Week 11: Musculoskeletal system alterations
1/117
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
118 Terms
Differences in skeletal system of children
More cartilage
More porous
Heal faster
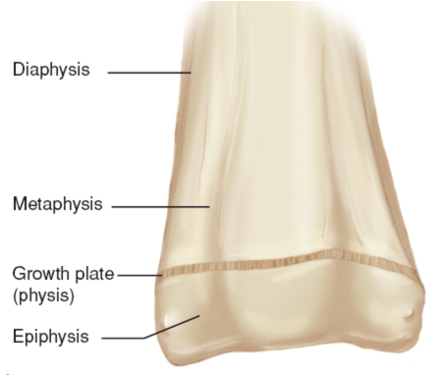
Growth plates — epiphyses (separated from main portion of bone by cartilage)
Sutures on skull
Growth of long bones occurs at the ____
epiphyses
Muscle development pattern
grows top, down, and then out
heads are larger at younger ages
Physiological effects of immobilization: musculoskeletal (2)
Bone demineralization
Muscle atrophy
Physiological effects of immobilization: metabolic
Decreased metabolic rate — slowing of all systems
Decreased production of stress hormones
Effect of decreased metabolic rate on food intake and consequences d/t immobilization
Decreased food intake
decline in nutritional state
impaired healing
electrolyte imbalance
Effect of decreased production of stress hormones d/t immobilization
decreased physical and emotional coping capacity
Physiological effects of immobilization: respiratory
decreased chest and lung expansion
decreased need of O2
mechanical/biochemical secretion retention
Results of decreased chest and lung expansion d/t immobilization
diminished O2 intake
dyspnea and inadequate O2 saturation
acidosis
Results of mechanical/biochemical secretion retention r/t immobilization
pneumonia
atelectasis
Physiological effects of immobilization: cardiovascular
decreased efficiency of orthostatic neurovascular reflexes
venous stasis
Consequences of decreased efficiency of orthostatic neurovascular reflexes d/t immobilization
inability to adapt readily to upright position — orthostatic intolerance
pooling of blood in extremities in upright posture
Physiological effects of immobilization: skin
altered tissue integrity
d/t decreased circulation and pressure leading to injury
difficulty with personal hygiene
Physiological effects of immobilization: elimination
abdominal distention d/t poor abdominal muscle tone
alteration in gravitational force (difficulty voiding in prone position)
impaired ureteral peristalsis (urine retention, bladder infection, renal calculi)
Consequences/complications of abdominal distention caused by poor abdominal muscle tone d/t immobilization
Difficulty feeding in prone position
Interference with respiratory patterns
Constipation/anorexia
What is the most common fracture site in childhood?
distal forearm
radial/ulna
Why do kids heal faster than adults when they get a bone fracture?
