Adult III: Exam 2
1/204
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
205 Terms
When a client presents to the emergency department with pneumonia, which signs and symptoms would the nurse expect the client to exhibit?
Dyspnea
Fever
Fatigue
Orthopnea
What is the priority action by the nurse when a client experiences sudden respiratory distress?
Assess the airway
The client experiencing an anaphylactic reaction may experience what signs and symptoms?
Pruritus
Dyspnea
Bronchospasm
Laryngeal edema
What should you assess in the assessment of a patient’s circulatory status?
BP
HR
Intra-arterial pressure
PAP
PCWP—pulmonary capillary wedge pressure (PAOP—pulmonary artery occlusive pressure)
CVP (central venous pressure)
CO
CI
What is CO?
How is CO determined?
What is a normal CO?
CO is the amount of blood ejected by the L ventricle to the aorta in 1 minute
CO = HR x SV (stroke volume)
4-8L/min
What is the cardiac index (CI)?
What is a normal CI?
CI = CO/BSA (body surface area)
Normal CI: 2.5 - 4.2 L/min/M2
What affects stroke volume (SV)?
Preload
Afterload
Contractility
What is preload?
How is preload estimated?
What happens if preload is too low?
What about if preload is too high in the right ventricle?
What if preload is too high in the left ventricle?
Preload (Volume): The volume of blood in the ventricles at the end of diastole (filling pressure)
EDP (end diastolic pressure)—the blood returned to the heart at the end of diastole is used to estimate preload
Starling principle—when the ventricles are stretched to their max, we have maximum CO (like a rubber band stretched to its max snaps harder, the heart is the same); so if we do not have enough preload, we do not have the volume necessary to stretch the ventricles and achieve adequate CO (because SV x HR = CO, low preload decreases stroke volume, the amount of blood pumped per beat, which would lower CO)
So basically, reduced preload = reduced CO
If we have too much preload (too much end diastolic volume) in the RV, the pressure is too great (b/c more volume = more pressure), and blood backs up to the systemic vasculature = edema in the extremities
High preload in the left ventricle = higher volume of blood and pressure in the left ventricle = blood backs up to the lungs, causing pulmonary edema
What is normal central venous pressure (CVP)?
Normal: 2-6
For testing purposes: 4-8
What is central venous pressure (CVP)?
What is it used for?
What is the normal range?
CVP: Pressure created by the volume of blood in the right side of the heart at the end of diastole
Used to guide assessment of fluid balance and responsiveness to fluid administration
Normal range: 2-6 mm Hg
What is afterload?
Afterload: The resistance the left ventricle must overcome to eject blood into the vasculature (to push blood into the aorta to perfuse the body + to push blood into the pulmonic valve to the lungs)
What conditions increase preload?
Hypervolemia
Regurgitation of cardiac valves
Heart failure
What conditions increase afterload?
HTN
Vasoconstriction (because smaller vessels = higher pressure, so it takes more force from the heart to get blood through)
What does increased afterload cause?
Increased afterload = increased resistance the heart has to overcome to eject blood and perfuse the body
—>So increased afterload causes increased cardiac workload (the heart has to work harder to overcome the greater resistance to perfuse the body, so instead of lifting a 10 lb weight, imagine the heart trying to lift 100lbs)
What are the indicators of left ventricular afterload?
LV afterload = the resistance the left ventricle has to overcome to eject blood to the rest of the body (through the aorta)
Systemic vascular resistance (SVR) = the Resistance that the left ventricle must overcome to open the aortic valve and eject a volume of blood into the systemic circulation; generally, as SVR increases, CO falls
Mean arterial pressure (MAP): The average pressure in the systemic arteries over a cardiac cycle
What is the indicator of right ventricular afterload?
RV afterload = the resistance the right ventricle has to overcome to eject blood to the lungs through the pulmonic valve
Pulmonary vascular resistance
What are the effects of increased afterload?
Increased afterload results in:
Decreased stroke volume
Decreased CO
Increased oxygen demand (increased afterload = increased resistance, so the heart has to work harder to overcome greater resistance, so it uses up more O2—like when you exercise, using your muscles uses more O2)
What is contractility?
How does preload impact contractility?
What else can impact contractility?
Contractility: Strength of the contractions of the heart
If we do not have enough preload, we do not have optimal stretch = decreased CO and contractility
Contractility can be altered by meds (i.e., dobutamine, digoxin, ect.) and cardiomyopathies (floppy left ventricle)
A patient who weighs 50 kg and a patient who weighs 120 kg both have a cardiac output of 4 l/min. Both patients have equal cardiac function—true or false?
