anticoagulants basics exam 3 PART 1
1/72
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
73 Terms
Anesthetic Implications
– Preop Considerations
👉 Undetected bleeding → life-threatening intraop
👉 Hx first, then labs: platelets, PT/PTT, fibrinolysis
👉 Meds matter: ASA, NSAIDs, herbals (ginkgo, garlic, ginseng) → ↓ plat
Anticoagulants
• Unfractionated heparin
• Low-molecular-weight heparin
• Coumarin derivatives
• Direct thrombin inhibitors
• Direct factor Xa inhibitors
Nonherbal Dietary
• Vitamin K
• Vitamin E
• Coenzyme O10
• Zinc
• Omega-3 fatty acids
Procoagulants
Vitamin K
Antiplatelets
• NSAIDs
Persantine
• Thienopyridine
Antifibrinolytics
• Aminocaproic acid
• Tranexamic acid
Herbal
• Garlic, Ginger, Ginkgo
• Feverfew, Fish oil and Flaxseed oil
• Black cohosh (KUSH)
• Cranberry
Antiplatelets (platelet problem)
GANG memory trick
ASA
NSAIDs
Clopidogrel / Prasugrel / Ticlopidine (ADP blockers)
GPIIb/IIIa inhibitors (Abciximab, Eptifibatide, Tirofiban)
Anticoagulants (clotting cascade problem)
Think: “factors blocked”
Heparin / LMWH
Warfarin
DOACs (dabigatran, rivaroxaban, apixaban, etc.)
Fibrinolytics (clot busters)
tPA
Streptokinase
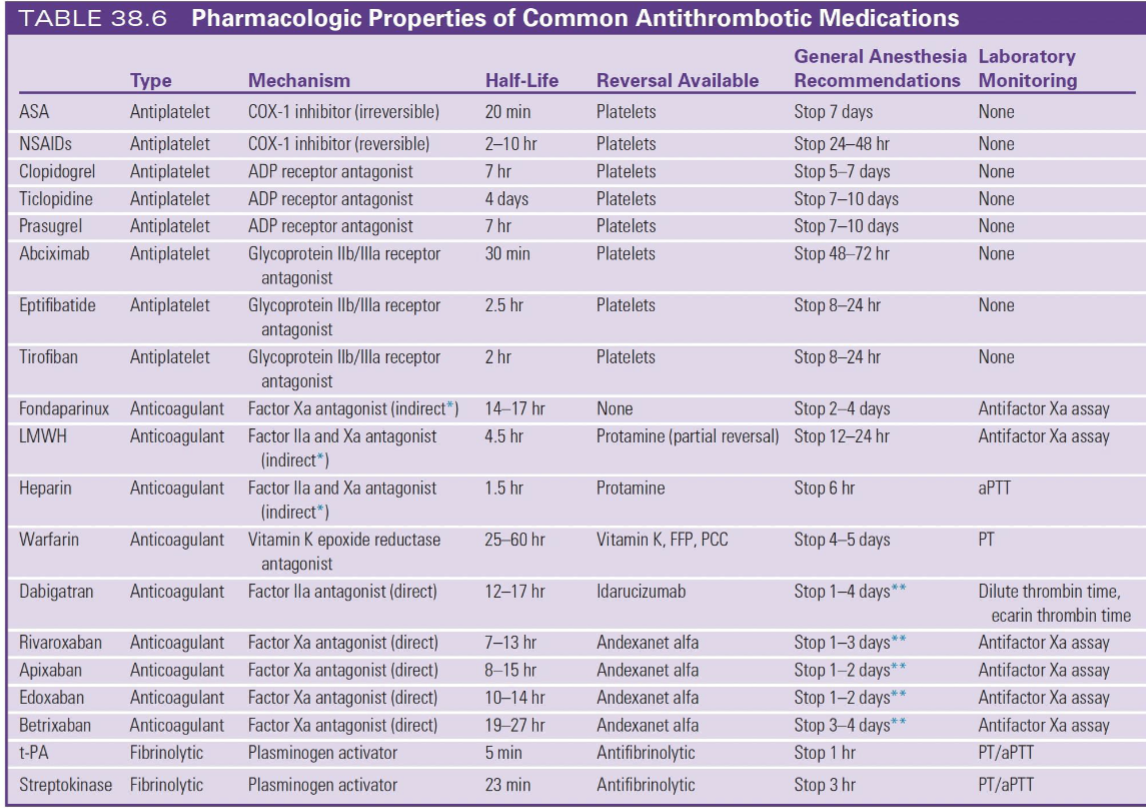
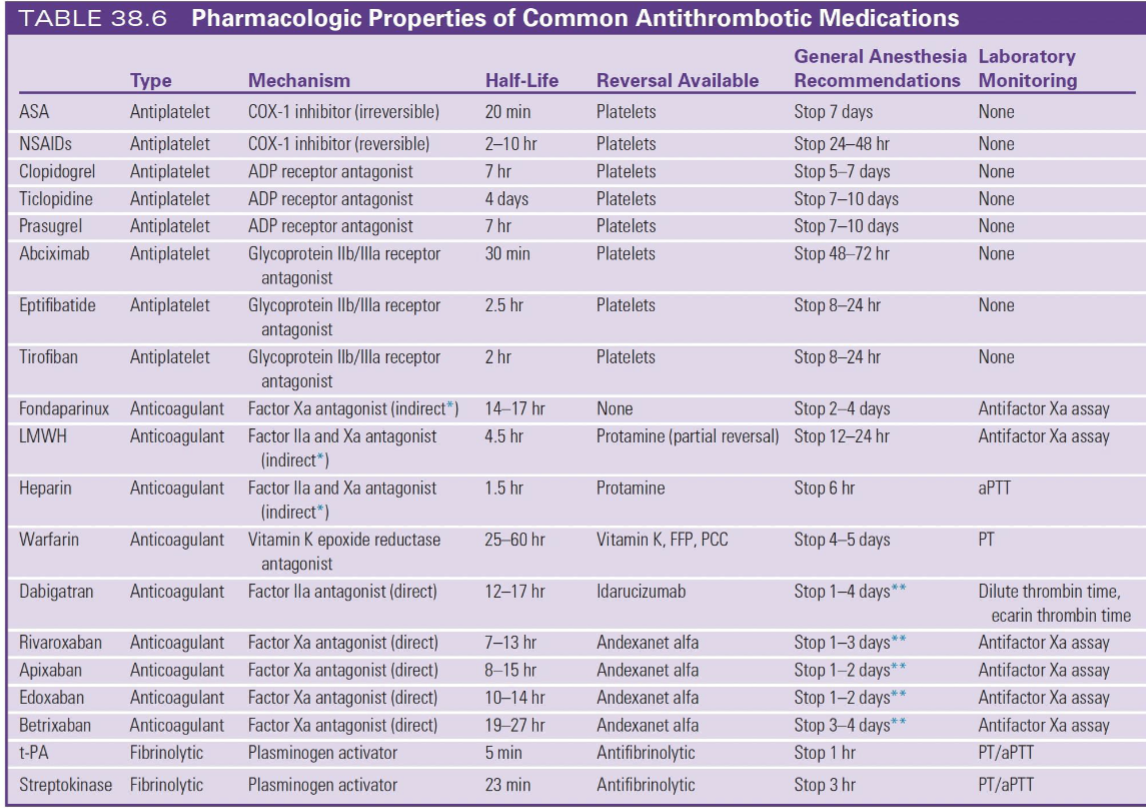
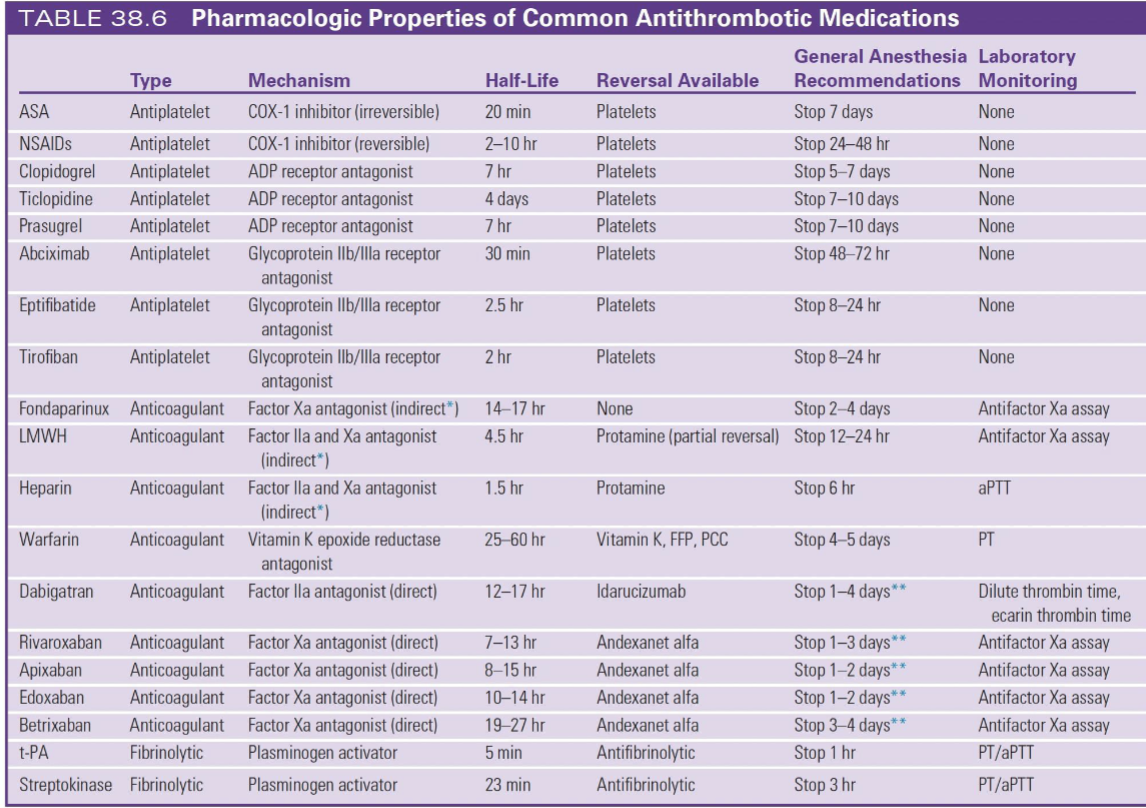
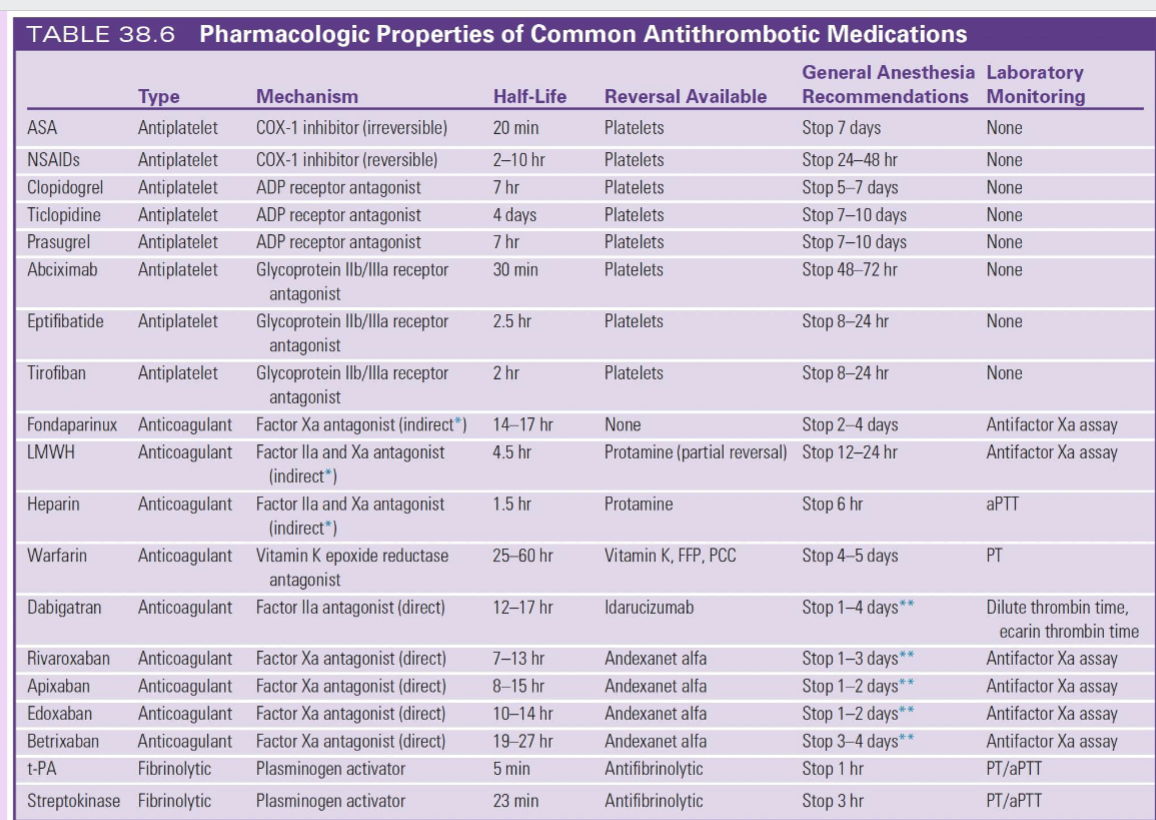
ANTIPLATELETS = LONG HOLD (especially ASA & Plavix)
ASA → stop 7 days (irreversible)
Clopidogrel → stop 5–7 days
Prasugrel/Ticlopidine → stop 7–10 days