d/t more blood supply to bones
Fracture healing time for a neonate
2-3 weeks
Fracture healing time in early childhood
4 weeks
Fracture healing time in later childhood
6-8 weeks
Fracture healing time for an adolescent
8-12 weeks
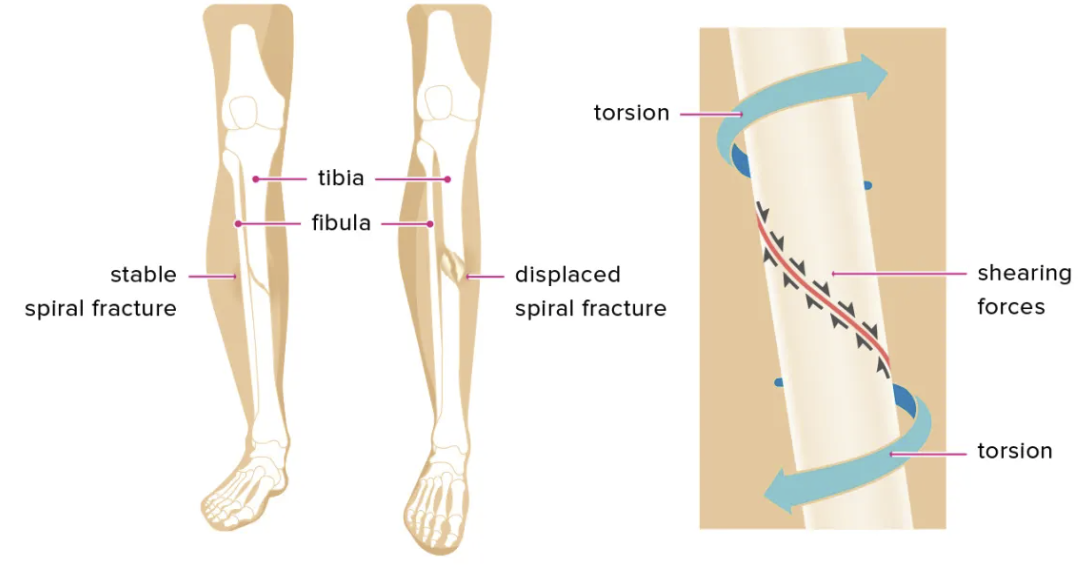
Spiral fracture
a strong twisting force of a long bone that results in a complete fracture
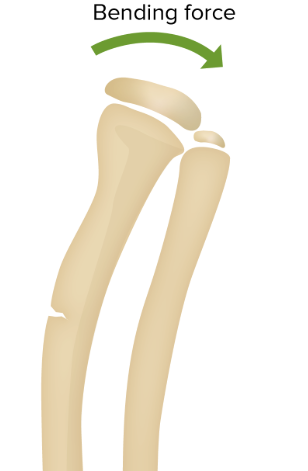
Bend fracture
when a bone bends and cracks on one side without fully breaking
Buckle fracture
a porous bone is compressed and rather that breaking, it bends and buckles, resulting in a raised area

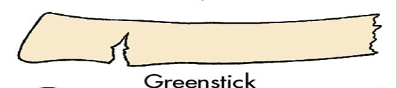
Greenstick fracture
incomplete broken bone d/t bending
Symptoms of fracture
Swelling
Pain/point tenderness
Deformity
Limited ROM
Open wound for ecchymosis
Limp or refusal to use limb
Acute fracture treatment goals (4)
Regain alignment
Retain alignment and length
Restore function of injured parts
Prevent further damage
Acute treatment of a fracture: heat application purpose (3)
warm muscles
vasoodilate
relieve inflammation and pain
Acute treatment of a fracture: cold application purpose (3)
vasoconstriction
prevents swelling, edema, and pain
decreases O2 needs
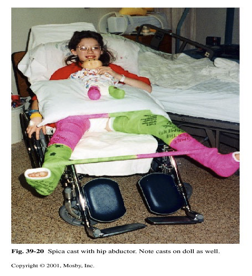
Spica cast
cast used to stabilize the hip or femur in infants and children after surgery for hip dysplasia or femur fractures
never use bar to reposition
6 P’s of a neurovascular assessment
Pain (not improved w/ pain meds)
