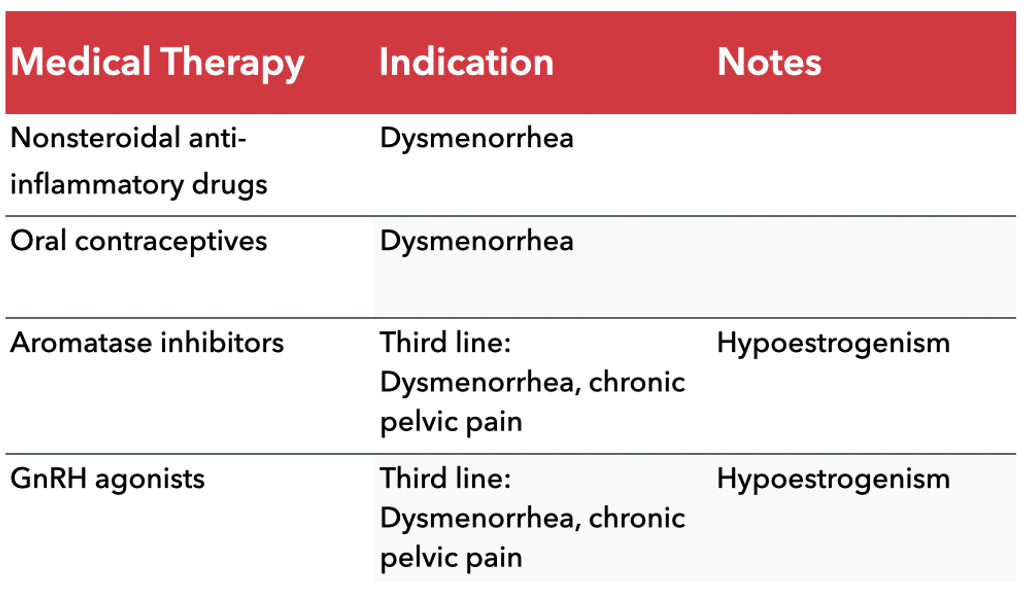
What are pain management/treatment options for PCOS?
Medical Therapy
Nonsteroidal anti-inflammatory drugs’
Indication: Dysmenorrhea
Oral contraceptives
Indication: Dysmenorrhea
Aromatase inhibitors
Third line: Dysmenorrhea, chronic pelvic pain
Notes: Hypoestrogenism (decrease in estrogen)
GnRH agonists (increase GnRH)
Third line: Dysmenorrhea, chronic pelvic pain
Notes: Hypoestrogenism (review this because it’s a bit counterintuitive)
What is Dysmenorrhea?
Dysmenorrhea is a medical term that refers to painful menstruation, which can occur just before or during a woman's menstrual period.
The pain is typically cramping in nature and may be felt in the lower abdomen, back, or thighs.
Other symptoms that can occur with dysmenorrhea include nausea, vomiting, headache, fatigue, and diarrhea.
Dysmenorrhea can be primary, meaning that there is no underlying medical condition causing the pain, or it can be secondary, which means that it is caused by a medical condition, such as endometriosis or uterine fibroids.
Treatment options for dysmenorrhea may include over-the-counter pain medications, hormonal birth control, or other prescription medications.
What is an ovarian cyst?
The most common type of ovarian cyst is called a functional cyst. These cysts are described as "functional" because they often develop during the menstrual cycle
There are 2 types (distinguished by thickness, amount of fluid, size):
[1] Follicular cysts: These usually go away on their own in 1 to 3 months. These form when an egg doesn't release as expected, so the follicle keeps growing.
[2] Corpus luteum cysts: These also usually go away on their own (1-3 months). These form after the follicle ruptures at ovulation. The follicle reseals and fluid starts to buildup within it. They can enlarge and cause pain, bleed, or twist the ovary.
Ovarian cysts can also be related to endometriosis, or formed from the outer surface of the ovary (cystadenomas), or formed with non-ovarian tissue (dermoid cysts)
Why is PCOS a common endocrine disorder?