False
Cardiac Index is a more sensitive indicator of cardiac function than CO because it takes into account body surface area
The client who weighs 120 kg has decreased cardiac function compared with the client who is 50 kg (b/c to adequately perfuse a larger person, the heart would need to work harder, so 4 L/min might be sufficient for the 50kg person, but it is not for the 120kg person)
All of the following are examples of noninvasive hemodynamic monitoring except:
Jugular venous pressure
Lactate
Swan-Ganz
NIBP
Answer: Swan-Ganz Catheter—an invasive way of measuring hemodynamic status by actually inserting a catheter into the heart for hemodynamic monitoring
Jugular venous pressure: We measure this by looking (i.e., for jugular venous distention)
Lactate: We draw blood, not as invasive as a Swan-Ganz
NIBP—BP cuff
You have a patient whose central venous pressure (CVP) is 1, but they have crackles, tachypnea, and dyspnea. What does this indicate?
So why use hemodynamic monitoring?
Hemodynamic monitoring (i.e., like checking CVP), should be integrated with in-person clinical assessment to check for accuracy.
A CVP of 1 indicates that the patient does not have enough fluid volume, but your assessment of them indicates fluid overload
Assessment and hemodynamic values do not always match each other
So why use hemodynamic monitoring?
To identify trends (we do not use just one reading to determine our entire clinical plan, we use trends)
They provide immediate info to guide interventions (not decide, guide)
Aids in diagnosis, minimizing complications/dysfunction, treating disorders, and evaluating the effectiveness of prescribed therapies
What should be used in addition to hemodynamic monitoring to guide medical interventions?
The Clinical Assessment
Mentation
Urinary output
Capillary refill
Skin color, condition, temperature, ect.
What must be present for a rhythm to be normal sinus rhythm (NSR)?
—>The patient has PQRST
A p-wave is present and uniform (identical in shape) for every QRS (so every QRS is preceded by one normal P-wave)
The rhythm is regular
Every P-P interval (atrial rate) is normal (using calipers, p-wave to p-wave is the same length)
Every R-R interval (ventricular rate) is normal (using calipers, R-wave to R-wave is the same length)
The P-QRS relationship is normal (PR Interval is normal)—the P-P intervals are the same as the R-R intervals (this means that the atrial rates and ventricular rates are the same) = using calipers, each P-wave to R-wave is consistent in length, and measures between 0.12 and 0.20 seconds (so 3-5 of the smallest boxes on an EKG strip)
QRS Complex: Narrow and uniform, lasting less than 0.12 seconds (so less than 3 of the smallest boxes on an EKG strip)
HR: 60-100
Where should the transducer be in a hemodynamic monitoring system?
Transducers need to be leveled at phlebostatic access
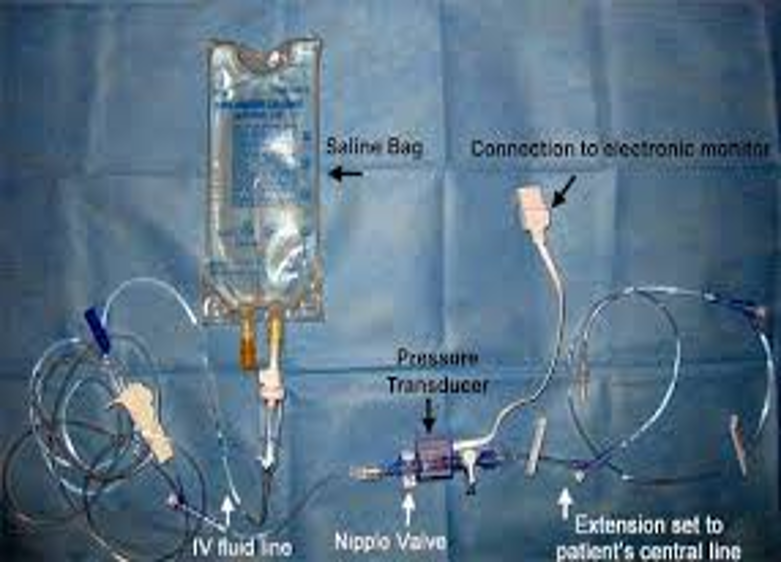
List the components of hemodynamic monitoring systems
Invasive catheter
High-pressure non-compliant tubing (need non-compliant tubing to avoid erroneous readings)
The transducer (and stopcocks) [transducers need to be leveled at phlebostatic access)
A pressurized flush system
Bedside monitoring system (cardiac monitor above the bed)
In a patient’s hemodynamic monitoring system, blood backs up into the tubing of the arterial blood pressure line. What should you do?