Pulse
Pallor
Paresthesia (tingling/burning)
Paralysis
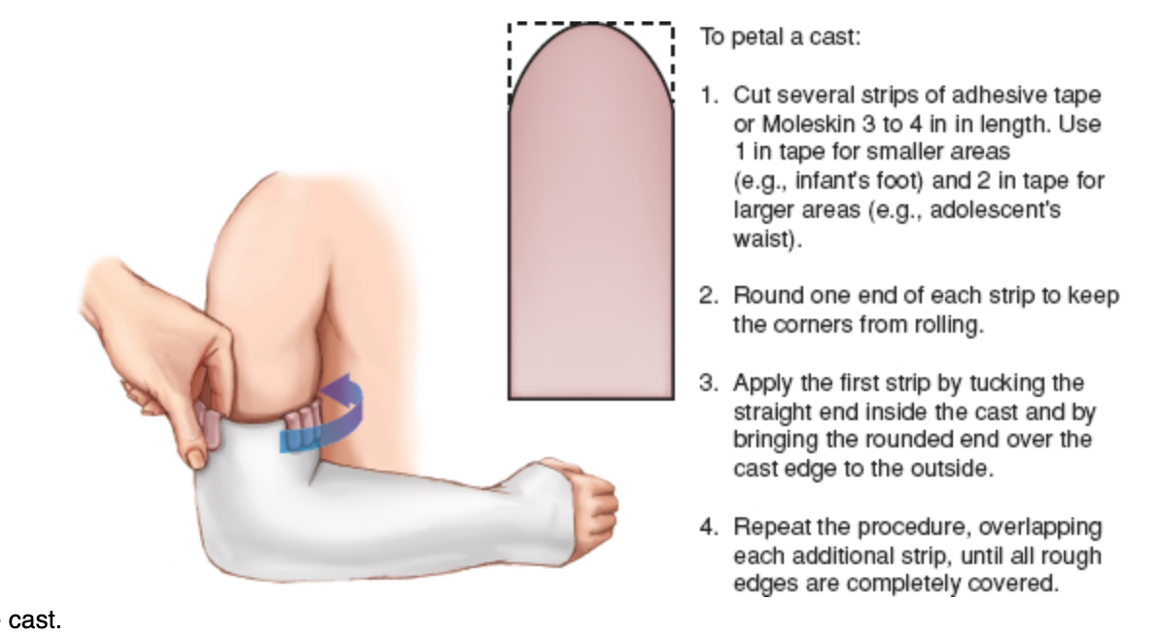
Cast skin care
line edges with moleskin or plastic line perianal to prevent skin damage
Talipes equinovarus
clubfoot
Clubfoot
congenital birth defect where a baby's foot is twisted inward and downward

Clubfoot deformities of foot (6)
Forefoot adduction
Midfoot supination
Hindfoot varus
Ankle equinis
Inversion of heel
Plantar flexion
Clubfoot signs/symptoms
Foot turned inward and down
Tight calf muscle
Rigid achilles tendon
Toe walking
Clubfoot treatment
Ponseti method
Surgery
Exercises, splits, and special shoes can be prescribed
Ponseti method for clubfoot
uses gentle, weekly serial casting to gradually correct foot deformity, followed by bracing to maintain proper alignment and prevent relapse
Clubfoot surgery
May require surgery to release tendons, reposition bones, reconstruct parts if sufficient correction not achieved in 3-6 months
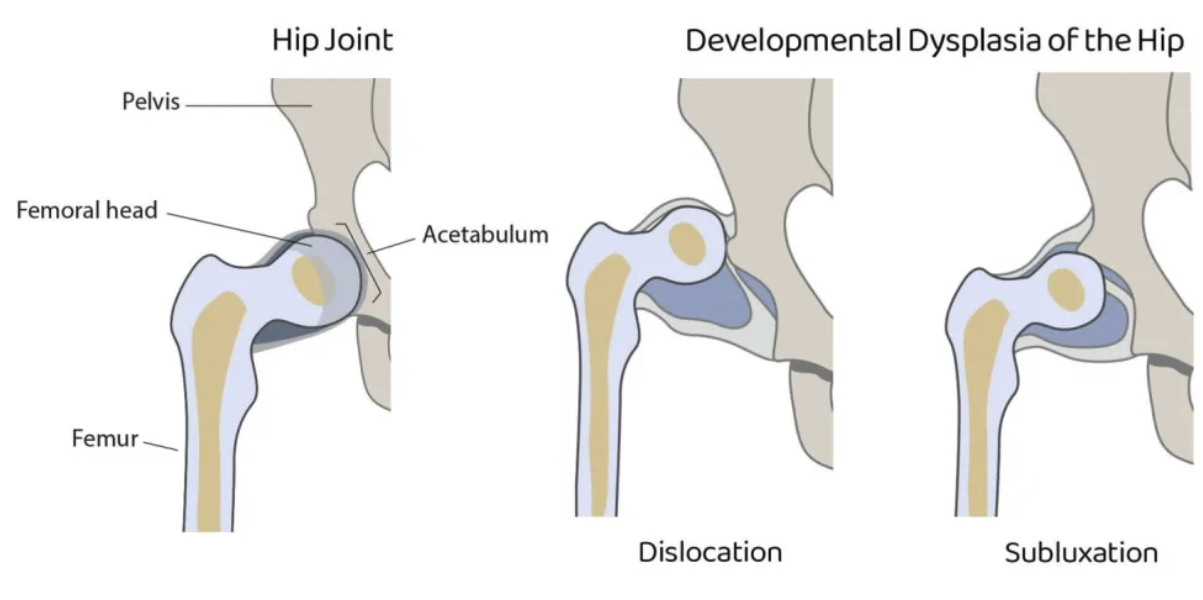
Developmental Dysplasia of the hip
A condition where the hip joint is improperly formed, causing the femoral head to be unstable, partially dislocated, or fully dislocated from the acetabulum
Developmental Dysplasia risk factors (7)
Maternal hormones
Oligohydraminos (low amniotic fluid)
Genetics
Multifetal birth
LGA
Swaddling of hips in extension or adduction
Female sex
Developmental Dysplasia signs and symptoms (4)
uneven thigh/buttock skin folds
one leg appearing shorter
