MSK Disorders of the Hand (2)
1/105
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
106 Terms
When the thumb and one or more fingers are in action the pattern is one of…
manipulative prehension and precision
When the thumb is not functional in the grasp pattern, the prehension is _________ and essentially one of ______.
nonmanipulative; power
Our thumb, index finger, and middle finger are essential for…
fine motor tasks
Our ring finger and small finger are essential for…
power gripping
1. Opening the hand
Closing the hand around the object
Application of appropriate force upon the object based on weight and size, surface characteristics, fragility, and use
Releasing of object by opening hand
In grasping, what parts of the hand are used?
all digits and the palm
In pinching, what parts of the hand are used?
digits on the radial side of the hand w/o contact with the palm
What finger contributes about 20-25% of grasping pattern?
small finger
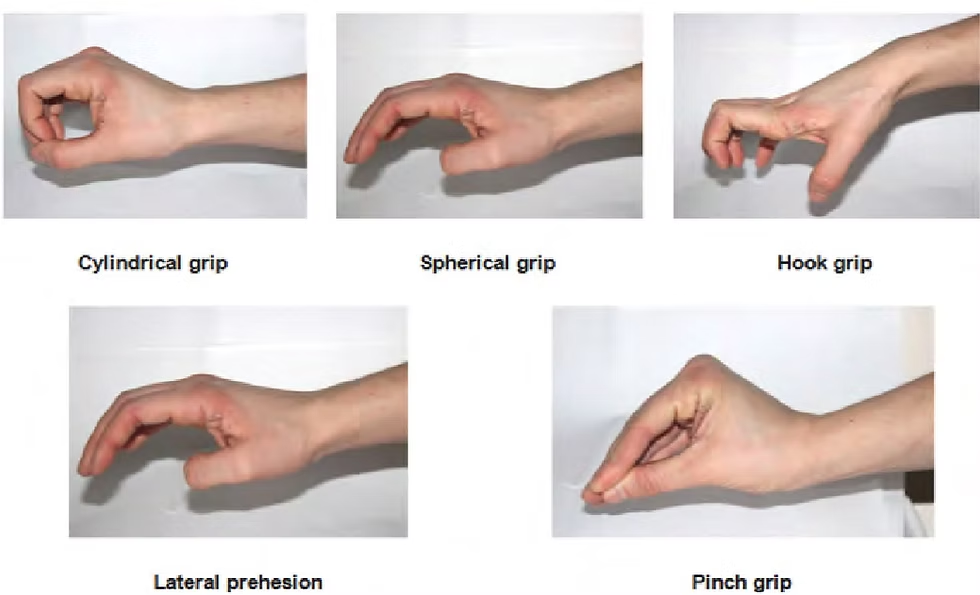
List the major functional pinch types.
lateral
tip-to-tip
3 jaw pinch
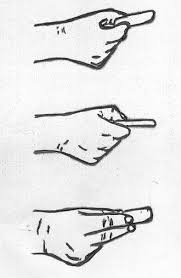
List the major functional grasp types.
hook, cylindrical, spherical
What are the three stages of tissue healing and their durations?
1. Inflammation (up to 72 hours)
Fibroplasia
Remodeling (early and late)
Describe the inflammation stage of tissue healing.
Vasoconstriction > vasodilation > WBC migration > removal of foreign bodies and dead tissues
Remodeling aims to…
Replace granulation tissue with mature scar to reconstruct near-normal matrix anatomy
Note > scar unable to achieve prewound architecture, strength, or fxn
Describe the fibroplasia stage of tissue healing.
2 to 6 weeks:
Fibroblasts begin the formation of scar tissue. Fibroblasts lay down new collagen, on which capillary buds grow, thus increasing tensile strength.
Wound tensile strength increases gradually
Pursue AROM and orthotics to protect healing
Describe the maturation stage of tissue healing. How long may this phase last?
AKA: The Remodeling Phase
The tissue’s architecture changes, reflecting improved organization of the collagen fibers and a further increase in tensile strength.
This allows the tissue to be more responsive.