Make sure pressure is at 300 mmHg
Who is allowed to draw from the arterial pressure line of a hemodynamic monitoring system?
Respiratory therapy
Through which line in a hemodynamic monitoring system can the nurse give medications and fluids through?
Through the blue proximal lumen that goes into the right atrium—never put meds in the arterial BP line
Where does the distal lumen in a hemodynamic monitoring system sit, and what is it used for?
The distal line sits in the pulmonary artery
Used to measure pulmonary artery pressure (PAP) at any time
Used to get pulmonary capillary wedge pressure (PCWP) by inflating a balloon at the end
Never give meds through the distal line
Where is an arterial blood pressure line in a hemodynamic monitoring system usually inserted?
Through the radial artery, with a board in place to keep them from bending the line
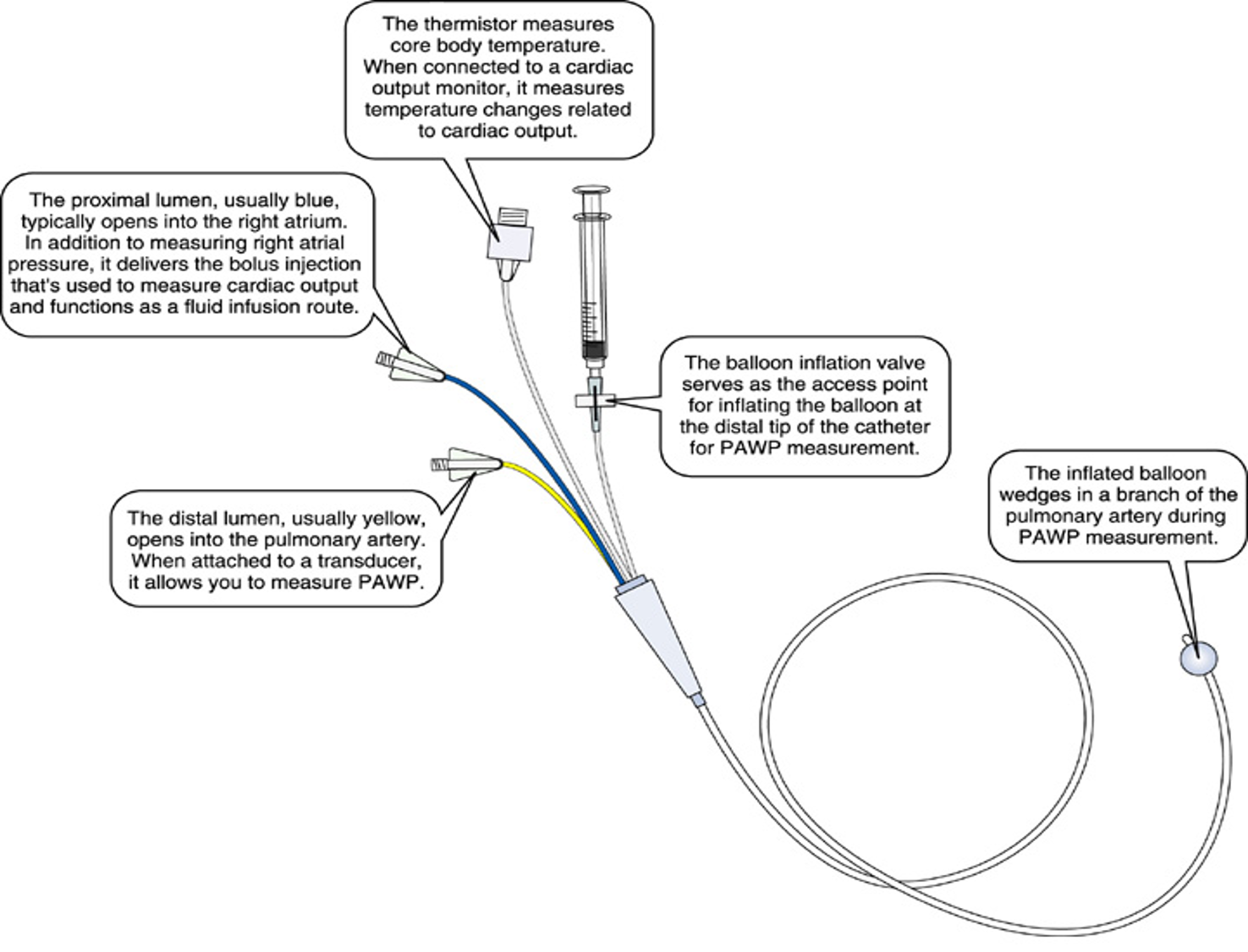
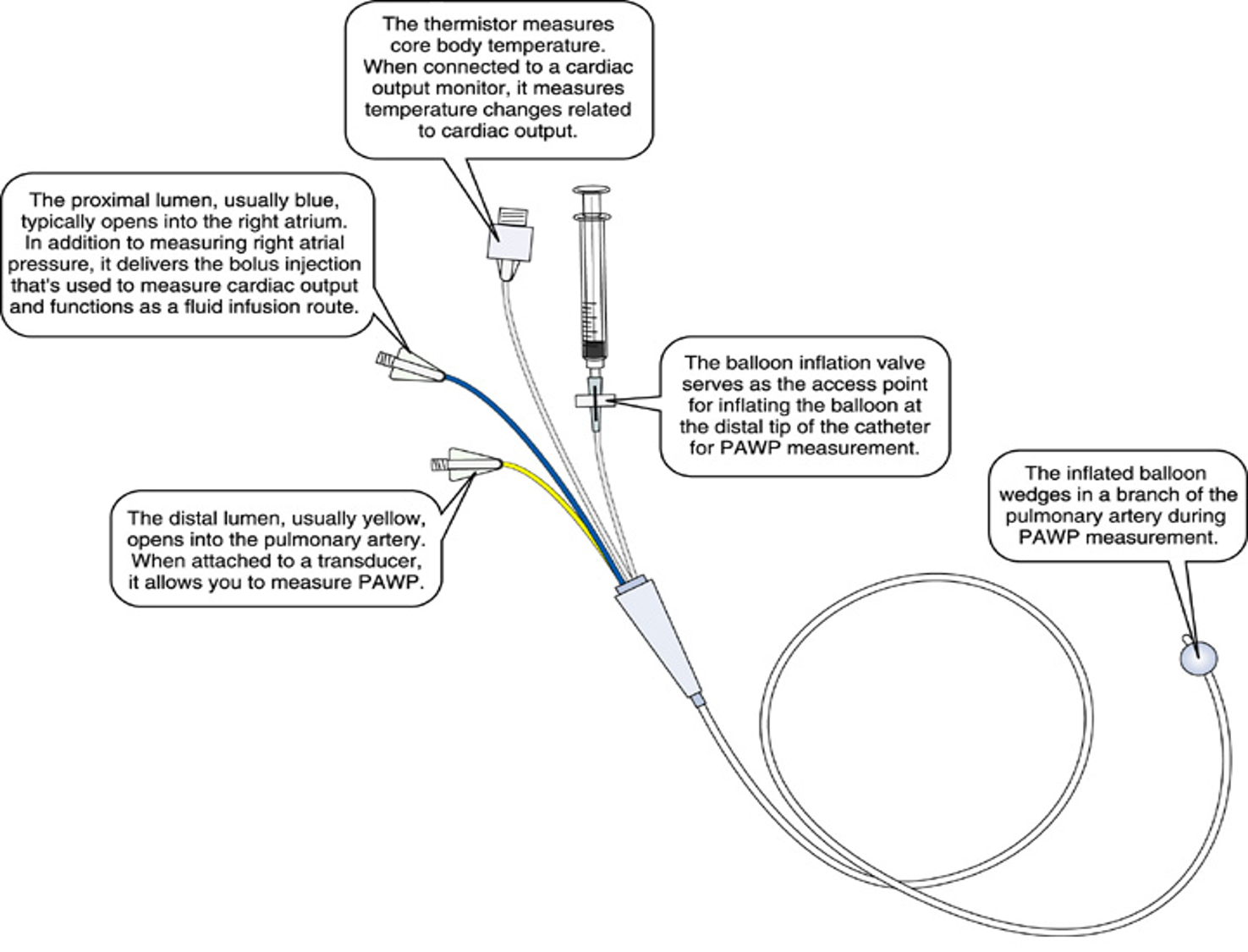
In a hemodynamic monitoring system, what is the thermistor used for?
