Chapter 4, Legal and Ethical Considerations of Providing Care, Wednesday, May 27th
1/31
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
32 Terms
Introduction
Understanding medical, legal, and ethical issues is an essential foundation for all emergency care.
You will learn information to reduce or prevent the legal liability you may face as a result of calls.
Lawsuits are commonplace (providers are RARELY sued)
Much of EMS work takes place in the public eye
Choices and actions influence risk of being sued
Know how the law affects EMS providers
Scope of Practice
The collective set of regulations and ethical considerations that define the extent and limits of an EMT’s job.
Defined by
national standards
state legislation
medical direction
Communicated in protocols, standing orders
Rules and guidelines differ from state to state and region to region.
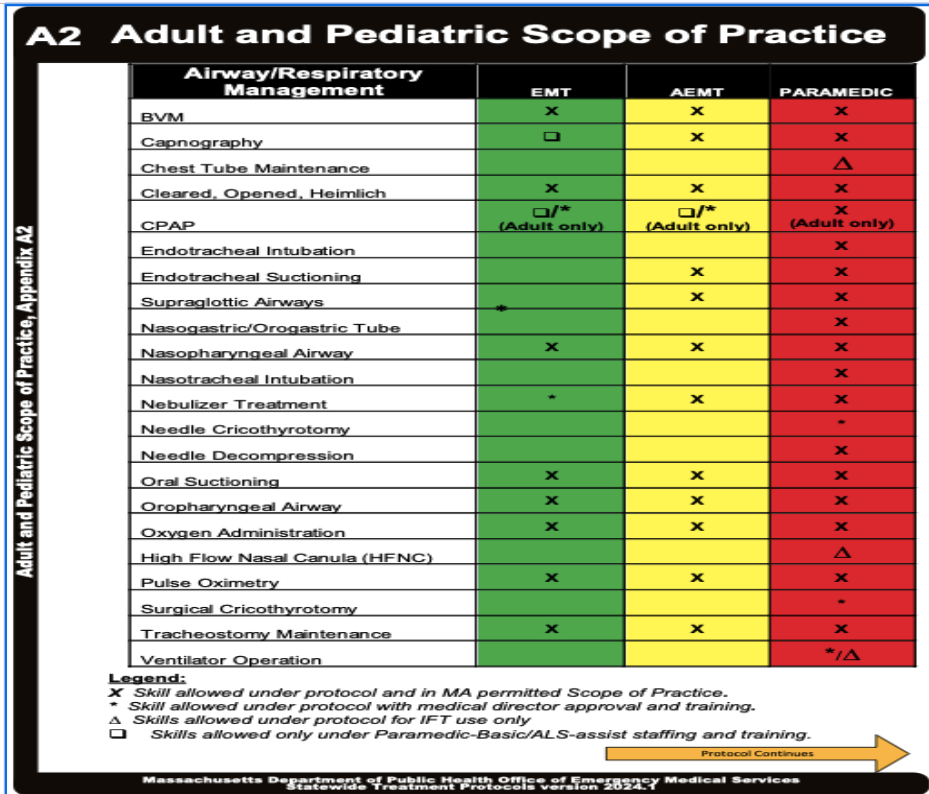
Adult and Pediatric Scope of Practice
Airway Respiratory Management
1. Oxygen AdministrationWhat it is:
Providing supplemental oxygen via nasal cannula or non-rebreather mask.
When to use:
Shortness of breath
Asthma
COPD exacerbation
Pneumonia
Pulmonary edema
Chest pain with hypoxia
Trauma with low oxygen saturation
Carbon monoxide exposure
Signs you should act:
SpO₂ < 94% (or per protocol)
Cyanosis
Increased work of breathing
Altered mental status from hypoxia
Example:
70-year-old with pneumonia:
RR 32
SpO₂ 87%
→ Administer oxygen immediately.
2. Pulse OximetryWhat it is:
Measures oxygen saturation.
When to use:
Almost every respiratory complaint.
Example:
Patient says:
"I feel fine."
But pulse ox shows:
SpO₂ = 82%
This tells you the patient is actually hypoxic.
3. Nasopharyngeal Airway (NPA)What it is:
Soft rubber tube inserted through the nose.
