Schizophrenia
1/50
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
51 Terms
two methods used to diagnose schizophrenia
DSM-V -USA - Requires two(or more) of the following symptoms: delusions, hallucinations, disorganised speech, catatonic behaviour, negative symptoms ie affective flattening alogia or avolition
ICD-10 - UK - Recognises subtypes of disorder eg paranoid SZ, catatonic SZ
positive vs negative symptoms
positive - an excess or distortion of normal functions which represent a change in behaviour or thoughts
negative- reduction or a loss of normal functions
Key symptoms of schizophrenia
Delusions
Hallucinations
Catatonic or disorganised behaviour - when someone acts in ways that seem inappropriate or strange to society
Disorganised speech
Affective flattening - lack of emotions, voice becomes dull and monotone, face looks blank
Avolition - lack of motivation
Alogia - speech poverty
Anhedonia - in inability to enjoy things that they used to enjoy (physical anhedonia). or social withdrawal (social anhedonia)
Reliability of diagnosis
How repeatable diagnosis of SZ is
Ways of measuring reliability of diagnosis
test - retest
Inter rater - measured by kappa score 1 is perfect above 0.7 is acceptable
Evaluation of Reliability of Diagnosis
Poor inter-rater validity: Rieger et al 2013 found diagnosis only had Kappa score of 0.46 - very low
Differences in classification of SZ: Copeland 1971 found that 69% of US psychiatrists diagnosed a ''patient'' with SZ compared to only 2% of British
Poor general reliability: Cheniaux et al 2009 found that not only was diagnosis vastly different between ICD and DSM but it was also just as varied from psychiatrist to psychiatrist
why is reliability low
-fluctuating symptoms
-different manuals
-subjective reports or self-reports of symptoms
how can we improve reliability
test retest
inter rater
patients keep diary
Rosenhan 1973
pseudo patient experiment, researchers admitted themselves into hospital claiming to be hearing voices thus diagnosed with schizophrenia - kept note of their experiences which was viewed as a symptom of mental illness
every ppt was admitted, stays ranged from 7-52 days avg 19 days. Their normal behaviour was often pathologized by staff to make it seem SZ.
Follow up study told a hospital they were admitting pseudopatient when they didnt admitt any. staff had still identified 41 people they thought were out of 193 patients
Co-morbidity
the simultaneous presence of two conditions in a patient
validity of diagnosis
the extent to which a diagnosis is accurate and leads to a successful treatment.
criterion validity
do different assessment systems arrive at the same diagnosis for same patient
Factors that affect validity
-Cheniaux et al research shows overdiagnosed with ICD(UK) and under-diagnosed with DSM. -- poor validity
Gender -- genderbiased diagnosis criteria based on stereotypes of women being more dramatic. Broverman et al found clinicians treated mentally healthy behaviour as "healthy male behaviour" and didnt account for women. however this was an older 1970 study- patriarchal society at time
Symptom overlap - under ICD a patient may recieve a diagnosis of SZ, however same patient may recieve bipolar under DSM. Some studies show that people with dissociative personality dissorder show more symptoms of SZ than people with SZ
both SZ and BPD Have positive and negative symptoms
Comorbidity
-extent to which two or more conditions occur at the same time. Common with SZ: Substance abuse, anxiety, depression
Buckley et al 2009 50% of his patients also had depression.
It could mean that it might not be seperate dissorders and may be one - lower validity
Evaluation Validity of diagnosis of SZ
-cannot be considered accurate if many cases go undiagnosed. Kim and Berrios 2001 found in Japan the idea of a disorganised mind is so stigmatised that psychiatrists are reluctant to tell patients of their condition. As a result few people are diagnosed.
-Gender-bias/differences female patients typically function better. Longenecker et al found that men are more often diagnosed with SZ than women. High functioning could explain why some women have not been diagnosed with SZ where men have similar symptoms and may have been.