NSAIDs = SHORT HOLD
Stop 24–48 hrs
👉 reversible = quick recovery
GPIIb/IIIa inhibitors = VERY SHORT
Stop 8–72 hrs
Eptifibatide and Tirofiban: stop 8-24 hrs
Abciximab - stop 48 - 72 hrs
ADP receptor antagonis
Clopidogrel: 5-7 days
Prasugrel: stop 7-10 days
Ticlopidine: stop 7-10 days
ANTICOAGULANTS = THINK HALF-LIFE
Heparins:
Heparin → stop 6 hrs, reversal = protamine, monitor = aPTT
LMWH → stop 12–24 hrs, partial protamine, monitor = anti-Xa
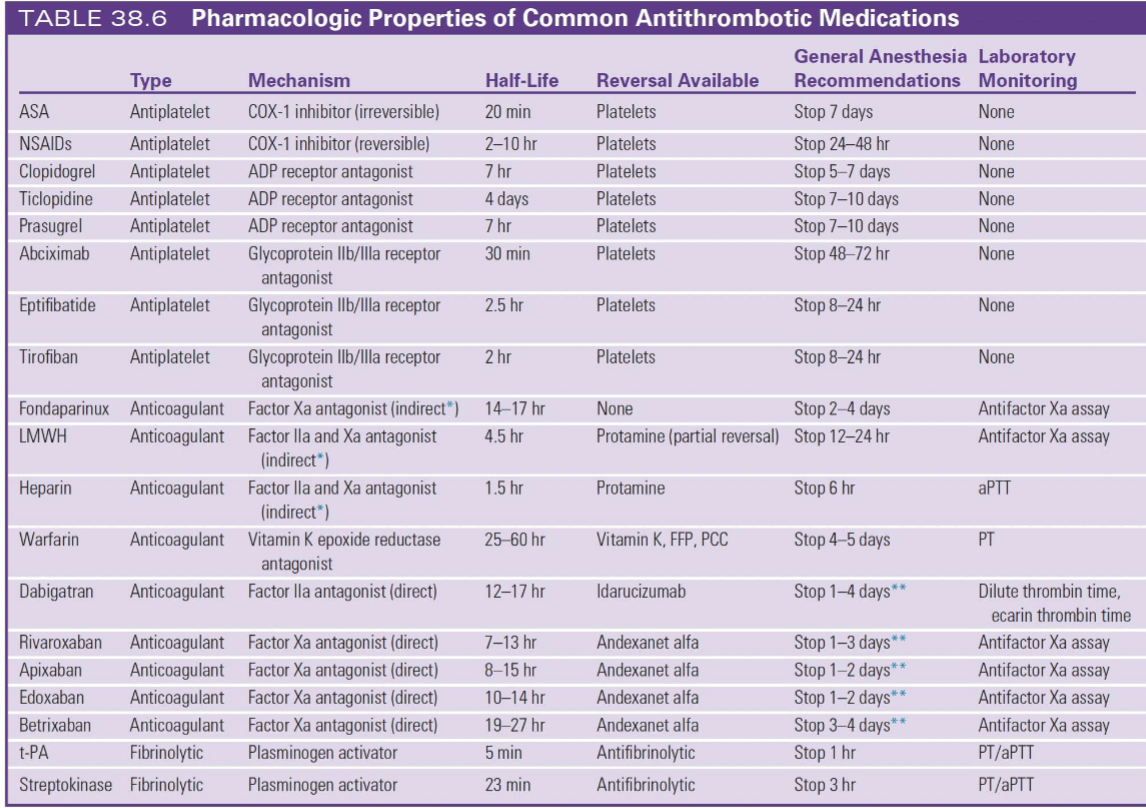
Warfarin = SLOW
Stop 4–5 days
Reversal:
Vitamin K
FFP / PCC
Monitor = PT/INR
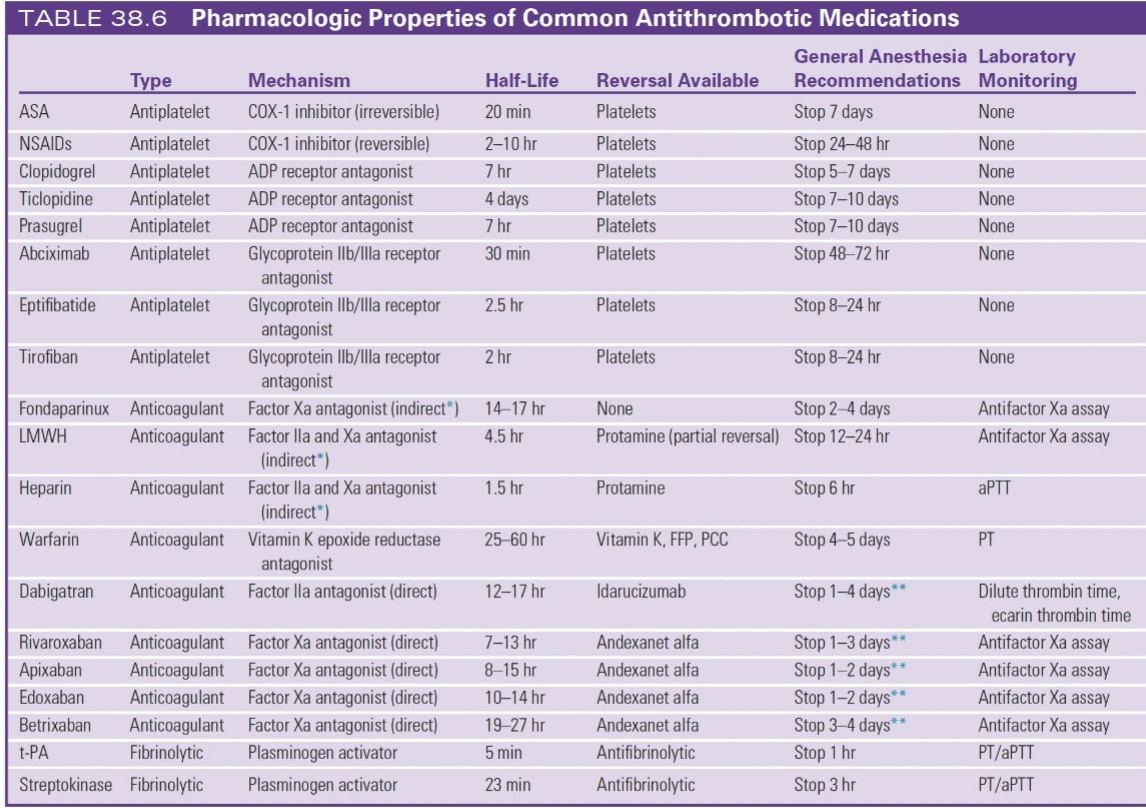
DOACs = SHORT + CLEAN
Dabigatran (Factor IIa)
Stop 1–4 days
Reversal = idarucizumab
Xa inhibitors (rivaroxaban, apixaban, etc.)
