HTHSCI 2H03 - Medication Safety & Pharmacodynamics: Cellular Receptors & Drug Action
1/81
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
82 Terms
Medication Safety - Lecture
Mistakes of Medication Administration
- Frequent problem = 1 med error/patient/daily.
- Significant use of resources: 700,000 ER visits & 120,000 hospitalizations/year for adverse drug events.
- Cause of death: 7,000 deaths/year from med errors.
- Costly: $3.5 billion/year on medical costs associated with drug events.
- ICU patients and children at higher risk (when fragile state; weight consideration; children med lower dose; already on so many medications = greater risk for error).
Case Scenario #1:
A 19 year-old patient with leukemia is prescribed the following chemotherapy:
- Vincristine 10mg IV x 1 (given as a slow IV push).
- Cytarabine 70mg IT x 1 (given intrathecally- in the spinal canal = so it can enter cerebrospinal fluid).
- Two syringes arrive on the oncology unit later that day.
- The patient’s nurse grabs a syringe from the medication room and brings it to the physician to perform the lumbar puncture.
- Soon after the procedure it was realized that vincristine was given intrathecally instead of intravenously (when given wrong most times = death).
Contributing Factors:
- Look-alike medications (both dispensed in syringe).
- Distractions, stress, confirmation bias (just assume).
Error-Reducing Strategies:
- Independent double check (high-alert medication).
- Auxiliary labels “for IV use only."
- Standardizing dilution of vincristine in minibags.
- Education on chemotherapy agents.
Medication Error
*DOES REACH the PATIENT*
- Preventable event that occurs during prescribing, transcribing, dispensing and/or administering and may or may not cause harm.
- Medication errors are preventable, frequent events that can result in significant patient morbidity, mortality and increase health care costs.
- Multiple environmental and human factors contribute to medication errors.
- Many strategies of varying power can be implemented to reduce the incidence of medication errors.
- Documentation and analysis of medication errors is important to determine their root causes and future preventative strategies.
- Omission = Drug error.
- Ex. Physician prescribes an incorrect dose of insulin. The patient develops hypoglycemia.
- Ex. A patient was started on IV vancomycin twice daily for a blood stream infection. The nurse is busy with her other patients and forgets to administer the evening dose.
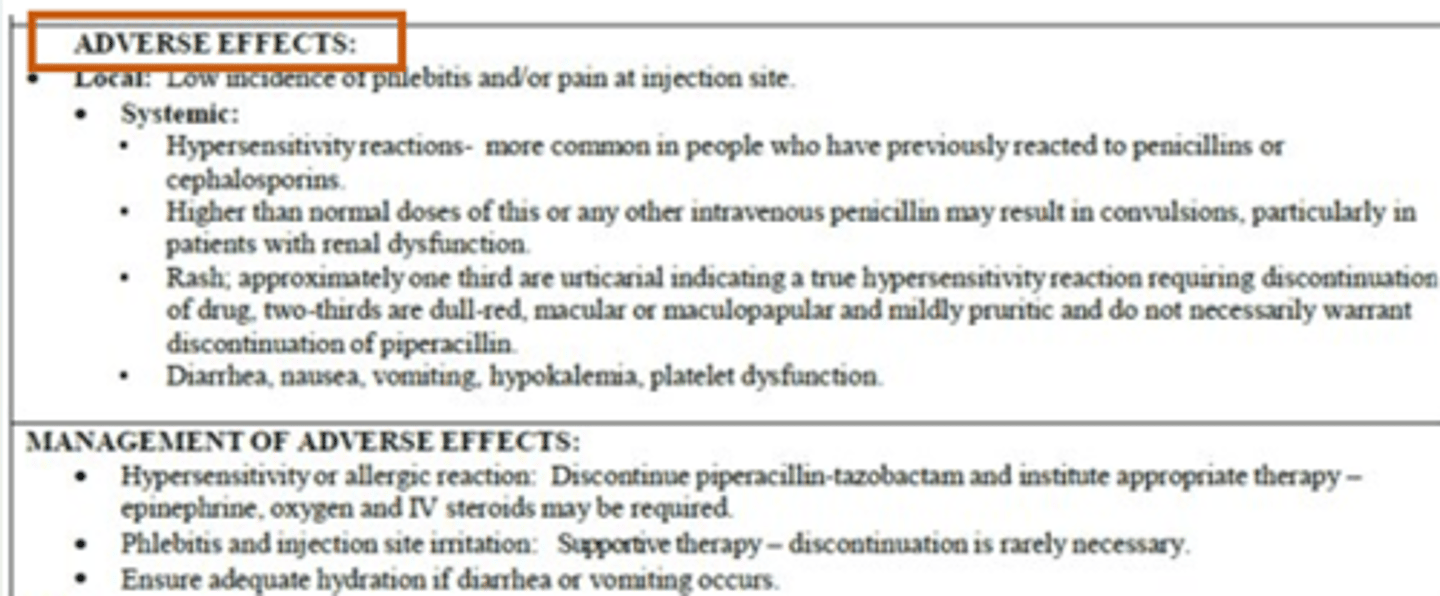
Adverse Drug Event (ADE)
- Harm resulting from use of a drug or the lack of a drug.
- Does not exactly mean drug error has occurred (done by nurses, caregivers, family).
- An error may or may not have occurred.
- Ex. patient presents to the emergency department with seizures after being non-compliant with their anticonvulsant, phenytoin.
- Ex. A patient is who is on the blood thinner, warfarin, is prescribed an antibiotic for their urinary tract infection. The patient experiences a brain bleed due to a drug interaction between the antibiotic and blood thinner.
Adverse Drug Reaction (ADR)
- A type of adverse drug event that occurs at normal doses that results in an undesired, unintended, or unexpected reaction (harm) to a medication.
- Includes: side effects, allergies.
- Ex. A patient is prescribed morphine for pain and experiences significant constipation
- Ex. A patient does not rinse their mouth after using their steroid inhaler and develops thrush (fungal infection in mouth/throat).
Vanessa's Law
- Protecting Canadians from Unsafe Drugs Act.
- Mandated reporting of serious ADR (ex. hospitalization, cancer, death) to Health Canada.
Near Miss
DOES NOT REACH PATIENT
- An event that could have harmed the patient but fails to do so because of an intervention.
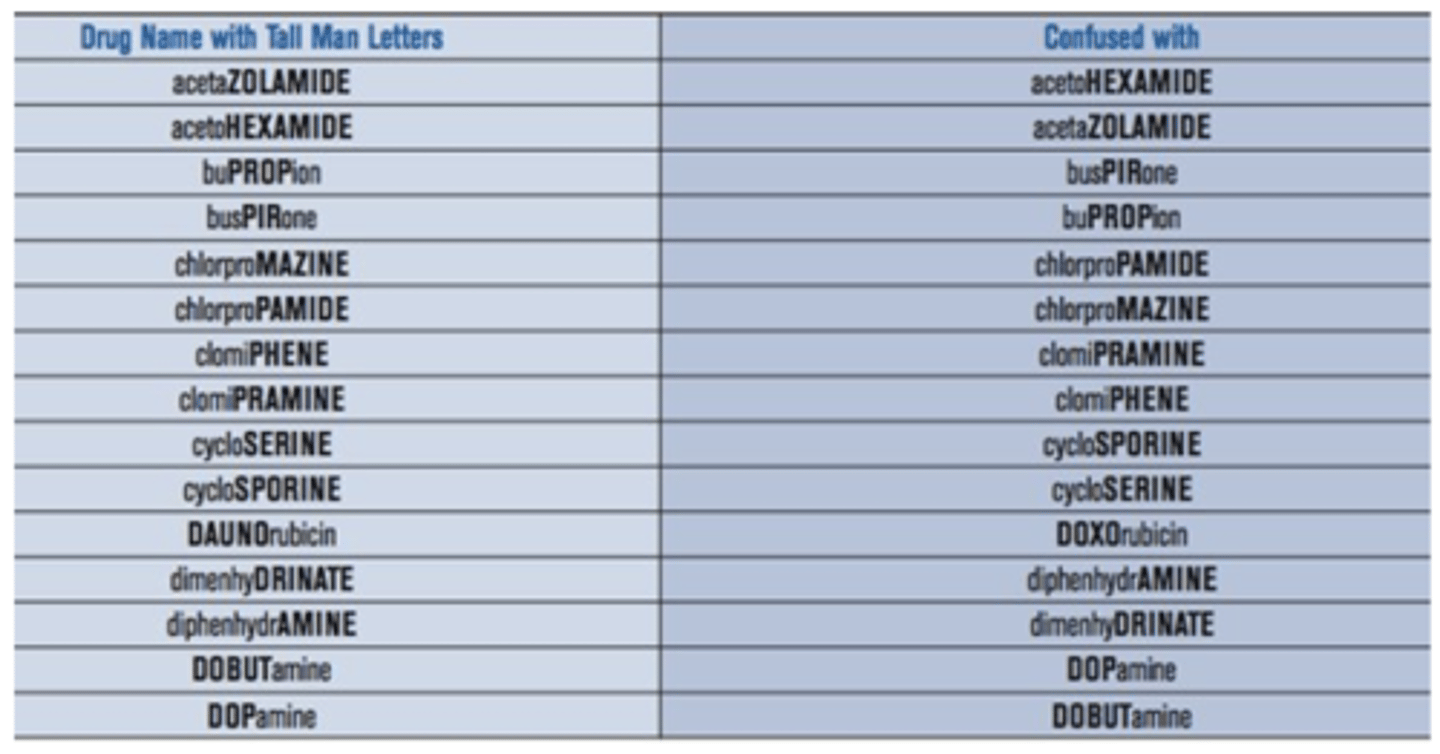
- Ex. Pharmacy dispenses dimenhyDRINATE 25 mg instead of diphenhydrAMINE 25 mg as ordered, however, the dispensing error is noted by the nurse and the incorrect medication is NOT administered to the patient.
- Ex. A nurse is about to administer acetaminophen for a fever but notices that the medication expired last month. They withdraw a second acetaminophen dose from the automated dispensing cabinet that has a future expiry date and alerts pharmacy about the expired product.