PCOS is the most common endocrine disorder in reproductive aged people, with a prevalence between 5% and 15%, depending on the diagnostic criteria applied
Familial Occurrence
It has been well documented that PCOS tends to aggregate within families
In a study of 115 sisters of 80 probands (people with PCOS), PCOS was demonstrated in 22% of reproductive-aged siblings whereas hyperandrogenemia was found in an additional 24% (Legro et al., 1998)
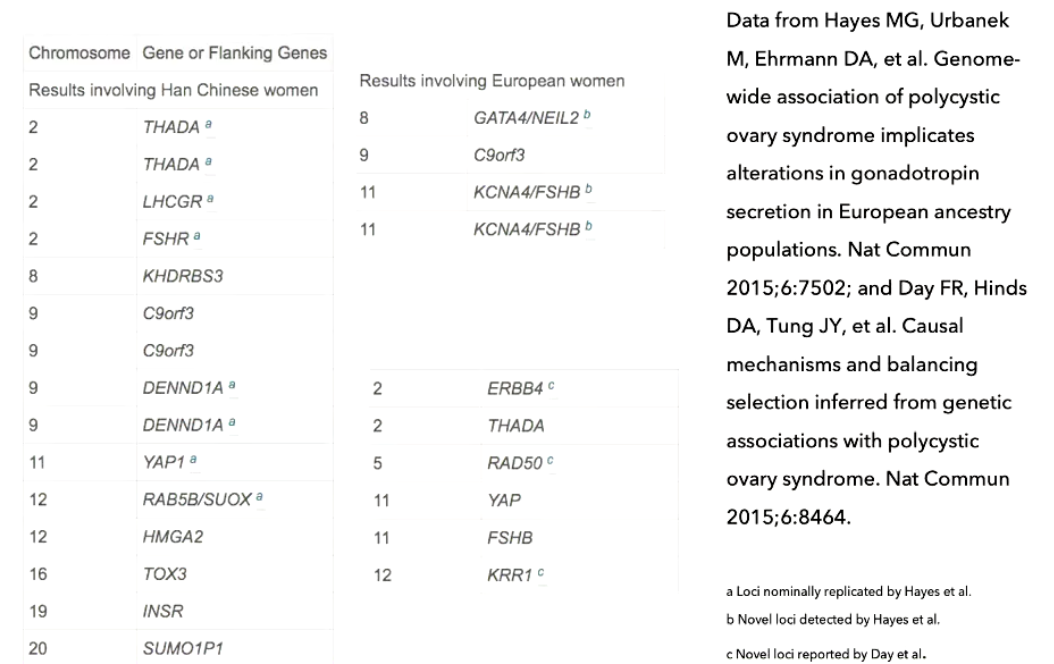
What are the genetics of PCOS?
Genome-wide association studies are a relatively new way for scientists to identify genes involved in human disease
This method searches the genome for small variations, called single nucleotide polymorphisms or SNPs, that occur more frequently in people with a particular disease than in people without the disease
Each study can look at hundreds or thousands of SNPs at the same time
Researchers use data from this type of study to pinpoint genes that may contribute to a person’s risk of developing a certain disease
What are genome-wide association studies?
GWAS = identifies many suspected genes across multiple chromosomes
PCOS genetics = complex + polygenic (not one single gene)
Flanking genes = genes located near the gene of interest
Ancestry matters:
Different populations (e.g., Han Chinese vs European) → different gene associations
Even on same chromosome → different implicated genes
Current limitation:
Findings are not yet directly useful for treatment decisions
Clinical diagnosis:
Based on patient signs/symptoms (phenotype)
Not primarily based on genetic findings (yet)
What is clinical description?
PCOS is a familial heterogeneous disorder of reproductive-aged people characterized by hyperandrogenism, ovulatory dysfunction, and polycystic ovary morphology
Despite intensive efforts by many investigators, the molecular basis of PCOS remains unclear
Available data indicate that PCOS is a complex trait modulated by genetic factors, intrauterine and environmental exposures, insulin resistance, pancreatic β cell function, steroidogenesis and steroid hormone metabolism
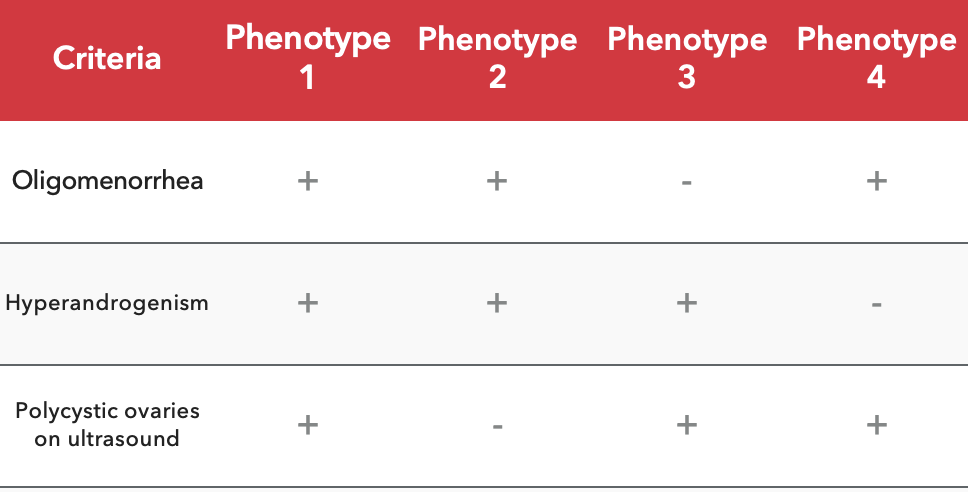
What are the clinical diagnostic criteria and phenotype variability in PCOS (clinical practice guidelines)?