Thermistor: Measures core body temperature
When connected to a cardiac output monitor, it measures temperature changes related to CO to estimate CO
What position should a patient be in for hemodynamic monitoring regarding accuracy?
Does not matter if the patient is supine or semi-fowlers regarding accuracy, you can place them in a position of comfort
Where should the transducer be when zeroed?
What does zeroing do?
What happens if the transducer is zeroed out below the phlebostatic access?
What happens if the transducer is zeroed out above the phlebostatic access?
When we zero the transducer, the transducer needs to be in line w/ the phlebostatic access at the 4th intercostal space
Zeroing eliminates the effect of atmospheric pressure, improving accuracy of results
Zeroed out below: Falsely high readings
Zeroed out above: Falsely low readings
What is the square wave test regarding hemodynamic monitoring?
Who is responsible for performing the square wave test?
What result on a square wave test is preferred? What is abnormal?
What causes abnormal square wave tests?
When do we perform the square wave test?
The square wave test is a bedside method used to verify the accuracy of invasive blood pressure monitoring systems, like arterial lines
The nurse is responsible for performing square wave tests
Optimally dampened is what we want (means pressures are where we want); overdampened and underdampened are abnormal results
Several things can cause—could be using compliant tubing instead of noncompliant tubing, air bubbles could be in the tube
What are the purposes of pulmonary artery pressure monitoring via Swan-Ganz or thermodilution PA catheters?
Monitor pressure in the right atrium, right ventricle, pulmonary artery, and distant branches of the pulmonary artery
Measure CO
Blood samples (cannot be used for ABGs b/c blood is mixed oxygenated and deoxygenated)
What is left atrial pressure related to?
Why is this important?
Left atrial pressure is closely related to left ventricular end diastolic pressure—the filling pressure of the left ventricle
We use left atrial pressure as an indicator of left ventricular function since it is not safe to float into the left ventricle
Where can a Swan-Ganz catheter be inserted?
Where is it placed after insertion?
What does this location/path allow the Swan-Ganz to do?
Inserted into the subclavian, jugular, or femoral vein
The catheter is floated through either the inferior or superior vena cava—through the R atrium—into the R ventricle—through the pulmonic valve into the pulmonic artery
Allows the catheter to get pressures in all of these different areas of the heart
What chamber has the lowest pressure in the heart, and why?
Right atrium b/c it has 2 holes in it (inferior and superior vena cava) and 1 valve (tricuspid valve) = lowest pressure chamber in the heart
Why and where is the balloon of a Swan-Ganz catheter inflated?
The balloon is inflated to no more than 1.5mL of air to get pulmonary capillary wedge pressure (PCWP, aka PAOP, aka pulmonary artery occlusive pressure, aka PAWP pulmonary artery wedge pressure)
When it is inflated, the balloon floats up into the pulmonary artery, blocking it to measure PCWP
How long can the the balloon of a Swan-Ganz catheter be inflated?
For no more than 5-10 sec
MAX = 10 SECONDS
How is infection prevented when using Swan-Ganz catheters?
Explain what is included in these.
Use central venous line/CLABSI bundle(central line-associated bloodstream infection) bundle to prevent infection
Central Line Bundle/CLABSI bundle
Strict handwashing
Strict sterile technique w/ maximal barrier precautions during placement
Chlorhexidine skin antisepsis—CHG used when line is inserted, when the site is cleaned at dressing changes, CHG baths q24h, CHG dressing
Optimal catheter site selection (decrease in CLABSI is associated with the use of the subclavian vein site, femoral site least preferred b/c of higher infection rates)
Daily review of line necessity (the longer they are in, the higher the risk of infection)
Minimizing the number of times the system is opened
Using sutureless securement devices
Changing the tubing system every 76-92 hours (3-4 days)
Aseptic treatment of tubing infusion ports (scrub hub b/f accessing lumens)
Aseptic treatment of medications and fluids given to the patient
For the proximal lumen of a Swan-Ganz catheter:
What does it look like?
Where is it located in the patient?
What is it used for?
