vascular system and special circulation
1/17
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
18 Terms
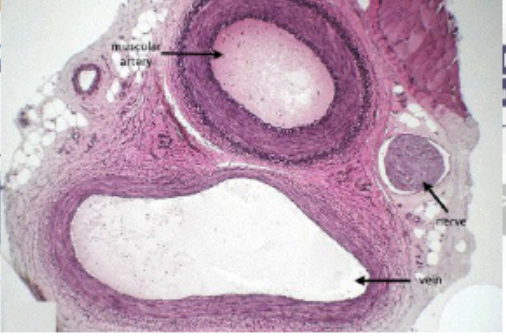
types of blood vessels
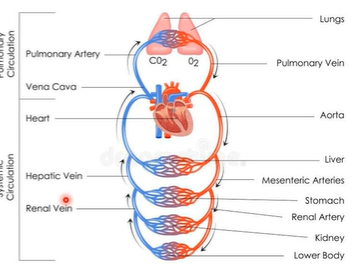
Circulatory system: Blood flows from the heart through arteries and into capillaries. I then returns to the heart through veins.
This system encompasses three types of vessels:
1. Artery - arteriole
2. Vein – venule
3. Capillary
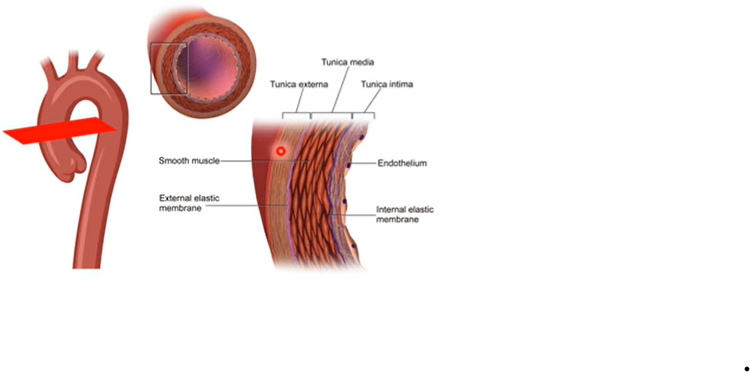
tunica intima - close proximity to blood - cells are enriched - endothelium
beneath that is thick of elastin - gives artery elasticity
then tunica media - gives collagen and elastin fibres - contractile behaviour of artery
tunica externa - made of collagen and elastin and fibroblasts - make less contractile - more vulnerable
arteries
Carries blood at high pressure
Thick walled – a thick smooth muscle layer will allow artery to withstand high systemic pressure
Elastin for elasticity: must have elastic property – ability to recoil
These abilities start decline with time – as we age compliance of arteries reduces
Arterioles are basically smaller arteries
High resistance
Less compliant than larger arteries
Control flow of blood into capillaries
Blood flow is controlled by local factors
Autoregulation
Sympathetic vasoconstrictio
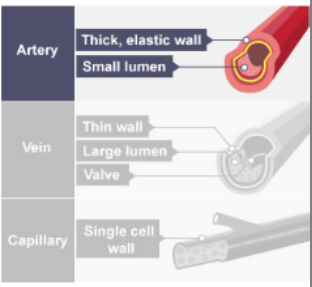
veins
Low pressure flow
Rich sympathetic innervation – so in sympathetic vasoconstriction – blood from veins supply a large portion of venous return
Carry blood back to heart
tunica media less developed - so less collagen, elastin and smooth muscle cells
histology compares flattened vein with bigger lumen with thinner tunica media compared to artery
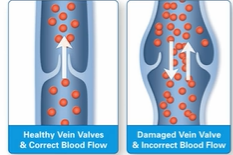
Valves in veins are delicate, two-flap structures that act as one-way doors to ensure blood flows toward the heart and prevent backflow (venous reflux) caused by gravity.
