Pharm 1
1/85
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
86 Terms
Zyrtec known as
serotine
Benadryl
diphenhydramine
Claritin
loratadine
hydroxyzine
the other gen 1
Allegra
fexofenadine
pharmkinetics
actions of the body on the drug
ADME
absorption:
distribution
metabolism/biotransformation
elimination/ excretion - without this step every medication would be toxic cause there is no way to leave. Majority is excreted through the kidneys
pharmdyanmics
the drug actions on the body
routes of administrations
oral: PO, has some most of the complicated pathways of absorption and there is differences all the times EX. if the medication is take with food or not. could make a different if a medication is affective or has side affects.
Can be enteric coated prevents stomach acid from dissolving.
extended-release coating that controls the drug release that allows slower absorption and prolonged duration of action and good for drugs with half short life (could take the drug multiple times a day but then adherence would go down) each bead as its own capsule for the coating- which means it can not be cut in half. After bariatric surgery modified coated drug does not work well.
Sublingual/ buccal- placement of drug in cheek and gum
Parenteral” introduces drug into systemic circulation
IV administration: does not need absorption because going into blood supply and is the most rapid
intramuscular
subcutaneous
intradermal- normally for diagnostic test ex TB
other routs
oral inhalation nasal prep
topical
transdermal
rectal- good for when patients always vomit
bb
look back to see what miss
barriers to drugs crossing cell membrane
lipophilic v hydrophilic- lipids drugs cross more easily
size ionization- large molecules may struggle to penetrate membrane-
pH difference affects the drug ionization, if the drug has a charge on it will have a hard time
+
absorption
drugs movement form site of administration into the blood
passive diffusion- goes with concentration gradient
facilitated diffusion
active transportation- needs proteins and energy
endocytosis - the cell engulfing the drug and used for very large molecules Ex. vit B 12
factors that influence absorption
dissolution rate (pH of drug and absorption site): increase dissolution means increase absorption
blood flow to the absorption site: increase perfusion means increase absorption
total SA
lipophilicity
expression of P-glycoprotein (pump things outside the cells so it kicks the drugs back out): increase P-glycoprotein means decrease absorption
how pH affects absorption example: drug A has pKa 7.8 at which site will absorption of drug be able to readily pass through the membrane: Mouth 7.0, stomach 2.5, duodenum 6.1, jejunum 8.0-
acids ionize in basic media while bases ionize in acidic media. When it is non ionized it absorbs the easiest.
IN pH gradients the acidic drugs accumulate on the alkaline side while that basic drug accumulate on the acidic side
Answer= the last one
Bioavilability
amount of active drug that reaches systemic absorption varies depending on the route of action (IV=100) other drugs it depends on the med meaning changes in doses based on the RoA
F - abbreviated to capital F
bioequivalence
when 2 products are equal in rate and extent to which active ingredients avliavble at site of drug testing exam brand v generic name of drugs
first pass metab
% of the drug that is metabolized by the liver before making it to the site of action- can further reduce the bioavailability
rectal first pass?
50% of drug absorbed will bypass the first pass system
Distribution
the transport of a drug at the site of absorption to various tissue in the body. Influenced by:
-CO
-blood flow
-capillary permeability
-lipophilicity
-volume of distribution
-binding to proteins
protein binding
albumin is the most prevalent protein in the plasma and the most important of the proteins to which it binds- when drug is bonded to albumin it is not having any effect on the body.