T/F: Scar tissue is an exclusively bad condition and has severe functional implications.
False- Is normal following an injury; however, increased amounts can be catastrophic > can lead to blockages to movement shift angles and lines of pull
Adhesions, changes in density, alignment, and shape of surrounding soft tissues can change
What should be monitored during all phases of intervention in the tissue healing process?
tolerance of tissues to controlled stress
What in particular helps to reduce edema and restore motion following an upper extremity injury?
proximal motion, well-tolerated functional use (particularly while elevated)
RECALL: What are tendons?
extensions of muscles that connect to bone to create changes in joint angle for function
Tendinitis vs. Tendinosis
ACUTE VS CHRONIC
Tendinitis is an acute inflammatory response (heat, swelling, pain)
Therapy focused in reducing inflammation + may use orthosis
Tendinosis: non-inflammatory response is present and such that there is a degeneration of connective tissue. Consists of a breakdown of collagen d/t aging, micro trauma, or vascular compromise. (chronic)
What impedes on the remodeling of microruptures in tendons?
Because of a lack of a robust intrinsic blood supply and uneven strain, healing and remodeling responses are altered. (hard for muscle to respond and heal)
T/F: DeQuervain’s is a form of tendinosis.
False- Tendinitis
T/F: Tennis elbow is a form of tendinosis
true
What is tendinopathy?
term for conditions of tendons known as tendonitis or tendinosis
What occupations can cause DeQuervain’s?
meal preparation
golfing
knitting
being a new mother
playing racket sports
computer work > sustained hyperabduction thumb posture on space bar
What interventions may be used for DeQuervain’s?
Joint protection techniques: supinated hands + lifting close to body; strengthening proximal musculature
Nonsteroidal anti-inflammatory drugs with possible corticosteroid injection at first dorsal compartment.
Nonresponsive cases may require surgical release of first dorsal compartment to relieve pressure & friction on APL and EPB tendons.
Teach clients to avoid wrist deviation (e.g., in conjunction with pinching).
Provide built-up handles and forearm-based thumb spica orthosis—leaving IP free.
Suggest alternatives to activities that bring on or make condition worse.
Use ice to reduce inflammation.
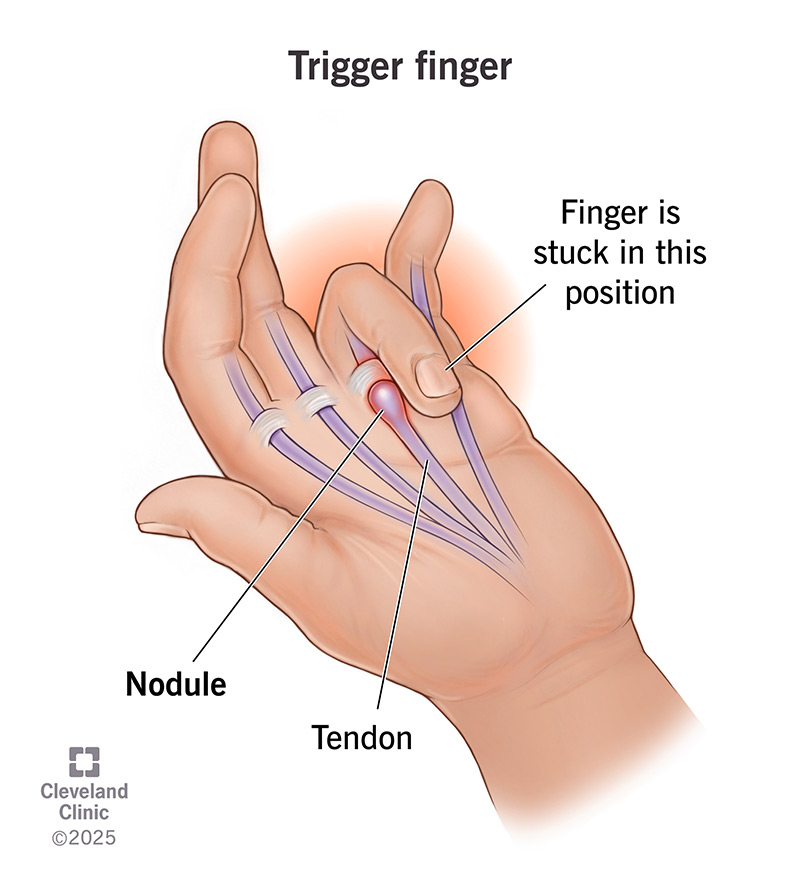
Trigger Finger
A nodule on the flexor tendon sheath and stenosis at the A-1 pulley causing "locking" or "snapping" during resisted grip
Pain present over A1 pulley
What interventions can be used to address trigger finger?