Primarily found in the limbs, these valves open as blood travels upward and close when blood halts, ensuring, for example, that blood in the legs does not
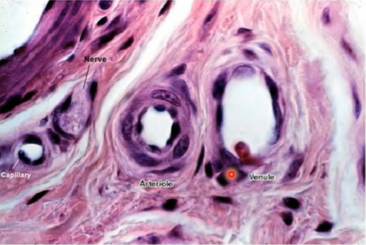
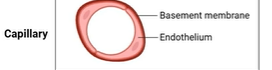
capillaries
Flattened endothelium – high permeability
Allow gases, nutrients and electrolytes to be exchanged
Large network
Connects arterioles to venules
thin layer of basement membrane
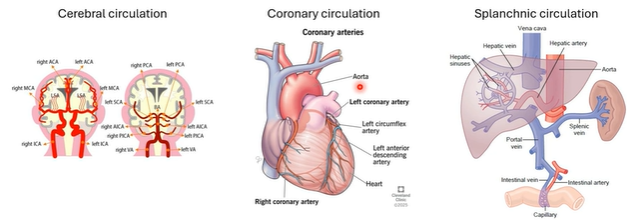
types of various special circulations
"Special circulations" are distinct from "normal" (systemic) circulation because they prioritize maintaining blood flow to vital organs despite changes in systemic blood pressure
we have 3 types of circulation
-cerebral
-coronary
-sphlanchic (liver + kidney)
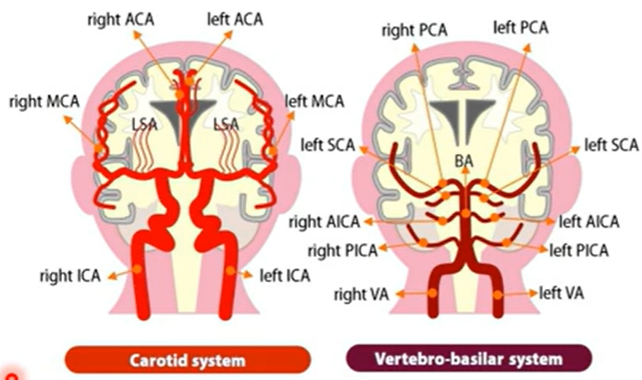
cerebral circulation
The brain is highly dependent on a continuous supply of oxygen and glucose delivered through cerebral blood flow.
The two systems are carotid and vertebro-basilar
Even brief interruptions in blood supply have severe consequences. If cerebral blood flow stops for 5–10 seconds, loss of consciousness occurs, and after approximately 3 minutes, irreversible neuronal injury and brain damage can develop due to oxygen deprivation.
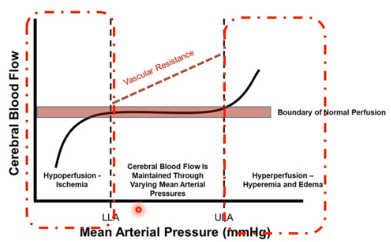
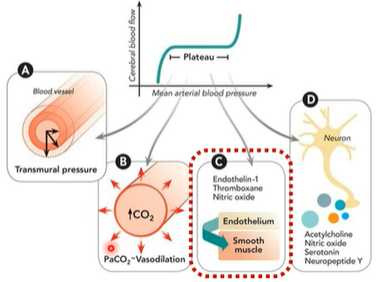
Despite fluctuations in systemic blood pressure, the brain maintains a relatively stable blood supply through a process called cerebral autoregulation
Within a mean arterial pressure (MAP) range of approximately 60–140 mmHg, cerebral blood flow remains nearly constant at around 750 ml/min. This stability is achieved by adjustments in cerebral vascular resistance—blood vessels constrict when blood pressure rises and dilate when it falls
cerebral blood flow cont.
When mean arterial pressure falls below the lower limit of autoregulation (LLA), cerebral vessels cannot dilate sufficiently, resulting in hypoperfusion and ischemia. (perfusion-delivering blood to capillary beds in tissues and organs, providing essential oxygen and nutrients while removing metabolic waste)
Conversely, when MAP exceeds the upper limit of autoregulation (ULA), vessels cannot constrict further, leading to hyperperfusion, which may contribute to cerebral edema (swelling) and vascular damage.
Overall, cerebral autoregulation protects brain tissue by maintaining consistent perfusion across physiological blood pressure variations, but outside the autoregulatory range the brain becomes vulnerable to ischemic or hyperemic injury
how is cerebral circulation controlled?
4 main parametres that work collaboratively
1) Myogenic Mechanism (Pressure- dependent regulation)
Changes in arterial pressure alter transmural pressure (difference in pressure across the wall of a hollow organ, vessel, or structure) across the vessel wall.
When blood pressure increases, vascular smooth muscle in cerebral arterioles stretches and responds with reflex vasoconstriction, increasing vascular resistance and preventing excessive increases in cerebral blood flow.
Conversely, reduced pressure leads to vasodilation
important note here - notice how vasoconstriction/dilation is not causing the pressure, it is a RESULT of it
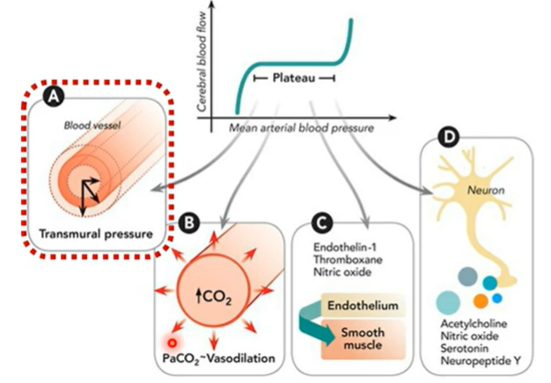
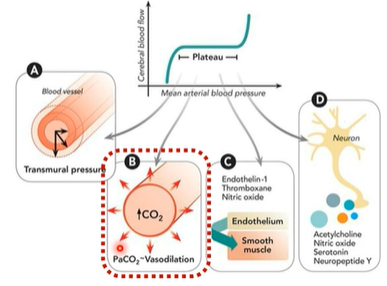
2) metabolic regulation (local chemical control)
vasodilation according to amount of CO2
Local metabolic activity strongly influences vascular tone.