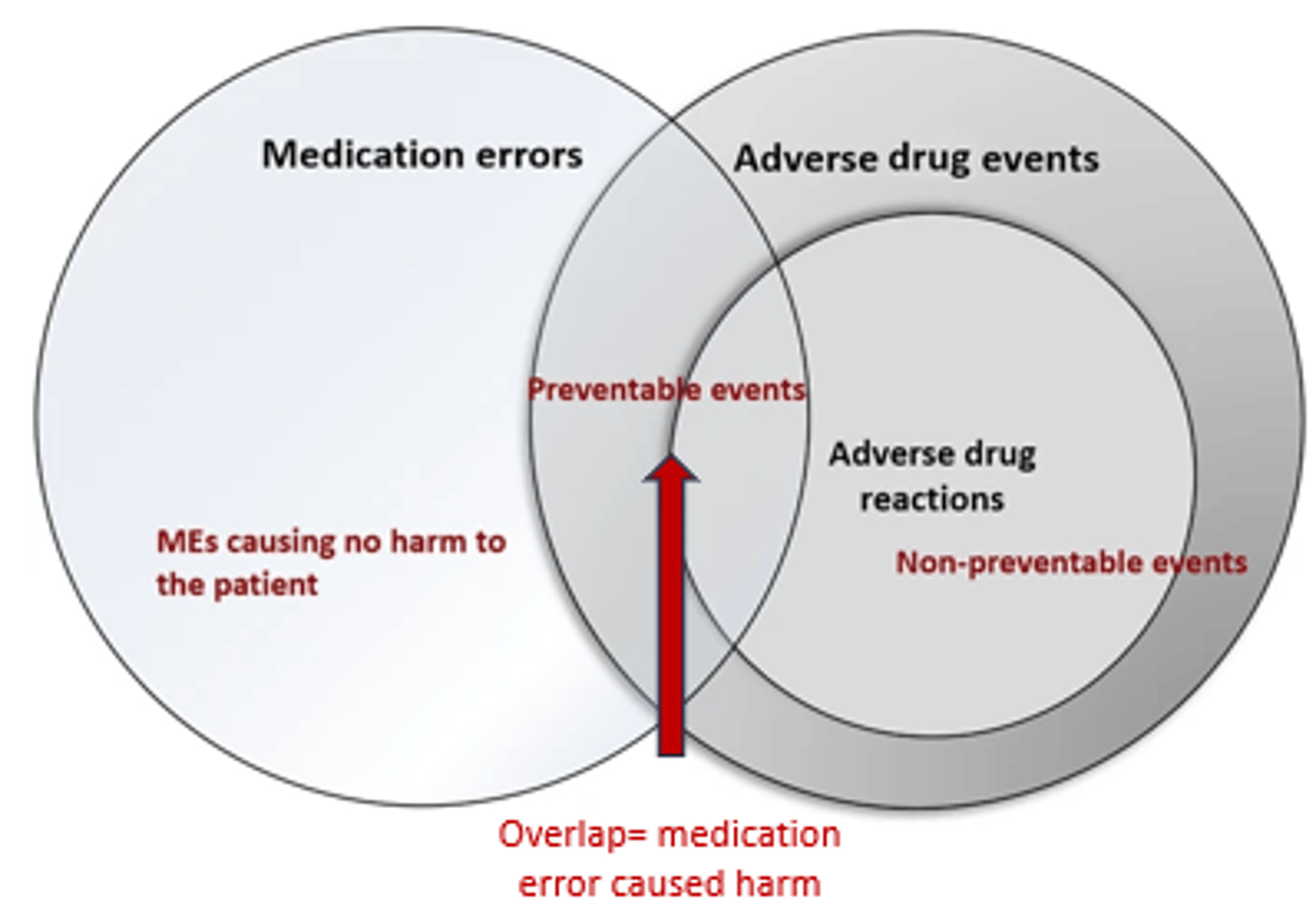
Medication-Related Adverse Events Diagram
- Non-Preventable: Because using drug correctly at the right dose.
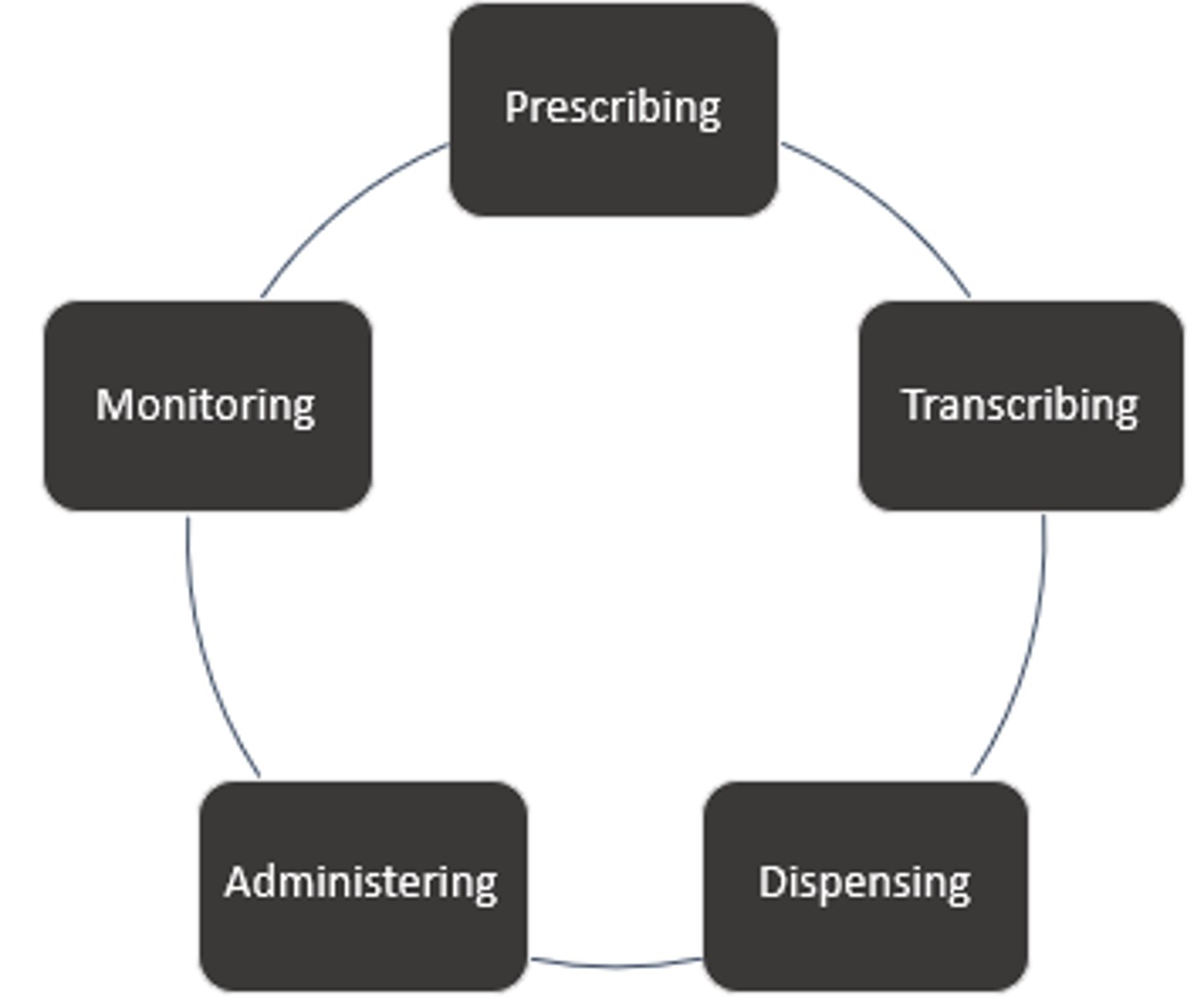
Medication use Process
- Transcribing: Paper-based system's ONLY (must be verified by a pharmacist).
- Administering: Nurses role.
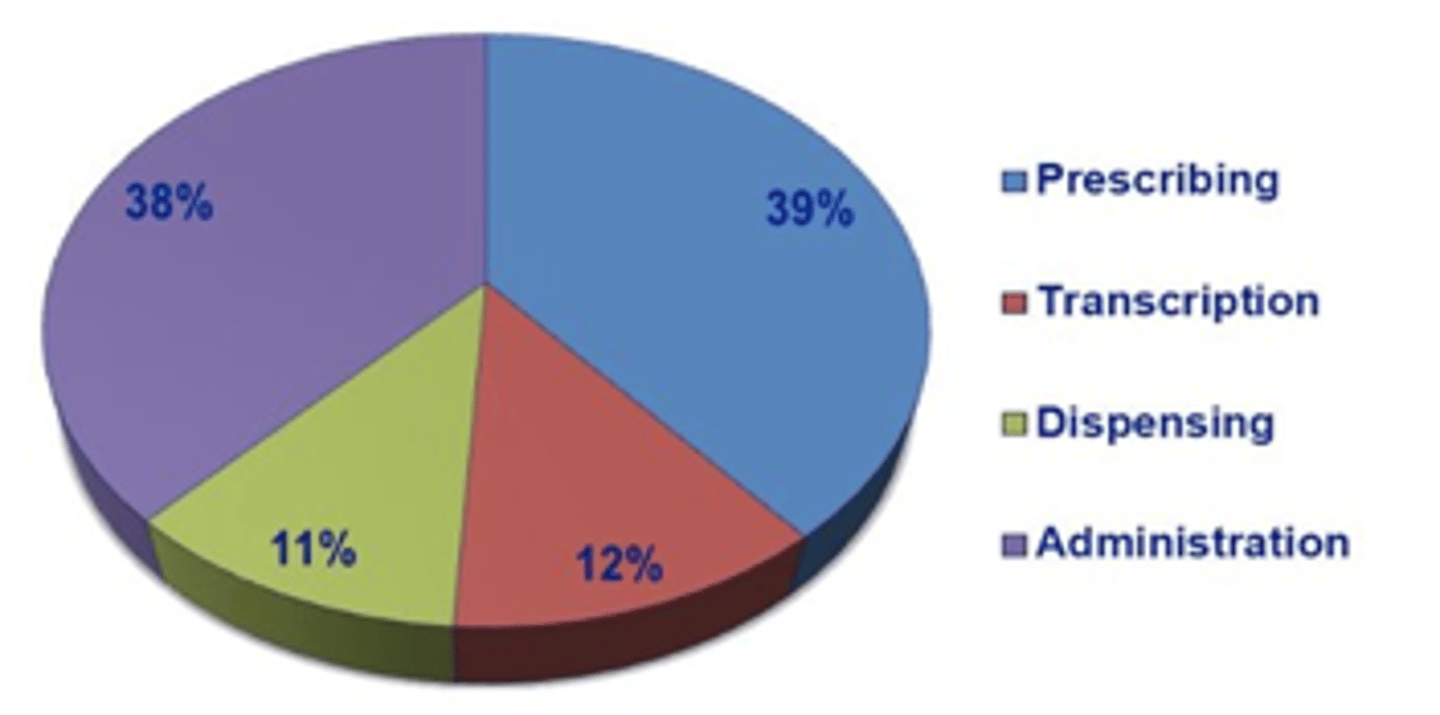
Medication Error %
*Nurses and pharmacists catch 30-70% of medication errors.
Prescribing
- Inadequate knowledge of indication, contraindication, or drug interactions.
- Patient factors such as allergies, pregnancy, renal impairment not taken into account.
- Inappropriate drug, dose, route or administration time.
- Poor communication when giving verbal orders.
Transcribing
- Medication transcribed at incorrect time or frequency.
- Not transcribed at all.
- Illegible handwriting.
- Misusing abbreviations.
- Decimal errors.
- Instead of writing (5mL, write 0.5 mL to accidental overdose).
Dispensing
- Incorrect medication, dose (including calculation), route or quantity dispensed.
- Medication labeled inappropriately.
- Incorrect storage.
- Room temperature vs fridge.
- Expired product.
Administering
- Incorrect patient, medication, dose (including calculation), route or time/frequency.
- Wrong rate selected on IV pump.
- Administration omission.
- Avoid "medication not available."
- Failure to document administration and vice versa.
Environmental/Human Factors Contributing to Med Errors
- Inadequate lighting.
- Messy work area.
- Distractions (noise, telephone, interruptions).
- Stress.
- Poor staffing.
