Burns
1/45
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
46 Terms
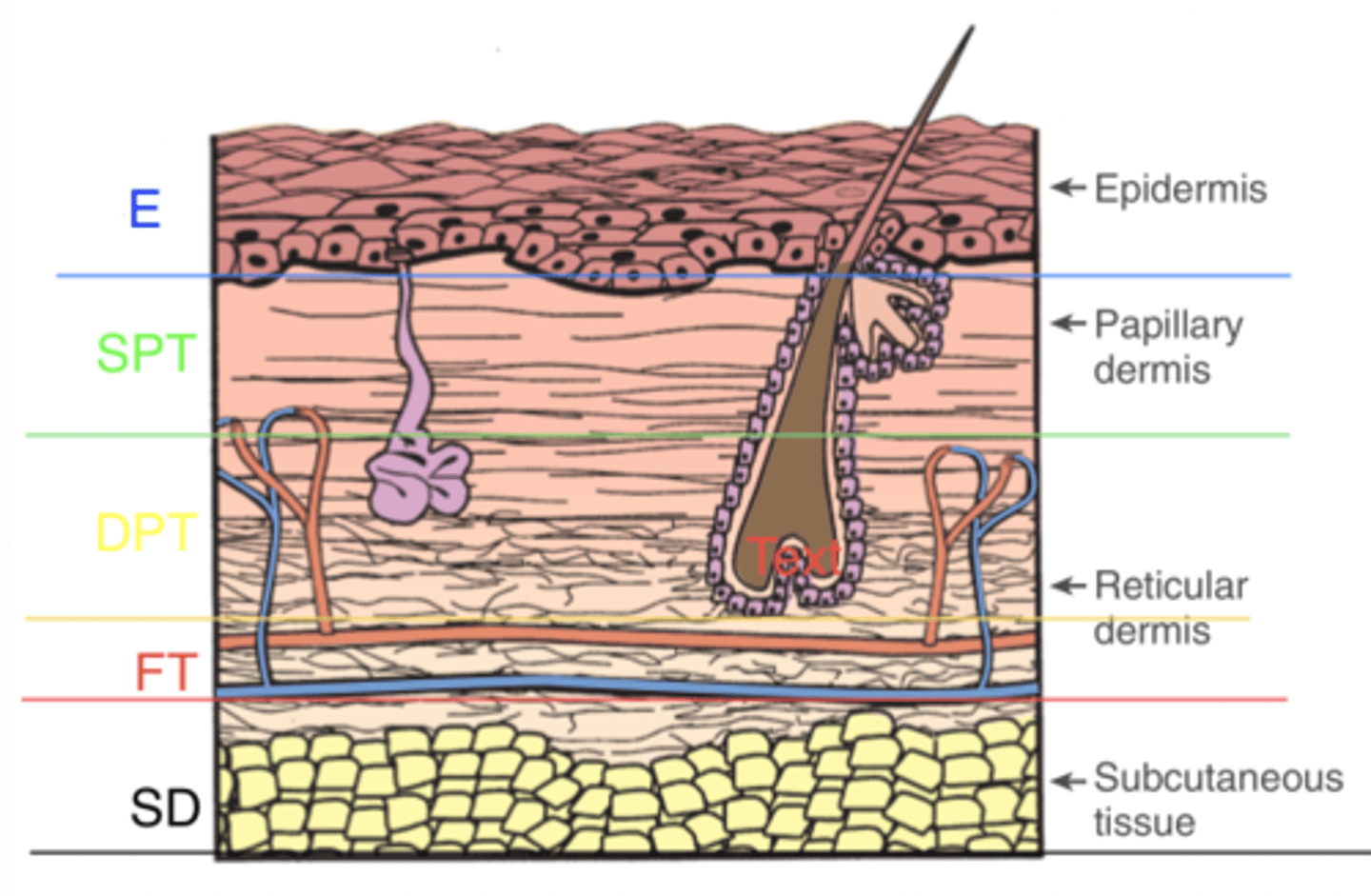
Epidermal burn (1st degree) presentation
Pink or red skin, no blisters, delayed tenderness