Increases in CO₂ (PaCO₂) and other metabolites cause vasodilation, increasing blood flow to match metabolic demand.
Cerebral vessels are particularly sensitive to CO₂ levels, making it a major regulator of cerebral perfusion
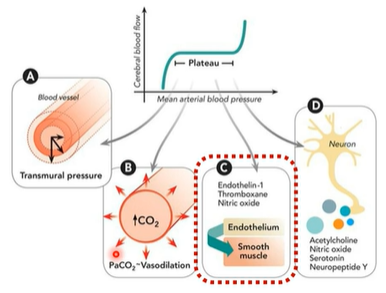
3) endothelial regulation
The vascular endothelium releases vasoactive mediators that act on smooth muscle to adjust vessel diameter. Important factors include nitric oxide (vasodilator), endothelin-1, and thromboxane (vasoconstrictors), which help fine-tune cerebral vascular resistance
4) neurogenic regulation (neurovascular coupling)
Neurons influence nearby blood vessels through neurotransmitters such as acetylcholine, nitric oxide, serotonin, and neuropeptide Y.
Increased neuronal activity promotes functional hyperemia (increased, excessive flow of blood to specific tissues or organs in the body), increasing blood flow to regions with higher metabolic demand
cushing’s reflex/triad
Occurs when intracranial pressure (ICP) (pressure exerted by fluids such as cerebrospinal fluid (CSF) and blood within the rigid skull) rises significantly.
The sequence begins with elevated ICP, which causes compression of cerebral blood vessels and vasoconstriction, leading to reduced oxygen delivery to brain tissue (because brain in skull not much room)
As cerebral perfusion decreases, CO₂ accumulates and pH falls, stimulating the central chemoreceptors in the medulla. This activates a powerful sympathetic response aimed at restoring cerebral perfusion.
The presence of the Cushing reflex indicates critical brainstem compression and reduced cerebral perfusion, often seen in conditions such as brain tumors, intracranial hemorrhage, traumatic brain injury, or severe cerebral edema, and is considered a late and life-threatening sign of raised intracranial pressure.
fo dumb people (me) to explain the respiratory suppression
As the baroreceptors see the increased blood pressure in the brain, it signals for the HR to slow down to ease the pressure of blood flowing to the brain. In order to help drop blood pressure further, the baroreceptors send a separate nerve signal that directly suppresses the breathing center in the brain. This is an unfortunate consequence as CO2 cannot be filtered out as quickly.

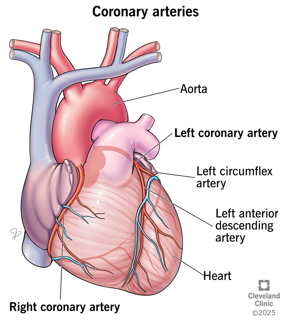
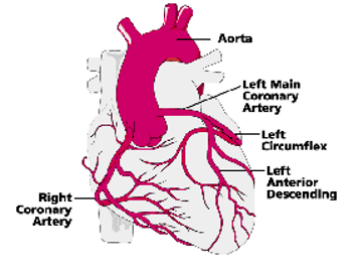
coronary circulation
§Arteries arise from the aorta close to the aortic valve
§Deoxygenated blood returns to the Right atrium via the coronary sinuses/anterior cardiac veins (this is from heart muscle itself, the vena cavae would be from the body)
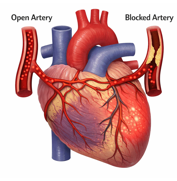
Collateral coronary circulation
The coronary arteries from small inter-connections called collateral vessels. These channels normally carry very little blood, but they can become functionally important when a coronary artery becomes partially or completely occluded.
In such cases, blood can be diverted from a patent (non-occluded) artery to the region supplied by the blocked artery, helping maintain myocardial perfusion and limiting the extent of ischemia (lack of blood flow to tissue). Over time, these collateral vessels may enlarge and become more efficient, especially in chronic coronary artery disease.
baseline coronary blood flow
§Baseline coronary blood flow
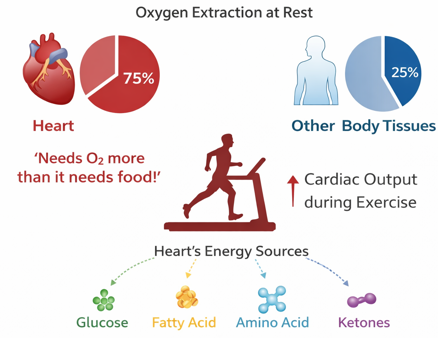
At rest, the heart receives approximately 5% of total cardiac output, corresponding to about 250 ml/min of coronary blood flow.