Stop 1–3 days
Reversal = andexanet alfa
👉 Monitor = anti-Xa
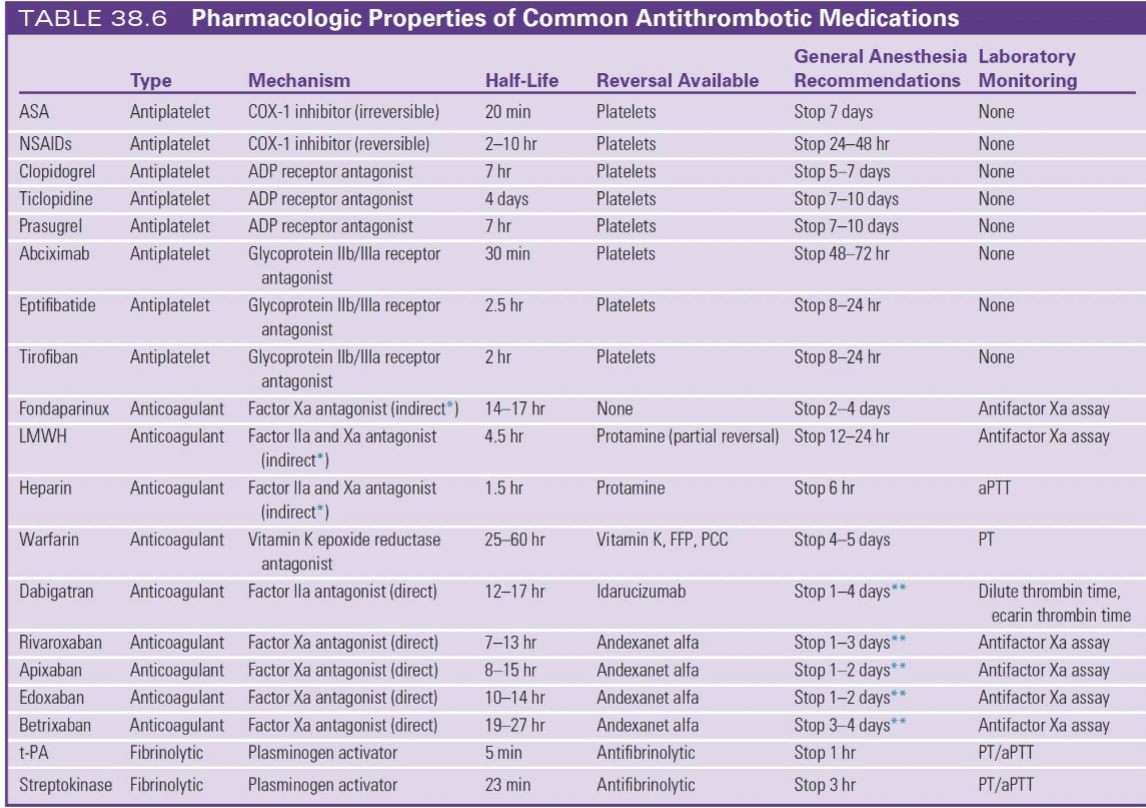
FIBRINOLYTICS
tPA → stop 1 hr
Streptokinase → stop 3 hr
👉 but HIGH bleeding risk
ULTRA-HIGH YIELD MEMORY TRICKS
“7–5–1 Rule”
7 days → ASA
5 days → Plavix
1–3 days → DOACs
Reversal Cheat Sheet
Heparin → protamine
Warfarin → Vit K + PCC/FFP
Dabigatran → idarucizumab
Xa inhibitors → andexanet alfa