Orthotic fabrication at the MPJ or PIPJ
Avoid full gripping, PIP joint blocking
Surgeon releases A-1 pulley to stop repeated inflammation caused by triggering— may reduce chance of recurrence.
Ultimately want to mobilize the PIP
Individuals with _______ are more at risk of developing trigger finger.
diabetes
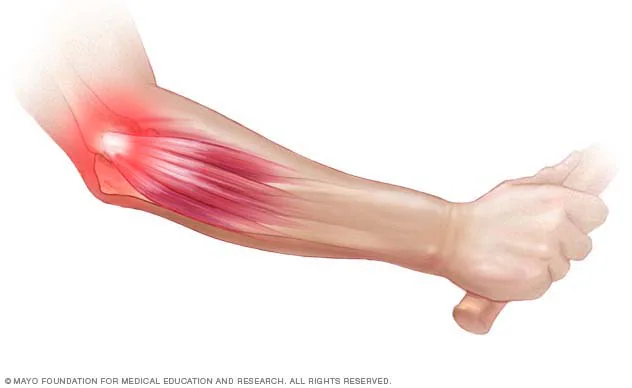
Lateral Epicondylosis (Tennis Elbow)
Overuse/force overload injury d/t degeneration of common extensor tendon (most commonly the ECRB) along the lateral epicondyle of the humerus
Typically aggravated by repetitive lifting with arms extended and palms down
What special tests are done for lateral epicondylosis?
Special testing:
Mill’s test:
Cozen’s test:
grip dynamometer with elbow extended
What are some interventions for lateral epicondylosis?
Wrist brace vs. Counterforce brace
wrist brace over counterforce brace > radial nerve travels over extensor mass; compressive forces placed on to radial nerve > can lead to radial nerve syndromes
15-20 degrees of extension when putting on brace
Joint protection techniques
Corticosteroids or Platlet-Rich Plasma
Too many corticosteroid injections may lead to tendon rupture
No supportive research on PRP injections
Surgery not very common. Physicians typically order series of therapy.
Surgical options may include arthroscopy or open procedure
growth of scar tissue > recovery not really seen
Shoulder strengthening exercises, neutral wrist > proximal stability
Identify the three types of nerve injuries (list).
Neuropraxia, Axonotmesis, and Neurotmesis
What may cause nerve injuries?
May result from compression by an internal or external source.
Internal examples: traction
May also occur secondary to traction or stretching of the nerve, burns, or radiation.
What is neuropraxia?
Neuropraxia: light compression on nerve (recall: foot falling asleep)
What is axonotmesis?
Axonotmesis: mild or severe
mild/moderate: splinting, soft tissue work, decreasing edema
severe: splinting might not work, might need surgery to decompress the area
What is neurotmesis?
Neurotmesis: severe, need surgery
Nerve injuries include…
acute or chronic compression
stretch ischemia
electrical shock
radiation
injection
laceration.
How does carpal tunnel syndrome typically present?
Typical complaints include hand numbness, particularly at night or when driving a car, along with pain and paresthesia in the distribution of the median nerve (thumb through radial ring finger pads), and clumsiness or weakness
The “carpal tunnel” consists of…
Carpal tunnel is formed by carpal bones dorsally and transverse carpal ligament volarly.
Acts as a pulley for nine long finger flexor tendons during gripping.
What are typical interventions to address carpal tunnel syndrome?