limited flexibility or inability to spread legs (abduction)
clicking or popping sound during movement
If the first-born child has DDH, what is the screening recommendation for future siblings?
all siblings born after DDH child will need screening because family hx increases risk 10x
DDH diagnostics
Ortolani and Barlow maneuvers (feeling/listening for a click/clunk)
Galeazzi sign
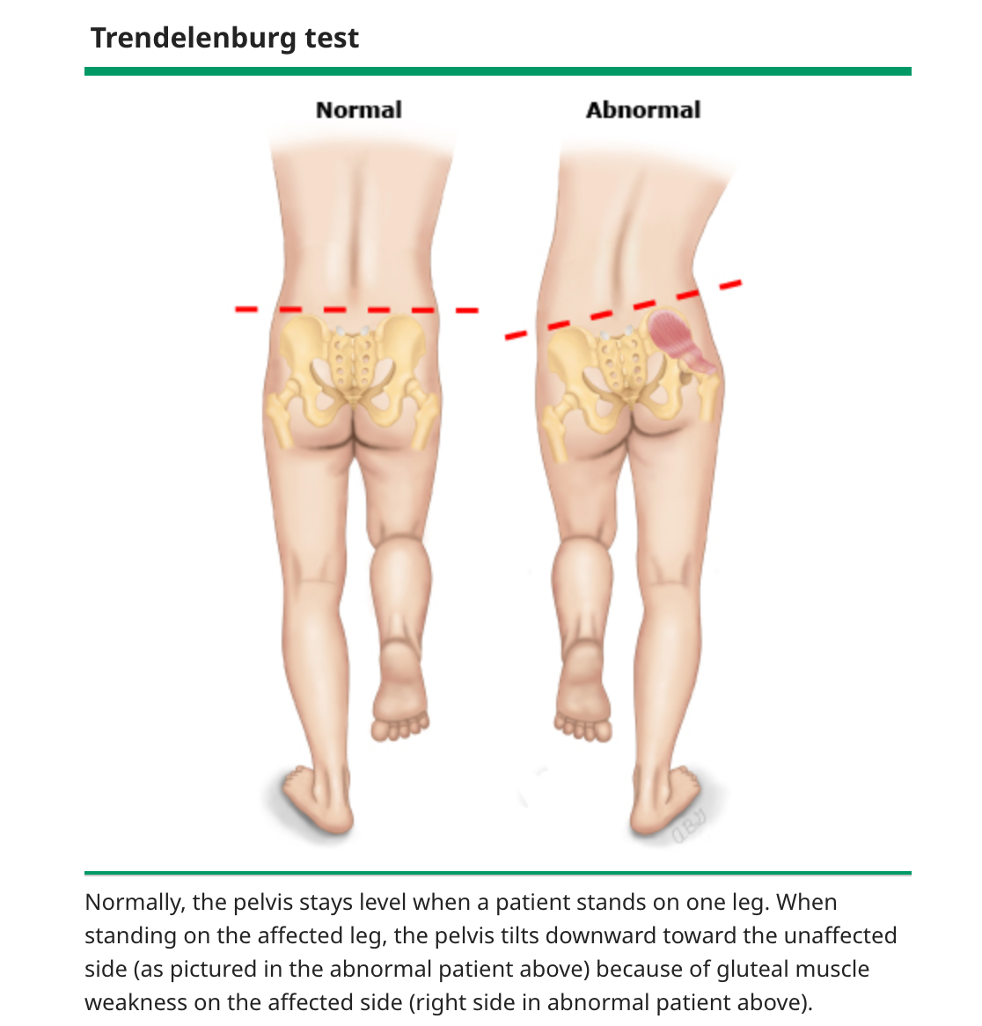
Trendelenburg sign
X-ray if >4 months
Ultrasound
Galeazzi sign
A clinical test for hip dislocation where, with the infant lying supine and knees flexed, one knee appears lower than the other, indicating possible developmental dysplasia of the hip (DDH)

Trendelenburg sign
A clinical finding where the pelvis drops on the unaffected side when standing on one leg, indicating weakness of the hip abductors (gluteus medius/minimus) on the weight-bearing side
DDH treatment
< 6 months
> 6 months
> 24 months
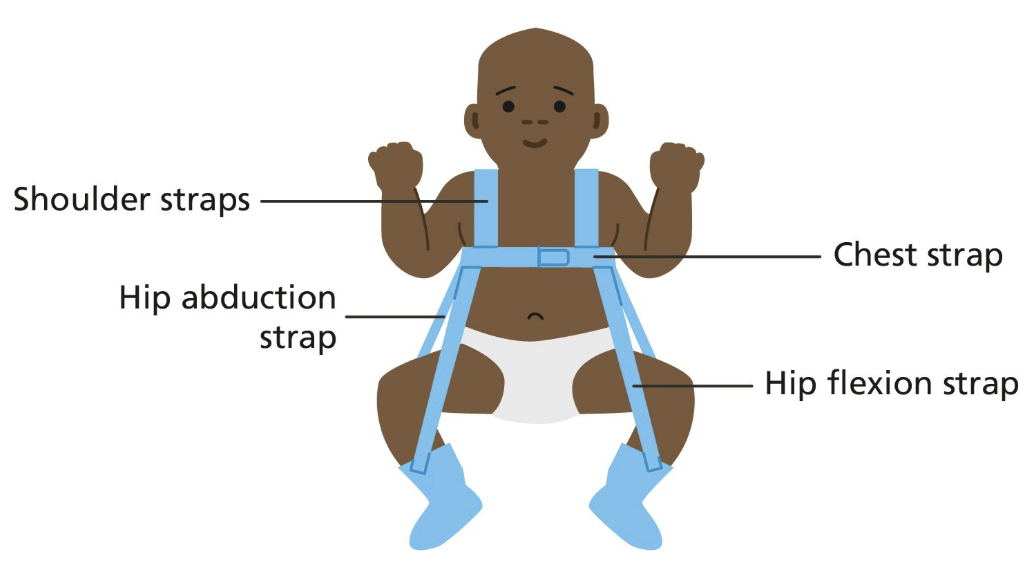
< 6 months: Pavlik harness
> 6 months: traction with manual reduction and hip spica cast after
> 24 months: reduction surgery with casting
Pavlik Harness
A brace that keeps an infant’s hips flexed and abducted to treat DDH and maintain proper hip alignment
Osteogenesis Imperfecta
brittle bone disease d/t less collagen production in the bone, teeth, skin, tendons, and parts of the eye
Osteogenesis Imperfecta signs and symptoms (6)
Blue sclera
Poor teeth development
Short stature