Antiplatelets → platelets
🔥 Monitoring
Heparin → aPTT
Warfarin → PT/INR
LMWH/DOACs → anti-Xa
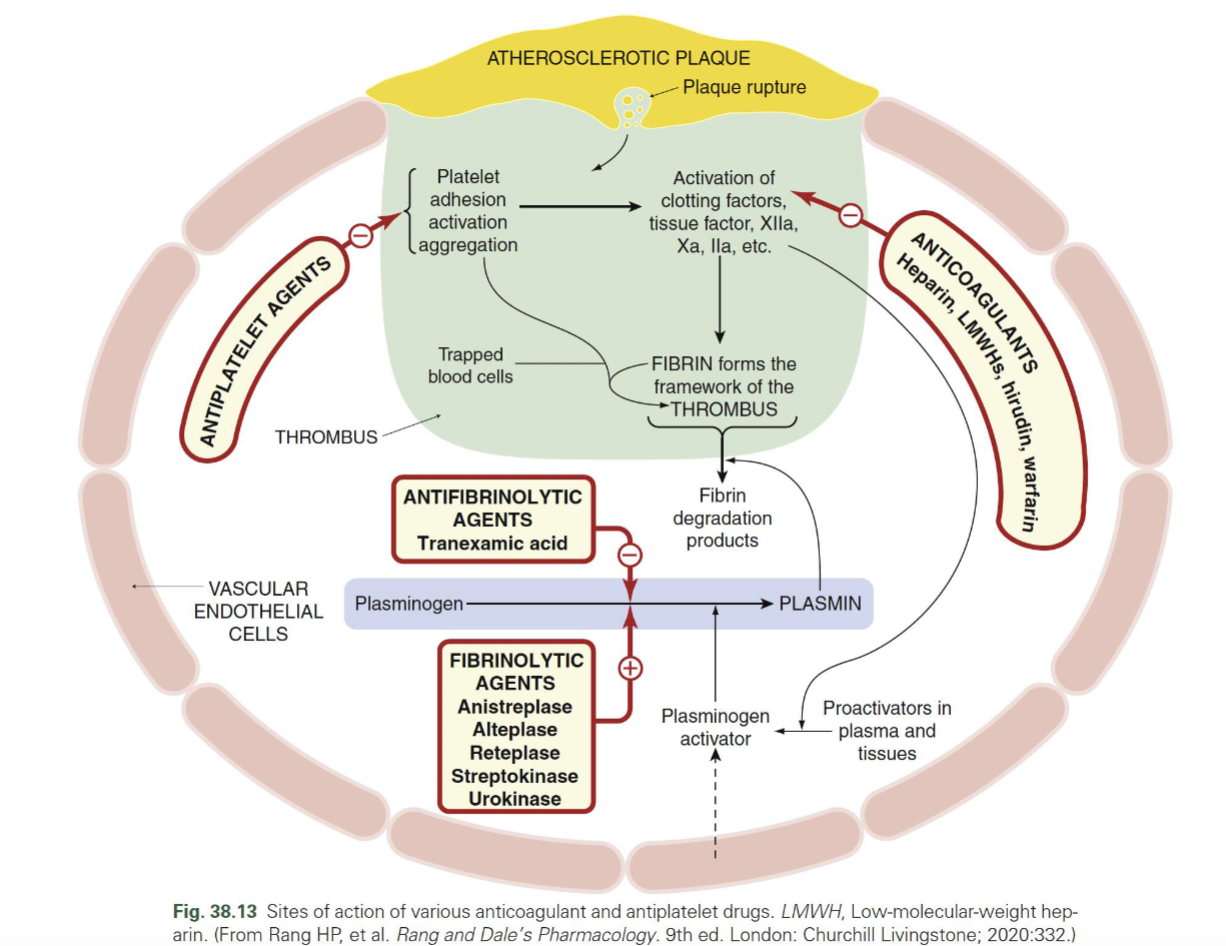
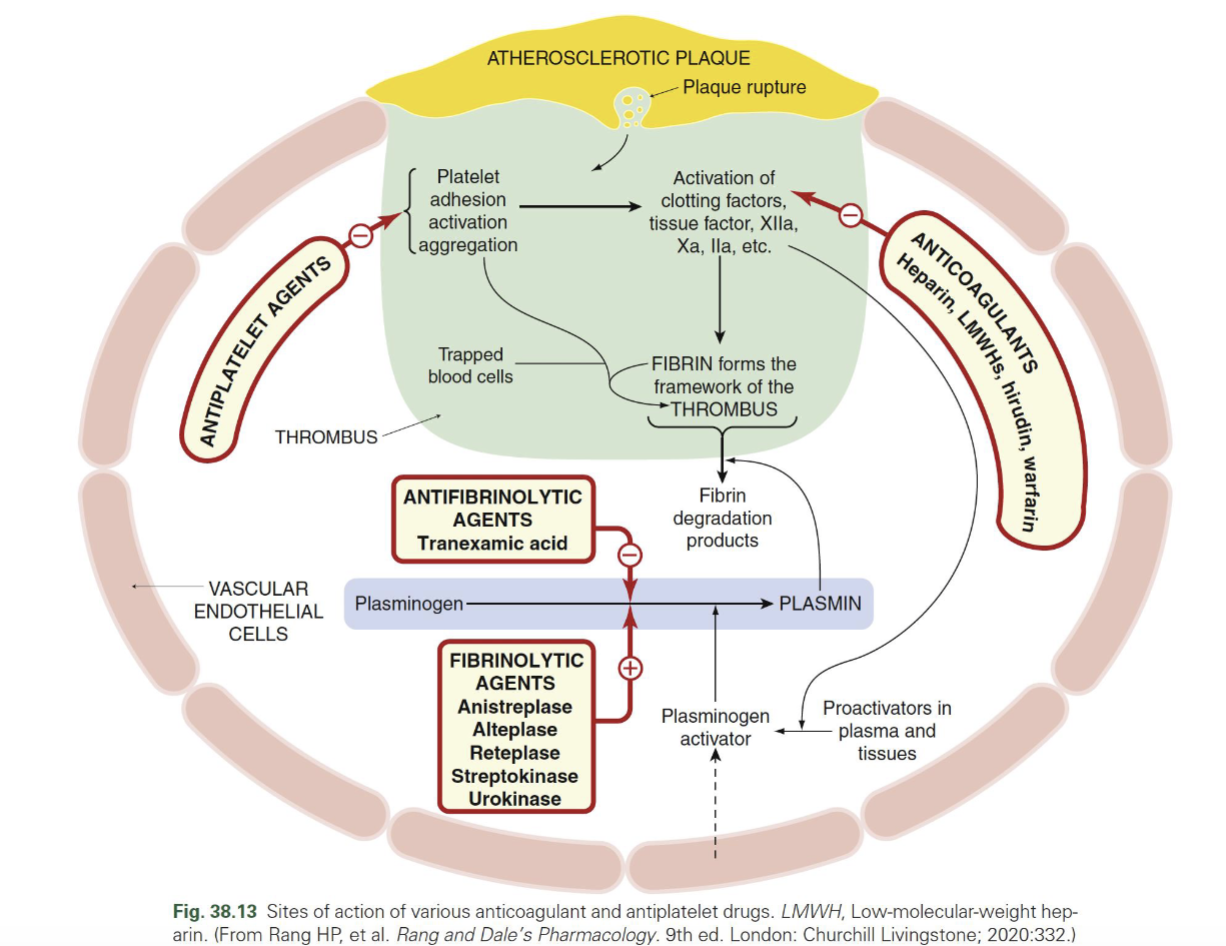
What forms the structure of a thrombus?
Fibrin = framework of thrombus
Traps blood cells → stabilizes clot
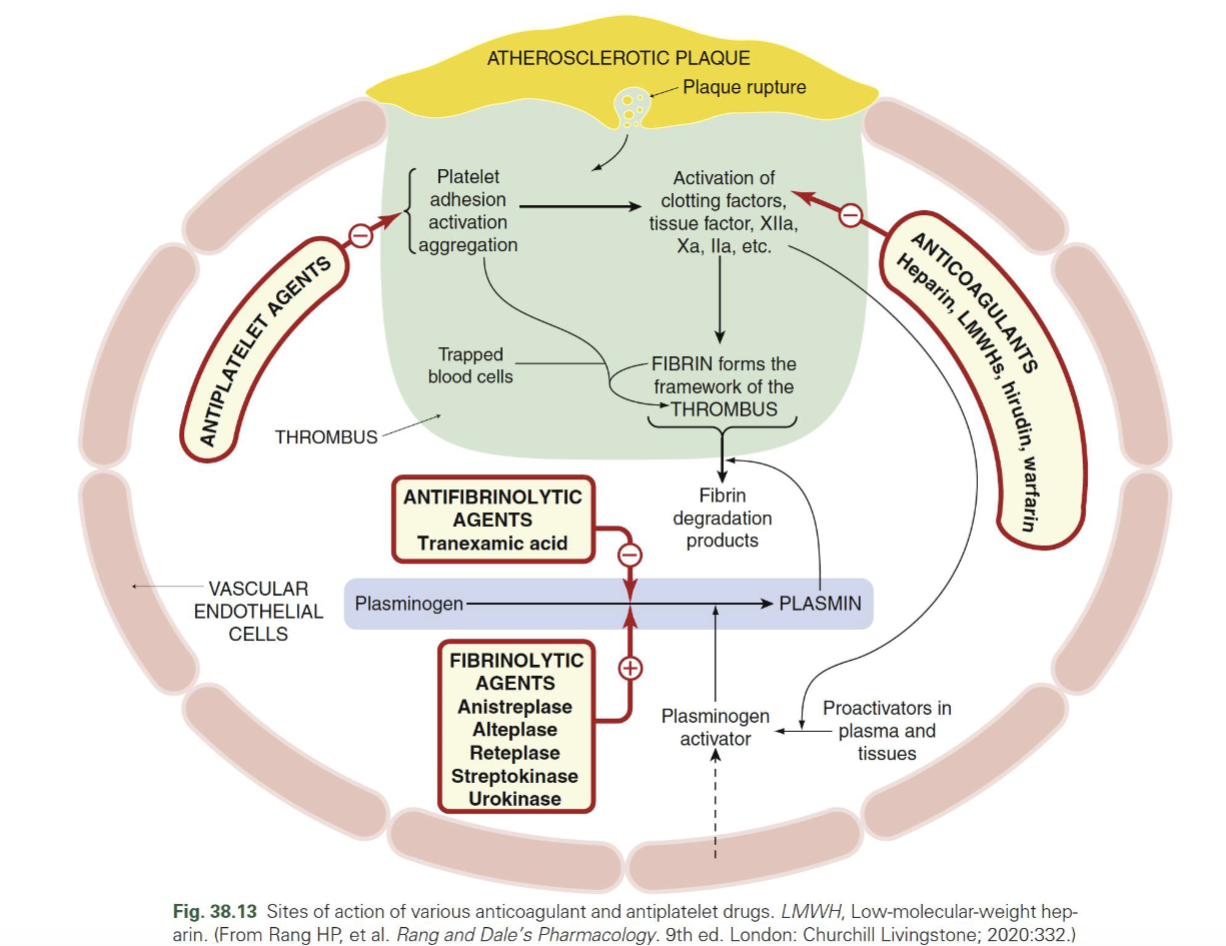
Where do antiplatelets vs anticoagulants act in thrombus formation?