Purpose:
Keeps airway open.
Use when:
Patient has:
Decreased LOC
Intact gag reflex
Example:
Overdose patient:
Breathing spontaneously
Semi-conscious
Gag reflex present
→ NPA is appropriate.
Do NOT use if:
Severe facial trauma
Suspected basilar skull fracture
4. Oropharyngeal Airway (OPA)What it is:
Rigid airway inserted into mouth.
Purpose:
Prevents tongue from blocking airway.
Use when:
Patient:
Unresponsive
No gag reflex
Example:
Cardiac arrest patient
Unresponsive
No gag
→ Insert OPA.
Never use:
Awake patient.
They will gag and potentially vomit.
5. Oral SuctioningPurpose:
Removes secretions, blood, vomit.
Use when:
Airway is obstructed by:
Vomit
Blood
Secretions
Example:
Seizure patient with vomit in airway.
Suction first before ventilation.
Airway always comes before oxygen.
6. BVM (Bag-Valve Mask)What it is:
Provides positive pressure ventilations.
Use when:
Patient is not breathing adequately.
Signs:
Adult:
RR < 8
RR > 30 with poor tidal volume
Child:
Severe respiratory failure
Example:
Opioid overdose:
RR 4
Cyanotic
→ Begin BVM ventilations immediately.
7. CPAPPurpose:
Pushes air into lungs using continuous pressure.
Best for:
CHF/Pulmonary edema
COPD exacerbation
Severe respiratory distress
Patient must:
Be awake
Follow commands
Maintain own airway
Example:
CHF patient:
Pink frothy sputum
Crackles
SpO₂ 84%
→ CPAP can dramatically improve oxygenation.
Do NOT use:
Vomiting patient
Unconscious patient
Significant hypotension
8. Nebulized AlbuterolPurpose:
Bronchodilator
Opens constricted airways.Use for:
Asthma
Wheezing
COPD
Example:
16-year-old asthma patient:
Audible wheezing
Difficulty speaking
→ Nebulized albuterol.
9. Supraglottic Airway (EMT Assist)Purpose:
Advanced airway placed above vocal cords.
Usually placed by ALS.
EMT may assist.
Use when:
Cardiac arrest
Severe airway compromise
Airway Decision Making
Think:
Is the airway open?
No:
Jaw thrust
Head tilt chin lift
OPA/NPA
Is the airway dirty?
Yes:
Suction
Is the patient oxygenating?
No:
Oxygen
CPAP
BVM
Is the patient ventilating?
No:
BVM immediately
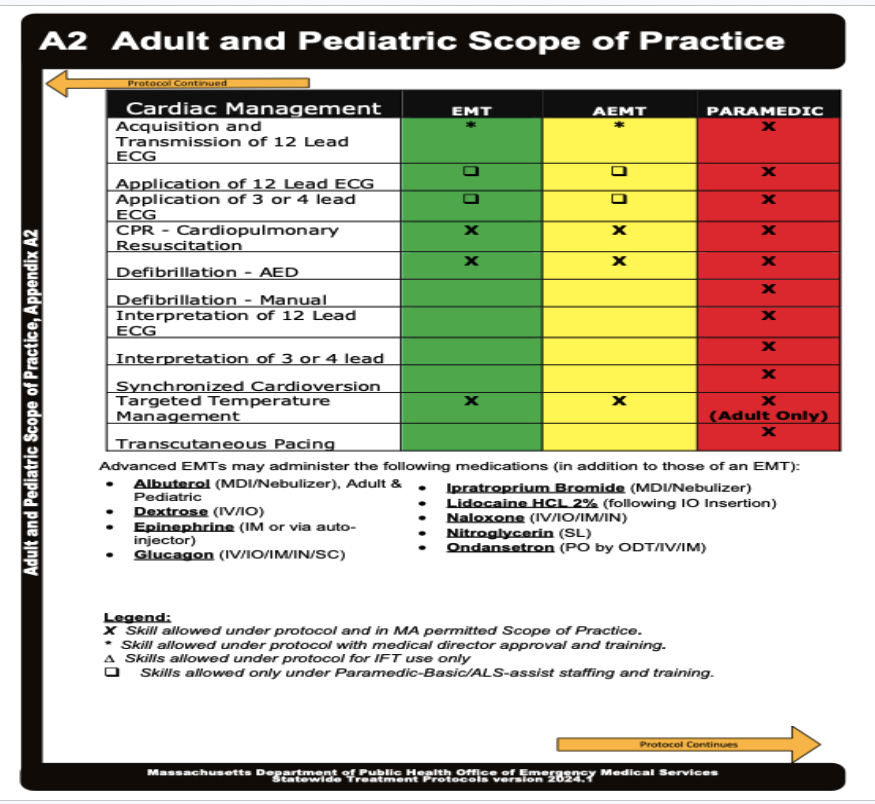
Cardiac management
1. CPRUse when:
Patient:
Unresponsive
Not breathing normally
Pulseless
Example:
You find:
No pulse
Agonal respirations
→ Start CPR immediately.