Swiss Cheese Model of Medication Error's
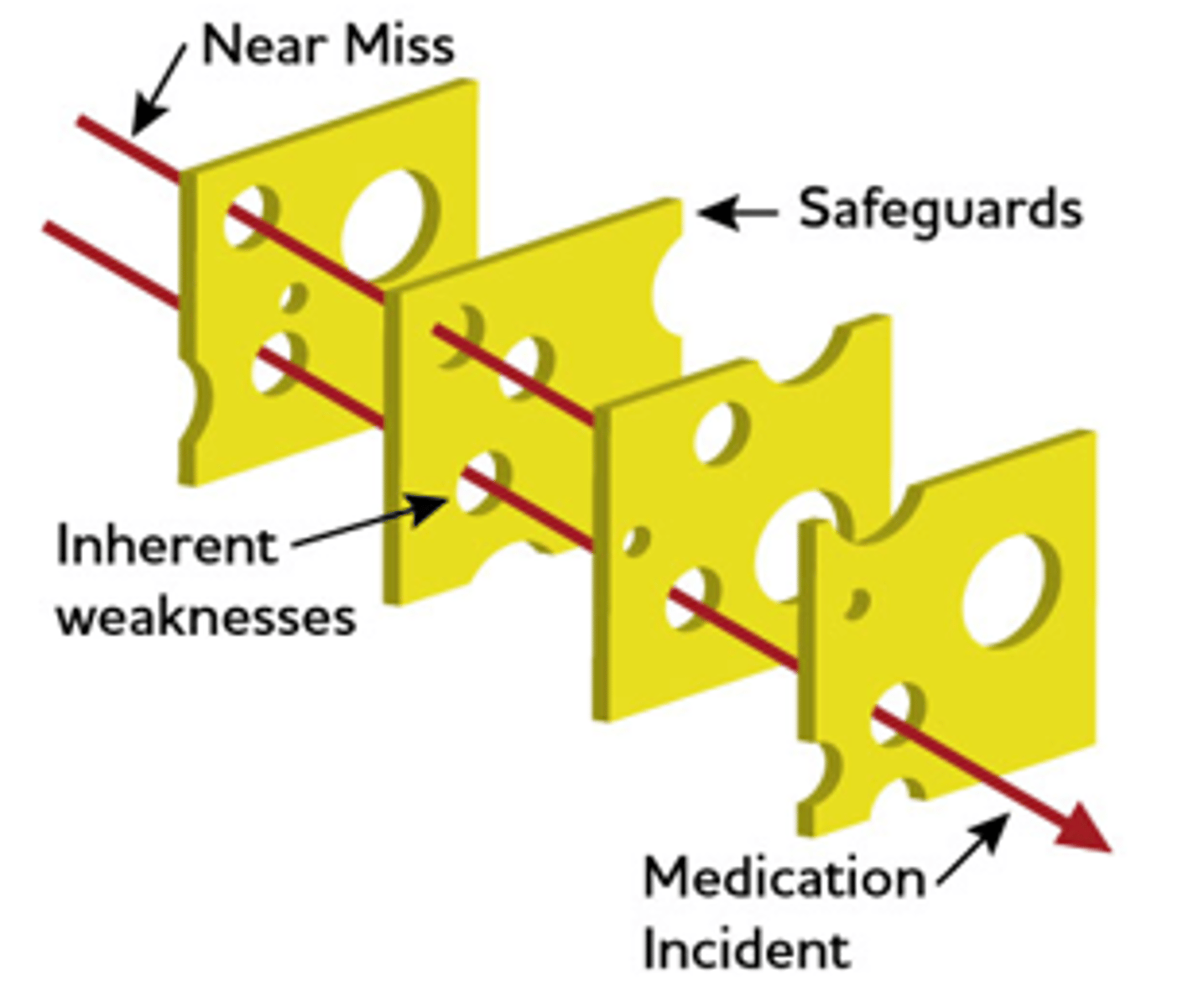
Medication Error Reduction Strategies
*Most effective to look at system as a whole.
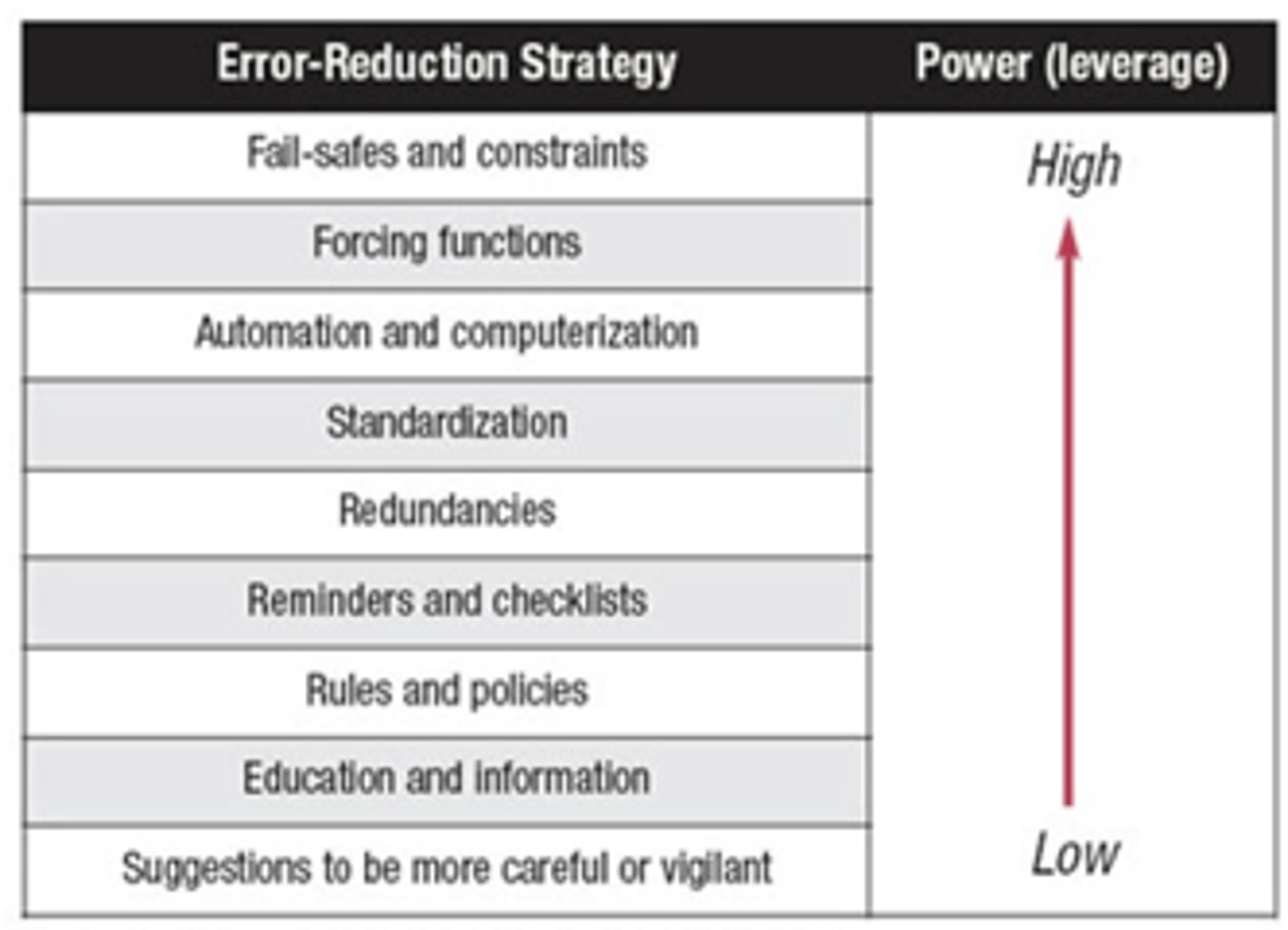
Fail-Safes & Restraints
- Get pharmacist to verify before nurse administration.
Forcing Functions
- Scanning patient barcode before administration.
Redundancies
*Double-check for high-alert drugs.
Reminders & Checklists
- MAR notification.
High-Alert Medications
- Medications that have an increased risk of causing patient harm if they are used incorrectly
- Ex. Insulin, opioids, anticoagulants, chemotherapy and potassium chloride
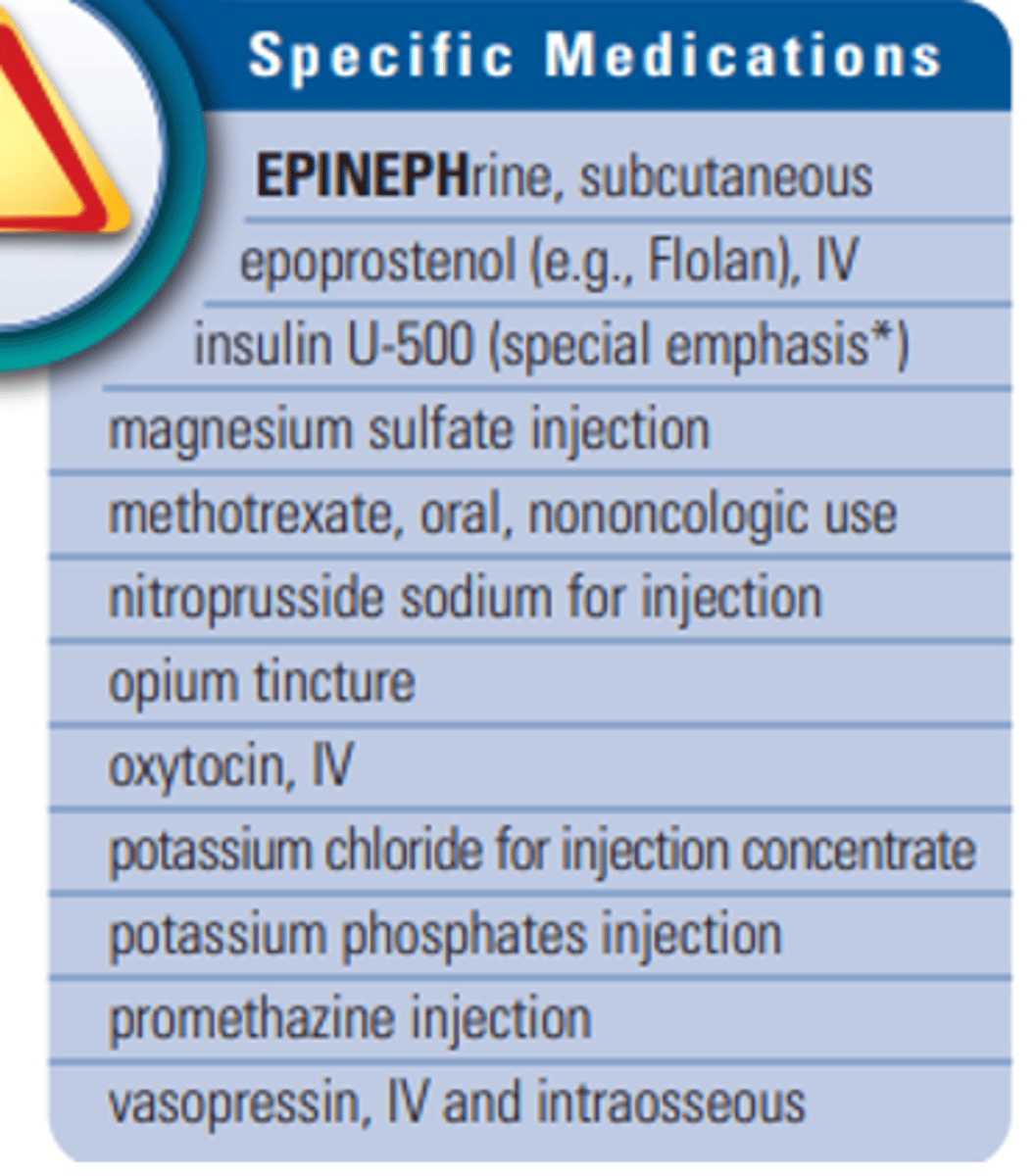
ISMP (institute for safe medication practice) High-Alert Medication List
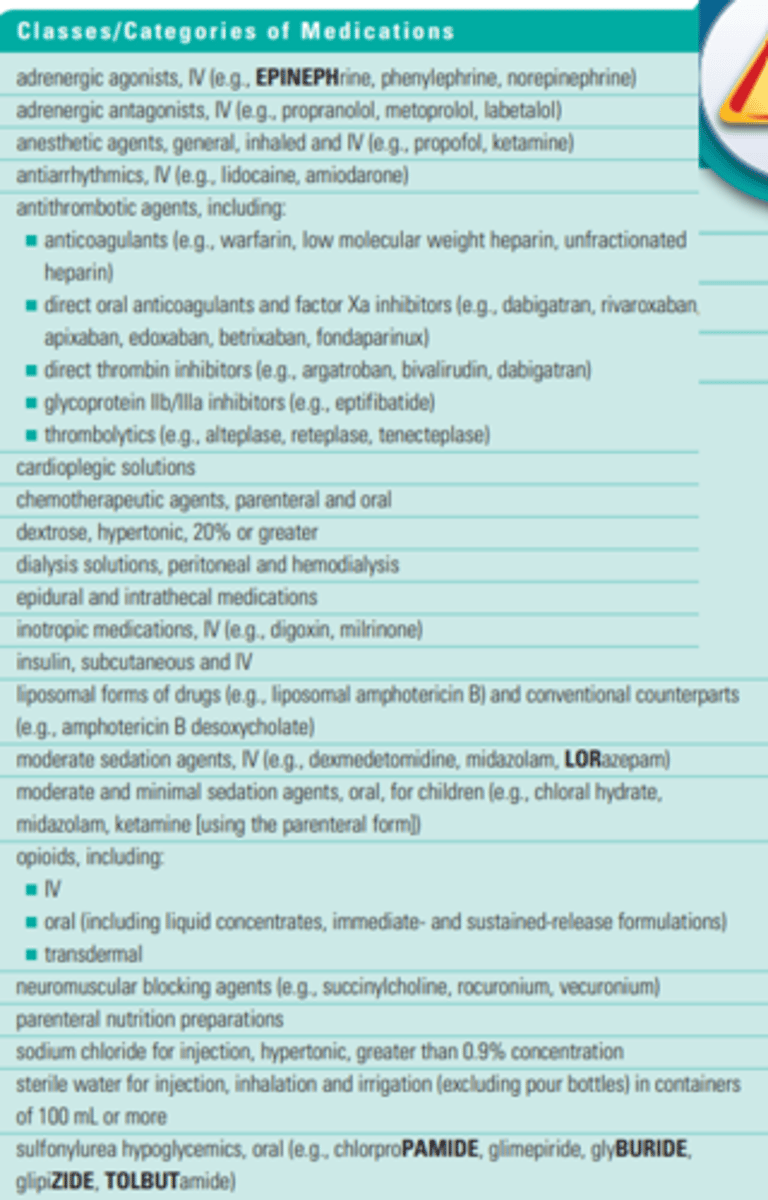
Specific Medications - ISMP High-Alert Medication List
Independent Double Check
- Especially important for “high-alert” medications and “high-alert” routes of administration ie. epidurals, intrathecal medications.