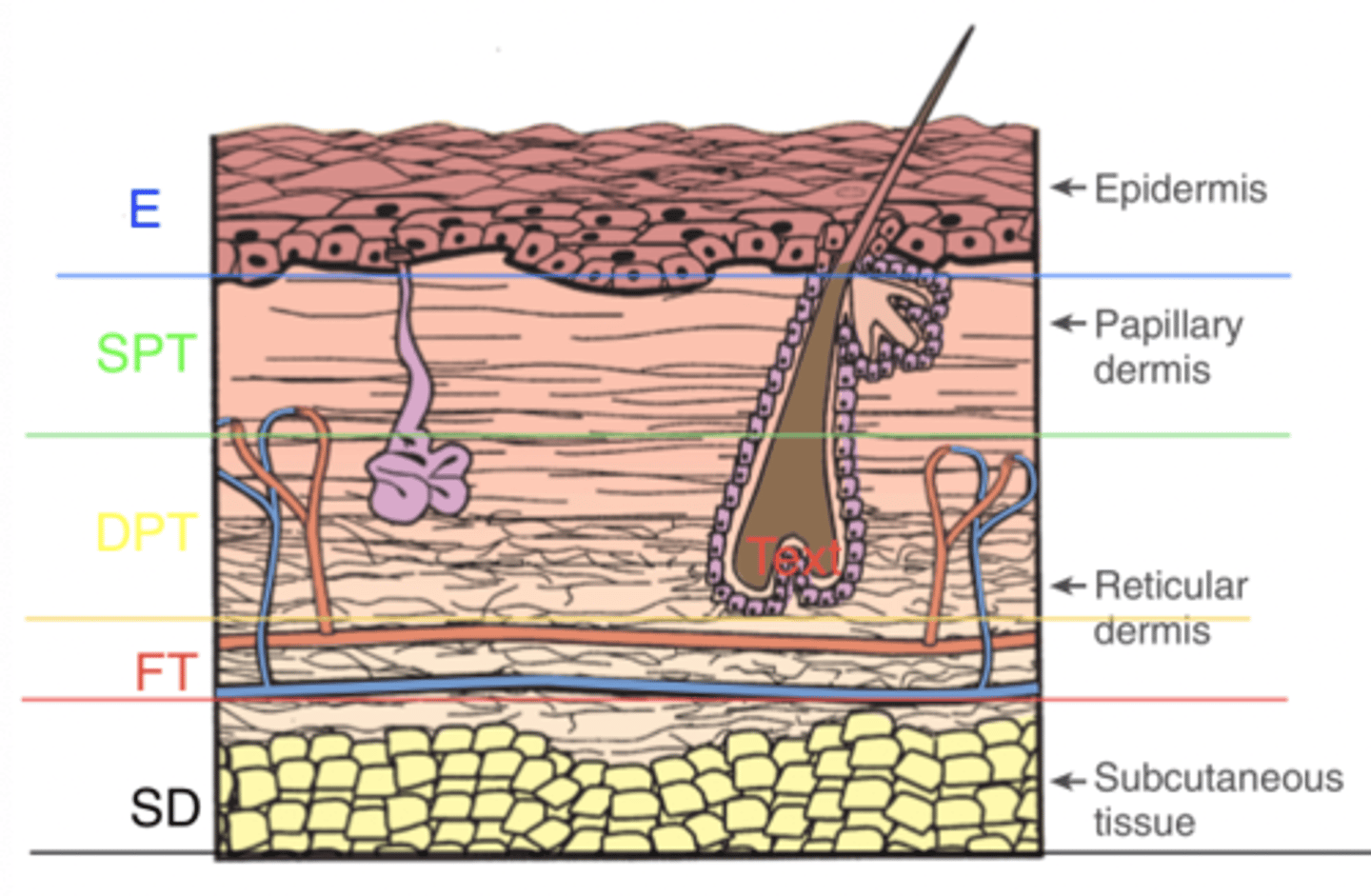
Superficial partial-thickness burn (2nd degree) presentation
Bright pink or red, blanching with brisk refill, intact blisters, very painful