2. AEDPurpose:
Detects shockable rhythms.
Use:
Any cardiac arrest patient.
Example:
Patient collapses at mall.
No pulse
Not breathing
→ CPR
→ Attach AED ASAP
Follow prompts.
3. Temperature ManagementPurpose:
Prevent worsening injury.
Hyperthermia
Use:
Cooling measures
Examples:
Heat stroke
Hypothermia
Use:
Blankets
Warm environment
Examples:
Cold-water drowning
4. 3-Lead ECG (Assist)Purpose:
Continuous cardiac monitoring.
Use:
Chest pain
Palpitations
Syncope
Allows ALS to watch rhythm continuously.
5. 12-Lead ECG (Assist/Acquire)Purpose:
Detect STEMI.
Use:
Chest pain patients.
Example:
55-year-old:
Crushing chest pain
Diaphoresis
Acquire 12-lead early.
Cardiac Medications (AEMT Section)
Even if you're currently studying EMT, you'll likely be tested on these.
AspirinWhy:
Stops platelets from forming larger clots.
Use:
Suspected heart attack.
Example:
Patient:
Crushing chest pain
Pressure radiating to arm
→ Give aspirin if protocol allows.
Do NOT give:
Allergy
Active bleeding
NitroglycerinWhy:
Dilates coronary arteries.
Use:
Chest pain from suspected ACS.
Requirements:
Adequate blood pressure
Prescribed medication
Example:
Chest pain patient:
BP 150/90
→ Assist with nitro.
Avoid if:
BP low.
EpinephrineWhy:
Raises blood pressure and opens airways.
Use:
Anaphylaxis.
Example:
Bee sting:
Wheezing
Hives
Swollen tongue
→ Epi immediately.
Naloxone (Narcan)Why:
Reverses opioid overdose.
Use:
Respiratory depression from opioids.
Example:
Patient:
RR 4
Pinpoint pupils
First:
BVM
Then:
Naloxone
Airway and breathing come first.
AlbuterolWhy:
Bronchodilator.
Use:
Asthma
COPD
Bronchospasm
Example:
Patient with wheezing and respiratory distress.
DextroseWhy:
Raises blood sugar.
Use:
Symptomatic hypoglycemia.
Example:
Diabetic patient:
Altered mental status
BGL = 35
→ Dextrose.
GlucagonUse:
Hypoglycemia when IV unavailable.
Ondansetron (Zofran)Use:
Nausea and vomiting.
Example:
Patient continuously vomiting and becoming dehydrated.
EMT Exam Tip
For almost every emergency, think:
1. Airway
Open?
Obstructed?
2. Breathing
Oxygenating?
Ventilating?
3. Circulation
Pulse?
Bleeding?
Perfusion?