Progressive skeletal deformity
Joint laxity
Deafness
OI type 1
mildest and most common form
most fracture occur before puberty
normal life expectancy
OI type 2
severe/lethal form that is often fatal
multiple fractures at birth
underdeveloped lungs
OI type 3
severe form with extreme bone deformities
frequent fractures
short stature
shortened life expectancy
OI type 4
Similar to type 1 but is a moderate form d/t:
Short stature
Bone deficiencies
OI treatment
drugs
supportive care — must be careful handling patient to prevent fractures (even taking BP)
OI drug
Bisphosphonate therapy
Bisphosphonate therapy purpose
Promote bone density
Prevent fractures
Mostly helps spine
Muscular Dystrophy (MD)
genetic disorder causing gradual degeneration of muscle fibers characterized by progressive weakness of skeletal muscles, increased fatting infiltration, and elevated creatinine/kinase
Most common type of MD
Duchenne MD
How is MD inherited?
Sex-linked recessive
affects only males
MD occurs when a gene on an X chromosome fails to make the protein _____
dystrophin
Dystrophin absence r/t MD
absence of dystrophin inhibits muscle cell function
degeneration of muscle fibers
progressive weakness and wasting of skeletal muscles
MD is more common in people with have _______ _______
neurodevelopmental disorders
e.g., autism/intellect disability
Muscular Dystrophy signs and symptoms
Children often late in learning to walk
Preschooler may seem clumsy and fall often
