41 - bone and soft tissue tumours
1/49
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
50 Terms
what is sarcoma
malignant connective tissue tumour that spreads along fascial planes
where does sarcoma often spread to
haematogenous spread to LUNGS
what are the benign bone forming tumours
osteoid
osteoma
osteoblastoma
what are the malignant bone forming tumours
osteosarcoma
what are the benign cartilage forming tumours
endochondroma, osteochondroma
malignant cartilage forming tumours
Chondrosarcoma
benign fibrous tissue tumours
fibroma
malignant fibrous tissue tumours
fibrosarcoma, malignant fibrous hystiocytoma (MFH)
benign vascular tissue tumours
haemangioma
aneurysmal bone cyst
malignant vascular tissue tumour
angiosarcoma
benign adipose tissue tumour
lipoma
malignant adipose tissue tumour
Liposarcoma
marrow tissue tumours - malignant
Ewings sarcoma
lymphoma
myeloma
what is the most common primary malignant bone tumour in younger patients
osteosarcoma
what is the commonest primary malignant bone tumour in older patient’s?
myeloma
tumour-like lesions
simple bone cyst
fibrous cortical defect
malignant bone tumour symptoms
pain that's activity related and progressive pain at rest and night
examination for bone tumours
general health
measurement of mass
location
shape
consistency
mobility
tenderness
local temperature
neuro-vascular deficits
what swelling signs are suspicious of a malignant tumour
rapidly growing
hard, fixed, craggy surface, indistinct margins
non-tender to palpation
associated with deep ache worse at night
may be painless
recurred after previous excision
investigations for bone tumours
plain X-ray most useful for bone lesions
- clear margins
- surrounding rim of active bone
- cortical expansion
what can cortical expansion occur with
aggressive benign lesions
where does calcification occur in?
synovial sarcoma
aggressive signs on X-ray that indicates malignancy
cortical destruction
•less well defined zone of transition between lesion and normal bone (permeative growth)
•Periosteal reactive new bone growth occurs when the lesion destroys the cortex.
- Codman’s triangle, onion-skinning or sunburst pattern
what is CT good for visualising in bone tumours
ossification and calcification
integrity of cortex
best for assessing nidus in osteoid sarcoma
staging - lungs
what are isotopes bone scans used for
staging for skeletal metastasis
multiple lesions
what is the imaging modality of choice of BOTH bone and soft tissue tumours
MRI
•size, extent, anatomical relationships
•Accurate for limits of disease both within and outside bone
•Specific for Lipoma, haemangioma, haematoma or PVNS.
•Non-specific for benign vs. malignant
what is PET useful for
investigating response to chemo
what needs to be done before biopsy
full work up
- bloods
- X-rays of affected limb and CXR
- MRI of bone lesion
- bone scan
- CT, chest, abdomen and pelvis
cardinal features of malignant primary bone tumours
increasing pain
weight loss
unexplained pain
deep seating boring nature
night pain
difficulty weight bearing
deep swelling
osteosarcoma clinical features
pain
loss of function
swelling
pathological fractures
joint effusion
deformity
neurovascular effects
systemic effects of neoplasia
pain cardinal features that point to osteosarcoma
increasing unexplained pain not relieved by analgesia and not related to exercise
deep ache worse at night
who does osteosarcoma affect more and which sites
men
distal femur and proximal tibia
swelling cardinal features in osteosarcoma
diffuse in malignancy
generally near end of long bone
warmth over swelling and venous congestion = ACTIVE
pressure effects e.g. intrapelvic
investigations for osteosarcoma
MRI
loss of function features in osteosarcoma
limp
reduced joint movement
stiff back esp. child
treatment of osteosarcoma
surgery and chemotherapy
treatment of Ewings sarcoma
chemotherapy
surgery
radiotherapy
are cartilage tumours benign or malignant
benign but aggressive
what is the commonest soft tissue tumour
lipoma
suspicious signs that point to soft tissue malignancy and need to be referred to a specialist tumour centre
deep - deep to deep fascia tumour
subcutaneous growth >5cm
rapid growth
hard
craggy
non-tender
soft tissue tumour signs
•painless
•mass deep to deep fascia
•any mass >5cm
•any fixed, hard or indurated mass
•any recurrent mass
imaging study for soft tissue tumour
MRI
swelling of soft tissue - malignancy
suspicious until proven otherwise
- rapidly growing
- hard
- craggy
- fixed and indistinct margins
- non-tender to palpate but deep ache at night
- key be painless
what are the most to least common cancers to metastasise to bone
breast
lung
prostate
kidney
thyroid
GI
melanoma
what type of metastatic bone disease is more common: primary or secondary
secondary > primary
where does breast and melanoma commonly metastsise to?
breast to bone
melanoma to lung
order of frequency in sites for secondary metastatic bone disease
vertebrae
proximal femur
pelvis
ribs
sternum
skull
prevention of pathological fracture
early chemotherapy/DXT
prophylactic internal fixation
+- use of bone cement
embolisation
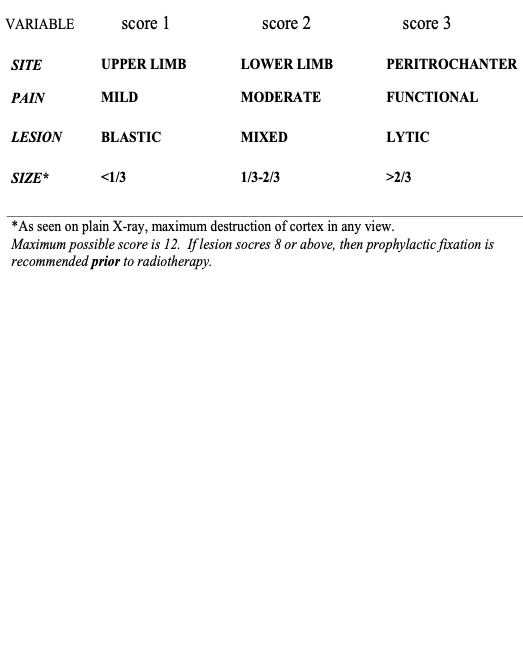
what is used for fracture risk assessment
mirel’s scoring system
when surgery is indicated for spinal metastases what is required
both decompression and stabilisation