Wrist brace
Joint protection techniques
still want to emphasize breaks
If symptoms continue, atrophy of the thenar eminence is noted.
Surgical intervention may be warranted if symptoms do not improve.
Surgical release of the transverse carpal ligament
CTS Special Tests
Phalen’s, Reverse Phalen’s, Durkan’s, and Tinel’s
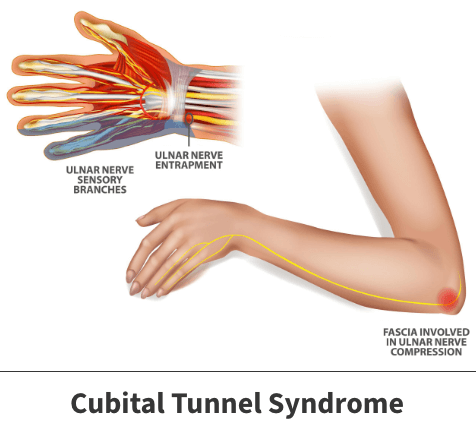
Cubital Tunnel Syndrome
Compression of the ulnar nerve at the elbow, causing medial forearm pain and numbness in the small and ring fingers
Osborne ligament > ulnar nerve gets compressed under constant pressure
Typically presents as:
Pain along medial forearm
decreased sensation along the dorsal and palmar surfaces of small finger and ulnar half of ring finger
weakness of RF and SF
What special tests are used to assess for cubital tunnel syndrome.
Elbow flexion test; Tinel’s test
What are some interventions for cubital tunnel?
Sleeping position, joint protection techniques
Long arm splinting preventing elbow from bending more than 90 degrees is ideal
Surgery:
in-situ decompression, subcutaneous ulnar nerve transposition, or submuscular ulnar nerve transposition
submuscular transposition (common):
reroute ulnar nerve anteriorly (beneath flexor-pronator muscles)
Individuals with what condition may be more susceptible to cubital tunnel syndrome? Why is this the case?
Clinical consideration: stroke and guarding position
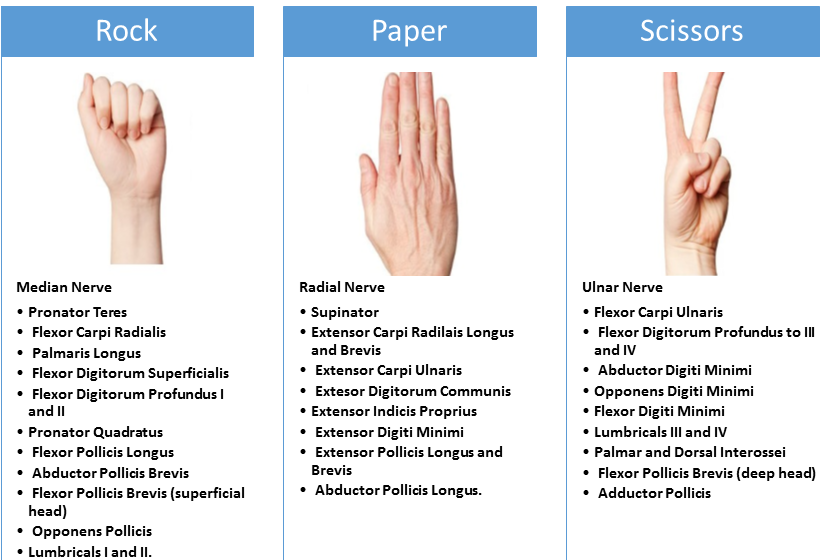
What is the "Rock, Scissors, Paper" mnemonic for nerve injury?