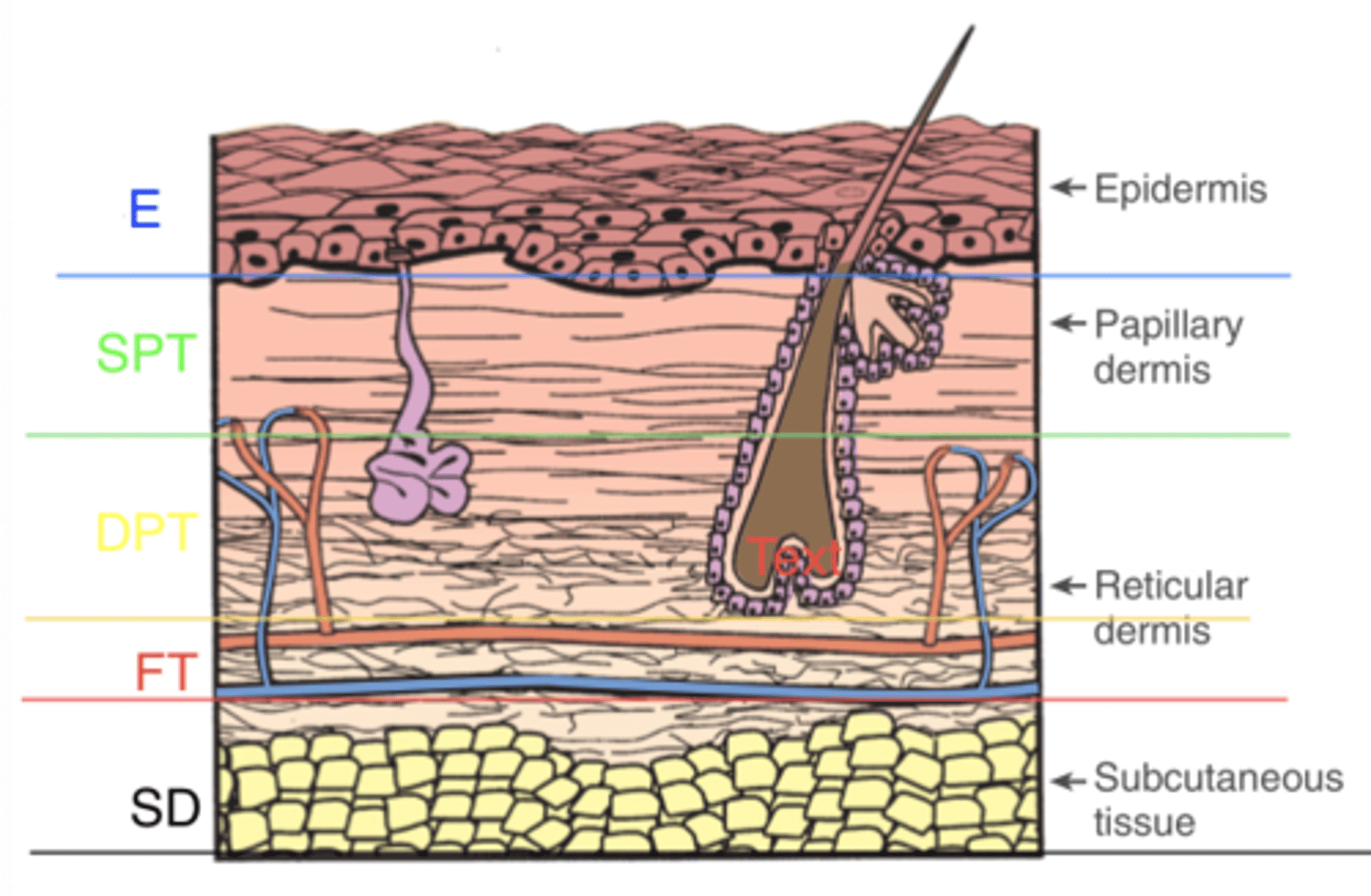
Deep partial thickness burn (2nd degree) presentation
Mixed red and waxy white, blanching with slow refill, broken blisters, wet surface, insensitive to light touch