3 key diagnostic criteria (know these):
Oligomenorrhea = infrequent menstrual periods (e.g., every 3–4 months)
Hyperandrogenism = excess androgens (e.g., testosterone)
Polycystic ovaries on ultrasound
Heterogeneity (key idea):
PCOS = variable presentations (phenotypes)
Do NOT need all 3 criteria for diagnosis
Examples of phenotypes:
All 3 present
Oligomenorrhea + hyperandrogenism (no cysts)
Hyperandrogenism + polycystic ovaries (normal periods)
Oligomenorrhea + polycystic ovaries (no hyperandrogenism)
Important implication:
Absence of cysts ≠ no PCOS
Suggests underlying follicle dysfunction (even if ultrasound normal)
Big picture:
Diagnosis = based on clinical features + variability, not one fixed presentation
What is an ovarian cyst?
The definition of a cyst is a fluid-filled sac
Cysts can occur anywhere in the body
With PCOS, individuals can develop "cysts" due to eggs not being released over time
The follicles keep growing and form multiple "cysts"

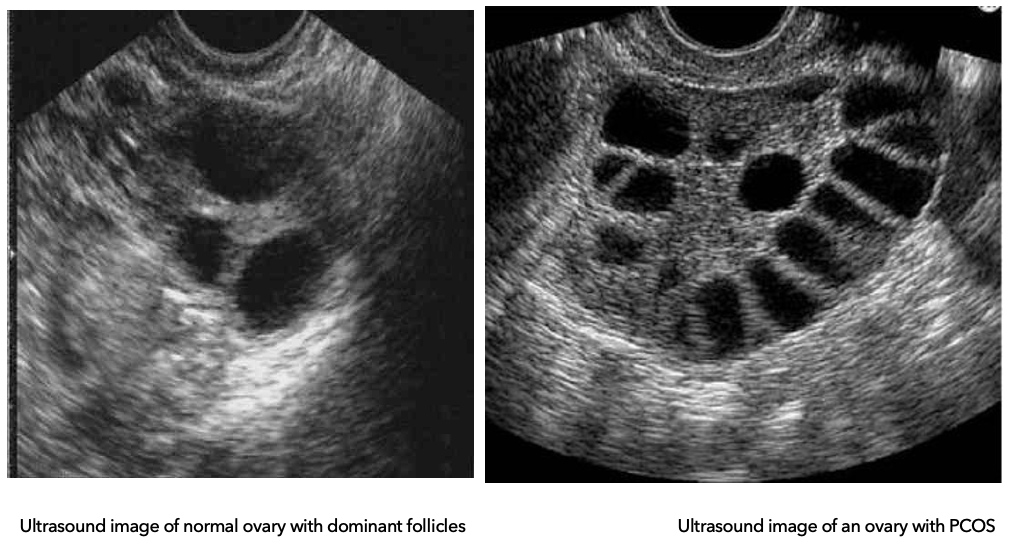
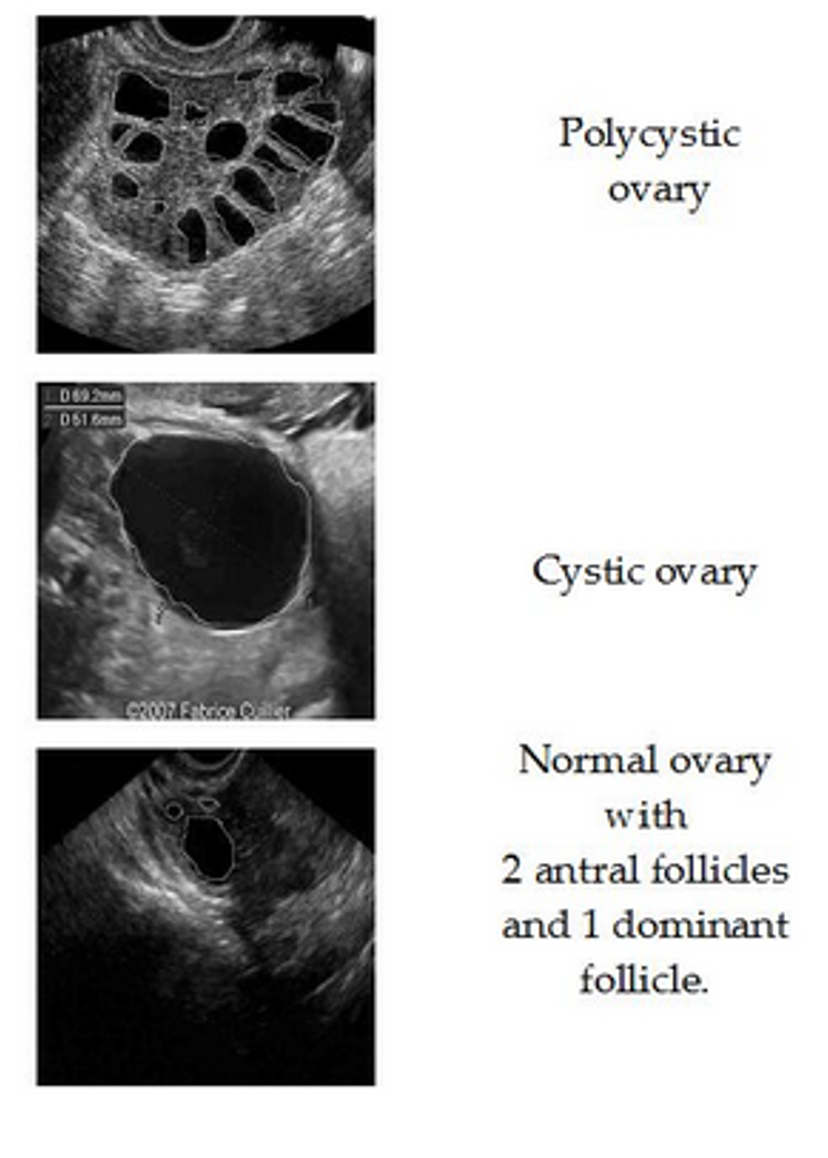
What is the difference between a normal ovary and a PCOS ovary on ultrasound?
Diagnostics: Ovarian Types
Normal ovary:
Multiple follicles develop
One becomes dominant → ovulation (egg released)
Others regress and are reabsorbed
PCOS ovary:
Follicles begin to grow but get arrested (don’t fully mature)
No dominant follicle → no ovulation
Follicles do not regress → accumulate in ovary
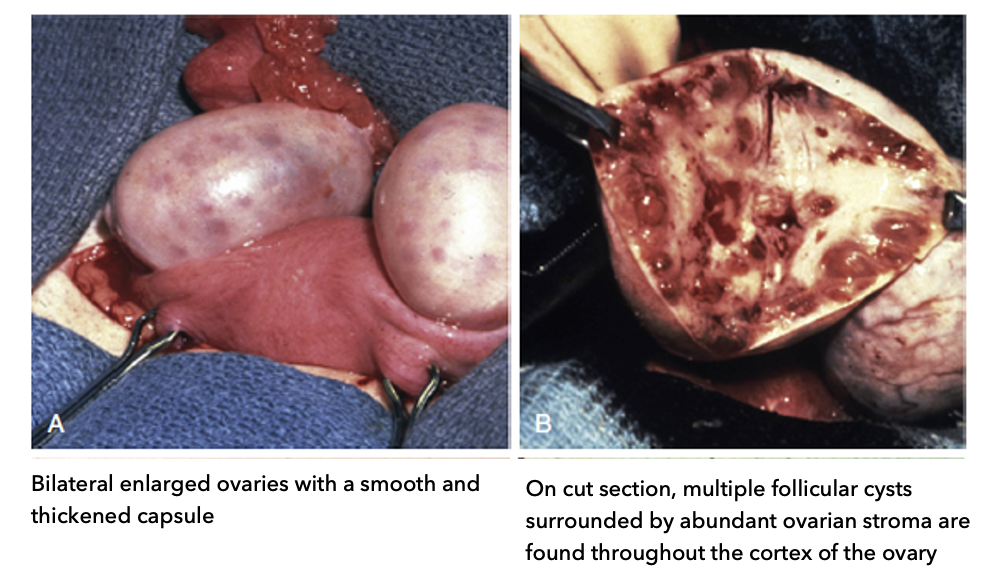
What are the gross (structural) characteristics of polycystic ovaries in PCOS?
