Palliative care; Nutritional Support
1/28
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
29 Terms
Human digestive system
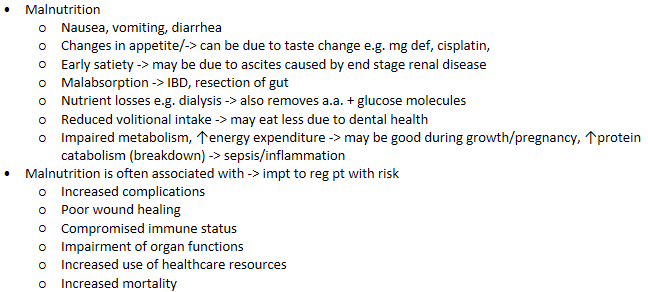
Effect of disease states on nutrition
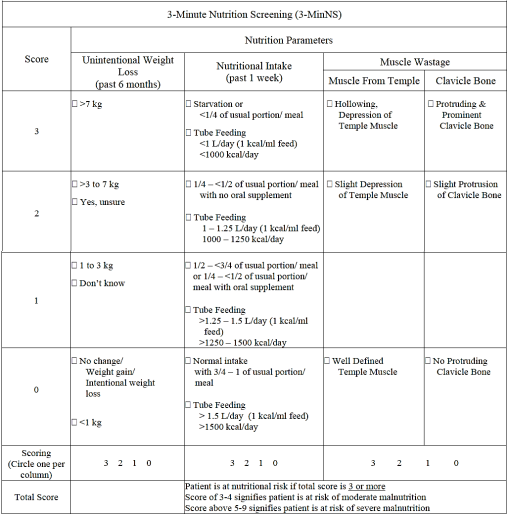
Nutritional screening and assessment
Nutritional screening
Usually done on admission to the wards
Can be done by ppl with no background in nutrition
To quickly identify individuals at nutrition risk
Refer to dietitian / nutritional specialist
Nutritional assessment
An in-depth, systematic process that integrates and interpret patient data to identify nutrition-related problems (ABCD)
e.g. Anthropometric measurements, Biochemical assessment (vit + min levels), Clinical assessment (clinical hist), Dietary assessment (has intake dropped in the past 3-6m)
Formulation of nutritional regime
Energy requirements
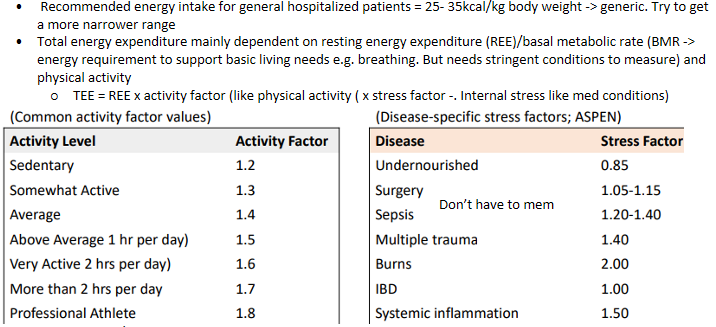
Energy requirements - Modes of REE/BMR measurement
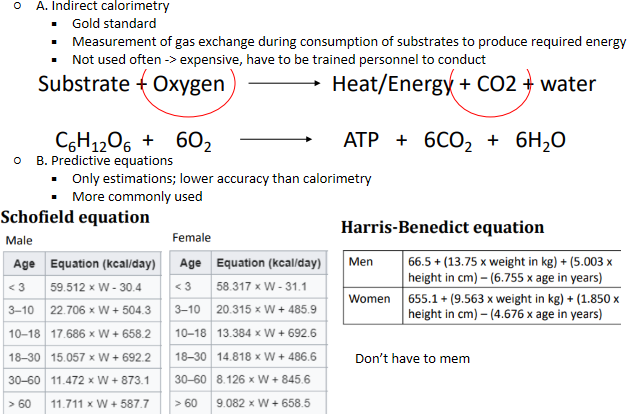
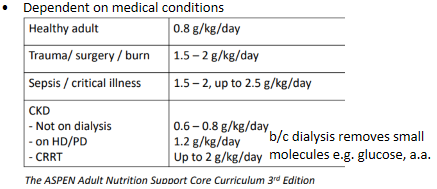
Protein requirements
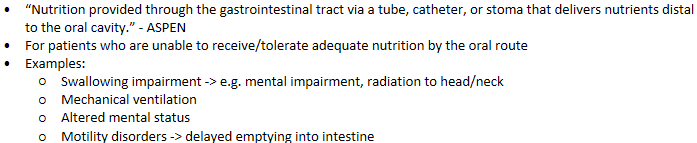
what is enteral nutrition
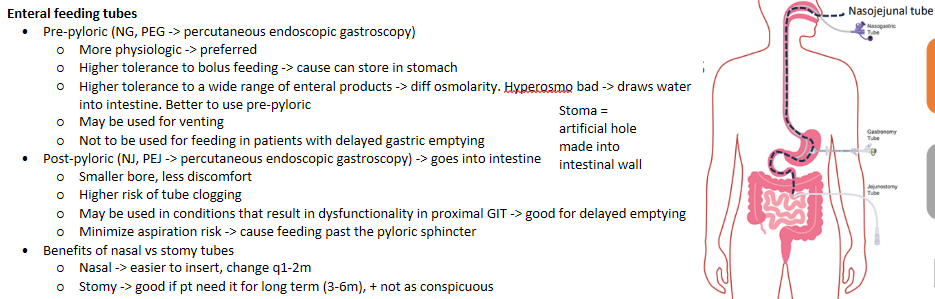
enteral nutrition - types of feeding tubes
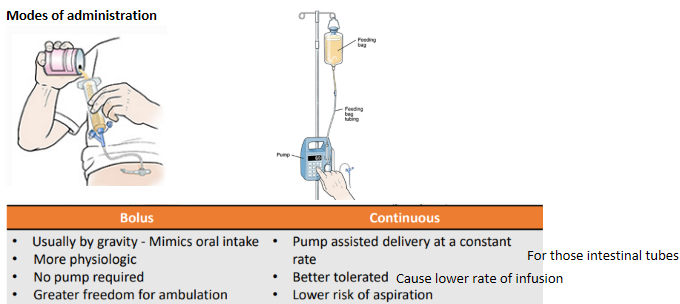