Usually blue
Typically opens into the right atrium
Used to:
Measure right atrial pressure
Deliver bolus injections used to measure CO
Functions as a fluid infusion route
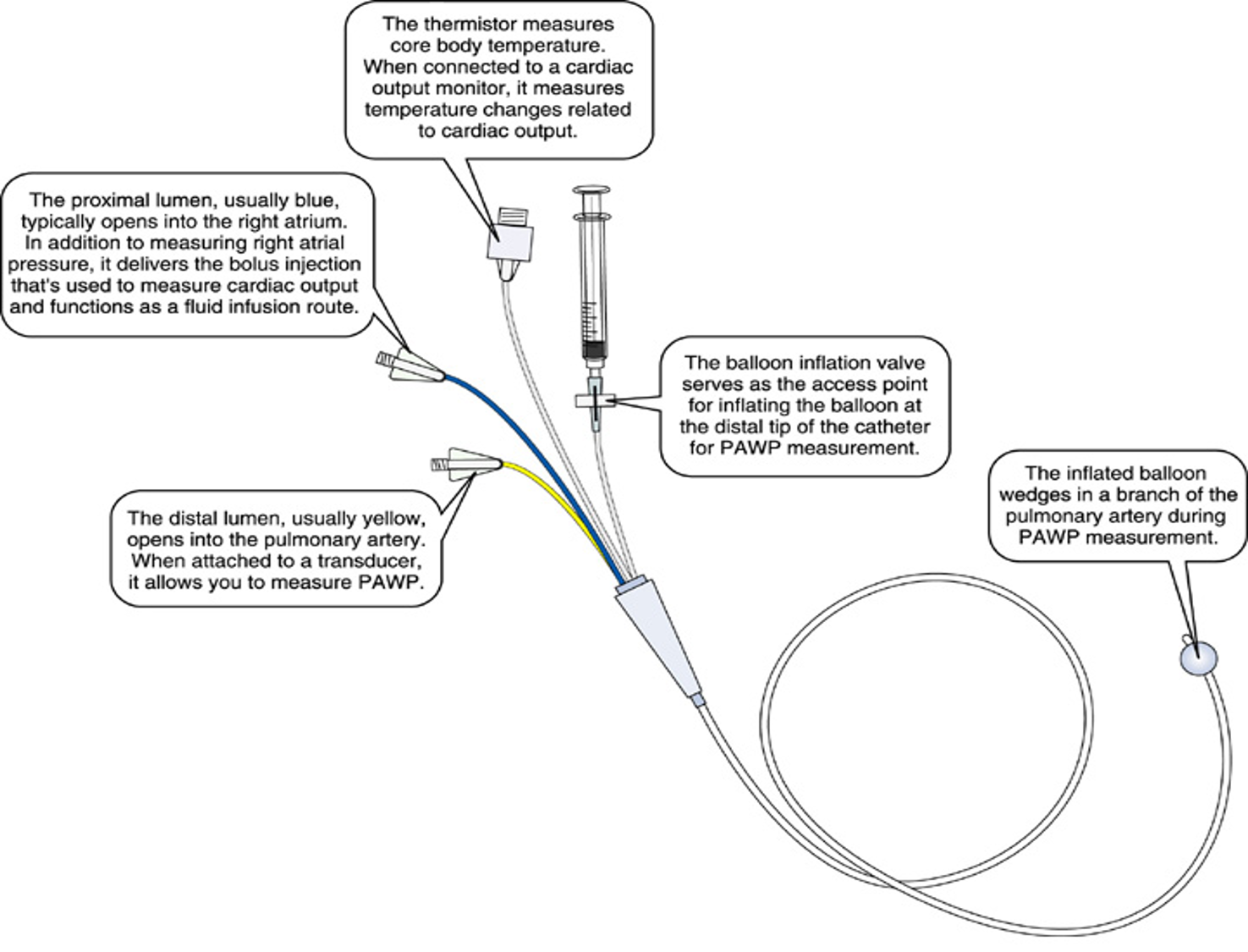
For the distal lumen of a Swan-Ganz catheter:
What does it look like?
Where is it located in the patient?
What is it used for?
Usually yellow
Opens into the pulmonary artery
When attached to a transducer, it allows the measurement of pulmonary artery wedge pressure (PAWP)
What is the nurses responsibility regarding the insertion of a Swan-Ganz catheter?
Physician inserts the line, nurses do not
Nursing Responsibilities During Insertion:
During insertion, the physician floats the catheter into the pulmonary artery, and the nurse monitors the waveform on the cardiac monitor, which correlates where the catheter is at in the heart
Wave form is taller in the right ventricle