Dialysis
1/41
Earn XP
Description and Tags
exam 3
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
42 Terms
dialysis overview
replacing work that kidneys used to be able to do
uses a synthetic semi permiable membrane to clean and return blood to the patient
different types
when kidneys fail need treatment to replace the work of your kidneys
= the movement of fluids and molecules across a semi permeanble membrane from one compartement to another
what dialysis does
loosens and separetes (impurities) from the blood
separates and removes:
toxins
excess electrolytes
fluids
used for acute and chronic renal failure
morbidity and mortality with dialysis
10% of people who need dialysis die per year
cause of death mainly related to cardiovascular problems
younger patients do better than older
non-diabetics do better than diabeteics
most patients under 55 are encouraged to get transplant instead of life ling dialysis
management choices for renal failure
diet and medication management
until renal function (GFR) 10-15% (stage 5)
dialysis (types)
peritoneal dialysis
hemodialysis
continuous renal replacement therapy (CRRT)
transplant
indications for dialysis
severe azotemia
BUN > 90mg/dL
creatinine > 9 mg/dL
drug toxicity
fluid overload
metabolic acidosis
pericarditis
encephalopathy
about 10%-15% of kidney function
severe fluid and elelctrolyte imbalances
hyperK
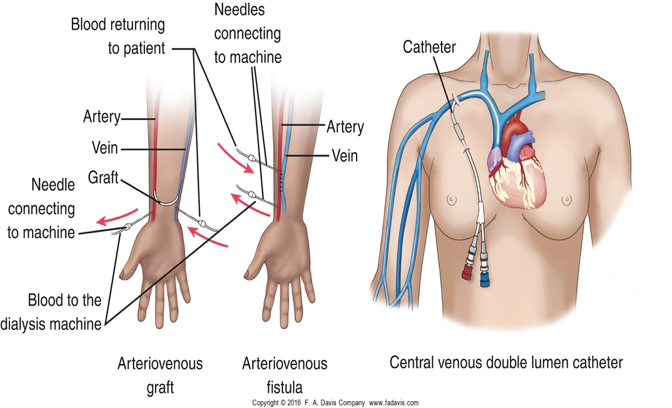
vascular access
used for hemodialysis
site on body from which your blood is removed and returned
usually prepared weeks or months before start dialysis
the site allows for easier and more efficient removal and replacement of blood with fewer complications
3 main types of venous access devides
central venous catheter
AV fistula
AV graft
central venous catheter (CVC)
used for emergecy situations
via IJ, femoral vein, or subcalvian
immediate access to the pts circulation for acute hemodialysis is achieved by inserting a doubel lumen non coffee large bore cath into vein
pros and cons of CVC
pros
can be used right away
no needles are needed to connect to the dialysis machine
cons
temporary access
prone to thrombosis, hematoma, infection, pneumotorax
may not have the blood flow needed for enough dialysis
need protective cover over catheter to take a shower
can cause barrowing of major blood vessels
Arteriovenous fistula (AV-Fistula)
fuses a artery and a vein of someones arm
surgically created: rapid flow for optimal hemodialysis
Repeated use of an AV fistula can cause bulging (pseudoaneurysms) that make the vessel larger and feel stronger, but actually damage the vessel structure, making it lower quality and more fragile over time.
cannot be used immediately after surgery
TAKES 2-3 months to mature
lasts about 3 years (or 10+?)