only unbounded (free) drug molecules ca leave the vascular system
protein bound molecules are too large to fit through the pores in the capillary wall
ex: pt with liver disease or kidney - has less albumin- important to keep in mind
crossing the BBB
can no be ionized or pilar
volume of distribution
theoretical concept that is the best way to gage how medication has moved around the body
amount of drug in the body over concentration in the blood
important for:
dosing decisions
where the drug is accumulation
how fast the drugs is being cleared
how concern you should be for toxicity
drug has a high molecular weight and bound to albumin, the drug will likely have a blank apparent volume of disruption
low- not able to get into body easily so dominator is larger because the drug is stuck in the blood stream
what are characteristics of a medication that remains in the bloodstream
large size
charges
plasma protein bound- more acidic compounds
ex: heparin anticoagulation that needs to work with clotting factors
metabolism
breakdown of a drug so it can be eliminated from the body
most drugs metab takes place in liver performed by cytochrome P450
substrate
the drug upon which an enzyme acts on
phase 1 metab
lipophilic drugs to hydrophilic polar substrates utilizes the p450 system, enzyme that breaks down drugs
enzyme induction
increase CYP 450 enzyme and decrease concentration of the drug which means you have to up the dose due to the decrease expected drug concentration
enzyme inhibition
results in decrease CYP 450 enzyme activity and increase concentration causing that there will be more of the drug taking the affect causing toxicity
drugs that have gone through phase 1
may go through phase 2 might not
drugs can jump to phase 2
phase 2= conjugation reactions happens when the metabolites are still lipophilic to be excreted so they do conjugation to make them polar and water soluble - sometimes the drug become inactive or active during phase 1
ex pro drugs are not active until phase one metabolism
usually after phase 2 the drug will become inactive
in liver disease which phase of drug breakdown is mostly affected
Phase 1 is more affect
so pt with liver disease needs medication that is breakdown mainly though phase 2
Drug A is metabolized by CYP3A4 while Drug B is an inducer what effect may occur, what actions should be considered
decrease concentration of drug A, increase the dose of Drug A
special consideration around metabolism
Age: infants do not have full metab capability until 1 year, older adults decrease ability
liver disease
drug tolerance
Excretion
kidney is the most important organ from drug excretion
others: biliary, fecal, breast milk, sweat, salvia, expiration
clearance= efficiency of drug removal decrease clearance (kidney disease) means decreased execration may need a lower dose to increase half life
renal excretion
GFR - only unbounded drug is filtered (drug enters with the blood and dependent on the GFR duh filtration step)
PCT: actively secreted into the tubules to increase drug loss
DCT: drugs can be reabsorbed back into systemic circulation. Happens for lipid soluble drugs, pH and ionization of drug can impact extent
how to determine pt renal function
creatine clearance used the CrCl equation to measure volume of blood plasma cleared per unit time
need the age, mass, sex, creatin serum levels
she will give you the equation on exam do not have to memorize this specific equation
normally 120 mL per min- but normal alternates
pt with renal disease needs drug x what would likely occur
increase affect because unable to filter and decrease the dosage - what
loading dose
large initial dose to achieve plateau more quickly
mechanical dose
rate of drug administration equal to rate of elimination at a steady state, smaller dose to maintain plateau
discontinuouation
94% of the drug is gone after 4 half lives
drug had half life of nine hours when will drug reach steady state
45 hours
takes 4-5 half life to achieves steady state
pharmacodynamics def again
what the drug does to the body
therapeutic affect + adverse effects
usually do not do novel activities- new interactions
drugs normally activate/ inhibit a pathway of something happening. Altering the pace.
Mechanism of action
effect happens when the drug (ligand) bind to the receptor
our body had endenous ligands
receptors are on or in a cell and when a drug binds an effect occurs
drugs act as signals
receptor family types
ligand gated ion channels: remain close until activated by agonist, once open there can be an exchange of ions (aka action potential)
G protein- coupled receptors =: extracellular ligand binding cause intracellular G protein interactions, cause further action within the cell by second massagers
enzyme linked receptors: extracellular receptor, when the ligand bind to receptor it changes the shape of the receptors that triggers intracellular cascade reaction
intracellular: primary targets are transcriptions factors that regulate gene expression inside the cell because they are lipid soluble and can enter the cell
when they do not like lipids ligands interact with receptors on the cell surface
onset of action is affect by
route of administration and drug dosage
think IV is quick
duration of action depends on
dosage
how it distributed
metab rate
execration rate
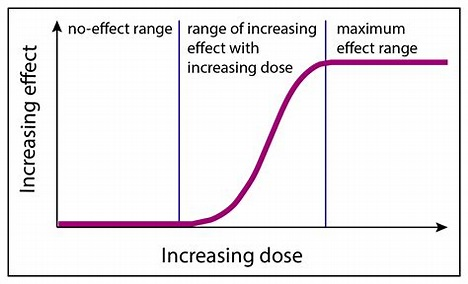
dose response relationship
how increase dose increase the effect
at a point (platue) no matter how much we increase dose no change in effect
flat
linear
platue
MEC min effective concentration
plasma drug level less than therapeutic effect will not occur
toxic concentration
no more therapeutic effect and can cause harm (platue phase)
therapeutic range
in-between the MEC and toxic concentration (linear part of the curve)
ED 50
dose at which 50% people who took it had theurputic response
LD50
50% who took this dose died
TI
the ration of a drug LD50 to ED 50 reflects a drugs safety, the larger the ration the difference between the therapeutic dose and lethal those means that larger T1 reflect greater safety
Narrow TI
need labs to monitor to make sure that the dose is affective and not at lethal range the periodic labels allow for opportunists for fine tunning the dose
simple occupancy th
intensity of the response is proportional to the numbers of receptors occupied
a max response will occur with all available receptors have been occupied - when all receptors are bonded that is the max result of the drug
modified occupancy th
the intensity of response is no proportional to number off receptors occupied influenced by drug-receptor interactions:
affinity: the strength of the attraction between drug and receptor
intrinsic activity: the ability of a drug to activate the receptor after binding
potency
comparing drugs
how much of the drug is required to get the desired result
efficacy
what is the maximal response this drug can produce think absolute value
greater efficacy> greater potency
beyond the max point the efficacy does not increase it will only increase adverse effects and toxicity
potency v. efficacy
Potency refers to the amount of drug needed to produce a specific effect.