Rock = Median nerve: unable to flex FDPs of the IF/MF
Scissors = Ulnar nerve: unable to abduct and adduct digits > affects interossei
Paper = Radial Nerve: unable to extend the MPJs
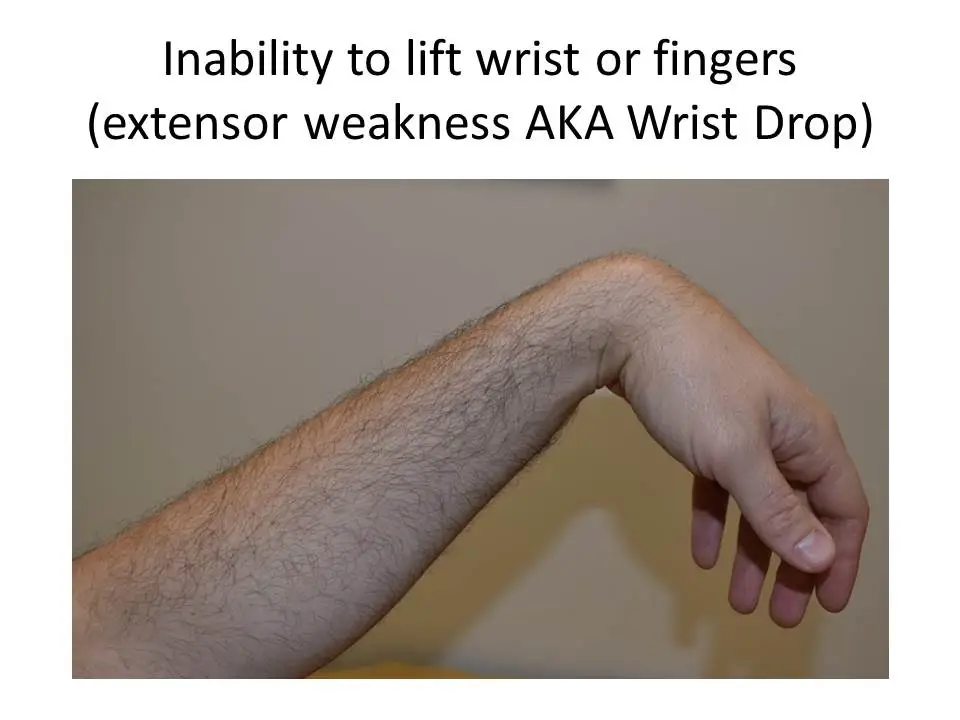
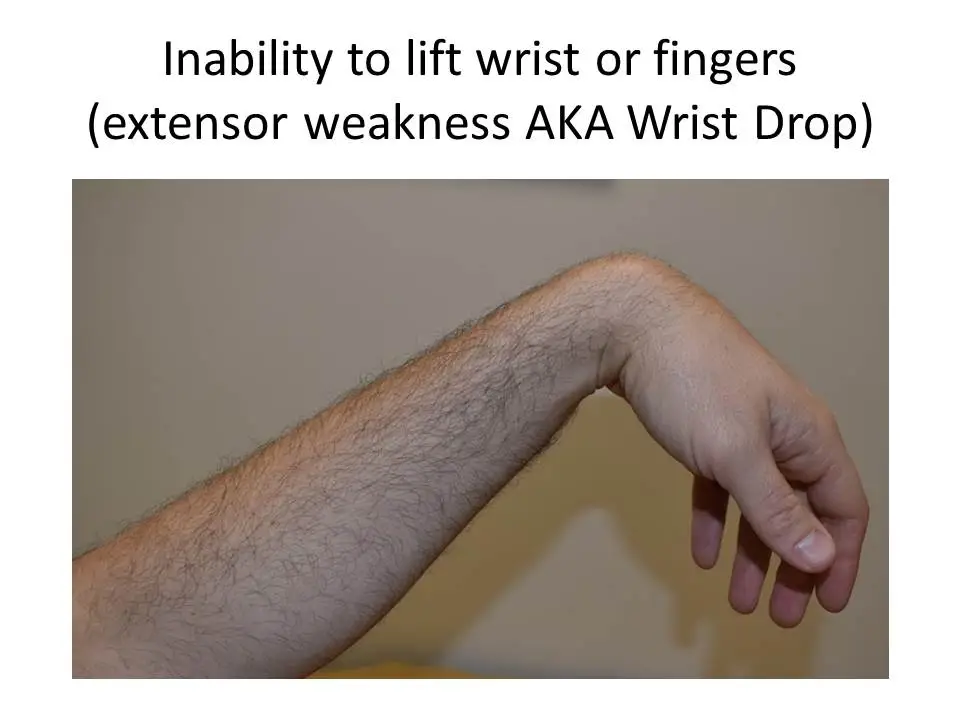
What is posterior interosseous syndrome?