-comorbidity confuses diagnosis and makes treatment difficult. Weber 2009 found many patient also had diagnosis of other medical conditions, he concluded that the very nature of diagnosis of psychiactric disorder is that they tend to recieve a lower standard of medical care. Therefore comorbidity not only complicates the diagnosis and treatment process but also contributes to poorer medical care for those with psychiactric disorders overal
-low validity in diagnosis in disorders has significant implications. The treatment process prescribed may be inneffective and harmful, potentially making worse symptoms of wrongly identified condition. which increases risk of suicide. Therefore misdiagnosis can result in stigma labelling and mistreating which can lead to a loss of trust of the healthcare system
Genetic explanation for SZ
suggests SZ is genetic and therefore runs in families. no one gene is responsible - more likely a combination of genes - polygenic
name for family/twin concordance study study
Gottsman and Shields
found children with two SZ parents had a concordance rate of 46%, children with one SZ parent 13% and siblings 9%
MZ - 48%
DZ - 17%
Siblings - 9%
parents 6%
Adoption studies
Tienari et al 2000
finland 164 adoptees with bio mother SZ 11(6.7%) had SZ
Compared to 4(2%) of control
genetic explanation evaluation
-concordance rates from family/twin studies can be explained by factors other than genetics. concordance rates are not 100% and other factors such as environment are shared.
-sample sizes often very small, its hard to find twins with sz for example
-Loehlin and Nichols argue that identical twins are treated more similarly than DZ
-many SZ twin and family studies are old and since then diagnosis criteria has changed
-a diathesis stress model may be more appropriate
Old dopamine hypothesis
excessive amounts of dopamine or oversensitivity to dopamine causes SZ.
Dopamine is active in limbic area of the brain, area governing emotion
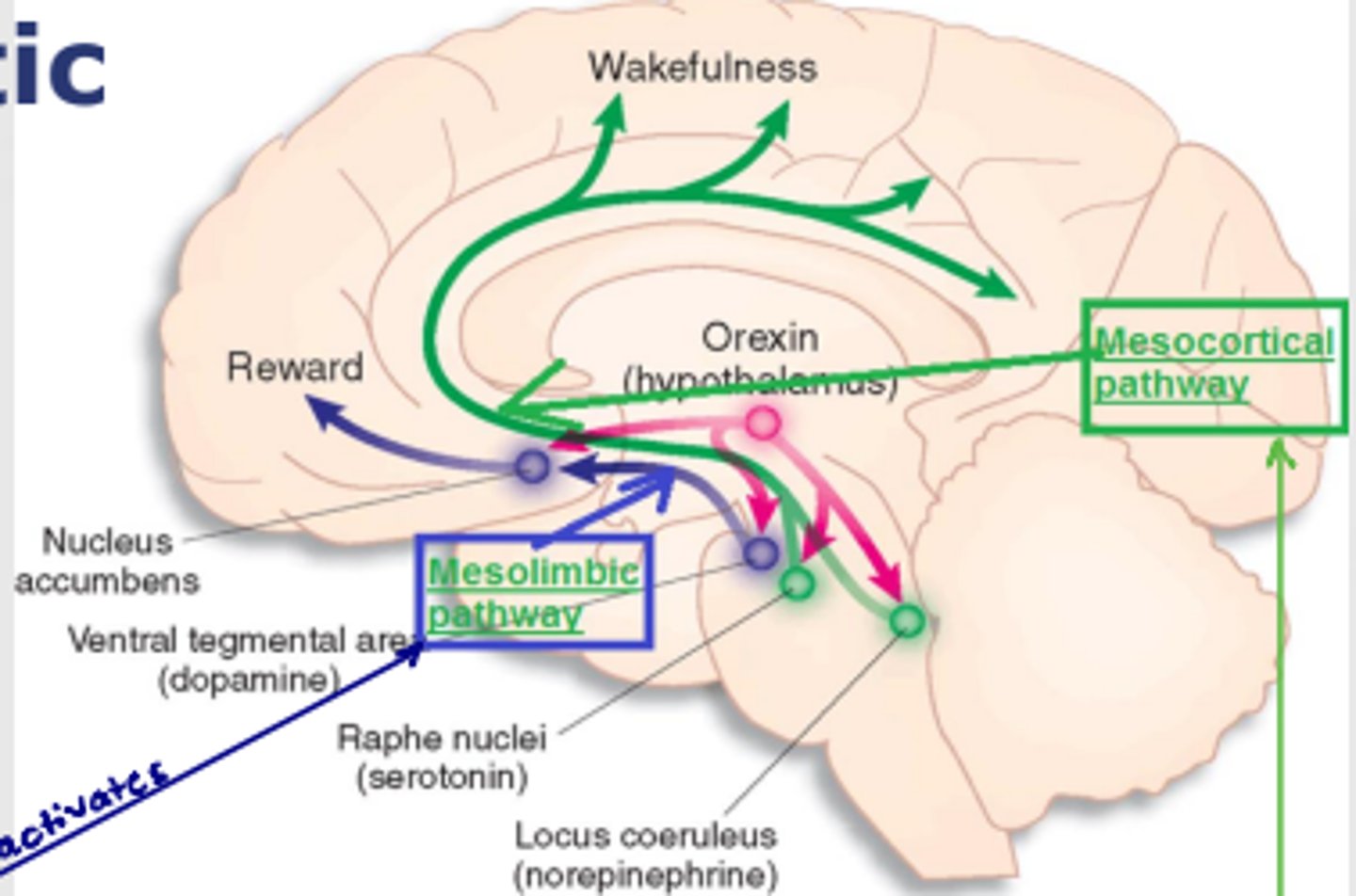
Revised dopamine hypothesis
Overactivity of mesolimbic pathway - positive symptoms
Mesocortical pathway dysfunction - Negative symptoms
location of mesolimbic pathway and mesocortical pathway
evidence of dopamine hypothesis
