Additional Liver Disorders
1/23
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
24 Terms
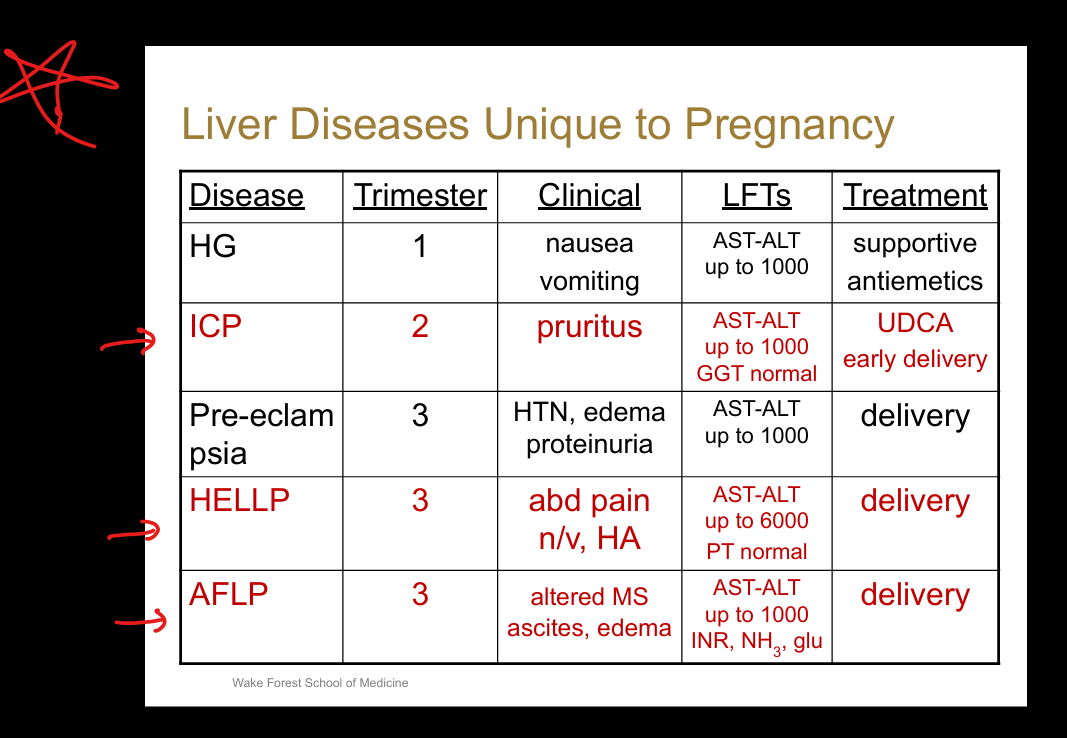
What liver diseases are unique to pregnancy?
Hyperemesis gravidarum, intrahepatic cholestasis of pregnancy (ICP), preeclampsia/eclampsia, HELLP syndrome, acute fatty liver of pregnancy (AFLP).
Hyperemesis gravidarum occur in? Sx? Treat?
First trimester. Intractable vomiting, >5% weight loss, ketonuria, dehydration, ALT/AST up to 1000, occasional jaundice. Supportive care—IV fluids, nutritional support, antiemetics
What is the cardinal symptom of intrahepatic cholestasis of pregnancy (ICP)? Caused by?
Pruritus (especially palms/soles, worse at night). Elevated serum bile Acids
What trimester does Intrahepatic Cholestasis of Pregancy occur in? Sx + Tests
Second trimester. ALT/AST up to 1000. Serum bile acids >10 µmol/L.