enteral nutrition - Modes of administration
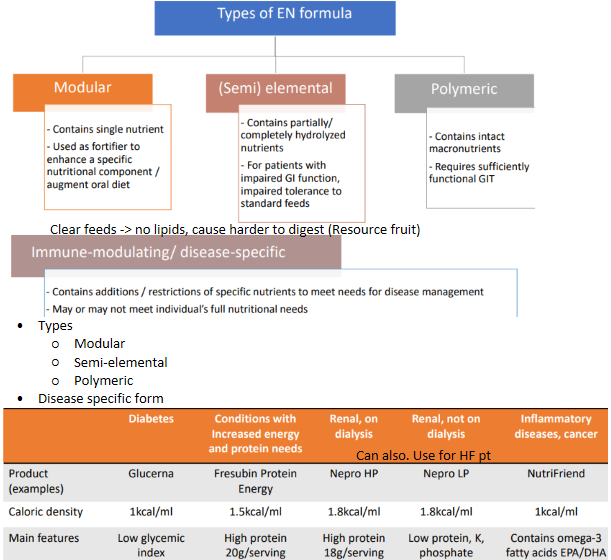
enteral nutrition - types of formula
enteral nutrition - Drug administration via feeding tube

enteral nutrition - Common complications
enteral nutrition - Monitoring parameters
Signs of intolerance (e.g. abdominal cramping, bloating, N/V/D)
Gastric residual volume -> intestinal aspiration of gastric contents 30-60min after feeding. To see how much feed is flowing into the intestine
Electrolytes
Fluid balance
Weight
enteral nutrition - Strategies to maximize tolerance to EN
Continuous instead of bolus
Use of prokinetic agents (e.g. metoclopramide, domperidone, IV erythromycin)
Post-pyloric feeding if intolerant to gastric feeding
Use of isotonic formula -> the higher the calorie the higher the osmolarity
Semi-elemental/elemental feeds for patients with malabsorptive issue (e.g. short bowel syndrome)
enteral nutrition - Make use of the physiological function of the GIT
Maintain functional integrity of the gut
Undergo first-pass metabolism -> helps to neutralize toxins in feed, promote efficient nutrient utilization (converts nutrient to active form)
Maintains normal gallbladder function -> production of cholecystokinin