- If done correctly, can detect up to 95% of errors
- Must be done INDEPENDENTLY.
- Incorrect: Holding up a syringe and vial of insulin and saying: “This is 10 units of insulin glargine, is this correct?”
- Correct: Providing a second health professional with the syringe, vial of insulin and the order or MAR and saying: “Would you check this for me?”
Dangerous Abbreviation & Symbols
- 1.0 mL: 1 mL
-.5 ml: 0.5 mL
- 10 U: 10 units
- SQ: Subcut or subcutaneous
- qd: Daily
- ug: Microgram
- > or <: Greater or less than
- MS: Morphine sulfate, magnesium sulfate
- D/C: Discharge or discontinue
*O never after, only before.
Don't Understand a Prescription?
- Ask another nurse.
- Call physician or pharmacist.
- Clarify with available resources.
- Double check!
- Be mindful of: Pediatric dosing; Generic vs. brand names.
Look-Alike/Sound-Alike Medications
- Physically separate on pharmacy shelves and in automated dispensing cabinets (i.e. Omnicell, Acudose, Pyxis).
- Use both generic and brand names on medication packaging.
- Use Tallman lettering in electronic systems and on medication packaging.
- Purchase one of the products from another source so vials look different.
- Ex. Look-Alike: Bupivacaine vs. Pantoprazole.
- Ex. Look-Alike: Verapamil vs. Naloxone.
Tall-Man Lettering Table
Confirmation Bias
- Expecting to see what you're familiar with, regardless of the actual information.
- Clinicians see the drug name or dose they are most familiar with, which may result in error.
- Ex. dimenhyDRINATE (anti-nauseant) vs. diphenhydrAMINE (antihistamine).
- Ex. Celebrex (anti-inflammatory) vs Celexa (anti-depressant).
Computerized provider order Entry (CPOE)
Prescribers enter orders electronically via a computer application such as Epic or Cerner:
- No illegible orders.
- Avoids transcription errors.
- Alerts prescribers to allergies, drug interactions, dose limits etc.
- Has been shown to reduce medication errors by 46-88% in US hospitals.
Bar Code Medication Administration (BCMA)
- Scanning a patient's wristband and intended medication to confirm the "rights" of medication administration.
- Can be linked with clinical decision support to alert nurse to important information such as allergies, vital signs, critical lab value.
- Most systems automatically prompt documentation on an e-MAR (medication administration record).
- Shown to reduce medication errors by 48%.
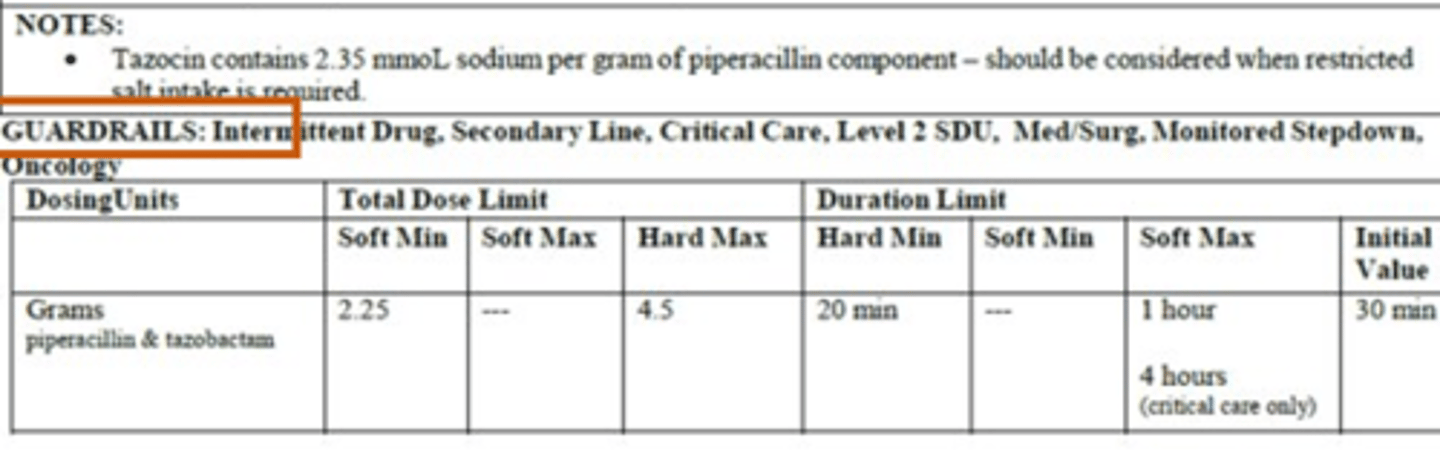
Guardrails
- Pump contains a drug library with limits specific to each medication to ensure medications are administered safely.
- Ensure administration of appropriate concentration, dose, and rate and help prevent medication errors.
- Use for all IV intermittent medications, IV continuous infusions and TPNs.
Soft vs. Hard
- Soft can be overridden.
- Hard can not be overridden.
Soft Minimum - Guardrails
- Minimum dose or rate for a given medication that can be administered (alert can be overridden by nurse after clinical check).
Soft maximum - Guardrails
- Maximum dose or rate for a given medication that can be administered (alert can be overridden by nurse after clinical check).
Hard Maximum - Guardrails
- Maximum dose or rate for a given medication that can be administered (alert cannot be overridden; pump will not allow administration).
IV Monographs Example Part #1
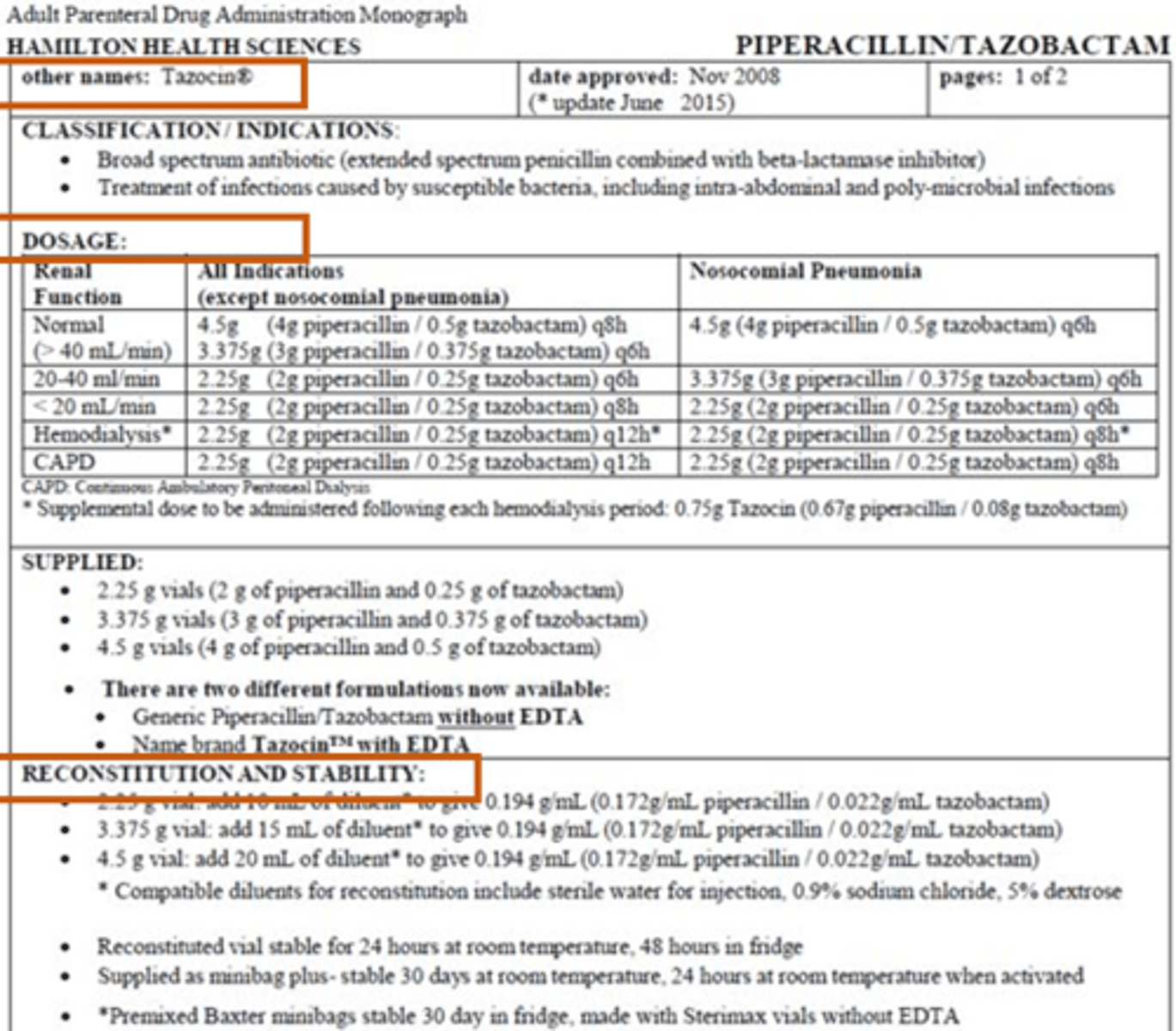
Reconstitution & Stability
- How to prepare drug from vial.