Amphetamines - dopamine agonist, stimulates nerve cells containing dopamine causing synapse to be flooded. - large doses cause hallucinations and delusions like a SZ episode
Antipsychotic drugs - antagonists they work by reducing the stimulation of dopamine system - many symptoms of SZ eliminated.
Evaluation of the dopamine hypothesis
+research support the role of dopamine - L dopa a drug for parkinsons that increases dopamine can produce SZ symptoms. SEEMAN found that Post mortems of SZ there was an increase in dopamine in parts of the brain
-cause and effect establishment - changes in neurotransmitter levels could be an effect of sz not a cause
- cannot see the sole cause, antipsychotics are effective for only 60% of cases. if it was soley dopamine it would work for everyone
-other neurotransmitters - Other NEUROTRANSMITTERS such as glutamate has evidence to show it has a role in negative symptoms Ripke et al to show that genes coded for dopamine and also OTHER neurotransmitters like glutamate habe a role in SZ
Neural correlates
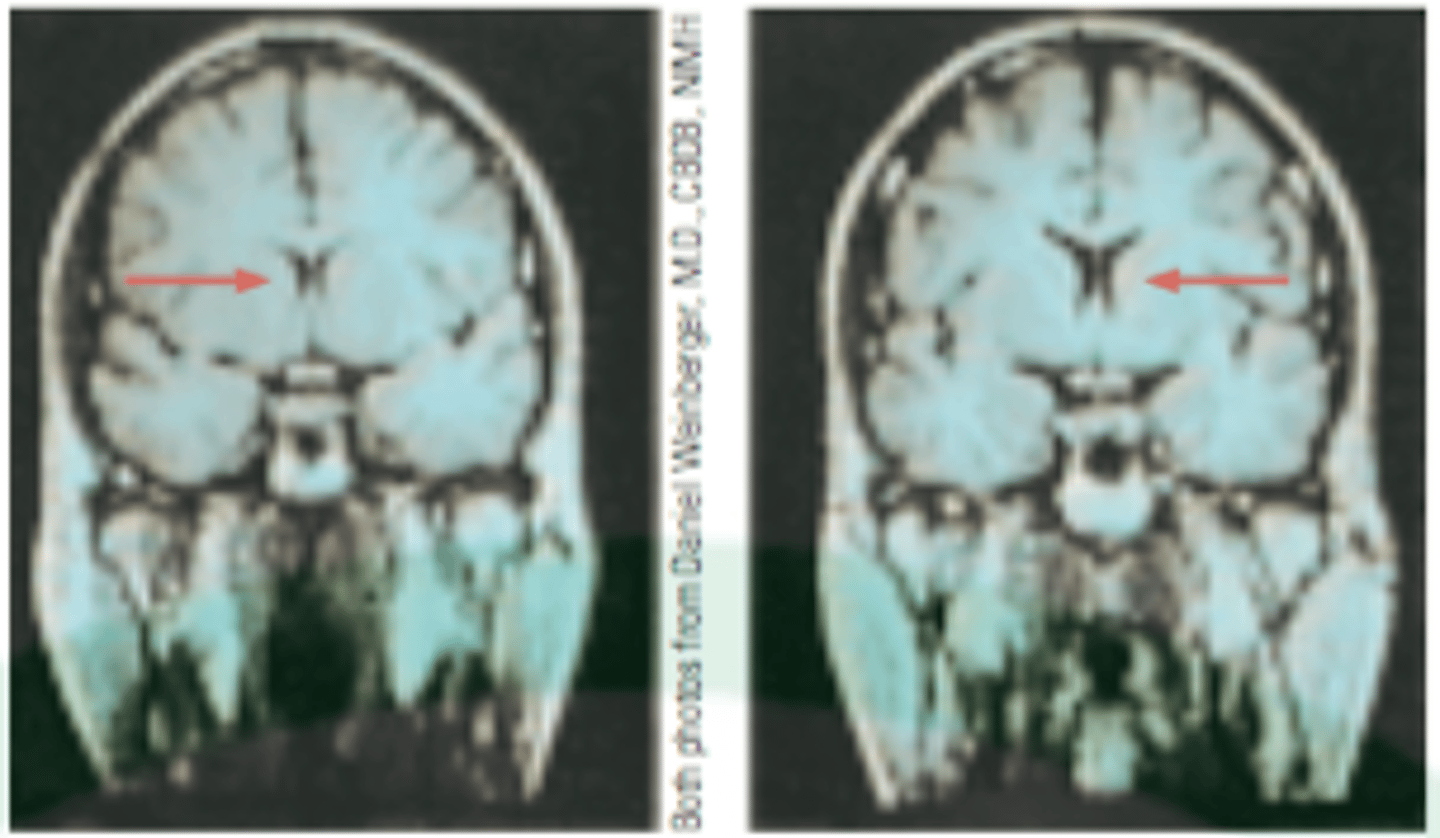
neuro imaging evidence has revealed structural differences in the brains between SZ and non SZ.