Maintain gut-associated and mucosal-associated lymphoid tissues
Less complications than parenteral nutrition
Less expensive
what is parenteral nutrition

parenteral nutrition - types of access devices
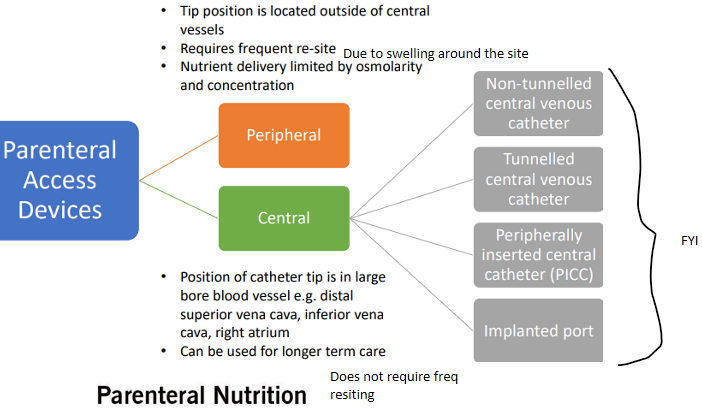
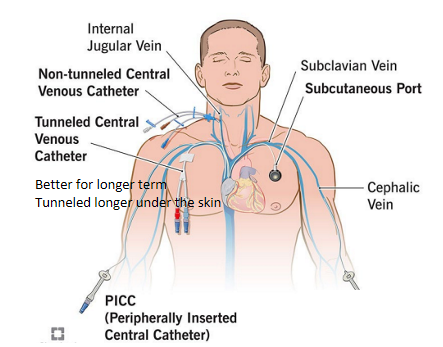
parenteral nutrition - types of catheters
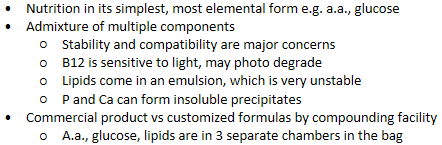
parenteral nutrition - composition
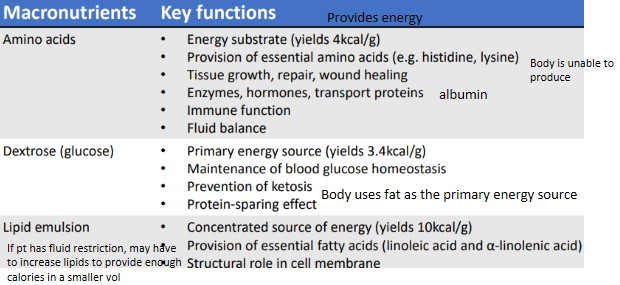
parenteral nutrition - macronutrients
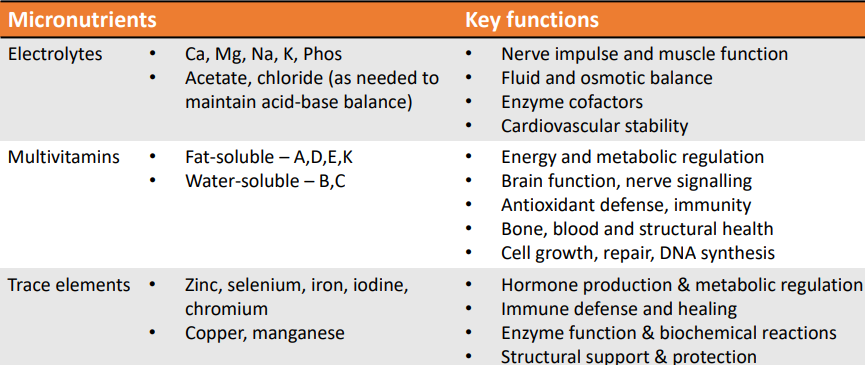
parenteral nutrition - micronutrients
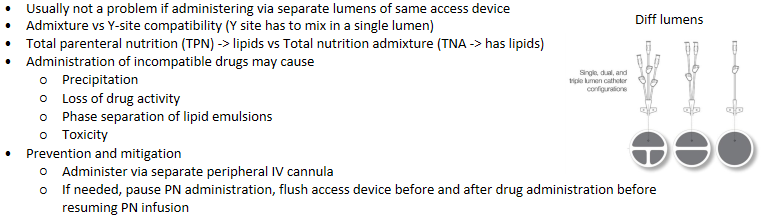
parenteral nutrition - Drug-nutrient interaction
parenteral nutrition - Device related complications
Occlusion in IV catheter -> body recognizes it as a foreign body
Thrombosis / clotting
Inappropriate flushing techniques -> push pull technique to create turbulence to flush out clots
Precipitates as a result of drug incompatibilities, crystallization
Lipid residues
Mal-positioning -> pt may accidentally touch and cause the line to move
Catheter-related bloodstream infection (CRBSI) -> cause may be contaminated + its nutrients for bacteria
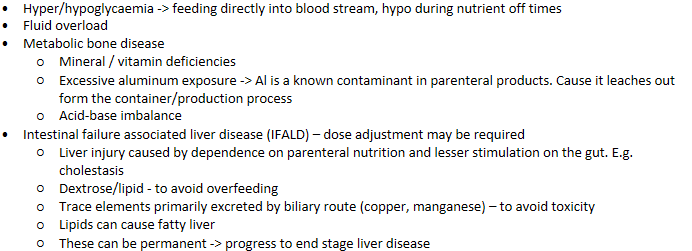
parenteral nutrition - Metabolic complications
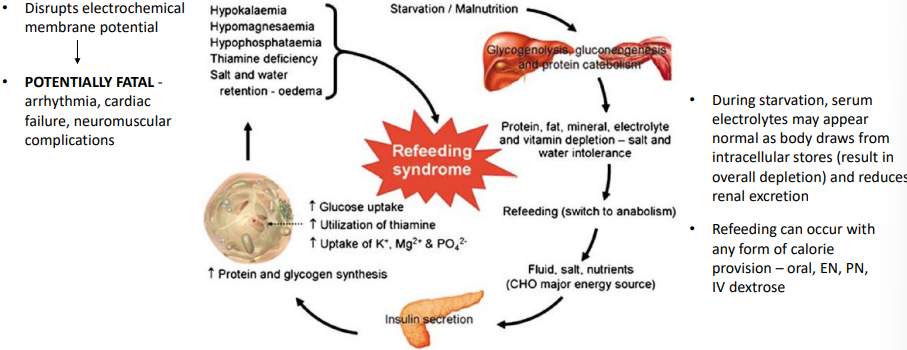