Antiplatelets → inhibit platelet adhesion/activation/aggregation (early step)
Anticoagulants → inhibit clotting cascade → ↓ thrombin (IIa), Xa → ↓ fibrin formation
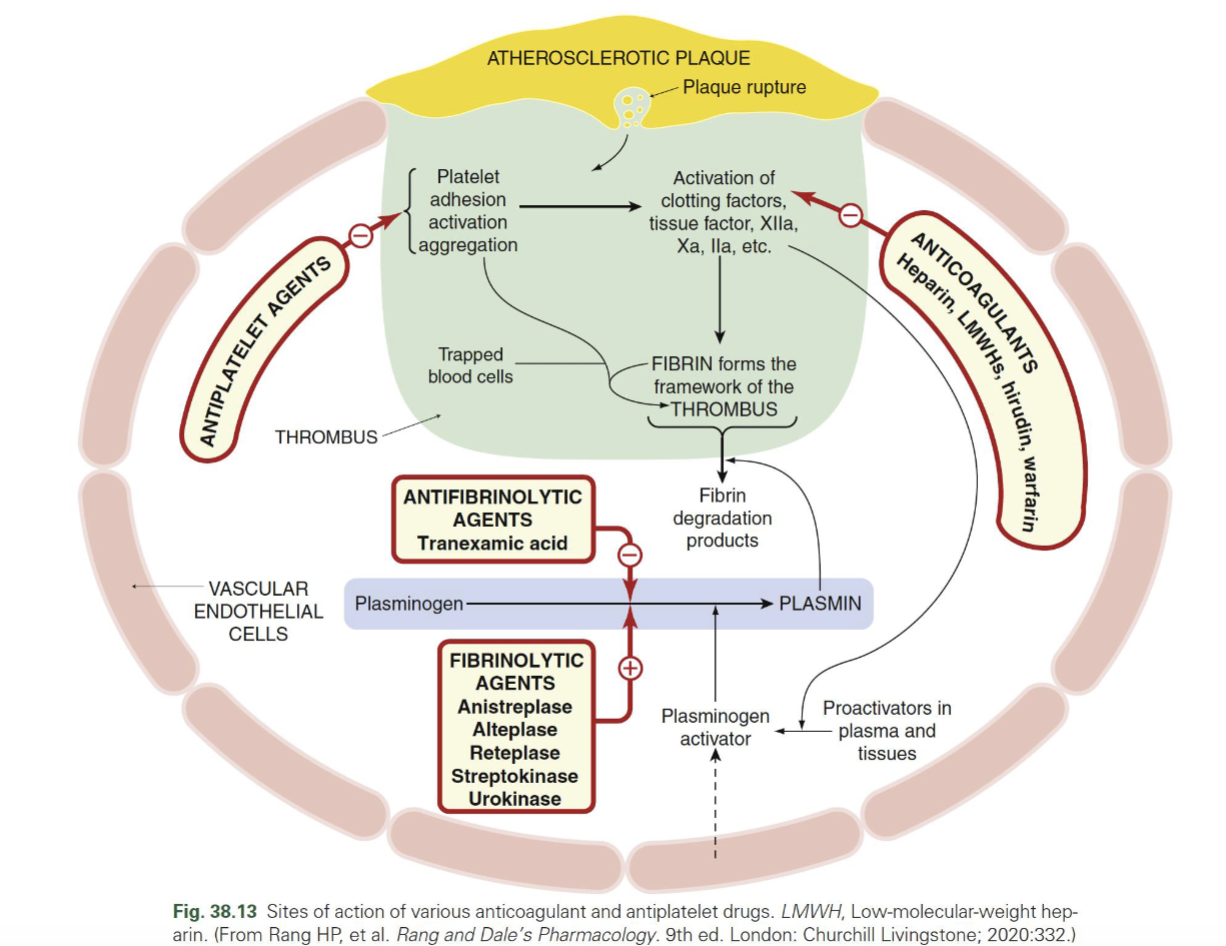
Fibrinolytics vs antifibrinolytics — MOA
Fibrinolytics (tPA, alteplase, etc.) → ↑ plasmin → break down fibrin (clot busting)
Antifibrinolytics (TXA) → inhibit plasminogen → plasmin → prevent clot breakdown
Antifibrinolytics (TXA)
inhibit plasminogen → plasmin → prevent clot breakdown
REVERSAL AGENTS (by class)
Antiplatelets (ASA, NSAIDs, clopidogrel, etc.) → Platelets
GP IIb/IIIa inhibitors → Platelets
Heparin (UFH) → Protamine (FULL)
LMWH → Protamine (PARTIAL)
Fondaparinux → NONE
Warfarin → Vitamin K, FFP, PCC
Direct thrombin inhibitor (Dabigatran) → Idarucizumab
Factor Xa inhibitors (Rivaroxaban, Apixaban, Edoxaban, Betrixaban) → Andexanet alfa
Fibrinolytics (tPA, streptokinase) → Antifibrinolytics (TXA, aminocaproic acid)
WHEN TO STOP BEFORE SURGERY
ASA → 7 days
NSAIDs → 24–48 hr
Clopidogrel → 5–7 days
Prasugrel / Ticlopidine → 7–10 days
GP IIb/IIIa inhibitors:
Abciximab → 48–72 hr
Eptifibatide / Tirofiban → 8–24 hr
Anticoags
Heparin (UFH) → 6 hr
LMWH → 12–24 hr
Fondaparinux → 2–4 days
Warfarin → 4–5 days
DOACs:
Dabigatran → 1–4 days
Rivaroxaban → 1–3 days
Apixaban / Edoxaban → 1–2 days
Betrixaban → 3–4 days
Anti-PLT
stop for neuroaxial anesthesia
NSAIDs → ✅ NO contraindication
Clopidogrel / Prasugrel / Ticlopidine → ❗ STOP 5–10 days
Ticagrelor → 5–7 days
Cangrelor → 3 hrs (IV = short)
GPIIb/IIIa inhibitors → 8–48 hrs
Cilostazol → 2 days
Dipyridamole → 24 hr
HEPARIN
neuroaxial anesthesia
LOW DOSE (5,000 units)
Do neuraxial: 4–6 hrs after dose
Remove catheter: 4–6 hrs after last dose
Restart: wait 1 hr
HIGH DOSE : Wait 12 hrs
FULL THERAPEUTIC: Wait 24 hrs
IV HEPARIN
Stop infusion → wait 4–6 hrs
Check normal coagulation
Remove catheter: 4–6 hrs
Restart: wait 1 hr
LMWH (ENOXAPARIN)
12 / 24 RULE
Prophylactic dose → wait 12 hrs
Therapeutic dose → wait 24 hrs
Catheter:
Remove ≥12 hrs after last dose
Restart LMWH → 4 hrs after removal
WARFARIN
Must have NORMAL INR before neuraxial
Remove catheter when:
INR ≤ 1.5
FONDAPARINUX
Avoid catheter (⚠ risky)
Single needle only
👉 Basically: DON’T MESS WITH IT
DIRECT THROMBIN INHIBITORS (IV)
Argatroban, Bivalirudin
👉 ❌ NO neuraxial anesthesia
DOACs (VERY TESTED) Dabigatran (Factor IIa
❌ Contraindicated
Restart → 6 hrs after
Xa inhibitors (Rivaroxaban, Apixaban, etc.)