AKA: Wrist Drop/Radial Nerve Palsy
Presents two ways:
Paralysis affects all muscles innervated by posterior interosseous nerve, with inability to extend MP joints of thumb, index, long, ring, or small fingers.
Person cannot extend MP joint of one or more digits.
What interventions can be used for radial nerve palsy?
Orthoses (“cock-up splint”)

Explain the regeneration/healing process of posterior interosseous nerve syndrome.
Muscles will slowly regenerate but takes time. Preservation is key. Tendon transfer recommended if pt’s muscles do not return by 6-12 months.
tendon transfer > reroute to the muscles
T/F: Individuals with posterior interosseous nerve syndrome with present with sensory deficits.
False- posterior interosseous nerve is a motor nerve > pt will present w/ muscle weakness or paralysis along thse muscles, but no deficits in sensation
What of the goal of treatment for a nerve laceration?
Goal now is to prevent joint contractures before tendon transfer is performed.
To attempt reinnervation—distal portion of severed nerve is reattached to proximal portion (containing nucleus) in close to perfect alignment. (Nerve transfer)
Desired outcome—axons to regrow into existing nerve tunnels in hope they will reach terminal (sensory or motor) end plates.
Laceration at wrist results in ______________, with denervation of…
low median nerve palsy
denervation of opponens pollicis & abductor pollicis brevis of thumb and lumbricals to index and long fingers.
Laceration at the elbow results in __________ , with denervation of the…
high median nerve palsy
denervantion of the FDP (IF/MF), pronator teres/quadratus
How are median nerve lesions treated?
In therapy, prepare clients for tendon transfers by preventing deformity with orthotics & by maintaining:
(a) PROM of pronation
(b) digital MPs in flexion
(c) digital IPs in extension
(d) thumb CMC abduction.
Laceration of ulnar nerve at wrist, a ____ ulnar lesion, results in loss of _________. Denervation occurs at the…
low ulnar lesion
loss of most hand intrinsics
denervation of abductor digiti minimi, flexor digiti minimi, & opponens digiti minimi results in flattening of hand with loss of ulnar transverse metacarpal arch.
FDS + FDP also affected
What are the functional impacts of ulnar nerve lesions?
loss of sensation
cannot go into intrinsic + positioning; going into intrinsic minus positioning
Ring and small fingers present a “claw hand” deformity.
compensation for extension

High radial nerve injury often occurs with what kind of injury?
Intrinsic tightness can occur, leading to difficulty with MP extension and IP flexion if length of interosseous and lumbrical muscles are not maintained during period of lost extrinsic extension.
humeral fxs
How does to radial nerve present?
leads to absent wrist, digital extensors, and “wrist drop” deformity.
What may occur with radial nerve laceration (muscle effects)?
Intrinsic tightness can occur, leading to difficulty with MP extension and IP flexion if length of interosseous and lumbrical muscles are not maintained during period of lost extrinsic extension.
Static vs. Dynamic Stabilizers
Ligaments are static stabilizers (connect bone to bone)
sustain the position of the joint
Muscles/tendons act as dynamic stabilizers
if surrounding muscles are weak, can lead to sprains/fxs
Grades of Ligament Sprains
Grade I—ligament remains intact, but there is diffuse individual fiber disruption.
Grade II—complete disruption of one of joint capsule’s major retaining ligaments.
Grade III—complete disruption of one collateral ligament and injury to dorsal and/or volar capsular structures.
What are common problems with grade I and II ligament sprains?
Pain, decreased ROM, and risk of flexion contracture are common problems with grades I and II injuries.
What are common problems with grade III ligament sprains?