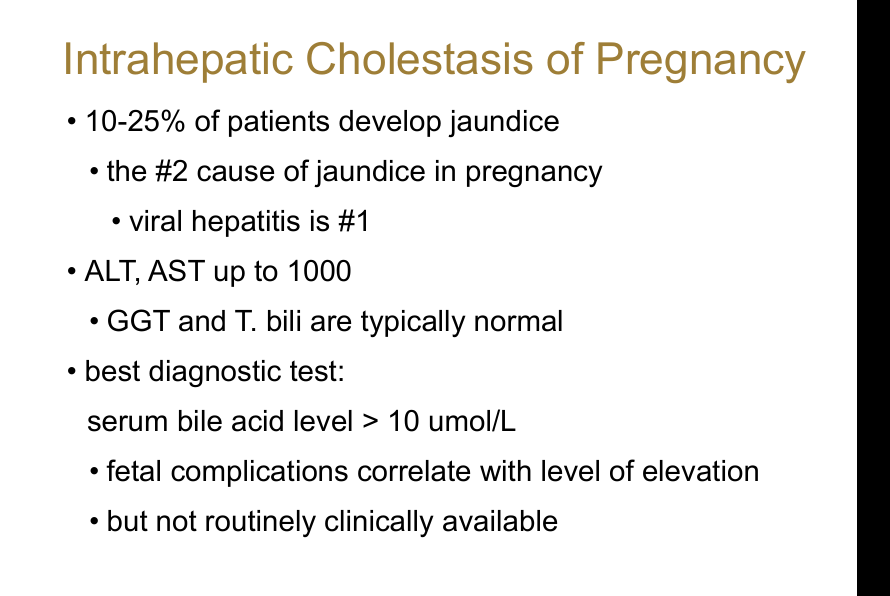
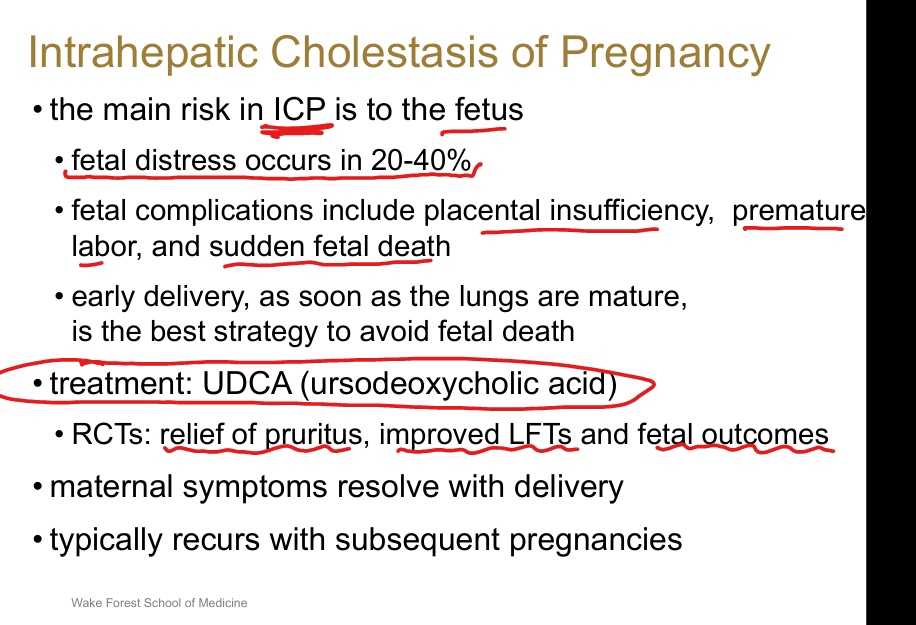
What is the major risk in Intrahepatic Cholestasis of Pregnancy? Treatment?
Fetal complications—fetal distress, placental insufficiency, preterm labor, sudden fetal death.
Treat: Ursodeoxycholic acid (UDCA) + early delivery once lungs mature.