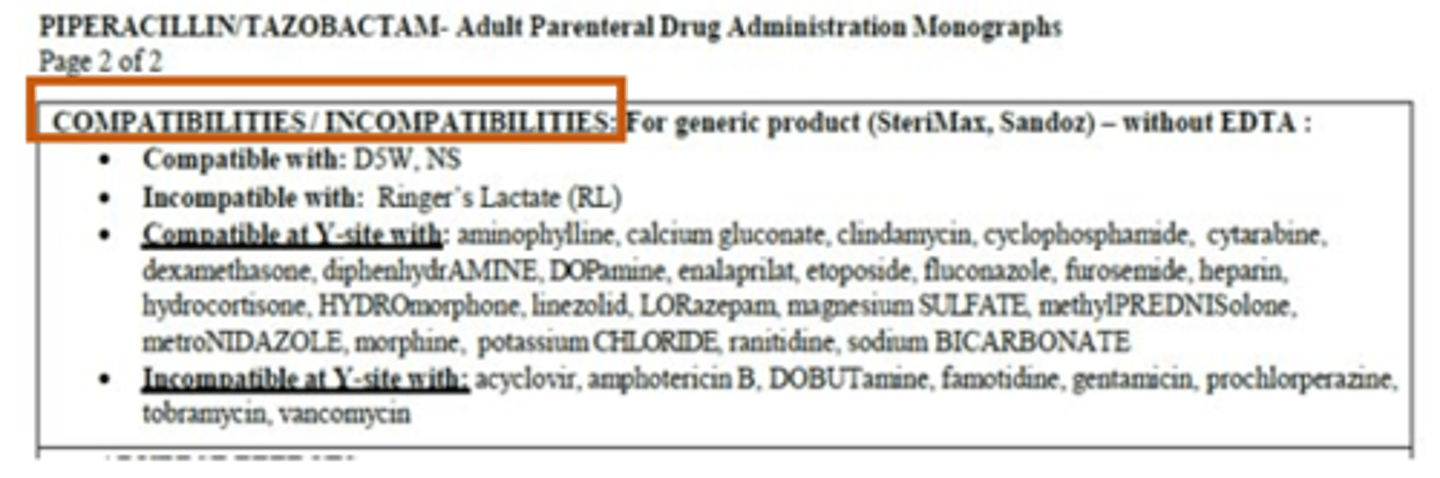
IV Monographs Example Part #2
Compatibilities & Incompatibilities
- Y-site: Drugs that are administered separating but eventually meet which can cause incompatbilities.
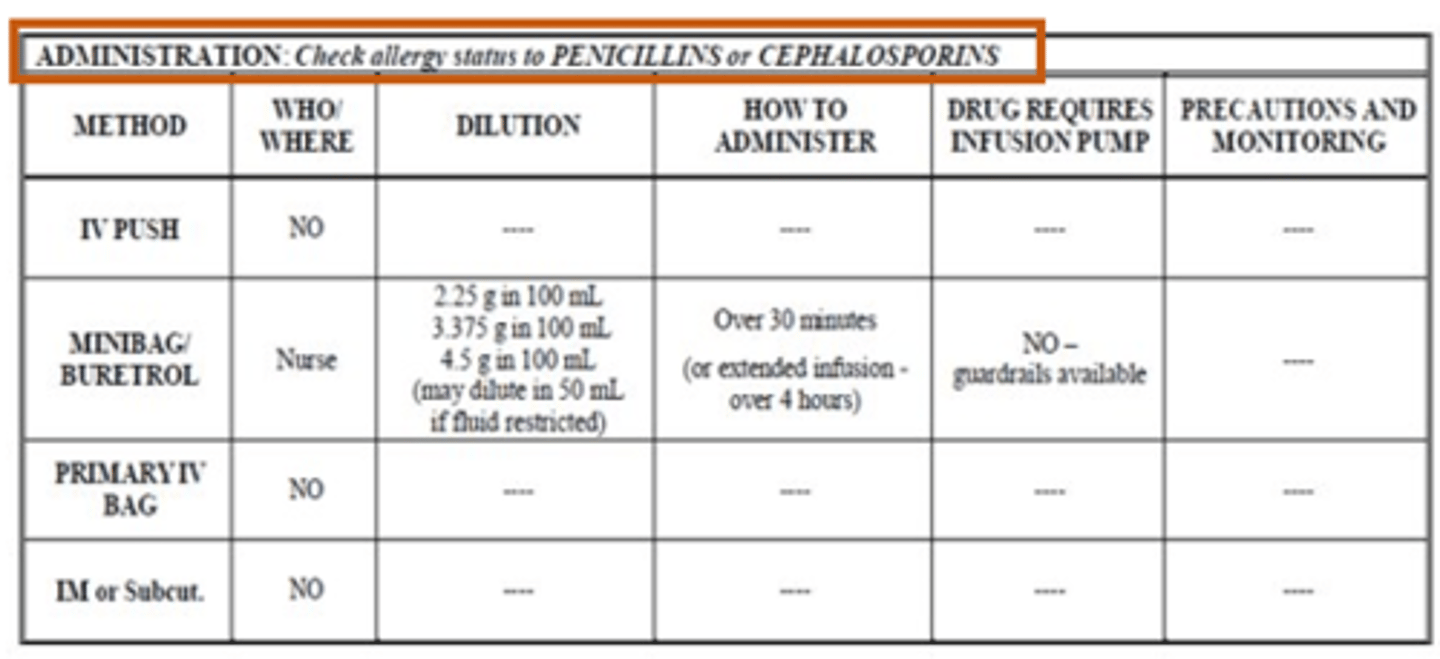
IV Monographs Example Part #3
IV Monographs Example Part #4
IV Monographs Example Part #5
Resources for IV Monographs
- Your pharmacist.
- Lexicomp/Uptodate/Micromedex.
- King IV compatibility guide.
- Compendium of Pharmaceuticals and Specialties (CPS) (Canadian reference including Health Canada approved drug monographs, vaccine information and product identification).
Medication Reconciliation
- A process where healthcare providers gather an accurate and comprehensive medication list and ensure it is communicated across transitions of care.
- Can be performed on admission, transfer or discharge.
- Allows prescribers to make the most appropriate prescribing decisions.
- Done by pharmacists, nurses and/or physicians (clarified with prescriber).
Medication Reconciliation - Step #1
Best Possible Medication History (BPMH)
- Process of obtaining a list of a patient’s prescribed and non-prescribed medications using a systematic process of interviewing the patient/family and ideally reviewing at least one additional reliable information source.
- Includes medication, dose, route and frequency.
- Sources may include pill bottles, pharmacy list, long-term care home MAR.
- Document list and keep list up-to-date!
Medication Reconciliation - Step #2
Reconciliation
- Compare medications currently ordered on admission, transfer and at discharge to previously ordered medications.
- Clarify that additions, changes and discontinuations are intentional and appropriate.
- Communicate discrepancies to prescriber to prevent/correct medication errors.
Documenting Medication Error
- Important to document all near misses, medication errors and adverse drug events.
- Chart in patient’s medical record.
- “Safety Occurrence Report” at Hamilton Health Sciences.
- Serious or unexpected medication reactions or reactions to recently marketed products should also be reported to Health Canada – Vanessa’s Law.
- Most errors are due to systems failure not human failure.
Root Cause Analysis
- An in-depth systems review after a critical medication error to identify underlying causes.
- Conducted with an interdisciplinary group including person(s) involved in the medication error, front line staff and management.
- Impartial and sensitive to conflicts of interest.
Goals:
- Determine what happened.
- Why it happened.
- How it can be prevented in the future.
- Not to assign individual blame.
Pharmacodynamics: Cellular Receptors & Drug Action - Lecture
Drug Binding - Affinity & Agonism
A drug’s affinity for a receptor tells us how well the drug binds to the receptor, but does not tell us anything about the action of the drug at that receptor.
Agonists:
- Full agonists.
- Partial agonists.
- Inverse agonists.
Antagonists (*occupy receptor, but do nothing*):
- Reversible, competitive or non-competitive antagonists.
- Irreversible antagonists.
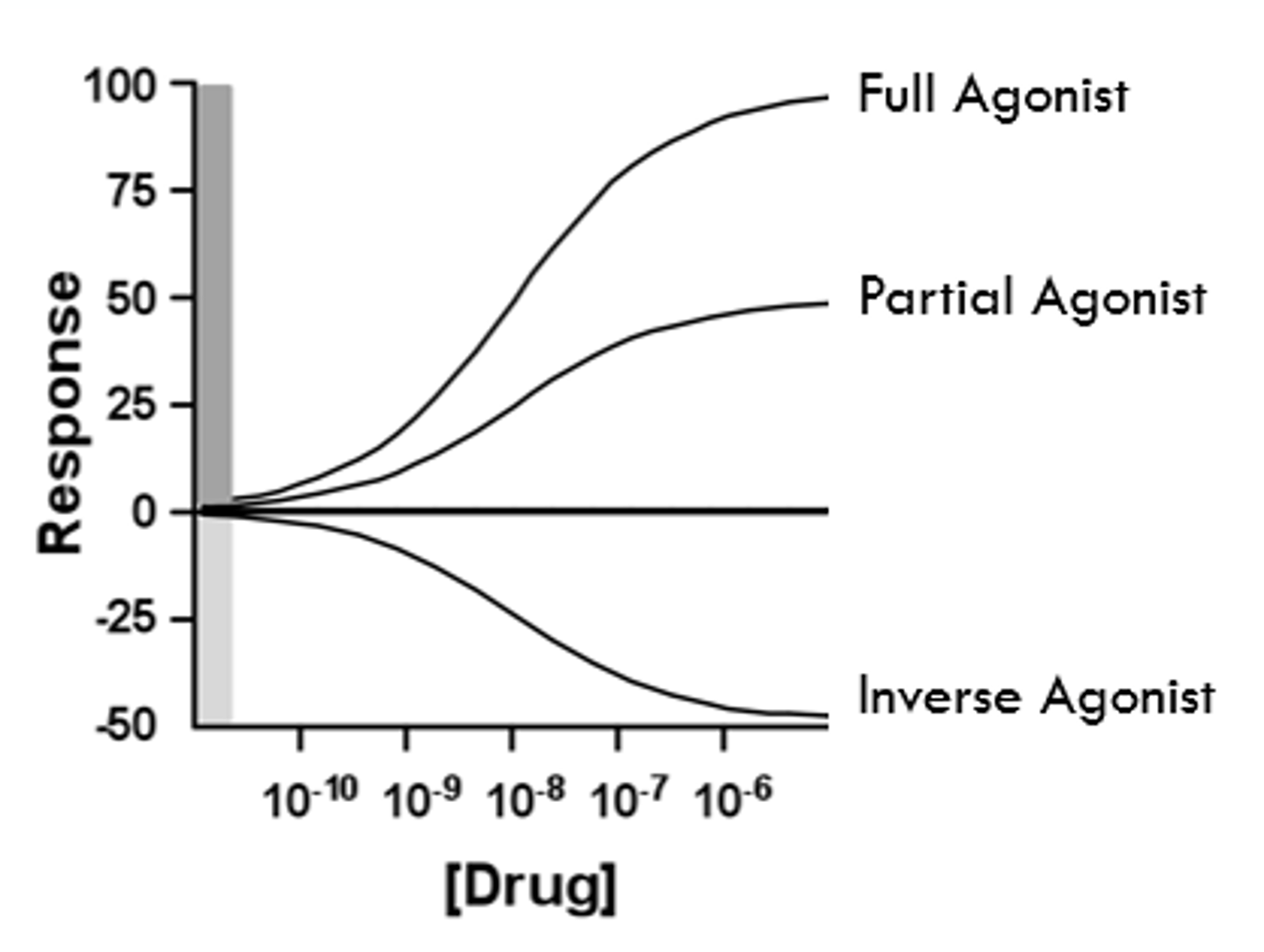
Full Agonist's
- Bind to the same receptor site as the endogenous ligand and produce the same biological effect as the endogenous ligand at that receptor site.