4. Determine the cause
Asthma → Albuterol
Opioid overdose → Narcan
Anaphylaxis → Epinephrine
ACS → Aspirin/Nitro
Cardiac arrest → CPR + AED
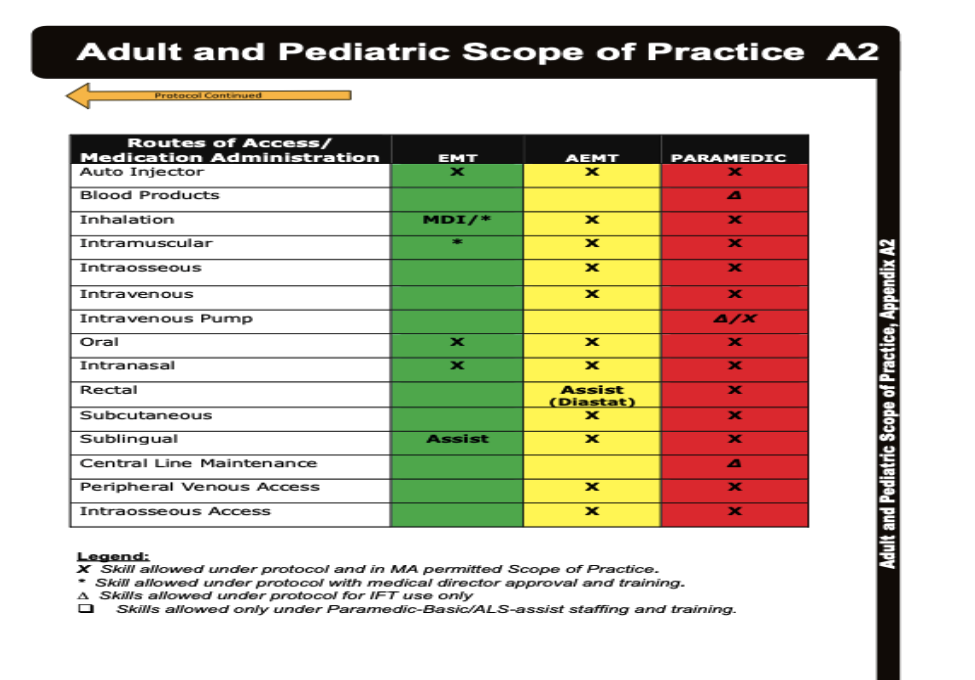
Routes of Access/Medication Administration
1. Auto InjectorWhat it is
A preloaded device that automatically injects medication.
Examples:
Epinephrine auto-injector (EpiPen)
DuoDote (special situations)
When EMTs use itAnaphylaxis
Patient has:
Trouble breathing
Wheezing
Swollen tongue/lips
Hives
Low blood pressure
Example
Patient stung by bee:
Respiratory distress
Swollen airway
Stridor
→ Use EpiPen IM through outer thigh.
Why?
Epinephrine:
Opens airways
Raises blood pressure
Reduces swelling
2. InhalationWhat it is
Medication breathed directly into lungs.
Examples:
Albuterol inhaler (MDI)
Nebulized albuterol
When to useAsthma
Patient:
Wheezing
Tight chest
Difficulty breathing
COPD
Patient:
Wheezing
Respiratory distress
Example
16-year-old asthma patient:
Audible wheezing
Speaking 2–3 words at a time
→ Assist with inhaler or nebulizer.
Why?
Gets medication directly into lungs quickly.
3. Intramuscular (IM)What it is
Medication injected into muscle.
Common site:
Lateral thigh
When EMTs encounter itEpinephrine
Most common EMT IM medication.
Example
Patient with anaphylaxis.
→ Epi IM into thigh.
Why IM?
Muscle has excellent blood supply.
Medication works rapidly.
4. Oral (PO)What it is
Medication swallowed.
Common EMT examplesAspirin
Chest pain / suspected heart attack.
Glucose
Conscious diabetic patient.
Example
65-year-old:
Crushing chest pain
Alert and able to swallow
→ Give aspirin per protocol.
Do NOT give PO medication if:
Unconscious
Vomiting
Cannot swallow safely
5. Intranasal (IN)What it is
Medication sprayed into the nose.
Absorbed through nasal mucosa.
Common EMT medicationNaloxone (Narcan)
When to use
Patient:
Opioid overdose
Respiratory depression
Pinpoint pupils
Example
Patient found unconscious.
RR 4
Pinpoint pupils
First:
Open airway
BVM ventilate
Then:
Administer Narcan IN.
Why IN?
Fast
Needle-free
Easy to administer
6. Sublingual (SL)What it is
Medication placed under tongue.
Common EMT medicationNitroglycerin
When to use
Suspected acute coronary syndrome.
Patient:
Chest pressure
Crushing chest pain
Example
55-year-old male:
Chest pain radiating to jaw
BP 160/90
→ Assist with prescribed nitroglycerin.