Wait 72 hrs before neuraxial
Restart → 6 hrs after
HERBALS
No strict stop rule
BUT:
Ginkgo, Garlic, Ginseng = bleeding ris
ULTRA-HIGH YIELD SUMMARY
⏱ TIME RULES
4–6 hr → Heparin (low dose / IV)
12 hr → LMWH prophylaxis
24 hr → LMWH therapeutic
72 hr → Xa inhibitors
5–10 days → Clopidogrel group
🚫 HARD NOs
Direct thrombin inhibitors (IV)
Dabigatran (neuraxial = avoid)
Fondaparinux (avoid catheter)
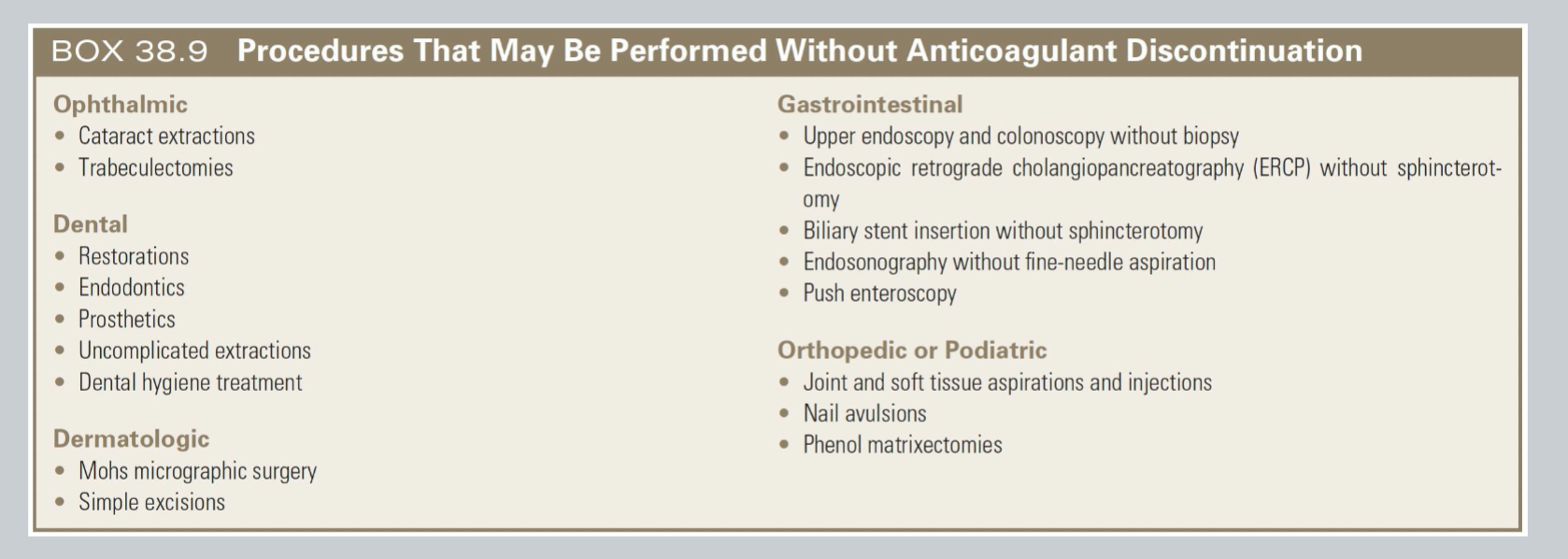
Procedures = SAFE to continue anticoagulation
Eye: Cataracts and Trabeculectomy
Dental (basic work)
Cleaning
Fillings/restorations
Root canals
Simple extraction
Skin (superficial): Mohs and Simple excisions
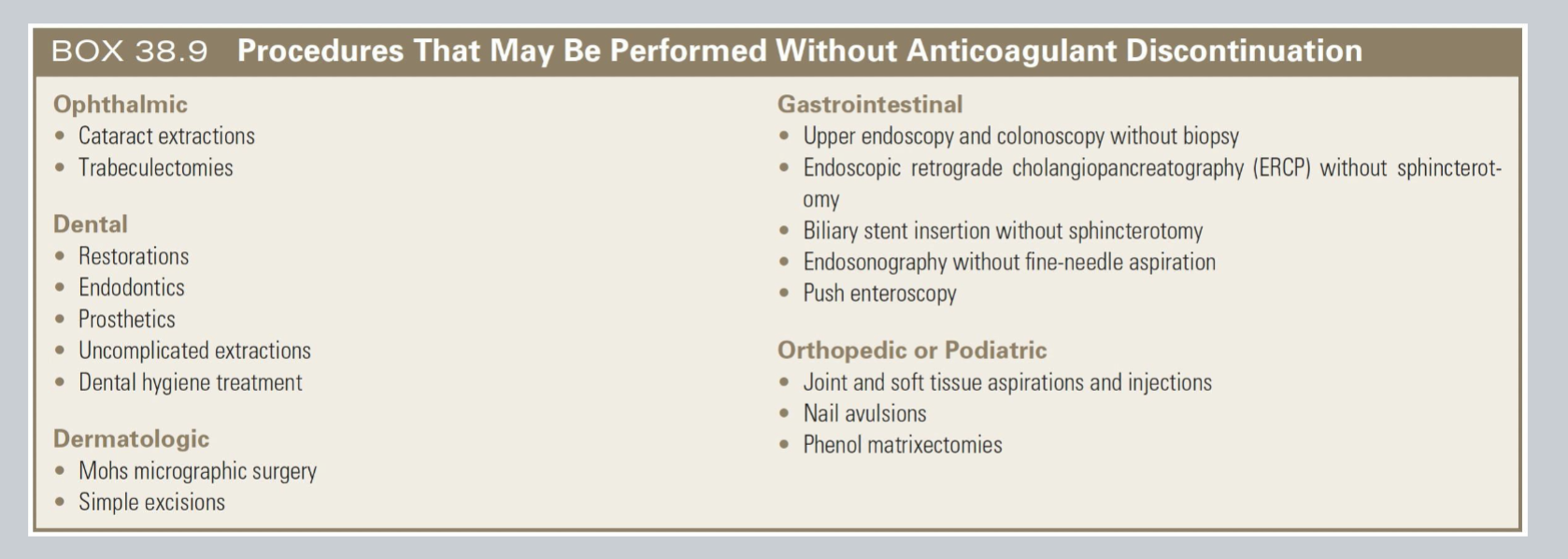
Procedures = SAFE to continue anticoagulation
GI = ONLY if NO CUTTING
If they add biopsy or sphincterotomy → STOP anticoagulation
Endoscopy / colonoscopy → ✅ ONLY if NO biopsy
ERCP → ✅ ONLY if NO sphincterotomy
Stent placement → ✅ if no cutting
Endosonography → ✅ no needle
No cutting, no biopsy, no deep tissue = continue anticoagulation
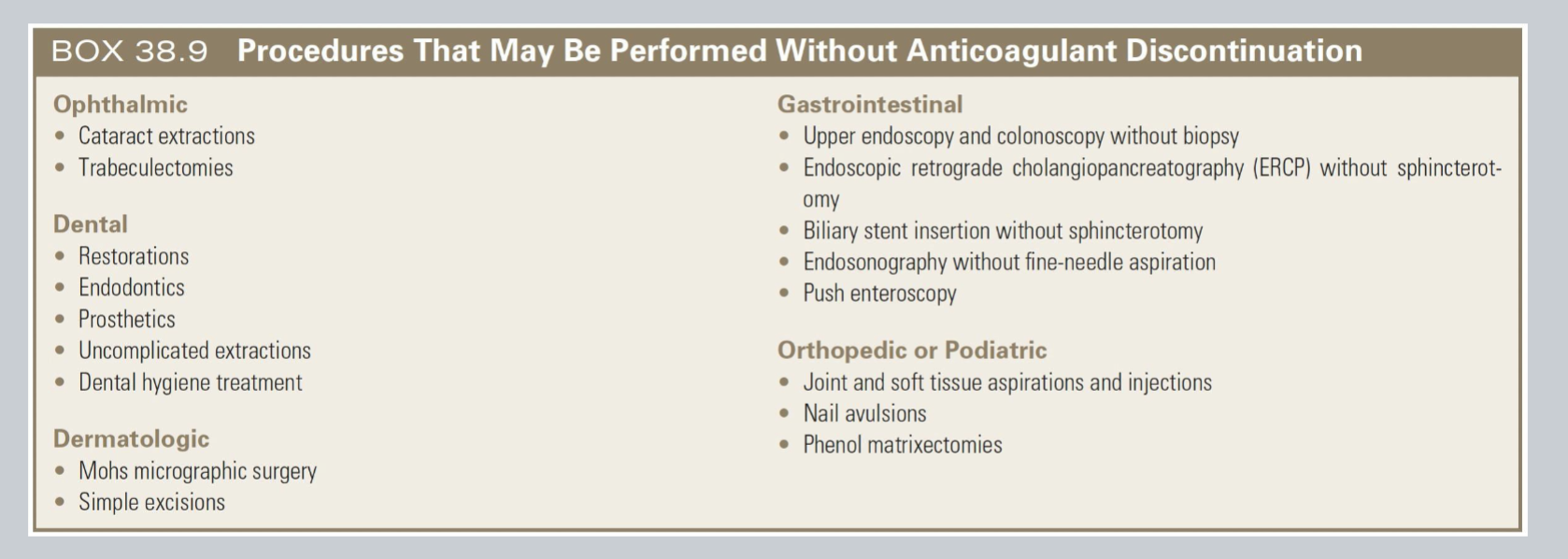
Ortho/Podiatry
» MSK procedures safe with anticoagulation
Joint injections / aspirations
Nail removal
Minor foot procedures
💉 Most commonly ordered:
Platelets → quantity
PT (INR) → extrinsic pathway (warfarin)
aPTT → intrinsic pathway (heparin)
Bleeding time → platelet function (rarely used now)
Blood availability:
Type & Screen
ABO + Rh + antibodies
“Just in case”
Type & Crossmatch
Fully matched blood ready
“We expect bleeding”
Platelet - Primary role
Primary role:
Maintain vascular integrity
Aggregate when a plug is necessary to stop bleeding
Help initiate the clotting pathways
Labs – PT
Efficiency of the extrinsic factors (III & VII) and common coagulation pathway (X, V, II, I) in generating a stable clot
Monitor oral anticoagulant therapy
Prolonged: Patient. with abnormalities or deficiency in extrinsic or common pathway factors
Not a very sensitive test
Only identifies an existing problem that may or may not cause bleeding
PLT count
Actual # of platelets present in blood per cubic millimeter
Used to monitor thrombocytopenia
Normal count: 150,000–300,000/mm³
Thrombocytopenia:
<100,000/mm³
Critical: <20,000/mm³
INR
Evaluates extrinsic and common pathway
Normal: 1.5 – 2.5