A: External (gross) appearance:
Bilateral enlarged ovaries (both ovaries bigger than healthy)
Smooth, thickened capsule (outer layer is thicker than normal)
B: Cut section (internal structure):
Multiple follicular cysts (arrested follicles)
Cysts located in cortex (outer region) → “ring” near edge
Surrounded by abundant ovarian stroma (supportive tissue)
Key idea:
Follicles accumulate at outer cortex instead of maturing → hallmark of PCOS
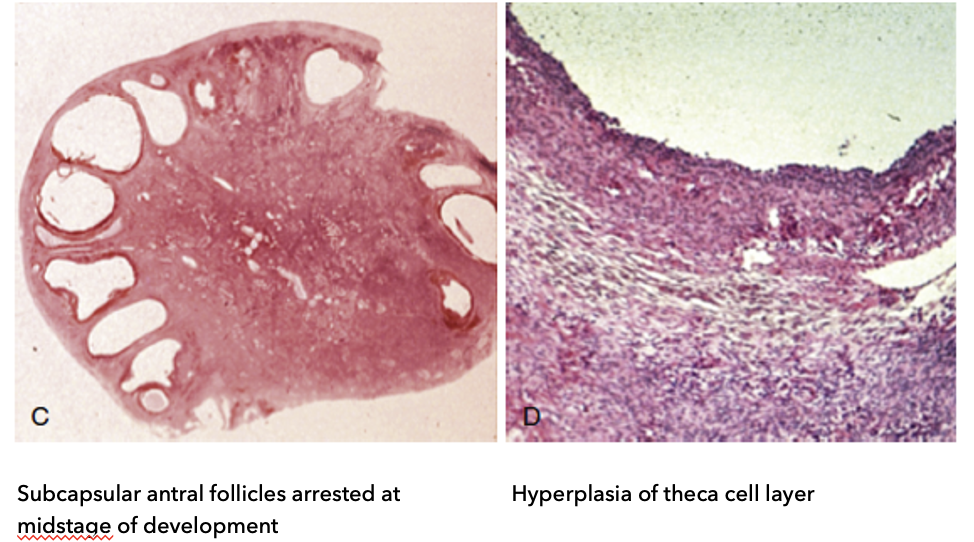
What are the microscopic features of polycystic ovaries in PCOS?
C: Follicle characteristics:
Subcapsular antral follicles (located just under capsule, near cortex)
Arrested at mid-stage development (do not fully mature)
Appear as “string of pearls” pattern
D: Cellular changes:
Hyperplasia of theca cell layer
↑ rate of cell reproduction → ↑ androgen (steroid) production
Key idea:
Arrested follicles + ↑ androgen-producing cells → core pathology of PCOS
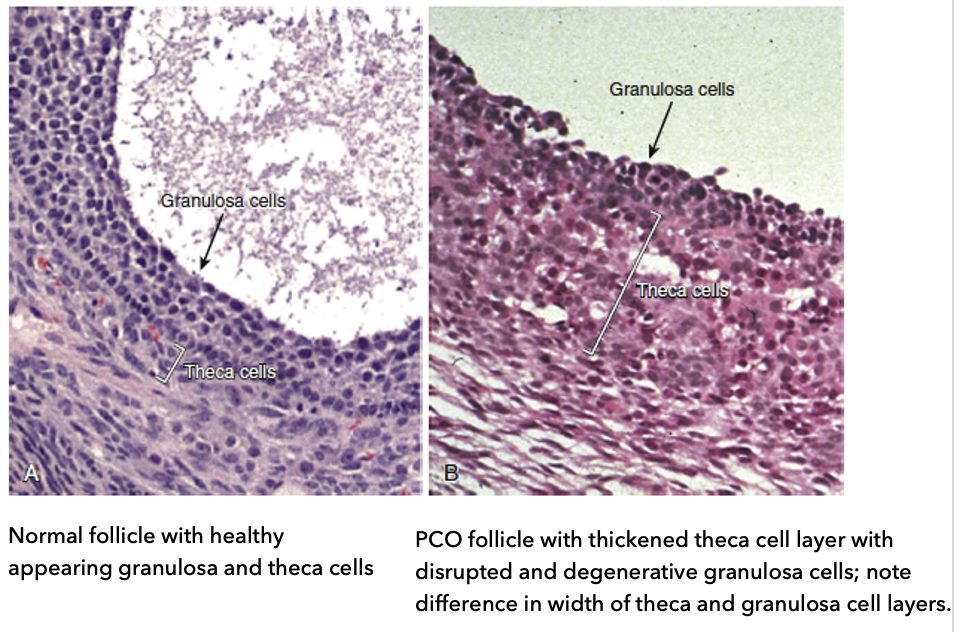
What is the histology of mid-antral follicular wall?