best option for hemodialysis “fistula first”
pros and cons of AV fistula
pros
last longer
not prone to infection
provides excellent blood flow once it is realy to use
less likely to develop blood clots and become blocked
able to take showers once the access heals after surery
cons
needs to mature 1-4 months before can be used
needles are inserted to connect to the dialysis machine
clotting may be a problem that may require surgery or other treatment to correct
needles are inserted
3 types of hemodialysis compared
nursing care for AV fistula/graft
check patency QID (4 times a day)
listen for bruit and feel for thrill
no blood draws or BP on affected extremity
watch for bleeding post dialysis
AV graft
usd for pts with inadequate blood vessels
created subQ inserting graft ,aterial between artery and vein
2-5 weeks to mature
lasts about 2 years
infection
thrombosis
stenonis
AV graft pros and cons
pros
provide axcellent blodo flow once it is realy to use
you can take showers once the access heals after surgery
cons
lasts less time than a fistila
more prone to infection that a fistula
needs at least two weeks before it can be used
clotting may be issue
needles inserted
teaching for fistulas and grafts
DO’s
use lanolin lotion to prevent dry skin
check bruit freqiently
leave patches in place for 4-6 hours post dialysis (report porlonged bleeding or oozing)
use medic alert bracelet
report anything unusual
DON’Ts
no blood draws, IVs or BP on affected extremity
no tight clothing, jewelry, or ID band over access site
do not lift heacy itens with teh access arm
do not allow pt to bump access extremity
do not scratch or pick at scabs
arterial venous needles
two needed: 14fr or 16fr
one carries blood to the dialyzer (pull)
one returns cleaned blood to body (push)
bleeding from access site
warning signs
bleeding from fistula or graft that lasts more than 20 mins after dialysis treatment is over
any bleeding from a catheter site or tube
actions to take:
for bleeding from a fistla or graft, gently press teh access with a clean gauze pad to stop the blood; if bleeding lasts more than 20 mins call doctor
for bleeding from a catheter site or tube call doctor immedietly
hemodialysis overview
done by a dialysis nurse
about 3 times a week, 4-4.5 hour session (plus ½ hour pre and post)
done either out patient or on dialysis floor
hemodialysis uses
used both for short term acute illness and longterm for patients with CKD and end stage renal disease
prevents death but does not cure renal disease
does not compensate for the loss of endocrone or metabolic activities of the kidneys (example: creating RBCs)
contraindications of hemodialysis
severe cardiac disease —> due to inability to tolderate fluid and electrolyte shifts
bleeding disorders - inability to coagulate
hemodynamic instability —> someone who has low bp or high HR
how demodialysis works
removes wastes and water by circulating blood through external filyer
blood flows in one direction and the dialysate soluation flow in the opposite direction of blood
urea and creatinine are removed from the blood
what happens: blood leaves through arterial needle a few oz at a time, heparin added to prevent clotting, then travels through dialyzer and back to pt
principles of dialysis
osmosis
movement of fluids across selective permiable membrane from an area of low concentration to high
diffusion
movement of dissolved particles across a semipermiable membrane fron an area higher concentration to an area of lower solute concentratoin
removes waste products from blood
filtration
process of passing fluid through a filter or semipermiable membrane
ultrafiltration
controlled fluid removal by manipulation of hydrostatic pressure
care of the dialysis pt *
before starting
weight
same scale, wearing same clothing, same time of day
vitals
pulse may increase during dialysis due to decreased BV
BP may decrease
monitor for dysrhythmias
monitor temp - may indicate infection: check for cold ss, cough, pain, check access site
listen for breath sounds
HF is frequent complications
check for edema - face, feet, hands
keep constant schedule for dialysis
dialysis is straining on glient - will be tired
check emotional status - can be difficult and drianing
check for medications
some are dialyzed out so might hold
use critical thinking to avalute anti hypertensives and dysrhythmic meds
Post dialysis care
check weight
should be lower
typically use 1-2 L of fluid
temp
may be slightly elevated
BP
should be lower- if hypotensive may require bed rest
pulse may increase due to fluid changes
RR may slow
assess for bleeding (heparin given)
if bleeding apply firm pressure
haparin remains in system for 4-6 hours
check for muscle cramps
common problem du to remobal of large amts of fluid at rapid rate
meds
admister meds that were held
hemodialysis complications
infection
bacteremia
edocarditis
exposure to blood born pathogens
hep B and C
disequalibrium syndrome
disequalibrium syndrome
typically new HD, results from shift between CSF and blood
develop cerebral edema
ss: mild HA, mental confusion, seizures, NV, restlessness, fatigue, increased BP
severe ss: agitation, twitching, confusion, convulsions
nursing action: slow down dialysis rate
frquently assess pt
peritoneal dialysis
wastes and fluids are removed from the blood inside the body, across peritoneal membrane
a dialysate solution is intermittently introduced into and removed from the peritoneal cavity through a catheter
uses: diffusion, filtration, osmosis
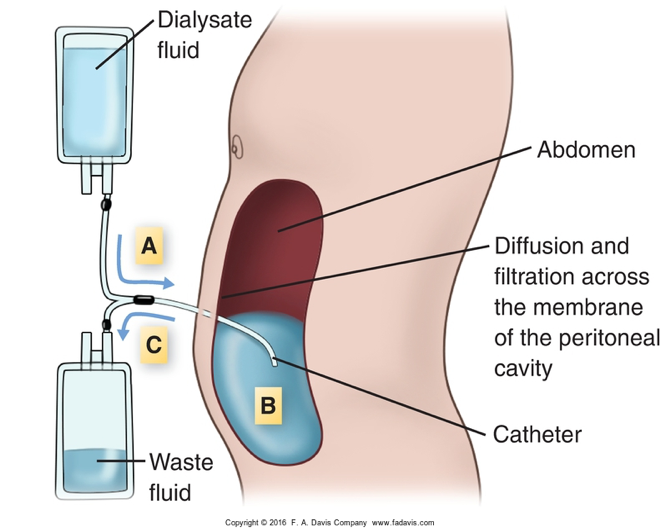
peritoneal dialysis catheter
flexible tube inserted into the peritoneal cavity to facilitate dialysis.