- Ex. Dexamethasone (a long-acting glucocorticoid drug) produces the same response as cortisol (the endogenous ligand) (FOR cortisol deficiency).
- If an agonist produces the full effect of the endogenous ligand, the drug is called a full agonist with high efficacy.
Partial Agonists
*Turns people down.
- If only a part of the endogenous effect is elicited, the drug is called a partial agonist partial effect).
- Ex. Aripiprazole Blocks dopamine's ability to bind) produces a weaker biological effect at the dopamine receptor compared to dopamine (for people with schizophrenia).
*Efficacy will always be lower than a full agonist.
Dopamine Antagonist
- Turns people off.
- Decreases their ability to engage and enjoy the world around them.
Inverse Agonists
- Bind to the same receptor site as the endogenous ligand, but induce the opposite response.
- Only occurs when receptors have an intrinsic (basal) level of activity.
- Receptors exert a biological effect independent of the endogenous ligand "constitutive activity."
- Considered to have "negative efficacy."
GABAa Receptor - Inverse Agonists
- Agonists (such as the benzodiazepines) elicit a sedative effect.
- Inverse agonists (does opposite; receptor is binded to, but causes receptor to have less activity then on own) at this receptor exert anxiogenic effects.
- Activity all on its own, can be bonded to and still complete other activities.
*Inverse agonists = Helps us to not be anxious.
*Benzodiazepines = Good at treating anxiety; GABAa heightens responses and makes patient VERY calm.
Agonism Diagram
Antagonists
- Antagonists bind to the same receptor site as the endogenous ligand, but DO NOT stimulate the receptor.
- Rather, antagonists occupy the receptor preventing the endogenous ligand from binding.
Antagonists Types
Reversible (bind and let-go):
- Competitive.
- Non-competitive.
Irreversible (bind and never let go):
- Is not produced a lot.
Reversible Competitive Antagonists
- Antagonists compete for the same receptor binding site as the endogenous ligand.
- When the antagonist is bound the receptor binding site, it blocks the endogenous ligand from binding.
- A competitive antagonist always dissociates from the receptor.
Reversible Non-Competitive Antagonists
- Binds to a site other than the endogenous receptor binding site "allosteric modulation."
- Prevents the endogenous ligand from binding at the receptor binding site.
- Drug has bound to enzyme, enzyme binds to allosteric site, changing shape of the receptor.
- Ex. PCP (phenylcyclidine) and ketamine are non-competitive antagonist of the NMDA receptor.
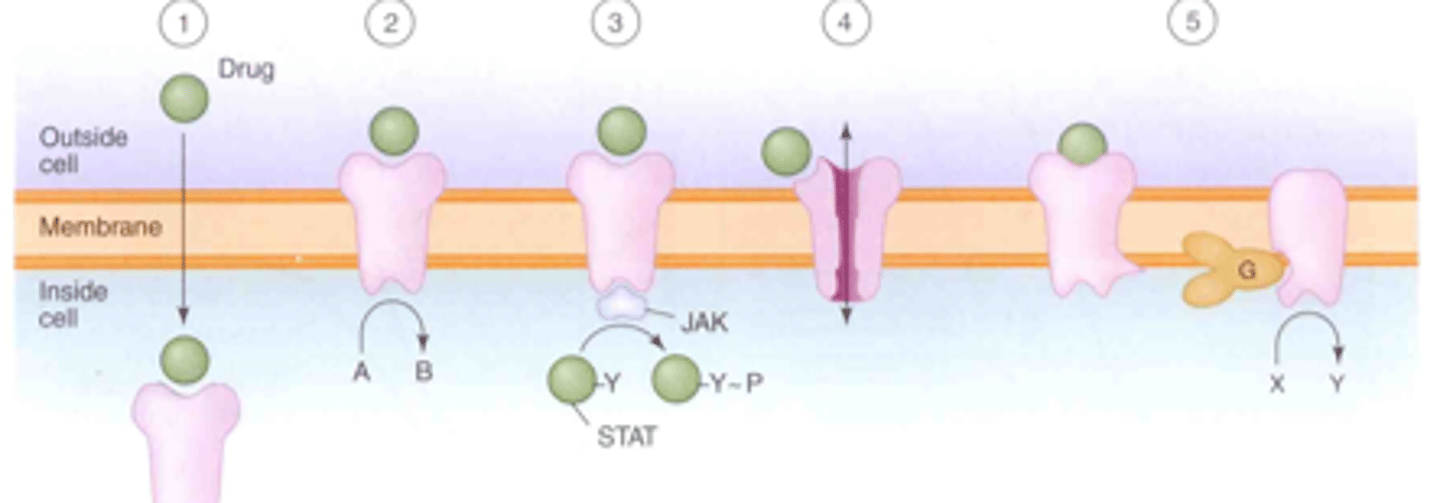
Signaling Mechanisms for Drug Effects
1. Intracellular receptors (molecules = drugs; have to be really small and fat-soluble).
2. Receptors located on membrane spanning enzymes (like tyrosine kinase) (ex. insulin receptor).
3. Receptors located on membrane spanning molecule that activates janus kinases (JAK).
4. Receptors located on membrane ion channels.
5. G-protein coupled receptors.
Signaling Mechanisms for Drug Effects Diagram
Irreversible Antagonists
- An antagonist that binds to the receptor binding site and does not dissociate from the receptor.
- k-1 is equal to zero; Kd is very low, and affinity is very high.
Some biological weapons are irreversible antagonists:
- Cholinesterase inhibitors (“nerve gases”).
Some irreversible antagonists are highly useful:
- Aspirin (analgesia, anti-inflammatory, antiplatelet).
- Omeprazole (gastroesophageal reflux disease; GERD).
G-Protein Coupled Receptors
- G-proteins stimulate effectors to produce intracellular changes.
- Receptors that interact with the G-proteins include those for some hormones, neurotransmitters, prostaglandins, etc.
A number of G-protein subgroups exist:
- Gs.
- Gi.
- Gq.
cAMP
- Cyclic AMP.
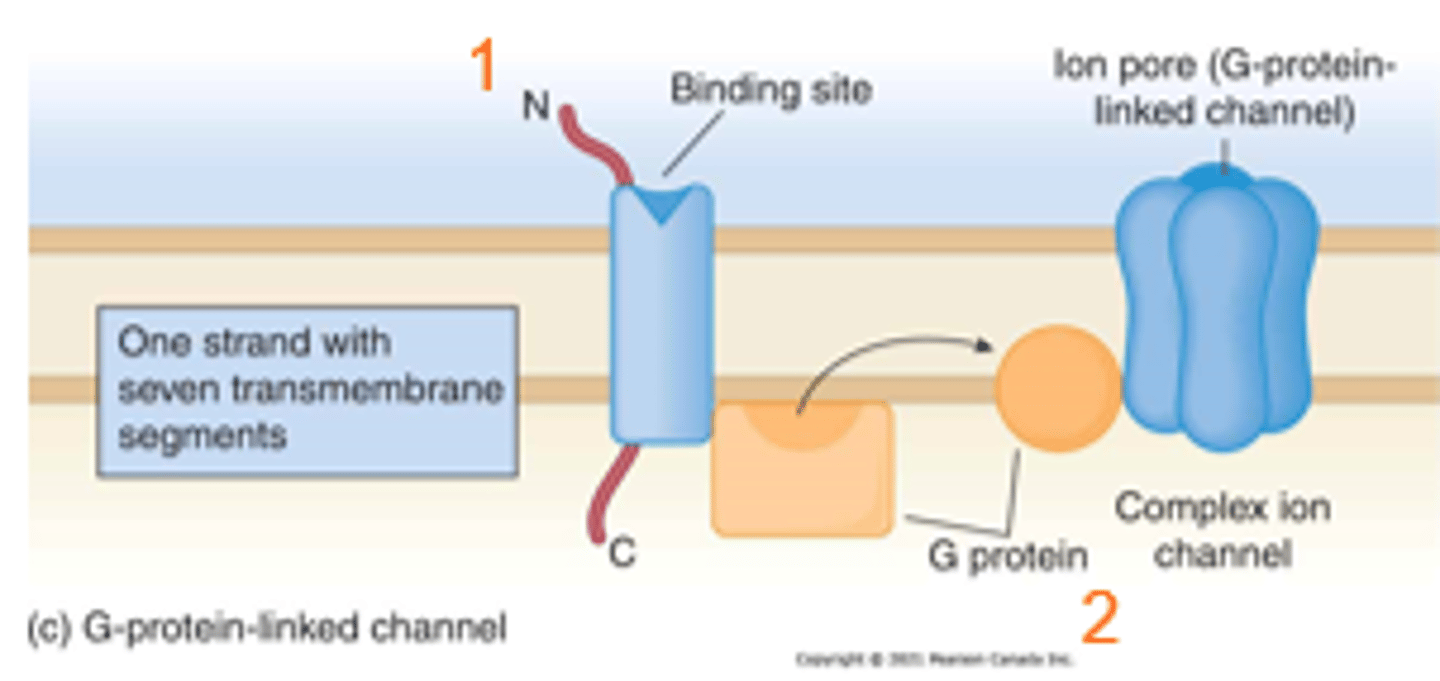
G-Protein Coupled Receptors & Effector's
- Binding of a ligand to its receptor causes the G-protein to stimulate an effector.
Effectors can be:
1. Ion channels (#1)
- Cardiac muscarinic receptor.
2. Adenylyl cyclase (for Gs + Gi proteins) (#2)
- This enzyme makes cAMP from ATP.
- cAMP is a 2nd messenger.
3.Phospholipase C (for Gq proteins) (PLC) (#2)
- PLC acts to cleave PIP.
- The cleaved PIP yields IP3 and DAG.
- IP3 and DAG are both 2nd messengers.