A: Normal follicle:
Healthy granulosa cells (supporting cells around oocyte)
Healthy theca cells (hormone-producing layer)
Balanced width of granulosa and theca layers
B: PCOS follicle:
Thickened theca cell layer (more cells → possible ↑ androgen production)
Disrupted and degenerative granulosa cells
Altered layer widths compared to normal
Key idea:
Histology shows follicle dysfunction + hyperactive theca cells, contributing to PCOS pathology
Hypothesis: Perhaps hyperandrogenism is coming from the ovaries
**Thecal cell = general term (thecal cells in adrenal gland); Theca = cells in the ovaries
What are clinical descriptions of PCOS?
[1] Hirsutism
[2] Menstrual Irregularity
[3] Ovarian Morphology
[4] Insulin Resistance
[5] Infertility
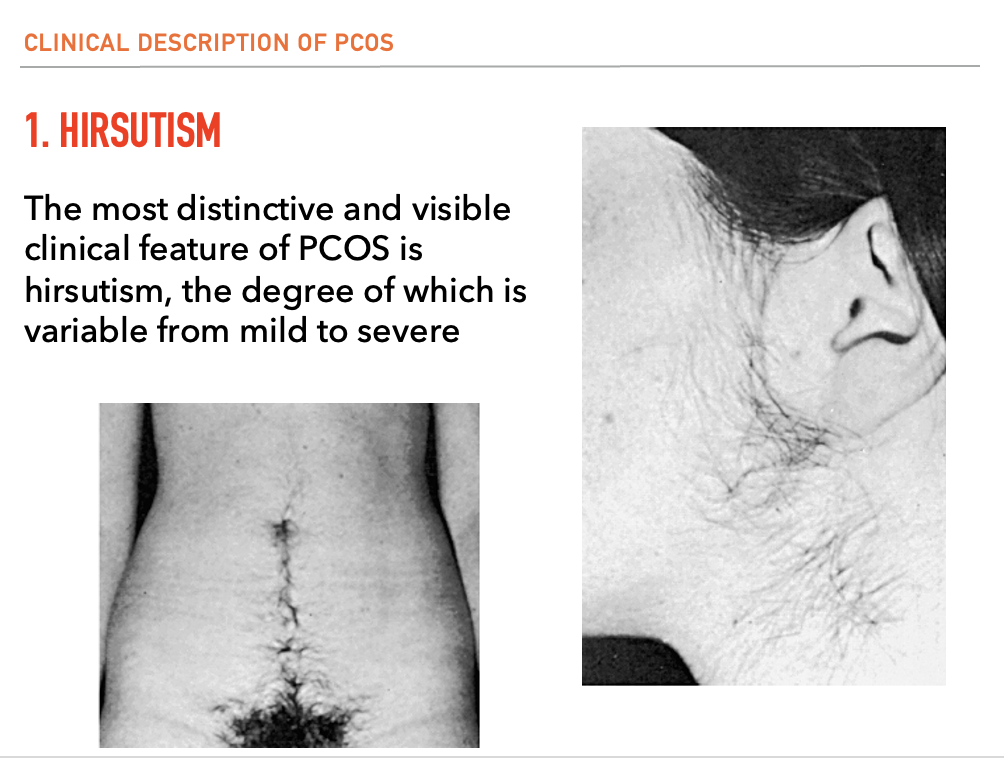
What is [1] Hirsutism?