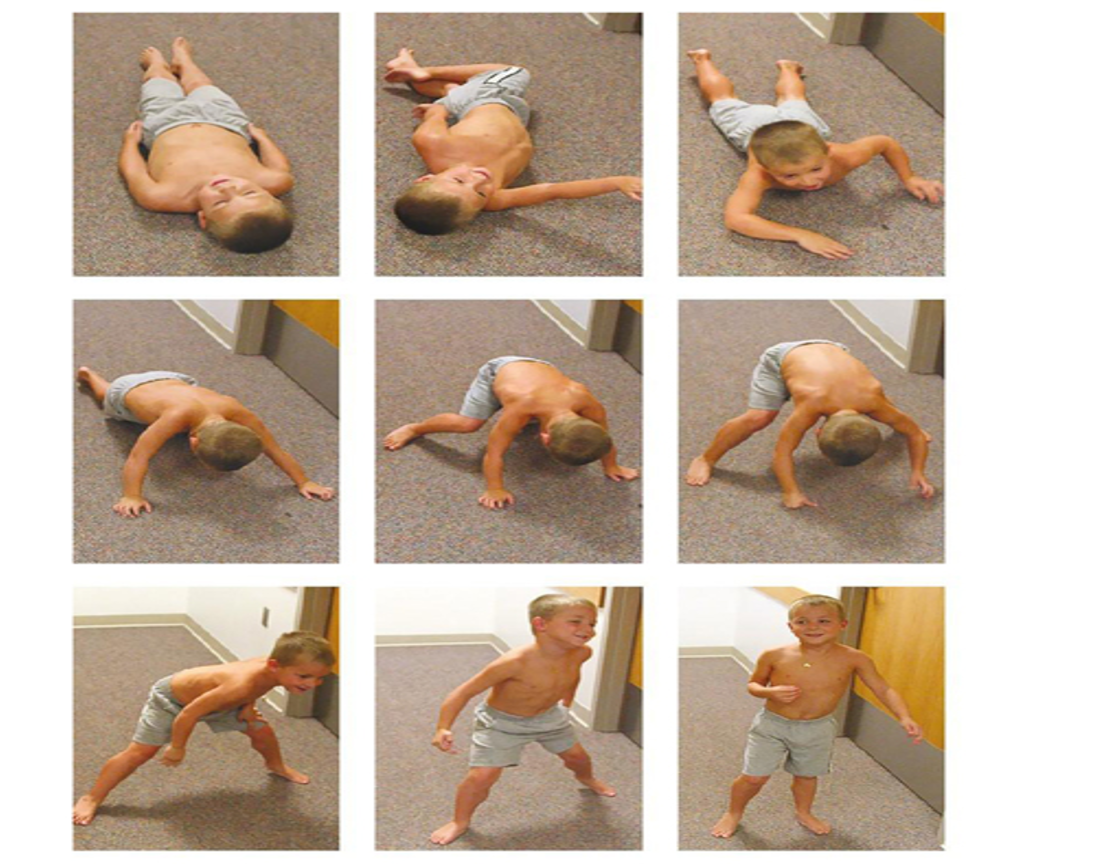
Trouble climbing stairs, getting up from floor (uses Gower maneuver)
By school age has waddling and unsteady gait d/t weak pelvic muscles
Tries to keep balance by sticking belly out and shoulders back
When do kids with MD lose the ability to walk?
7-13 y/o
Gower’s Maneuver
A sign of proximal muscle weakness where a child uses their hands to “climb up” their legs to stand from a sitting or lying position
MD complications (7)
*Mobility
Hip and knee contractures + foot deformities
Scoliosis / lordosis
Nutritional concerns
Inability to feed self / can’t chew
Hypoventilation — difficulty coughing / airway clearance
Cardiac failure
Most common cause of death in MD patients and when it occurs
cardiac failure in late 20s-30s
MD cardiac failure prevention
digoxin
MD nutrition
will eventually loose ability to chew — risk to aspirate and will need an enteral source
monitor calories
as fine motor and gross motor abilities decline, self feeding becomes difficult
MD respiratory interventions
hypoventilation d/t weakness
cough assist machines, CPT, or vests may be required
CPAP/Trach
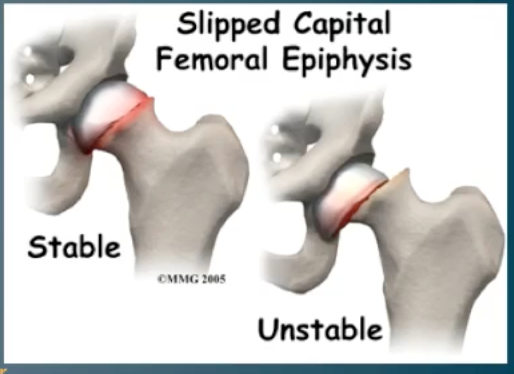
Slipped Capital Femoral Epiphysis (SCFE)
Gradual displacement / slippage of the femoral head at the growth plate, causing hip pain and limp in adolescents
SCFE age
10-15 y/o
occurs during/before puberty
SCFE is more common in what groups? (3)
Obese children
Adolescents
Boys
SCFE signs and symptoms (5)