aPTT
Monitoring of heparin therapy
Factor concentration ↓ 30% = prolong PT or aPTT
Intrinsic coagulation pathway (factors XII, XI, IX, VIII) and common coagulation pathway
Identify abnormalities in all factors except III and VII
“WHAT TO GIVE”
Platelet problem? → Platelets
Factor problem? → FFP
Fibrinogen low? → Cryo
Heparin? → Protamine
vWD? → DDAVP
↑ aPTT ONLY
Heparin / Hemophilia
Cause: Factors VIII, IX, XI or heparin
💉 Treatment:
👉 Protamine (if heparin)
👉 FFP (if factor deficiency)
↑ PT ONLY
Issue with Factor VII / Warfarin
💉 Treatment:
👉 FFP
↑ PT + ↑ aPTT
BIG PROBLEM (multiple factors)
Causes:
Liver disease
Warfarin overdose
Severe deficiency
💉 Treatment:
👉 FFP ± cryo ± protamine
↑ BT (bleeding time)
Platelet PROBLEM
If platelet COUNT ↓ 👉 Thrombocytopenia. » 💉 Give: Platelets
If platelet COUNT normal
👉 Platelet dysfunction (ASA, NSAIDs) » 💉 Give: Platelets
↑ BT + ↑ aPTT
👉 Think: von Willebrand disease
👉 Desmopressin (DDAVP)
👉 ± Cryoprecipitate
LOW FIBRINOGEN
Cryo problem
💉 Treatment:
👉 Cryoprecipitate ± FFP
EVERYTHING ABNORMAL💀💀💀💀
DIC / liver failure
↑ PT, ↑ aPTT, ↑ BT, ↓ platelets, ↓ fibrinogen
💉 Treatment: FFP + Platelets + Cryo
↑ aPTT only (no bleeding)
Cause: Factor VIII deficiency, heparin, lupus anticoagulant, poor sample
Treatment: No treatment
↑ aPTT only + bleeding
Cause: Factors XI, IX, VIII deficiency or heparin
Treatment: FFP; protamine if heparin
↑ aPTT + ↑ PT
Factors V, X, II, dysfibrinogenemia, heparin, coumarins
Tx: FFP, cryoprecipitate, protamine
↑ PT only
Factor VII
Tx: FFP
↑ aPTT only due to heparin
Cause: Heparin therapy
Treatment: Protamine
↑ aPTT + ↑ BT
von Willebrand disease
Tx: Desmopressin acetate, cryoprecipitate
↑ aPTT + ↑ PT + ↑ BT + ↓ fibrinogen
Hypofibrinogenemia
Tx: FFP, cryoprecipitate
↑ BT + ↓ platelet count
Thrombocytopenia
Tx: Platelet concentrate (8–10 units)
↑ BT (platelet count normal)
Thrombocytopathy, aspirin, NSAIDs
Tx: Platelet concentrate
↑ aPTT + ↑ PT + ↑ BT + ↓ platelets + ↓ fibrinogen
DIC, severe liver disease, dilutional coagulopathy
Tx: FFP, cryoprecipitate, platelet concentrate, whole blood
Recognize and efficiently control blood loss
• Hemodynamics
• Surgical site
• Sponges
• Canisters
• OR floor
Most commonly transfused blood components
RBCs
Platelets
FFP
Cryoprecipitate