refeeding syndrome - pathophysiology
Starvation → low insulin, body uses fat/protein → total body depletion of electrolytes
Refeeding (↑ carbs during feed time) → ↑ insulin → shift of electrolytes into cells
Result: rapid ↓ in serum:
Phosphate (most important)
Potassium
Magnesium
Also: sodium/water retention → fluid overload
refeeding syndrome - Management strategies
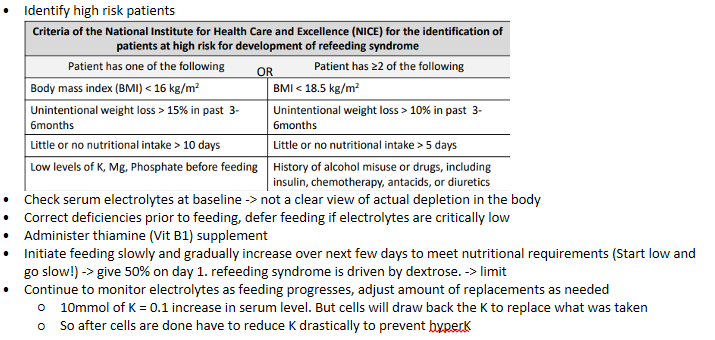
refeeding syndrome - Monitoring parameters
Electrolytes
Blood glucose level
Fluid balance
Weight
Renal function tests - creatinine, blood urea nitrogen, Chloride/CO2
Liver function tests
Triglycerides
Signs of infection e.g. differential blood count, fever, redness/pus around site of line access
Ethical considerations to artificial nutrition
Key dilemma in provision of artificial nutrition and hydration in patients nearing end-of-life, advanced dementia
Artificial nutrition = oral nutritional supplements, EN, PN
Deemed as medical interventions/clinical therapy, not just “foods”
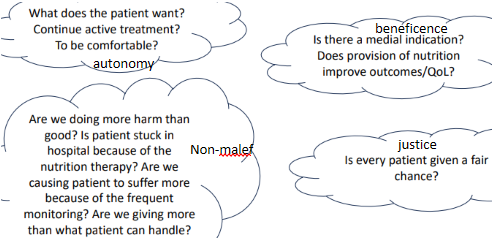
Aims of palliative/EOL care: to provide relief and support, manage physical symptoms, address psychological needs
Guiding principles: autonomy, beneficence, non-maleficence, justice
Summary