The most distinctive and visible clinical feature of PCOS is hirsutism, the degree of which is variable from mild to severe
What is the pathophysiology of hirsutism?
In PCOS, the amount of hirsutism has been correlated to serum androgen concentrations
Coexisting conditions that alter the bioactivity of androgens, such as hypothyroidism and obesity may also give rise to excessive hair growth
↑ = Free testosterone
↓ = Sex-hormone binding globulin (SHBG)
What is Sex Hormone-Binding Globulin (SHBG) and its role in PCOS?
Definition:
Protein produced primarily by the liver
Circulates in the bloodstream
Function:
Binds sex hormones → reduces their bioavailability
Key hormones bound: testosterone, DHT (dihydrotestosterone), estradiol
Prevents excess hormones from activating receptors
PCOS connection:
Low SHBG → more free testosterone
Contributes to hyperandrogenism → male-pattern hair growth, other symptoms
Liver dysfunction + ovarian hyperplasia + insulin resistance all interact in pathophysiology
Key idea:
SHBG acts as a regulatory buffer for sex hormones; disruption amplifies PCOS hormonal imbalance
What is [2] Menstrual Irregularity?
Menstrual dysfunction is primarily characterized by irregular, infrequent, or absent menstrual bleeding
In some, the onset of chronic anovulation emerges beyond adolescence, but this is unusual
In approximately 20% of people, there is complete absence of menses, whereas 5% to 10% of cases demonstrate regular ovulatory function
Recognition of normal ovulation in PCOS is significant in that a history of regular menstrual cycles does not exclude the diagnosis
What happens to menstrual irregularity as PCOS women age?
It has been reported that in late reproductive life, PCOS women begin to experience regular ovulation [for unknown reasons]
Aging PCOS women with regular menstrual cycles appear to have a
[1] smaller follicle cohort,
[2] higher serum FSH levels and,
[3] lower androgen levels compared to age-matched PCOS with persistent anovulation
![<ul><li><p>It has been reported that in late reproductive life, PCOS women begin to experience regular ovulation [for unknown reasons]</p></li><li><p>Aging PCOS women with regular menstrual cycles appear to have a </p><ul><li><p>[1] smaller follicle cohort, </p></li><li><p>[2] higher serum FSH levels and,</p></li><li><p>[3] lower androgen levels compared to age-matched PCOS with persistent anovulation </p></li></ul></li></ul><p></p>](https://assets.knowt.com/user-attachments/08cc40b7-4748-4407-8ae4-71b740dfd631.png)
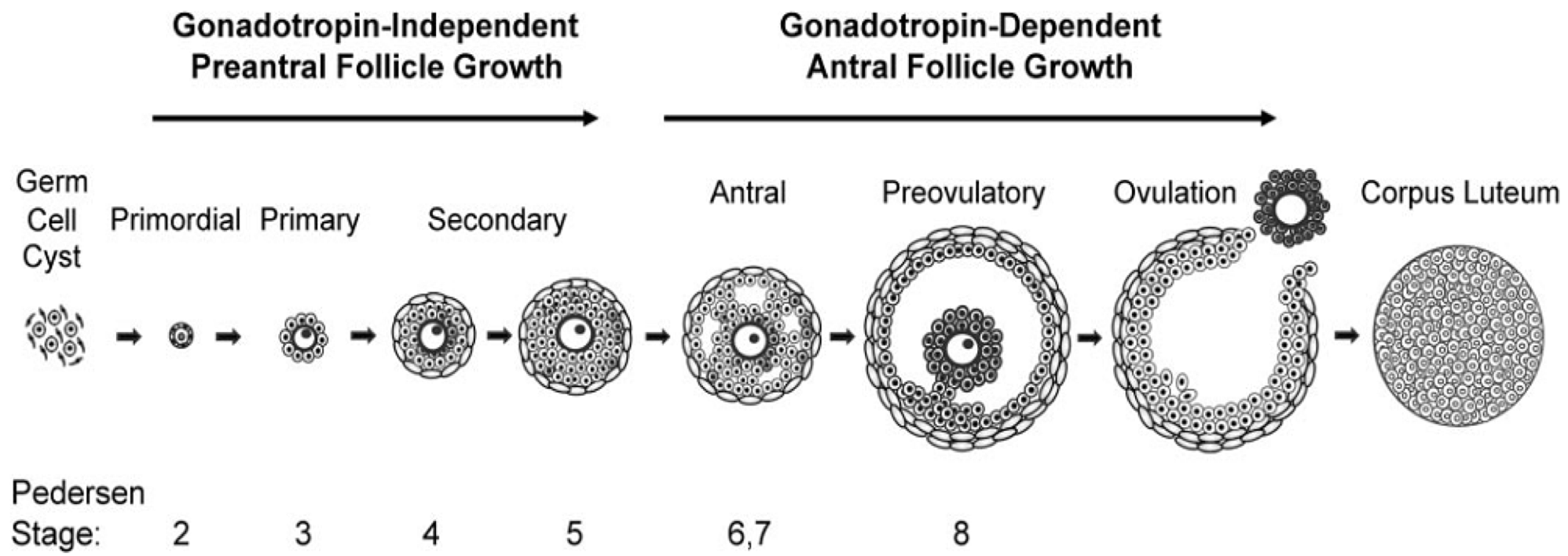
Why is follicle staging important in PCOS and what should be reviewed?