Why under tongue?
Very rapid absorption.
Avoids digestive tract.
Do NOT use if:
Hypotension
Recent erectile dysfunction medication use (per protocol)
Altered mental status
7. Rectal Administration
Mostly seen in pediatrics.
Example
Rectal diazepam for seizures.
EMTs may assist in some systems.
Scenario
Child actively seizing.
Caregiver has prescribed rectal medication.
→ Assist according to protocol.
Advanced Routes You'll See on Exams
Even though EMTs don't typically perform these, you should recognize them.
8. Intravenous (IV)What it is
Medication directly into a vein.
Why use it?
Fast medication delivery.
Immediate bloodstream access.
Common uses
Dextrose
Fluids
Cardiac medications
Pain medications
Example
Hypoglycemic patient:
BGL = 25
AEMT/Paramedic:
→ IV Dextrose.
9. Intraosseous (IO)What it is
Needle placed into bone marrow.
Usually:
Tibia
Humerus
When used
Cannot obtain IV access.
Patient critically ill.
Example
Cardiac arrest patient.
No veins visible.
→ Establish IO access.
Why?
Bone marrow connects directly to vascular system.
Functions almost like an IV.
10. Peripheral Venous AccessWhat it is
Standard IV placement.
Common locations:
Hand
Forearm
AC (antecubital vein)
When used
Trauma
Shock
Cardiac emergencies
Severe dehydration
11. Blood ProductsWhat it is
Administration of:
Whole blood
Packed red blood cells
Plasma
When used
Massive hemorrhage.
Example
Motor vehicle crash.
Patient:
BP 70/40
Severe bleeding
ALS/critical care may administer blood products.
Putting It Together: EMT Scenario ThinkingChest Pain
Patient:
Crushing chest pain
Alert
Routes:
PO → Aspirin
SL → Nitroglycerin (assist)
Asthma Attack
Patient:
Wheezing
Respiratory distress
Routes:
Inhalation → Albuterol
Anaphylaxis
Patient:
Airway swelling
Wheezing
Hypotension
Routes:
Auto-injector
IM Epinephrine
Opioid Overdose
Patient:
RR 4
Pinpoint pupils
Routes:
IN Naloxone
Diabetic Emergency
Patient:
Low blood sugar
Conscious
Route:
Oral glucose
If unconscious:
IV Dextrose (AEMT/Paramedic)
IM/IN options depending on protocol
Quick EMT Exam Memory Table
Route | Medication | Typical Scenario |
|---|---|---|
Oral (PO) | Aspirin, Glucose | Chest pain, hypoglycemia |
Sublingual (SL) | Nitroglycerin | Suspected heart attack |
Intranasal (IN) | Naloxone | Opioid overdose |
Inhalation | Albuterol | Asthma/COPD |
IM | Epinephrine | Anaphylaxis |
Auto-Injector | Epinephrine | Severe allergic reaction |
IV | Dextrose, fluids | Shock, hypoglycemia |
IO | Emergency medications | Cardiac arrest/no IV access |
Blood Products | Blood transfusion | Massive hemorrhage |
Standard of Care
Standards of care is the care that would be expected to be provided by an EMT with similar training when caring for a patient in a similar situation
What EMTs should, and are expected to do, do
Prudent person criterion - public is going to expect you to do things as an EMT; provide care and get them to hospital for example
Defined stakeholders
Communicated in protocols, standing orders
To be an effective EMT, you must maintain your skills and knowledge as well as participate in quality improvement
Exception Principle of the protocols
The Exception Principle allows EMTs to safely bend standard treatment rules in rare, unanticipated clinical situations. Because no rulebook can predict every medical emergency, it gives providers permission to do what is best for the patient’s immediate survival, provided they stay within their legal training and call a doctor first. [1, 2]
Here is exactly how the Exception Principle works, broken down step-by-step:
1. The "Rule-Bending" Rule
Standard protocols act as a step-by-step "recipe" for treating common emergencies. The Exception Principle acknowledges that sometimes a patient has a unique, unpredictable condition where following the standard recipe might actually cause harm. [1, 2, 3, 4]
2. The Four Strict Conditions
You cannot simply use the Exception Principle to do whatever you want. It only applies if all of the following conditions are met: [1, 2]
The patient's life is in immediate danger and standard care isn't working.