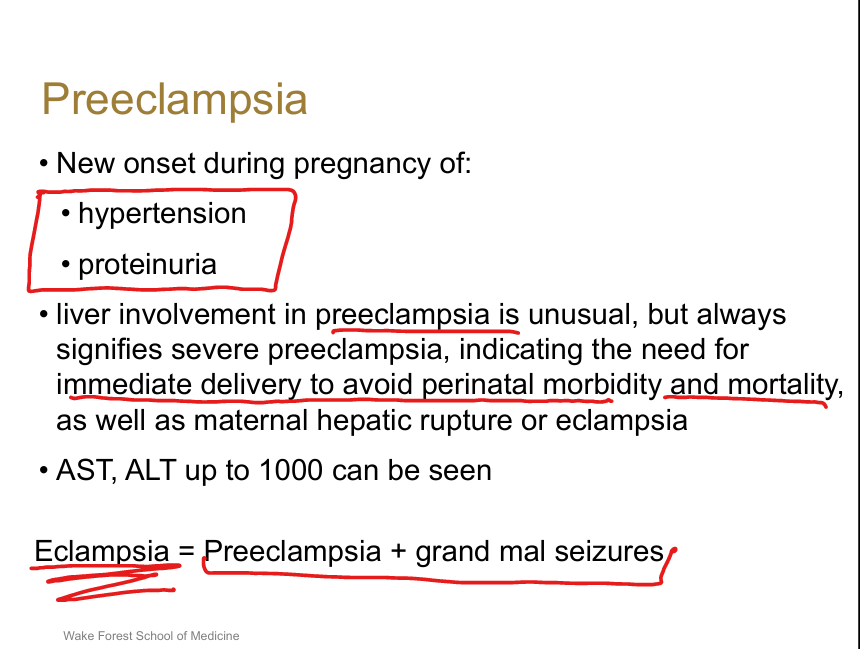
What defines preeclampsia?
New‑onset hypertension + proteinuria during pregnancy.
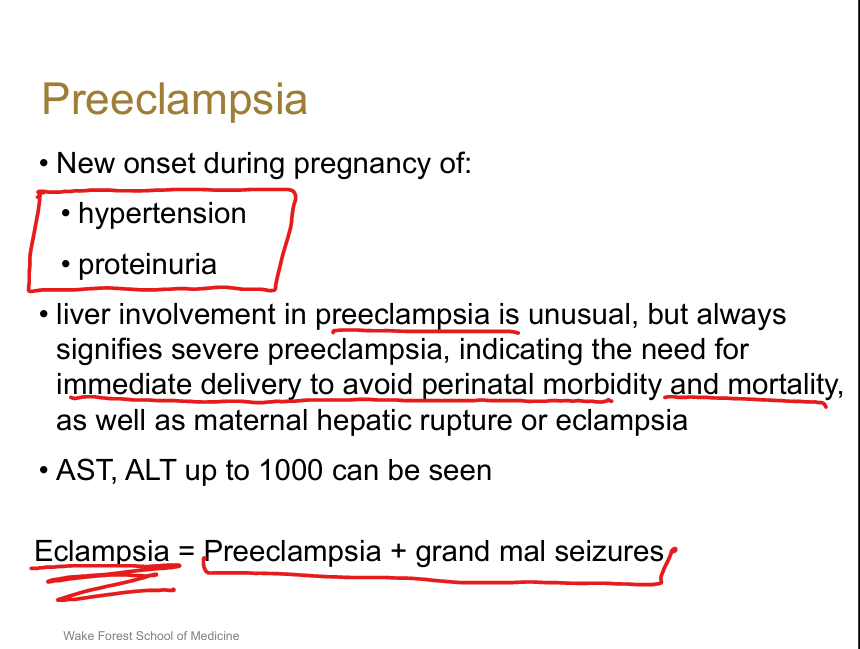
What is eclampsia?
Preeclampsia + seizures.
What does HELLP Syndrome stand for?
Hemolysis, Elevated Liver enzymes, Low Platelets.
What trimester does HELLP occur in? Sx?
Third trimester (can be postpartum). Epigastric/RUQ ab pain, N/V,Headache
What is the treatment for HELLP?
Immediate delivery (usually C‑section).
What causes acute fatty liver of pregnancy (AFLP)? Trimester? Tx?