This relatively high perfusion reflects the very high metabolic demand of the myocardium, which extracts a large proportion of oxygen from the blood even at rest.
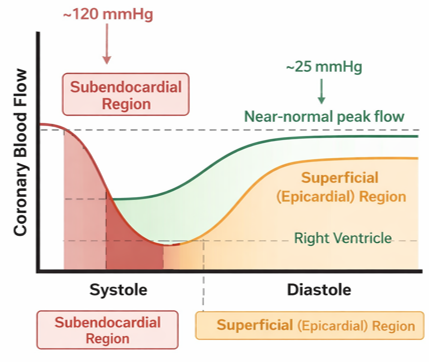
Effect of ventricular contraction on coronary flow (systole)
During systole, the contracting myocardium compresses the intramyocardial coronary vessels. This mechanical compression significantly reduces coronary perfusion, particularly in the left ventricle where intraventricular pressures are high.
Because the left ventricular systolic pressure reaches ~120 mmHg, the pressure within the contracting myocardium exceeds coronary perfusion pressure.
Perfusion is the passage of blood or other fluid through vascular beds into tissues and organs, delivering oxygen and nutrients while removing waste.
coronary circulation cont.
•Subendocardial region of the left ventricle:
The vessels are most strongly compressed in this inner myocardial layer, resulting in almost no blood flow during systole. This makes the subendocardium particularly vulnerable to ischemia.
(The subendocardium is simply the deepest boundary zone of the myocardium, right where it transitions into the endocardium (endocardium acc lines the blood).)
•Superficial (epicardial) regions of the left ventricle:
These regions experience less compressive force, so some coronary flow may still occur during systole, although it is reduced.
•Right ventricle:
The right ventricle generates much lower systolic pressure (~25 mmHg). Because the compressive force on coronary vessels is therefore smaller, coronary blood flow in the right ventricle can occur throughout systole and may approach near-normal peak flow.
clinical implication
§Clinical implication
Because systolic compression restricts coronary perfusion in the left ventricle, most left ventricular coronary blood flow occurs during diastole (≈80%).
Consequently, conditions that shorten diastole—such as tachycardia—can significantly reduce myocardial perfusion and predispose to ischemia, particularly in the subendocardial region.
Ischemia is a serious medical condition defined by reduced blood flow to tissues or organs, causing them to receive insufficient oxygen to function properly
splanchnic circulation
Composed of gastric, small intestinal, colonic, pancreatic, hepatic, and splenic circulations
Arranged in parallel with one another.
The three major arteries that supply the splanchnic organs:
-celiac trunk
-superior mesentric artery
-inferior mesenteric artery, give rise to smaller arteries that anastomose extensively.
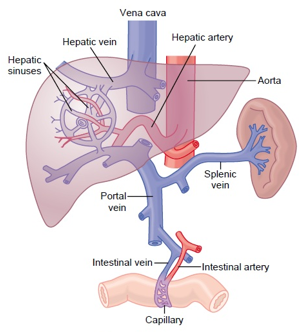
Portal system - responsible for directing blood from parts of the GIT to the liver. Substances absorbed in the small intestine travel first to the liver for processing before continuing to the heart
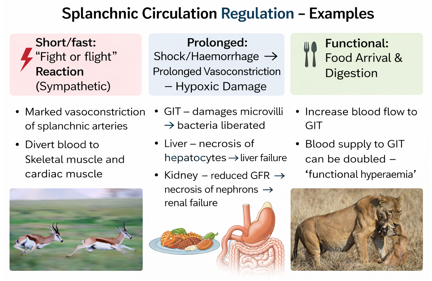
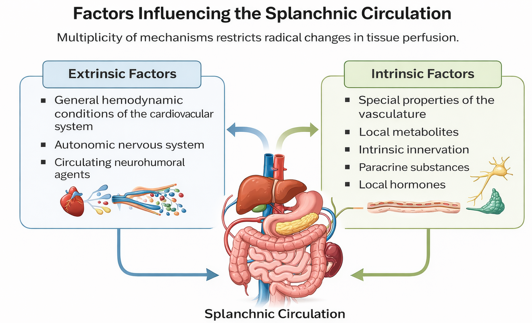
Factors influencing the splanchnic circulation
Intrinsic factors are internal elements originating from within an individual, system, or organism (e.g., genetics, age, personal motivation), while extrinsic factors are external forces acting from the outside (e.g., environment, rewards, societal pressures