The action you want to take is within your legal training level (e.g., an EMT basic cannot suddenly perform a paramedic-level surgery).
You must get approval from Medical Control (a doctor you speak with over the radio or phone) before making the move.
It is used for a single specific patient, not as a permanent shortcut to bypass standard paperwork or operational rules. [1, 2, 3, 4, 5]
3. Why It Exists
It essentially acts as a legal safety net. It protects the EMT and Medical Control doctor when they step outside the standard box to perform a life-saving intervention for a uniquely complex emergency. [1, 2]
4. What Happens After
After the emergency is over, the provider must file highly detailed paperwork. They have to document exactly what they did, why they did it, and the verbal approval they got from the doctor
Here is a realistic scenario where an Advanced EMT (AEMT) would use the Exception Principle:
The Situation
An AEMT is called to a remote hiking trail for a 50-year-old male experiencing an extreme, life-threatening asthma attack. Standard treatment protocols dictate giving the patient inhaled nebulizer medications (like albuterol) and a continuous flow of oxygen.
The Problem
The patient’s airways are completely closed up. Because no air is moving in or out of his lungs, the inhaled nebulizer medication cannot actually reach his airways to work. He is rapidly losing consciousness from a lack of oxygen.
The Protocol Conflict
The standard protocol for this specific medical service states that only Paramedics—not AEMTs—are allowed to inject epinephrine intramuscularly (an EpiPen-style shot) for severe asthma. The AEMT is fully trained and certified to inject epinephrine, but their local protocol restricts them from doing it for asthma (it is normally reserved for severe allergic reactions).
The nearest Paramedic unit is 30 minutes away. If the AEMT waits or sticks strictly to the standard asthma protocol, the patient will experience cardiac arrest and die.
Applying the Exception Principle
Immediate Danger: The patient's life is at risk and standard treatment is failing.
Within Training: The AEMT is legally certified to give epinephrine injections.
Medical Control Approval: The AEMT calls the hospital doctor on the radio, explains that the patient is dying because no air is moving, and asks for an exception to give the epinephrine injection. The doctor grants verbal approval.
Action Taken: The AEMT gives the shot, the airways open up, and the patient's life is saved.
The Follow-Up
Once the patient is safely at the hospital, the AEMT writes a detailed narrative report. They document the patient's critical condition, the failure of the standard protocol, the exact time they received verbal permission from the doctor, and the successful outcome.
For an asthma attack or severe bronchospasm, a Massachusetts EMT's standing orders restrict them to administering inhaled bronchodilators (like Albuterol) via a nebulizer or CPAP machine. They cannot give a shot of epinephrine for asthma. [1, 2]
The rules handle epinephrine for asthma differently based on certification level:
EMT-Basics & Advanced EMTs (AEMTs): They carry epinephrine (either an auto-injector or a "Check and Inject" syringe kit), but they are legally limited to using it for anaphylaxis. They are completely locked out of using it for standard asthma flare-ups under standing orders. [1, 2, 3, 4]
Medical Direction
EMTs are extensions of medical director
Physicals and medical director required for all EMS systems
Oversees all aspects of patient care
Continuous quality improvement
We have a medical director for the EMT and Paramedicine Programs
Zachary Kramer, MD
There is also a state medical director, Jonathan Burstein, MD, as well as regional medical directors and affiliate hospital medical directors within a region
Medical Director Oversight
Indirect
Respondeat-superior
MD is responsible for EMTs actions vicariously
This principle also applies to employers
Direct
CQI Monitoring/Validation
Supervision
Protocol development
Medical director oversight is the legal and clinical safety net for Emergency Medical Technicians (EMTs). It ensures safe, standardized patient care. [1, 2, 3, 4, 5]
The specific terms in your query break down as follows:
Medical Director Oversight Categories
Indirect Oversight: The behind-the-scenes administrative duties performed by the Medical Director, such as developing standing orders, policies, and educational requirements. [1, 2, 3, 4]
Direct Oversight: Real-time, two-way communication between the Medical Director and the EMT, such as calling a doctor on the radio for specific treatment instructions on a live scene. [1, 2]
Legal & Employer Liability
Respondeat Superior: A Latin legal doctrine meaning "let the master answer". It holds that employers are vicariously (indirectly) responsible for the negligent acts of their employees, provided those acts occurred within the normal scope of their job duties. [1, 2, 3]