SZ have larger ventricles, fluid filled cavities. means sz brains are typically lighter than normal. 20-25% of sz have larger ventricles
how neural correlates relates to +ve and -ve symptoms
negative
activity in ventral striatum linked to development of avolition (loss of motivation), this area has been linked to anticipation of reward therefore if there is an abnormality in areas such as the ventral striatum then this would result in avolition
Positive
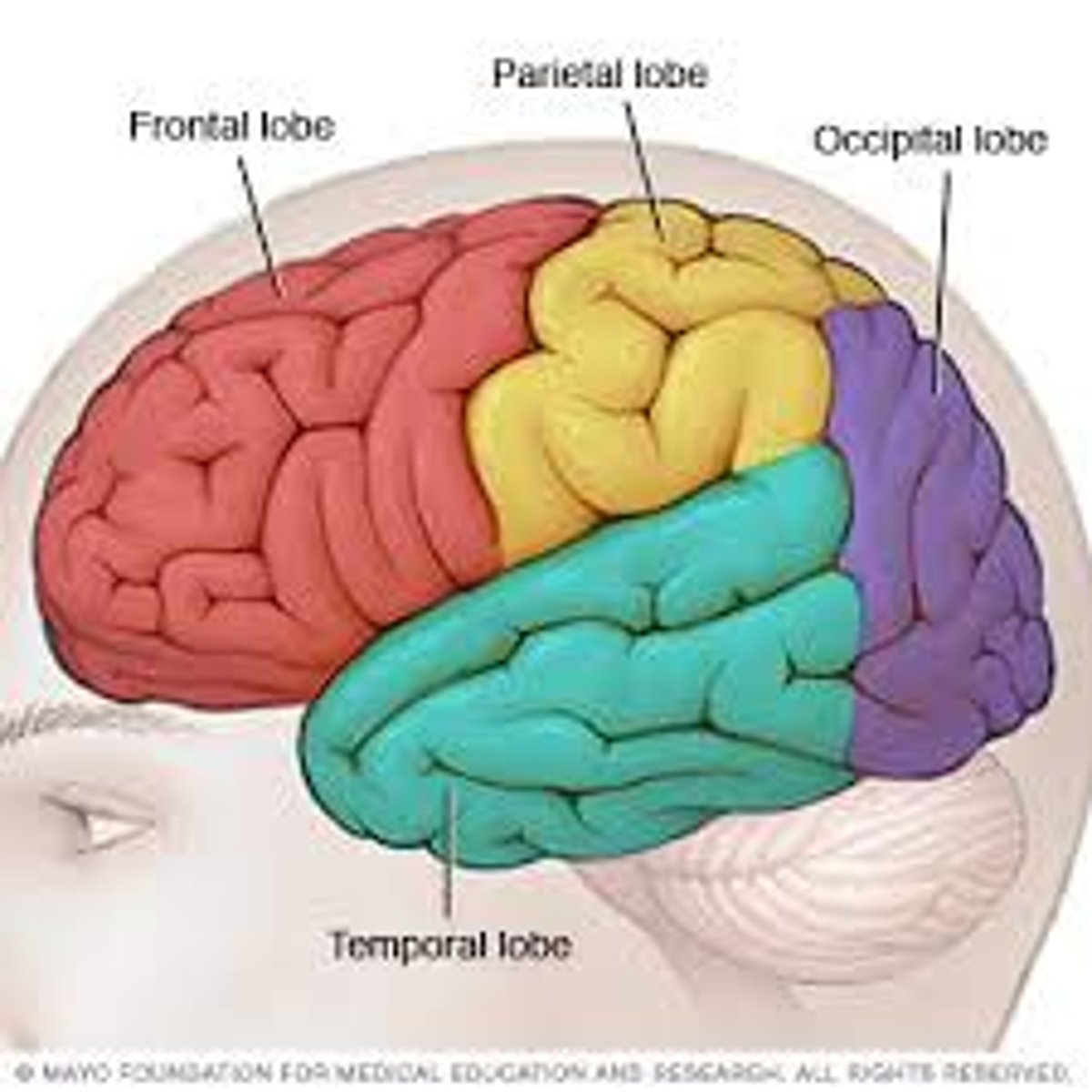
reduced activitiy in superior temporal gyrus and anterior cingulate gyrus have been linked to auditory hallucinations. patients with auditory hallucination showed lower activity in those areas
location of superior temporal gyrus and anterior cingulate gyrus
in temporal region near auditory cortex - near ear
Research evidence for neural correlates
Andreasen et al 1990 controlled CAT scan. Found enlargement in ventricals in SZ compared to controls
Juckel 2006 compared brain activity in SZ patients with controls and found the SZ patients had significantly lower activity in the ventral striatum
Allen et al 2007 compared brain scans of SZ with auditory hallucinations to a control. SZ group much less activity in the superior temporal gyrus and the anterior cingulate gyrus
neural correlates evaluation
- findings are inconsistent and therefore inconclusive. these correlations are not seen in all SZ sufferers
+MRIs have made it possible to investiage living brain images which is an advantage over relying on postmortems
- cause and effect relationship can not be established with brain abnormalities, these could be onset by having sz not causing it. in addition medication or symptoms of sz could cause these changes. eg medication could slow down activity in superior temporal gyrus
psychological explanations - family dysfunction
schizophrenogenic mother by Fromm-Reichmann
Double bind theory - Bateson et al
Expressed emotion
Schizophrenogenic mother
Fromm-Reichmann 1948
Many sz sufferers described their parents.