Diagnostic relevance:
Essential for ultrasound analysis in clinical/diagnostic settings
Helps identify arrested follicle stage
Review:
Different follicle stages (primordial → antral → preovulatory)
Gonadotropin-independent vs. gonadotropin-dependent stages
What is [3] Ovarian Morphology?
Classically, those with PCOS have enlarged ovaries with numerous peripheral small antral follicles and increased central stroma
Possible Mechanism: normal follicular growth appears to occur up to the midantral stage, after which maturation ceases
As the follicle reaches the midantral stage, the granulosa cell layer becomes progressively degenerative and the entire structure may have the appearance of a thin-walled cyst
In contrast, the thecal cell layer that surrounds the follicle becomes substantially hyperplastic and thickened compared to that of normal follicles and is responsible for increased androgen production
**Androgen increase in livers AND ovaries = hyperandrogegism is hallmark feature
What have histomorphometric studies revealed?
The ovarian follicle population in PCOS also is distinctive in that histomorphometric studies have revealed a twofold to threefold increase in the numbers of primary, secondary, and tertiary follicles compared to those of the normal ovary
Whether the ovaries are endowed with a greater number of follicles or whether the rate of programmed cell death is decelerated compared to the normal ovary has not been systematically studied
What is the pathophysiology of ovarian morphology?
A mechanism for the morphogenesis of the polycystic ovary has not been established
Although a role for androgen excess on follicle growth and development has been suggested from ovarian morphology in hyperandrogenic people with congenital adrenal hyperplasia and androgen producing ovarian tumours
Nonhuman primates treated with subcutaneous silastic capsules containing testosterone have been observed to develop enlarged ovaries and increased follicle number
What is AMH?
Ovarian Morphology: Anti-Müllerian Hormone (AMH)
Peptide hormone; primarily produced by granulosa cells of ovarian follicles; AMH is also a marker of ovarian reserve (reflecting the number and quality of remaining eggs); AMH declines as people approach menopause (fertility clinics also measure AMH)
It has been proposed that AMH has two potential functions
[1] AMH may serve to inhibit recruitment of primordial follicles into the pool of growing follicles to prevent early depletion
[2] AMH may decrease follicle sensitivity to gonadotropin stimulation to control the number of large preantral and small antral follicles that reach the preovulatory stage
These proposed actions of AMH are consistent with the report of decreased AMH expression in preantral and early antral follicles of women with PCOS compared to values observed in normal women
What is [4] Insulin Resistance?
Not only are people with PCOS predisposed to insulin resistance and risk for diabetes, but evidence exists that first-degree relatives also exhibit disordered glucose metabolism and insulin secretion
Importantly, this predisposition includes both sisters and brothers of affected individuals
Aside from the increased risk for diabetes, there is indirect evidence to indicate that insulin resistance may worsen the clinical manifestations of PCOS
Administration of insulin lowering drugs has been shown to improve insulin sensitivity, reduce androgen levels, and restore ovulation in some, but not all patients with this disorder
What is [5] Infertility?
Clearly, anovulation would appear to be the primary defect responsible for the failure to achieve pregnancy in this disorder
There is some evidence that those with PCOS have a higher incidence of spontaneous pregnancy loss, the mechanism of which remains unclear
It has been reported in a small series of people that the prevalence of polycystic ovaries in those with recurrent miscarriage is 56%