MD Vicarious Liability: Because EMTs practice medicine under the medical director’s license, the MD assumes responsibility for the system's clinical performance. [1, 2]
Clinical Supervision & Quality Management
Protocol Development: The Medical Director is responsible for writing the strict, evidence-based rules, algorithms, and standing orders that dictate exactly how EMTs assess and treat patients. [1, 2]
CQI (Continuous Quality Improvement): A structured system used to review and validate patient care. It involves auditing call reports, reviewing patient outcomes, and monitoring medical data to spot errors, improve system performance, and provide targeted training to EMTs
3 Avenues of Authority for EMTs
LICENSING/CERTIFICATION AGENCY
MA OEMS
NREMT
EMPLOYMENT
PUBLIC or PRIVATE
Union CBA
Rules and Regs
Policy Handbook
MEDICAL DIRECTOR
Grants authorization to practice
Ethical Responsibilities
Study of morals and moral choices; rules of right and wrong conduct
Ethical issues can pose dilemmas
EMT Code of Ethics
Provide care based on need without regard to nationality, race, creed, color, or religion
Protect patient confidentiality
Respect patient dignity
Promote high standard of care
Take responsibility for actions and conduct
Uphold standards of practice and education
Quality training promotes a high standard of care for your patients.
Core Values
People act and decide according to values and beliefs
Core values
Integrity
Compassion
Accountability
Responsibility
Empathy
Legal Aspects of Providing Care
Licensure vs Certification
Authority to Practice
Certification
a process, often voluntary, by which individuals who have demonstrated the level of knowledge and skill required in the profession, occupation, role, or skill are identified to the public and other stakeholders
voluntary process;
by a private organization;
for the purpose of providing the public information on those individuals who have successfully completed the certification process (usually entailing successful completion of educational and testing requirements) and demonstrated their ability to perform their profession competently.
Licensure
State’s grant of legal authority, pursuant to the state’s police powers, to practice a profession within a designated scope of practice
The use of certification is used by some states as a basis for granting individuals the right to practice
an occupation has a statutorily or regulatorily defined scope of practice and only individuals authorized by the state can perform those functions and activities, the authorized individuals are licensed
An EMT certification validates that you have met specific educational standards and passed competency exams, usually issued by a private or national organization like the National Registry of Emergency Medical Technicians. [1, 2]
An EMT license is the mandatory, legal permission granted by a government or state authority (such as a state EMS office) that actually allows you to work and practice in the field
Duty to Act
Implied or contractual
Off-duty responders generally do not have duty to act
However, once care is begun, a duty is created
Failure to continue care until patient care is transferred can result in claims of negligence or abandonment
A. In certain situations an EMT has a duty to act, or an obligation to provide emergency care to a patient.
B. An EMT who is on an ambulance and is dispatched to a call has a duty to act.
C. If an EMT initiates care and then leaves the patient without ensuring that the patient has been turned over to someone with equal or greater medical training, this is considered abandonment.
D. A duty to act is not always clear.
1. In many states, an off-duty EMT has no legal obligation to provide care.
2. If you are off-duty but begin care and then leave before other trained personnel arrive, this could still be considered abandonment.
Always follow local protocols and laws
Good Samaritan laws
Intended to protect passersby from liability if they stop to render aid
Applies to those responding in good faith and without compensation
Prudent person standard applies
Does not cover gross negligence
Consent
Expressed Consent
Patient must be alert, competent adult
Verbal, nonverbal, written
Must determine: competence, capacity
Consent
EMTs must have consent before treating patients
Several forms of consent
Patient can withdraw consent at any time
Implied Consent
Patients who are unresponsive can be cared for on implied consent
Consent is assumed when someone cannot consent
Minors - implied consent always; cannot get refusal from parents over the phone. Parents need to be seen. If minor has a baby, they are not a minor anymore (female)
Unresponsive
Mentally incompetent; if they can answer questions appropriately, they have the right to refuse because they are mentally competent. If they can’t answer simple questions, then they are mentally incompetent.