And several mothers fitted the SZG mother
the distrust and instability caused by such a prents was thought to introduce a sz reaction from their offspring
Mothers would show mixed signals, controlling overprotective, mood swings, cold dominant and creating conflict
Schizophrenogenic mother evaluation
-Parent blaming
-no longer a relevant theory, by the 1980s most research had disproven and found no correlation
-we cannot develop a cause and effect relationship even if the mother did fit catagories, it may be mother reacting to SZ child
Double bind theory
Bateson et al
focused on the role of communication within the family
in some families children can find themselves trapped in situations where they fear doing the wrong thing. they recieve contradictory information from parents.
double bind refers to these mixed messages eg children are punished for giving a hug and then punished again when parents gives them no reason for pushing away
‘mother tells child theyre no affectionate enough, but when they hug them they get pushed away’
—> By being given these mixed messages they learn not to trust messages from others. as a result they don’t trust their own feelings and perceptions, get confused and lose grip on reality—> leading to negative symptomssuch as social withdrawal and affective flattening
Double bind evaluation
-parent blaming
+research support Berger - SZ reported higher recall of double bind statements from mother
-contrasting hall and levin found no differents in parental communication
Expressed emotion
refers to level of emotion, particularly negative emotion expressed towards patients by carers or parents
thoughts or emotions of parents can create anger or negative thoughts which is a source of stress for the patient cause of SZ or trigger or relapse
Can include verbal criticism hostility and anger E
expressed emotion evaluation
Research support Brown - families where expressed emotion was high resulted in 58% of people with SZ returning to hospital for further treatment, compared to only 10% of those from low expressed emotion families
Cause vs Effect - it is unclear whether ee is a causal in relapse rates or just families reaction to sz behaviour
Metholodogical issues -levels if ee are collected through an interview with patient rather than study of their environment etc or a more detailed
Psychological Explanation - Cognitive
Meta Representation - the cognitive ability to reflect on your own thoughts and behaviour. Disruption to this takes away ability to distinguish our own thoughts and actions from others —> leads to positive symptoms like hallucinations and dellusiosn
Central control — cognitive ability to suppress automatic responses while we perform deliberate actions. Poor central control results in failure to distinguish between behaviours of conscious intent and that of automatic response. eg what should I do vs What i want to do —> leads to positive symptoms such as catatonic behaviour and disorganised speech
impaired selective attention - process by which the brain selects what stimulus to respond to. In normal processing the brain allows us to filter and direct attention correctly
Helmsley states SZ had difficulty attending and blocking out stimuli
Pickering stated breakdown in in auditory selective attention makes social interaction difficult.