usually used after waiting about 2 weeks (can be used within a couple days if needed)
use of peritoneal dialysis
treatmemt choice for pts w renal failure who are unable or unwilling to do hemodialysis or renal transplant
more independant
can be managed at home or in hospital
great for pts with:
cardiovascular disease
diabetes
advanced age or young age
exchange process is slower and less stress on the cardiovacular system
automated peritoneal dialysis
Continuous Cycler-assisted Peritoneal Dialysis (CCPD)
Requires a machine called a cycler to fill and drain your abdomen, usually while you sleep
Done in home setting
Portable so patient can travel
manual - tontinuous ambulatory peritoneal dialysis
portable system done by nurses or pt
2L of warm dialysate infused through catheter by gravity then clamped
empty dialysate bag folded and placed in pocket or pouch and pt can move around
pt unfolds bag and drains dialysate into it using strict aseptic technique
new bag of dialysate is hung, and again drains into abdomen
cycle is repeated
3 phases of peritoneal dialysis
infusion/fill
infused over about 10 mins
dwell
20-30 mins, up to 8 hours depending on method
drain
10-20 mins
note: PD usually takes 36-48 hours to acheive what hemodialysis accomplished in 6-8 hrs
disadvantages to peritoneal dialysis compared to hemodialysis
contrainvicated with: severe obesity, severe COPD, abnormalties of peritoneal membrane
need clean home with space for supplies
family/pt must know sterile technique
dialysis must be sterile
glucose in dialysate
more concentrated to remove fluid
may need insulin
les efficient
takes more tome to achieve desired outcome
high risk for infection —> peritonitis, catheter site infection
hernias and pleural leak
catheter can clog or become displaces
cant be used after recent surgery
hypertriglyceridemia
nursng care of peritoneal dialysis
I&Os
check /weigh output bag
weights
vitals
ss of peritonitis: elevated temp, cloudy drainage, pain)
aseptic technique
assess for:
constipation
abdominal cramping
prevent catheter clogging
peritonitis - complication of peritoneal dialysis
assess for ss: cluody effluent (liquid waste), and pain, rebound tenderness, N?V, fever
obtain effluent sample for culture
administer antibiots as ordered
tach pt and family ss and prevention
exit site infection - complication of peritoneal dialysis
monitor site daily for ss of infection: induration, erythema, purulence and hyperthermia
increase daily cleaning of site
apply topical antibiotics as ordered
teach pt and family to avoid agents sich as creams and lotions around exit site
catheter tunnel infection - complication of peritoneal dialysis
assess fro ss of infection: pain along tunnel, induration for several sm away from catheter, erythema leading away from exit site, and drainage at exit site or as tunnel is “milked” towards exit site
teach pt and fam to avoud pulls ro tugs on the catheter or traima to exit cite
emphasize the need to maintain cleansing regimen at exite site
fluid obstriction - complications of peritoneal dialysis
change position of patient
irrigate catheter
enure that sufficient fluid is in abdomen (sometimes requires a residual reservoir)
complications of peritoneal dialysis (pain and more)
rectal pain
ensure a sufficient reservoir of fluid
use slow infusion rate
shoulder pain
ensure that all air is promed from infusion tubing
attempt draining the effluent with client in knee chest position
hernia
monitor for increase in size of or pain in area of nernia
decrease volume of exchnages as ordered
dialyze with client isupine position
use abdominal binder or support for pt
avoid initiation of PD until exut sit healing has taken place
fluid overload
peripheral edema, crackles in lungs, chnages in wt
dehydration
dehydration
skin turgor, muscle cramps, hypoTN, tachycardia, dizziness
if dehydrated: discontinue hypertonic soluation and increase PO fluid inatke
CRRT dyalysis (continuous renal replacement therapy)
indications:
used for hemodynamically unstable pts —> often multi system failure
process
fluid, electrolytes, small to medium sized molecules are removed by slow continuous ultrafiltration
may be used in combination with dialysis
process can continue up to 30-40 days
slow continual - momics kidney
managed by critical care nurse
types
contunuous venocenous hemodialysis diffuse
continuous venovenous hempfiltration concention
methods are similar - require access to the circulation and blood to pass through an artificial filter
hemo filter is used in all types
advantages of CRRT
does not produce rapid fluids shifts
does not require dialysis machines or personnel
can be initiatided very quickly
done by ICU nurses
useful for pts who cannot tolerate HD, PD, or require large amounts of fluids
complications for CRRT dialysis
fluid and electrolyte imbalances
acid/base imbalance
hemorrhage from anticoagulation or distruption of filter or tubing
infection
rupture of filter
clotting in filter
loss of vacular access/clogged catheter is very common