Includes intoxication
Includes law enforcement if needed
Refusal of Care
Obtaining Patient Refusal
Patients who refuse care
Competent adults have the right to refuse care
Legal guardian or parent can refuse care for dependents
Patients can withdraw consent; cannot be over the phone in massachusetts
When a patient refuses care:
Try to convince patient to allow care; explain risks and consequences
Determine patients understanding of information
Try to convince patient to allow care;explain risks and consequences
Determine the patient's understanding of information
If conditions of protocols are met, have patient sign a release
If a patient refuses to sign, have a witness.
When a patient refuses care
CONTACT MEDICAL CONTROL FOR HIGH RISK REFUSALS
When in doubt, on the side of treatment
Involve law enforcement in extreme cases
Use detailed documentation
Additional Legal Concepts
Statue of limitations
Amount of time after an event that legal proceedings can be initiated
Contributory negligence
Any behavior on the patients part that may have led to the injury for which he is suing another party
Sovereign immunity:
Exemption from liability for government agencies
1. Statute of Limitations
Think of this as the legal "expiration date" for your lawsuit. It is a law that sets a strict time limit (usually 2 to 3 years, depending on the state and type of case) after an event occurs to formally begin legal proceedings. If you wait too long and miss this deadline, you lose your right to sue and seek compensation. [1, 2, 3, 4]
2. Contributory (or Comparative) Negligence
This is a rule used to figure out who is to blame when both parties share some of the fault. If a patient ignores their doctor's instructions or lies about their medical history, this behavior can be used to argue the patient contributed to their own injury. In most states, your compensation is reduced by your percentage of fault. If your percentage of fault crosses a certain limit (usually 51% or more), you are completely barred from recovering any damages. [1, 2, 3, 4, 5]
3. Sovereign Immunity
This is a legal shield that largely protects government agencies (like cities, states, or federal branches) from being sued. The rule comes from the old idea that "the king can do no wrong." Today, it means the government is generally immune to lawsuits unless they have passed specific laws—such as the Federal Tort Claims Act—that waive this immunity, allowing citizens to sue under strict conditions. [1, 2, 3, 4, 5]
Advance Directives
Legal statement of patient's wishes regarding health care
Different types
Living will
Do not resuscitate order
Durable power of attorney for health care
Physician's orders for life-sustaining treatment
MOLST in MA
Negligence
Criminal and civil laws apply to EMS providers
Torts are civil cases based on wrongdoing by the defendant
Negligence is an omission or neglect of reasonable care, precaution, or action
Four elements necessary to prove negligence
EMT had a duty to act
EMT breached the duty to act by not living up to his legal obligations
Patient suffered damages
EMT's breach of duty was the cause of the patient's damages
Abondement
EMT with duty to act leaves a patient in need of care without turning care over to a person of equal or higher training
Always formally turn over patient care with a verbal report and, usually, written patient care report
Assault and Battery
Assault
Threat of force against another person; including threatening physical contact against a patient's wishes
Battery
Carrying out the threat, including providing care a patient does not consent to
Use of restraints
Can be legally risky
False imprisonment
Kidnapping
Use only when patient is imminent risk to self or others
Involve law enforcement if possible
Document all aspects of situation
Patient Transfers
Emergency Medical Treatment and Active Labor Act (EMTALA)
Issues with transporting patients and transferring care
Closest hospital is often best; follow protocols
For transfers, make sure patient's needs are in your scope of practice
Excellent communication needed to safely transfer care
Confidentiality and Privacy
Health Care Insurance Portability and Accountability Act (HIPAA)
Restrictions on sharing patient information
To maintain patient confidentiality, discuss your patient only with those who will be continuing patient care.
Mandated Reporting
Special Reporting Situations: State laws identify specific situations that EMS providers must report
Issues include abuse and neglect
Elderly
Mentally handicapped
Children
Lesson Summary
Scope of practice and standard of care
Ethical and moral obligations
Patient confidentiality
Legal issues
Duty to act
Advance directives
Assault, battery
Abandonment
Negligence
Organ donor status
Crime scenes
Mandatory reporting