Efficacy is the maximum effect a drug can achieve, regardless of dose.
ended on slide 27
biggest category for substances involved in human exposure
analgesics - over the counter and prescription medication mostly from people not using there medication correctly
what to looks for with a poison patient
puiple size size, RR(might have to manually retake, temp, skin, tremor, ankle, clonus
hemodialysis
can help speed up elimination if the toxin has low protein binding, small Vd, water soluble, small molecular weightur
urinary alkinalinization
pee more acidic
activated charcoal
best used within an hour of ingesting toxin, can cause some poison to absorb to the charcoal- very porous (high surface area) which is why it is so effective
important to test bowel sounds for obstruction because will worsen
only work on substances but not on heavy metals, alc, corrosive, iron, hydrocarbons inorganic minerals
activated charcoal can still have some benefit after the one hour window
gastric emptying
forceful vomiting must be one 1-3 hours not used as much because many toxins are more harmful on the way up
whole bowel irrigation
uses laxative medication - profound laxative effect meaning all content of GI tract will be evacuated do not use with absent bowel sounds, cardiovascular, renal, or electrolyte imbalance
simulates GIT motility
dermal decontamination
contaminated clothing should be completely removed and double bagged to prevent contamination others and for lab testing
skin should be thoroughly cleaned in general water in copious amounts is the decontaminant of choice for skin irrigation
mixing heavy metal chemicals and water not good cause metalic forms can be active
common pharm toxins
acetaminophen
opioids
benzo
organophosphate
methemoglobinemia
in the reading: methanol, isopropanol, cyanide, iron, lead- is material you are responsible for
acetaminophen
too much NAPQI normal byproduct of hepatotoxic metabolite glutathione in liver detoxify NAPQI but when too much liver unable to keep up
max dose= 4000mg/day
S: abdominal pain, jaundice
labs 4-24 post inject will determine need for N Acetylcysteine (antidote)
intreated can mean acute liver failure, common, death, encephalopathy- could take weeks
Rumack-Matthewnomogram to determine the next step
Review of action potential
resting state- cell is neg
trigger
sodium- makes the cell positive
potassium- potassium leaving the cell causing the cell to become neg
hyperpolarization: too much potassium leaves
opioid
cause hyperpolarization means that the neurons are not firing as much:
repressed RR
lower HR
reduce consciousness
constipation
pinpoint pupils
Narcan- naloxone opioid receptor antagonist - is pretty short acting so may need multiple administration may be needed - they are not going to feel well with antidote because they will feel withdraw symptoms
opioid the same receptor with a higher affinity means it kicks of the opioid that are currently on that receptor.
exitatory pathways
like Ach
stimulate ion movement= depolarization of post synaptic membrane
inhibitory pathways
GABA
BB
organophosphate posining
inhibits AchE the enzyme that breaks down Ach means there will be an overstimulation of acetylcholine
DUMBELLSS- cholinergic effects
medication- atropine is a muscarinic agnost?
acquired methemoglobinemia
oxidize hemoglobin means the hemoglobin can not bind and release oxygen well can be caused by a variority of chemicals and medication. Giving supplemental O2 will not help these patients they need methylene blue (dont have to know mech) know that can turn pt urine green or blue
anyone works on a farm what should you think
organophosphate poisoning
pinpoint pupils, tearing, bradycardia, excessive saliva and tears- choleric effects
you should give atropine
NAC
can be over the counter as well used for aceteophinophine regimen
main factors for individual drug response
drug factors- like the route
clinical factors
environmental
genetic
range means one person med work greats and in another they dead
liver disease
reduce albumin means more free drug which is more active drug
acid base imbalance
change in blood, urine ph affects if the drug is in the ionized or not ionized state so affects where it can be absorbed. An imbalance can cause the chemical to get stuck in a specific tissue.
genetic variant and genetic polymorphism
variant- changes to DNA sequence -both rare and common
polymorphisms- a variant that is common in the population - more than 1 %- example different blood type
can influence how drugs are metabolized
SNP single nucleotide polymorphism
one letter difference in the DNA sequence (most common variation in DNA) To be a SNP must be present in more than 1% of population
PGx variants
PGx variants are typically found in 3 main types of genes:
drug metab enzyme genes
drug transport releated genes
immune system genes- predisposed hypersensitivity to a drug
star represent a specific variant of the allele
start 1& no function
star 17 increased expression means they would be a rapid metabolizer