Joint instability with grade III
T/F: Injury to the ulnar collateral ligament of the thumb MCP is common
False- only occurs 1/10 as often
How are grade III ulnar collateral thumb ligament injuries treated?
injuries require surgical repair with interosseous wire because an avulsed ligament will retract and not return to original insertion on bone—leaving joint instability.
Skier’s Thumb
Injury to the ulnar collateral ligament (UCL) of the thumb MCP joint (Grade III)
Osteoarthritis (OA) vs. Rheumatoid Arthritis (RA)
OA involves cartilage degradation and bone remodeling (osteophytes)
RA involves synovial inflammation; cartilage and bone destruction that leads to deformity, and impacts CV, pulmonary, and skeletal systems.
Why is it that CMC OA of the thumb is more painful in the non-dominant hand?
Non-dominant hand used more for isometric/stabilizing movements
pain in thumb from pinching, typically w/ tip and 3-jaw pinch
increased laxity in the CMC of the thumb
Why is it that the radius is most commonly fractured in wrist fractures?
During WBing, radius takes ~80% of load, thus most commonly fractured.
any fracture > ligament damage
What are the functional impacts of wrist fractures?
Decreased wrist ROM, decreased grip strength, alteration of the carpal alignment, and instability may ensue. Other complications include extrinsic tightness, tendon rupture, compression of the median or ulnar nerve, and complex regional pain syndrome (CRPS)
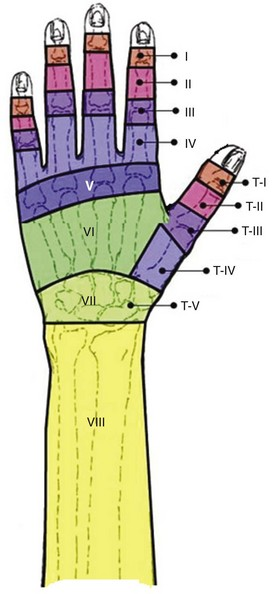
Identify and describe the zones of flexor tendon injury.
Zone I - Insertion of FDS to FDP
Zone II - Area where FDS & FDP lie within flexor sheath
Zone III - Area from distal edge of carpal tunnel to A-1 pulley of flexor sheath
Zone IV – Where flexor lie under transverse carpal ligament in carpal tunnel
Zone V - Area from forearm flexor musculotendinous junction to border of transverse carpal ligament
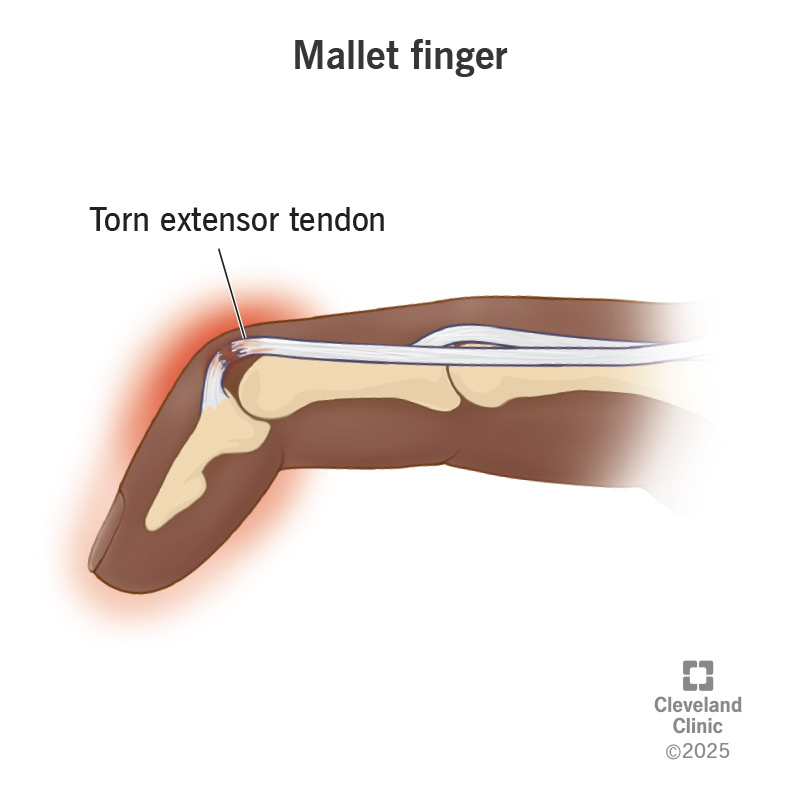
Tendon injury at Zone I and II of the extensor tendon can lead to what? Also describe interventions and healing time.