*#1: Through cAMP signal transduction pathway.
*#2: Through phosphatidylinositol signal transduction pathway.
Cardiac Atrial Muscarinic Receptor - G-Protein Linked Ion Channel
1. Ligand binding at a receptor site leads to stimulation of a G-protein.
2. G-protein stimulation induces opening of an ion channel.
- Coupled to a G-protein that is connected to a K+ channel.
- When acetylcholine binds to the muscarinic receptor, the associated G-protein is stimulated.
- The G-protein in turn activates the K+ channel to open.
- K+ leaves the cell, hyperpolarizing the cellular membrane and slowing heart rate.
Cardiac Atrial Muscarinic Receptor - G-Protein Linked Ion Channel Diagram
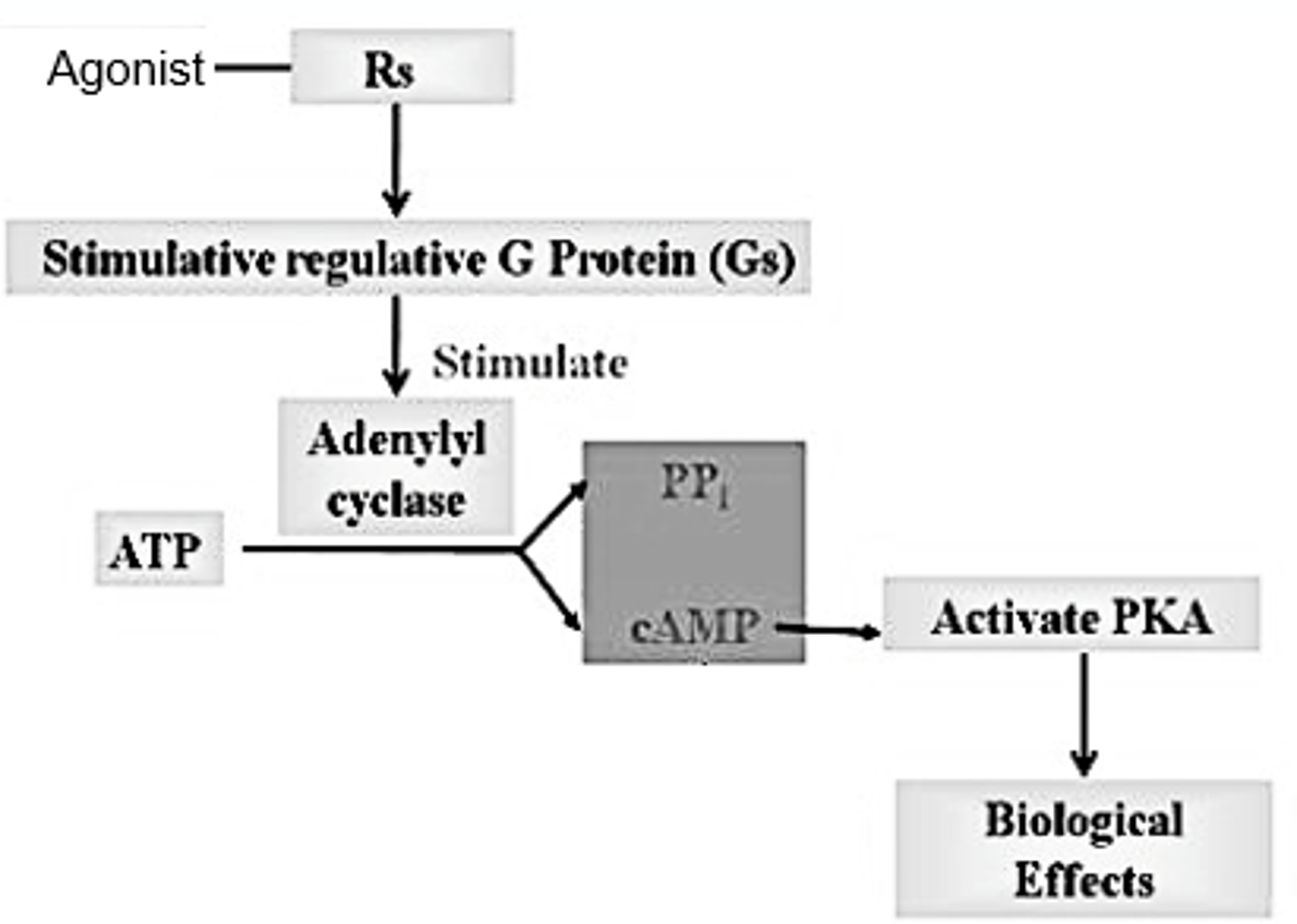
Gs Proteins - G-Proteins Linked to Adenylyl Cyclase
- Stimulator proteins*
- Stimulate adenylyl cyclase (the effector).
- Adenylyl cyclase converts ATP into cAMP.
- cAMP is a 2nd messenger that binds to, and activates protein kinases.
- Protein kinases activate enzymes by adding a phosphate group.
Gs-Proteins Linked to Adenylyl Cyclase
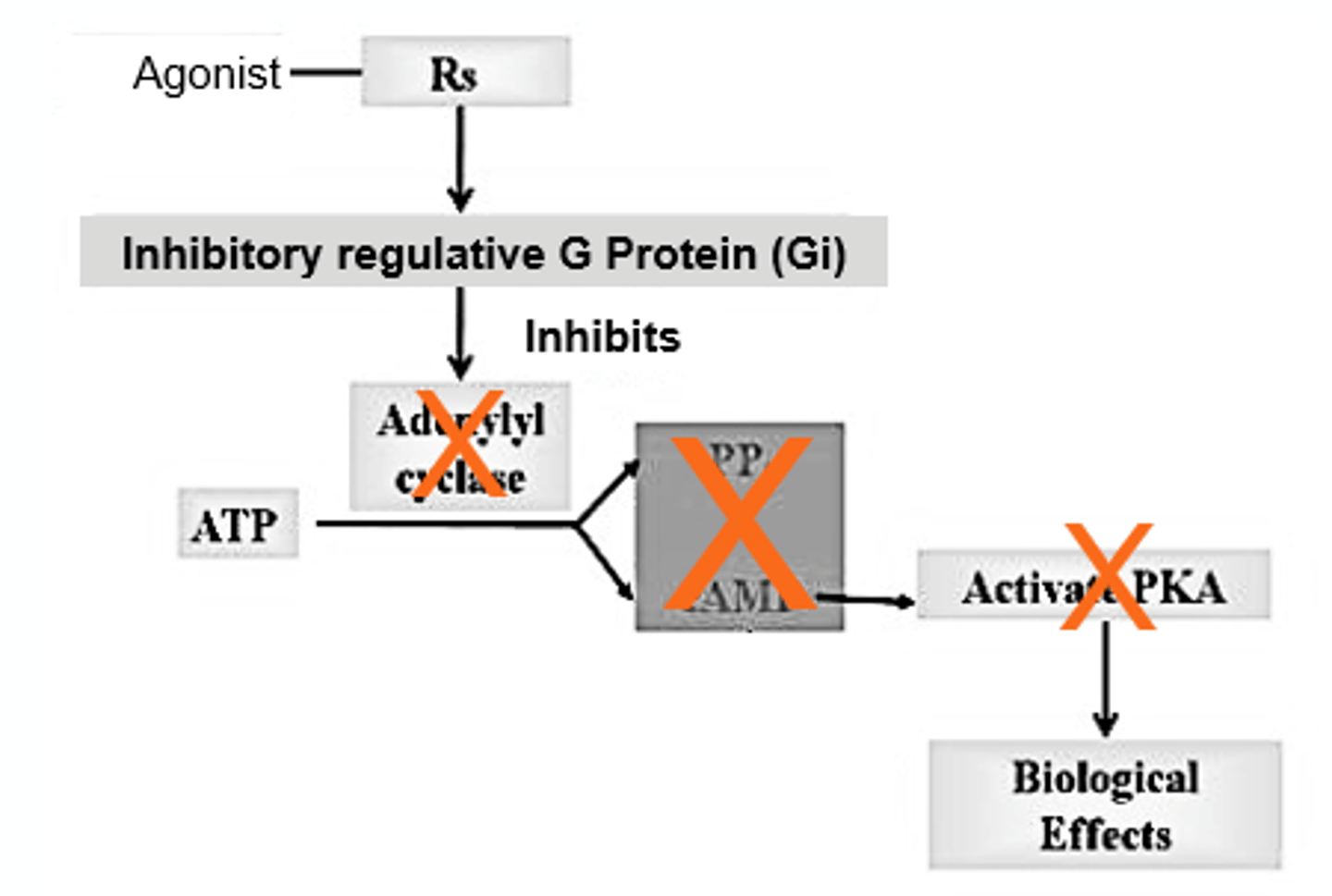
Gi-Proteins Linked to Adenylyl Cyclase
- Inhibitor proteins*
- Inhibits adenylyl cyclase (the effector).
- Activation of Gi leads to a decrease in cAMP since no new cAMP is made.
Gi-Proteins Linked to Adenylyl Cyclase Diagram
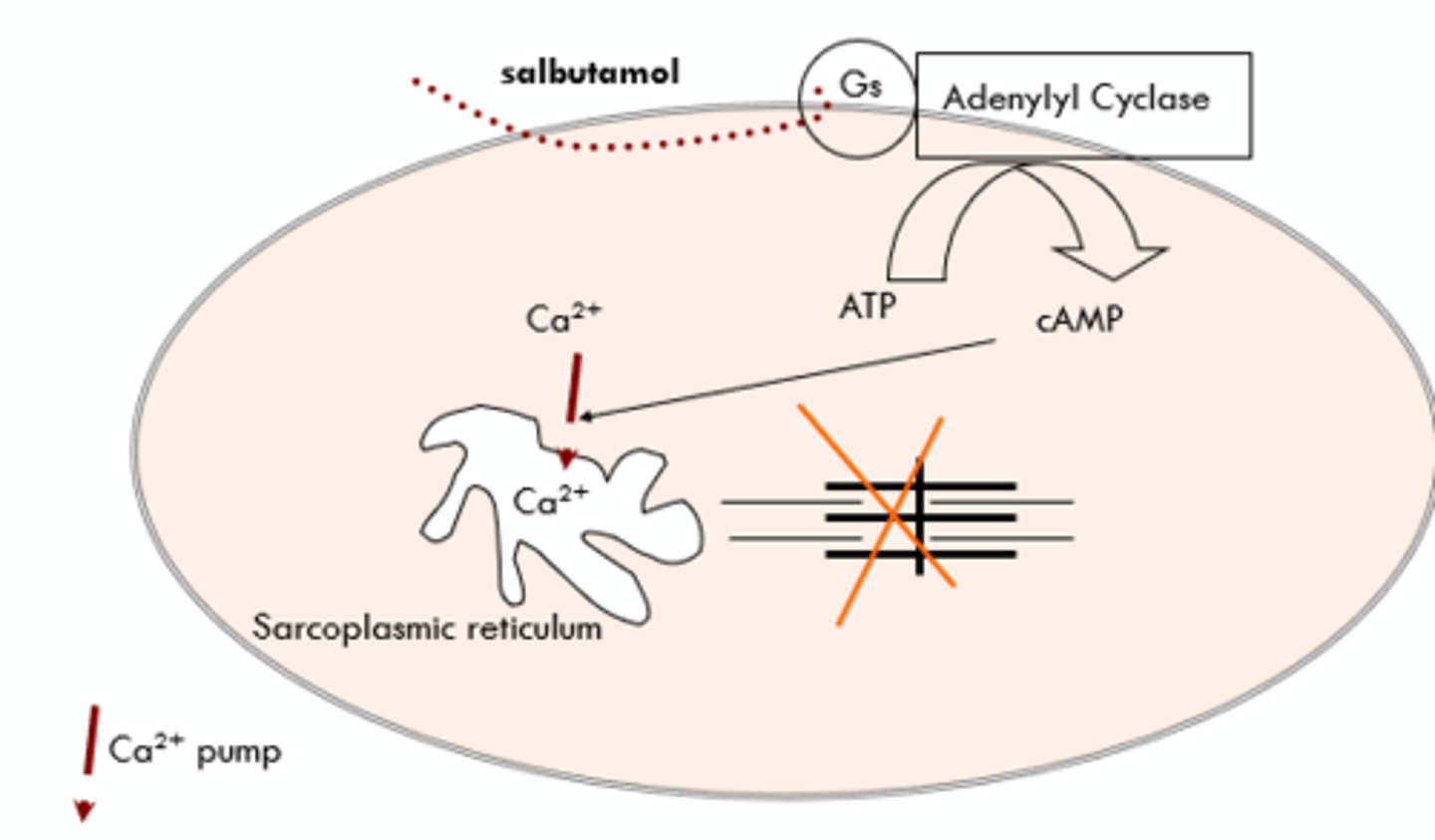
Albuterol/Salbutamol - Gs Linked to Adenylyl Cyclase
Albuterol/salbutamol (a bronchodilator) is a specific beta2-adrenergic receptor agonist:
- Binding to the receptor activates adenylyl cyclase via the Gs protein.