Mitochondrial fatty acid oxidation defect (LCHAD deficiency). Third trimester. Sx: N/V, RUQ pain, jaundice, edema, encephalopathy, hypertension. Tx: Immediate delivery
What are causes of portal vein thrombosis?
Cirrhosis, hypercoagulable states (Factor V Leiden, Protein C deficiency, PNH, antithrombin deficiency, prothrombin mutation), OCPs, HCC, IBD, pancreatitis.
What are symptoms of chronic portal vein thrombosis?
Cavernous transformation of the portal vein
What is the management of portal vein thrombosis?
Evaluate etiology, screen for varices, consider anticoagulation (acute PVT).
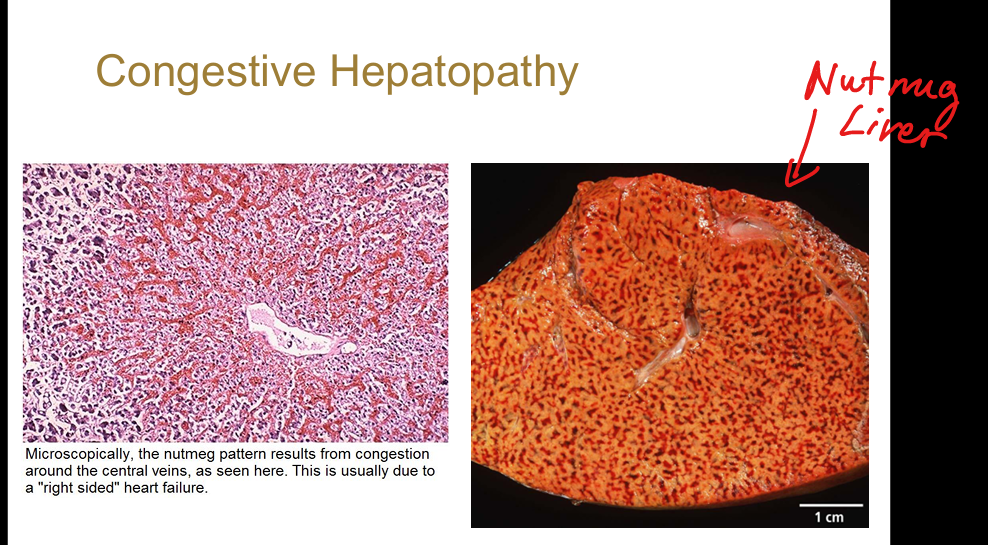
What causes congestive hepatopathy?
Right‑sided heart failure, tricuspid regurgitation, restrictive cardiomyopathy, constrictive pericarditis.
What is the classic pathology of congestive hepatopathy?
“Nutmeg liver”—centrilobular congestion.
What causes Budd‑Chiari syndrome?
Hepatic vein thrombosis.
What are risk factors for Budd‑Chiari?
Polycythemia vera, essential thrombocytosis, JAK2 mutation, Factor V Leiden, Protein C deficiency, PNH, OCPs, IBD, HCC invasion.
What are the clinical features of Budd‑Chiari?
=>obstruction of hepatic veins leading to Abdominal pain, hepatomegaly, ascites.
What is sinusoidal obstruction syndrome (SOS)? Sx? Risk factors?
Chemotherapy/radiation‑induced injury causing sinusoidal endothelial sloughing and obstruction. Causes: RUQ pain, jaundice, hepatomegaly, ascites, weight gain. Risks: Allogeneic bone marrow transplant.
What are key features of cavernous hemangioma?
Most common liver tumor (collection of blood vessels)
What are key features of focal nodular hyperplasia?
Benign, hyperplastic response to anomalous artery; most often in women
What are key features of hepatic adenoma?
Young women; strongly associated with estrogen therapy (oral contraceptives)
What are risk factors for hepatocellular carcinoma?
Cirrhosis (any cause), HBV (even without cirrhosis), HCV, alcohol, MASLD, hemochromatosis.