Zones I and II—mallet deformity
Zone I or II may not require surgical intervention
Intervention immobilized in slight hyperextension for 8 weeks—leaving PIP joint free.
When analyzing occupational performance of the hands, what should be assessed?
Analysis of occupational performance
Assessing ROM, grip strength, sensation
Assess more proximal and the whole body
Shoulder, neck, posture, body language, etc.
Identify some common hand assessments.
Visual Analogue scale (VAS)
Goniometry
Grip & pinch strength
Manual muscle testing
Disabilities of the arm, shoulder, and hand assessment (DASH)
What physiological impacts can anxiety have affecting the healing of hand injuries?
⬆ anxiety ➡ ⬆ BP ➡ ⬆ edema and scar tissue
Describe some practices for edema control.
Elevation, active exercise, deep breathing, compression
Foam wedges, cold corn
fingers tend to go into adduction
want to increase webspace
Retrograde massage, compressive wrapping, compression garments, flossing, therapeutic cold.
Flossing: wrapping with theraband to help circulate edema
What is the difference between peripheral edema and lymphedema?
Peripheral edema—caused by increase in blood supply with capillary leaking.
Lymphedema—chronic; caused by impaired lymphatic function— requires specialized therapy.
What structure of the hand contributes to ulnar sided stability?
TFCC
using splints/orthoses to stabilize w/ ulnar sided wrist pain
What is the purpose of digital tendon gliding exercises?
Reduce risk of scar adhesions between tendons and surrounding tissue that can occur following tendon repair, crushing injury, and fractures (i.e., finger bones).
If doctor approves, what intervention should you encourage the client to do?
If doctor approves, encourage client to use gentle full arcs of ROM—avoid quick or incomplete arcs.
Use meaningful activities to target structures that require motion.
During acute inflammatory stage, _______ is appropriate. After inflammation subsides and joint displays a soft end feel,_______ is productive.
static splinting > dynamic splinting
Acute tendinopathy should be treated with…
Treat acute phase with ice, compression, elevation of involved structures, and rest, if needed, to manage pain.
After inflammation subsides, tendinopathy interventions can be upgraded to restore function via gradual… It is best to start with what kind of movements/exercises? Why?
use of hand balanced with rest—avoid pain.
Start with isometrics as they provide an analgesic response
What is the purpose of “blocking” exercises?
Technique to improve tendon gliding/excursion— can assist capsular stretch.
Involves blocking finger joints from flexing or extending to increase tendon force at impacted joint.
Why best to perform digital tendon gliding exercises while elevated?
Want the lymph to circulate back to the heart
What can be done for scar management?
Compression (e.g., Isotoner gloves, Tubigrip, etc.) and mechanical forces of vibration used to soften and mature scar.
Silicone gel applied to scar is effective in reducing appearance of scar.
Elastomere padding
What are interventions for distal radius fractures during the immobilization phase?
Focus on edema management
Goals of immobilization are to normalize edema and achieve nearly normal AROM.
Intrinsic and extrinsic tightness, digital joint tightness may occur
active insufficiency at the wrist
Describe the functional impacts of each ligament injury grade.
Grade I: May produce discomfort during activities—requiring rest, thermal modalities, and temporary modifications to work, ADL, and leisure activities.
Grade II: Require longer immobilization until ligament fibers are healed—gentle protected movement encouraged, within anatomical lines, to maintain joint flexibility but prevent reinjury.
Grade III: Require surgical intervention to reattach ligament to bone with OT to improve functional use of hand following full healing.