- Increase in cAMP causes the activation of enzymes that sequester Ca2+ and inactivate MLCK (myosin light chain kinase).
- Decreased levels of Ca2+ and MLCK leads to relaxation of the bronchial smooth muscle.
Salbutamol & the Beta2 Adrenoceptor
- Gs = Relaxation.
- Gi = Increase reaction.
- Gs + Gi work together.
- End: Relaxation of bronchi smooth muscle; decreases risk for asthma attack.
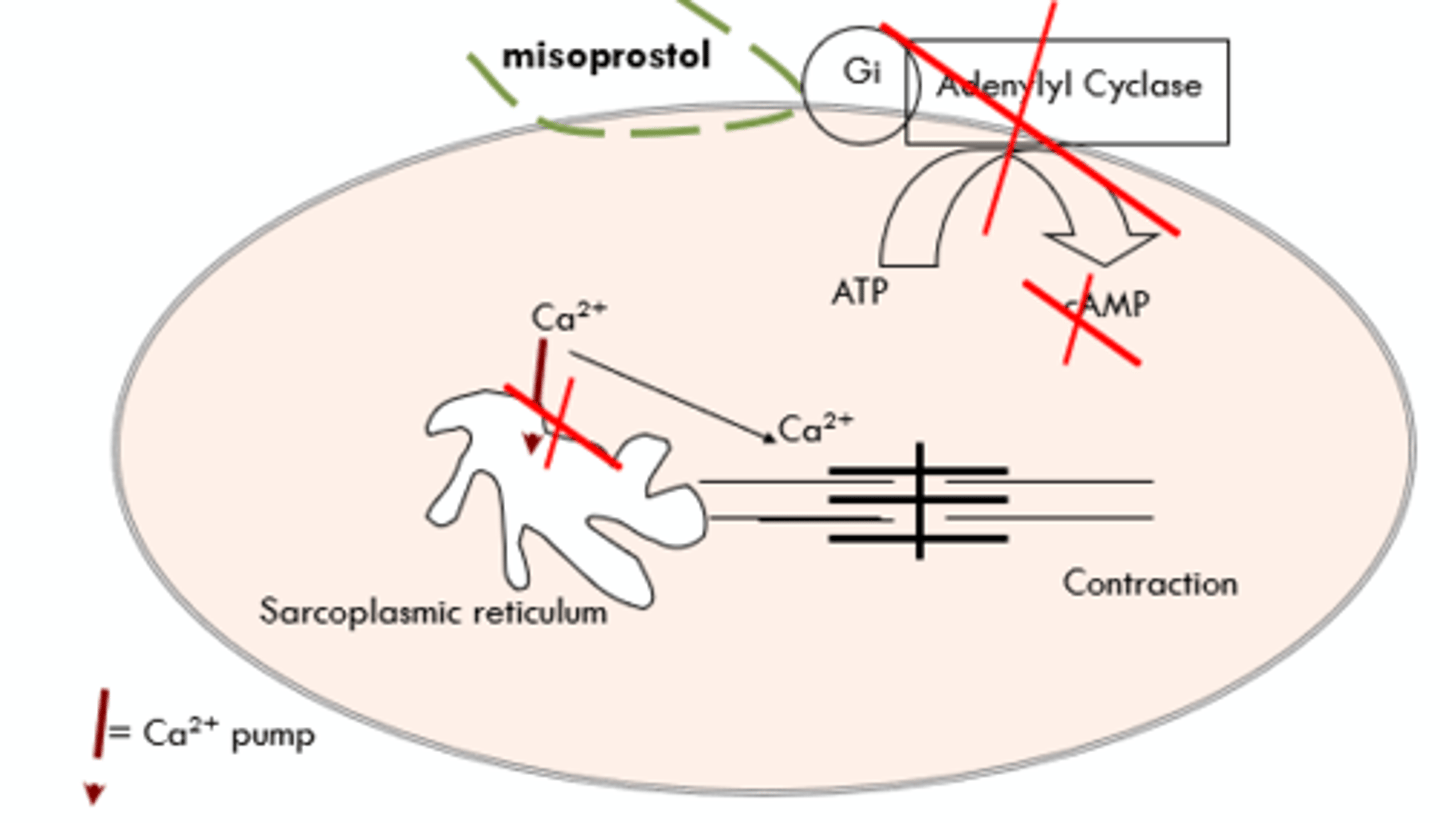
Misoprostol - Gi Linked to Adenylyl Cyclase
Misoprostol (a peptic ulcer drug) binds to the Gi-linked prostaglandin EP3 receptor:
- Receptor binding inhibits adenylyl cyclase.
- cAMP production decreases.
- Protein kinases are not activated by cAMP.
- Enzymes and pumps that help produce stomach acid are no longer activated.
- The production of stomach acid decreases.
- This drug also causes uterine contraction and is CONTRAINDICATED in pregnancy.
Misoprostol & the Uterine EP3 Receptor
*DO NOT GIVE DURING PREGNANCY
Gq Linked to Phospholipase C
Phospholipase C (PLC) is activated by Gq proteins:
- PLC acts to cleave PIP (phosphatidylinositol bisphosphate).
- The cleaved PIP yields 2nd messengers: Inositol trisphosphate (IP3); DAG (diacylglycerol).
- IP3 binds to the sarcoplasmic reticulum and stimulates the release of Ca2+ into the cytoplas.
- DAG binds to calcium channels on the cell membrane, facilitating the movement of extracellular calcium into the cell.
- Calcium influx into the cytoplasm (both pathways) produces the biological response.
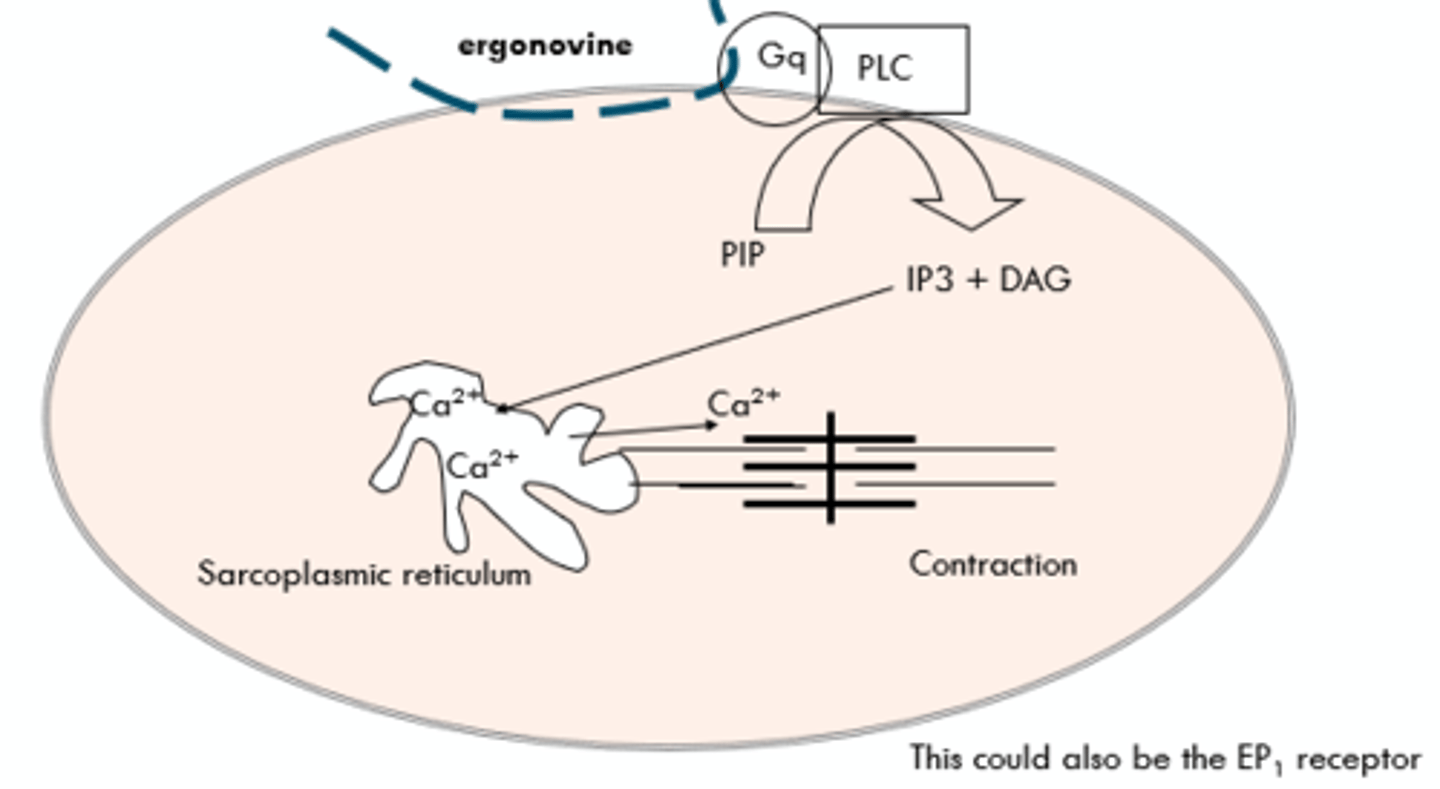
Ergonovine - Gq Linked to Phospholipase
Ergonovine binds to Gq-protein linked prostaglandin E1 receptors in the uterus and Gq-protein linked a1 adrenoceptors in the blood vessels:
- Receptor binding stimulates PLC to produce IP3 and DAG.
- IP3 binds to the sarcoplasmic reticulum and induces the release of Ca2+ into the cytoplasm.
- Induces contraction of the uterus and blood vessels.
- Can be used clinically to manage postpartum hemorrhage.
- Monitor patient for dangerous increases in blood pressure.
Ergonovine - Gq Linked to Phospholipase Diagram