Pain in hip toward groin, thigh, or knee that is worse with activity
Limp (progresses)
External rotation of affected hip
Loss of hip flexion, abduction, and internal rotation
Obesity / growth spurt
SCFE diagnostics (2)
Xray
MRI
SCFE complications (4)
Acute necrosis of the hip cartilage
Femoroacetabular impingement
Avascular necrosis of the femoral head
Later concerns of degenerative hip arthritis as an adult
SCFE treatment
Is an emergency once diagnosed, requiring:
bedrest
surgical fixation
immobilization/spica casting/traction to keep hip completely still
SCFE treatment goals
Prevent avascular necrosis of hip
Early gait training
Pin/screw inserted across growth plate to secure femoral head
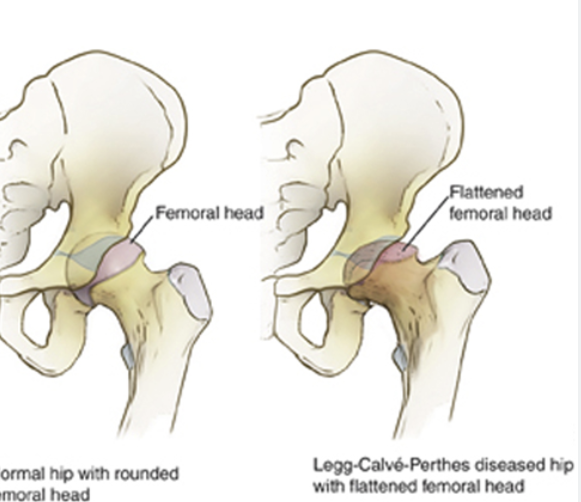
Legg Calve-Perthes Disease (LCP)
A condition where temporary loss of blood supply to the femoral head causes bone death, leading to hip pain, limp, and limited motion in children
LCP affected ages
2-12 y/o
Avascular necrotic head
Loss of blood supply to the femoral head leading to bone death and collapse
Legg Calve-Perthes Disease: stage 1
Decreased blood supply → early bone death
avascular necrosis of the femoral head
Legg Calve-Perthes Disease: stage 2
Fragmentation
Femoral head breaks down and is resorbed
Legg Calve-Perthes Disease: stage 3
Reossification
New bone begins to form
on xray it looks like increased bone density in area
Legg Calve-Perthes Disease: stage 4
healing and fuller remodeling