—> causes negative symptoms such as social anhedonia
Evaluation for cognitive
Liddle and Morris found SZ perform poor on stroop test showing they have impaired selective attention or poor central control
-doesnt explain what causes these cognitive changes and therefore does not offer understanding on original cause of SZ- limited explanation
-cognitive distortions may be a symptom of the disorder rather than aa casue —Cause and Affect
+has practical application in therapy
-Garety said SZ is better understood by linking together explanations —> interactionist more appropriate
Biological treatments - drug therapy
Typical -1950s bind to dopamine receptors(d2 receptors) and block their action , by reducing stimulation of dopamine this can eliminate positive symptoms such as hallucinations and dellusions, the use of these led to the dopamine hypothesis. taken as tablets 2-4 times per day, dosage can be increased if needed - eg Chloropromazine
Atypical - newer type found in 1990s- eg clozapine or riseridone
claim to combat positive and negative symptoms
they act on dopamine system and block serotonin receptors
they also bind to d2 receptors but rather than permanently blocking they temporarily and then seperate to allow normal dopamine transmission
Drug treatment evaluation
-Lieberman 2005 - 1000 patients, 74% discontinued drug therapy due to side affects
55% on typical relapses compared to 42% on atypical
Sampath et al - placebo study - typical is clearly affective
Melzer - atypical is more affective than typical and is especially useful when patients dont respond to typical
Cognitive Behabioural therapy for SZ CBTp
NICE recommend all sz patients get cbtp
4 main aims:
1 to challenge and modify dellusionary beliefs
2 to help the patient identify delusions
3 to challege delusions through looking at evidence
4 to help a patient begin to test reality of evidence
stratageies
1 trace back origins of symptoms
2 evaluate content of dellusions and hallucinations
3 Behavioural assignments to improve functioning
4 distraction from intrusive thoughts
5 encourage increasing/decreasing social actrivity to distract from low mood
6 using relaxation stratagies
CBTp procedure
1 assessment
2 engagement- therapise engages with patients perspective and feelings
3 ABC model
4 Normalisation - knowing other people also have these feelings reduces distress
5 critical collaberative analysis - gentle questioning to understand and dispute dellusions
6 developing alternative explanations - patient develops their own alternative ideas for previously unhealthy assumptions
CBTp Evaluation
+can be combined with drug therapy to provide better outcomes
+research support Drury et al shows a reduction in positive symptoms such as hallucinations and dellussions
-not widely availible
-not suitable for all patients as they may not be able to engage
-works better after initial phase has slown down particularly afterdrug therapy
-usualyl studies alongside drug therapy
Family therapy
focusses on helping family members support someone with SZ
Relatives need support as looking after someone with sz is demanding
medical boards say every patient should be offfered this
through out understanding of expressed emotion we know that people with sz are more likely to relapse if families are criticising and hostile
Family therapy aims to reduce high ee and reduce relapsefa
family therapy process
2 therapists
3-12 months min 10 sessions
1 ensure or family members have all information they need
2 encourage everyone to ask questions
3 views of every family member listened to including patient often patient will be asked to talk about their symptoms and discuss them
4 goal is to provide the whole family with coping skills and enables to manage everyday difficulty associated with sz
Family therapy evaluation
Hogarty 2 year follow up 25% of those with family therapy replapsed compared to 62% of just drug therapy
-more of a management not a treatment
-not appropriate for all patients without family
-social desirability, family might be embarrseed to might not want to engage properly or act differently around therapist
Token economy - psychological therapy
tend to help with positive symptoms
adjusts behaviour to be more suitable to everyday world - reduces institutuionalisation
use operate conditioning - positive reinforcementp
principle of token economy
tokens can be exchanged for something patient wants
examples of behaviour could be washing, eating, bieng kind
tokens act as secondary reinforcers
which get exchanged for primary reinforcers
there needs to be a clear system of how tokens are allocated and what is rewarded
applying token economy to sz
baseline data about behaviour recorded
initially tokens are frequent (frequency of token dispensal is called reinforcement schedule) by gradually decreasing this individuals should learn to display behaviour without token
Token economy evaluation
Comer - claimed we cant establish cause and effects since researchers arent using control groups, may be other factors involves such as increased attention from staff
+research support dickerson et al 11 out of 13 studies reported psotive affects from token economy
+produces better relationships between pateitn and psychiatrists
-not affective in long term outside of instituation
do not eliminate hallucinations of dellusions meaniong its more of a managment tool rather than treatment
interactionist approach
diathesis stress
vulnerability and a stressor
eg Meehl found a SZ gene a vulnerability
Read et al found childhood trauma as a vulnerabilityE
evaluation interactionist
+tienari et al adoption study, more at risk if bio parent had sz but then adoptive parents had high criticisim low empathy
+houstan et al childhood seggsual trauma vulnerability and cannibis use could be a trigger
+more hollisttic, more than one type of treatemetn can be used which means different symptoms can be targetted.