gradual reforming of head
occurs until compete recovery
LCPD treatment goals (4)
eliminate hip irritability/inflammation
restore and maintain adequate hip ROM
prevent capital femoral epiphyseal collapse, extrusion, or subluxation
ensure a well-rounded femoral head at the time of healing
LCPD treatment methods
Non-surgical (3)
Surgical
Non-surgical
NSAIDs
PT
Potential casting/abduction bracing
Surgical
Osteotomy
LCPD vs SCFE: ages
LCPD: 4-8 y/o
SCFE: 10-15 y/o
LCPD vs SCFE: body size
LCPD: typically shorter in stature
SCFE: typically overweight
LCPD vs SCFE: physiology
LCPD: deformity of femoral head
SCFE: displacement of femoral head
LCPD vs SCFE: primary treatment method
LCPD: conservative
SCFE: operative
LCPD vs SCFE: surgery
LCPD: femoral osteotomy (avoided if possible)
SCFE: usually involves internal fixation with a screw
Osgood-Schlatter Disease (OSD)
Overuse injury causing inflammation and pain at the knee in adolescents
anterior tibial tuberosity
benign
OSD exacerbations (2)
*Rapid growth spurts
Sports
When does OSD typically resolve?
once growth plate ossifies
OSD treatment
PT to strengthen quad and hamstring
Ice
NSAIDs
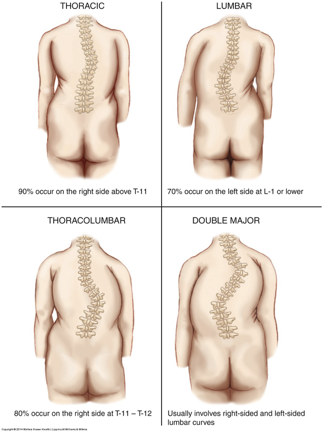
Scoliosis
lateral curvature of the spine
causes rib asymmetry
Scoliosis classifications by age
Congenital = during fetal development
Infantile = birth to 3 y/o
Juvenile = 3-10 y/o
Adolescent >10 y/o
Scoliosis types (3)
Idiopathic
Neuromuscular (e.g., NTDs, CP, MD)
Congenital