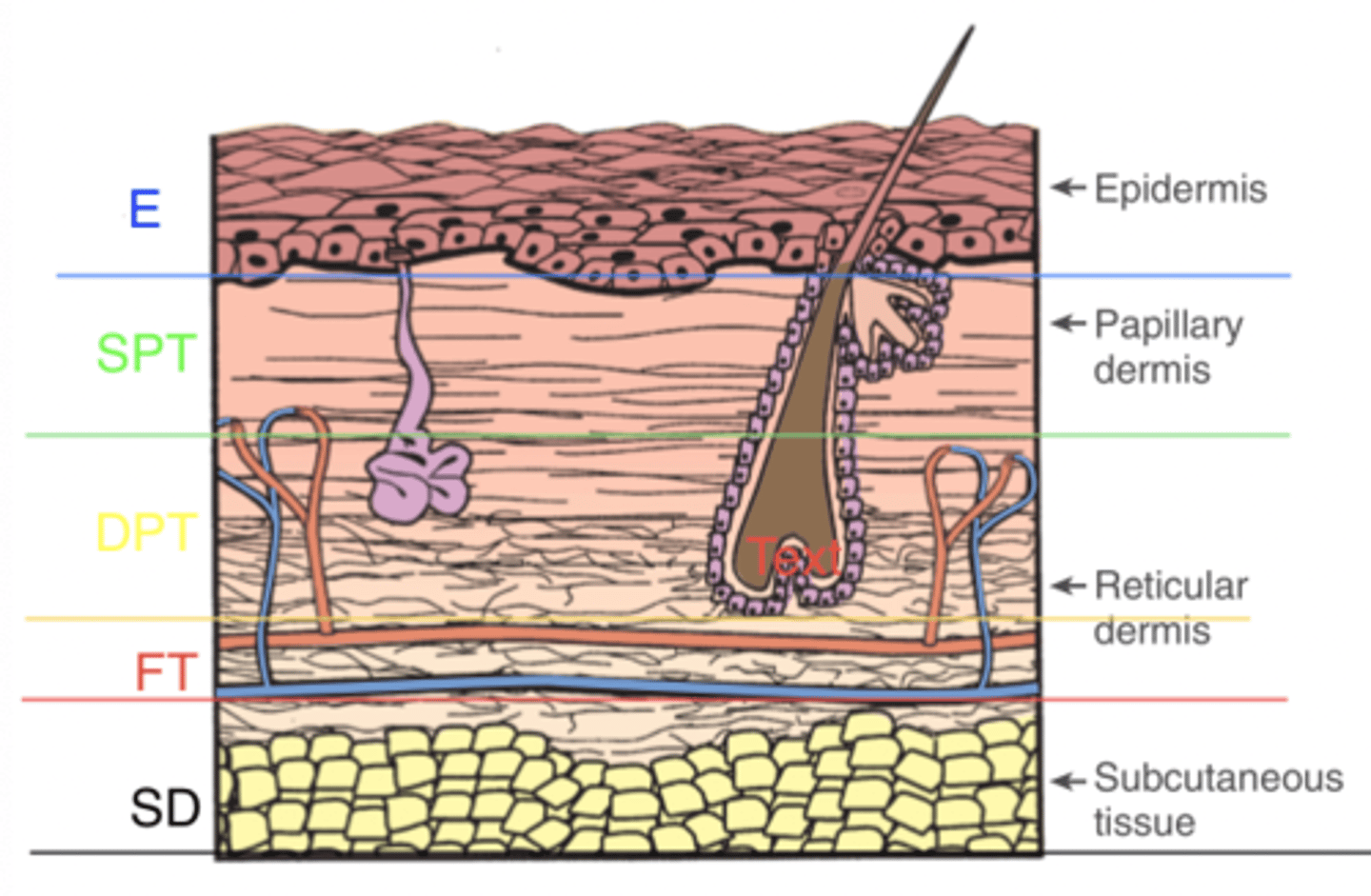
Full thickness burn (3rd degree) presentation
White, tan, black, no blanching, thromboses vessels, leathery, hair pulls out easily
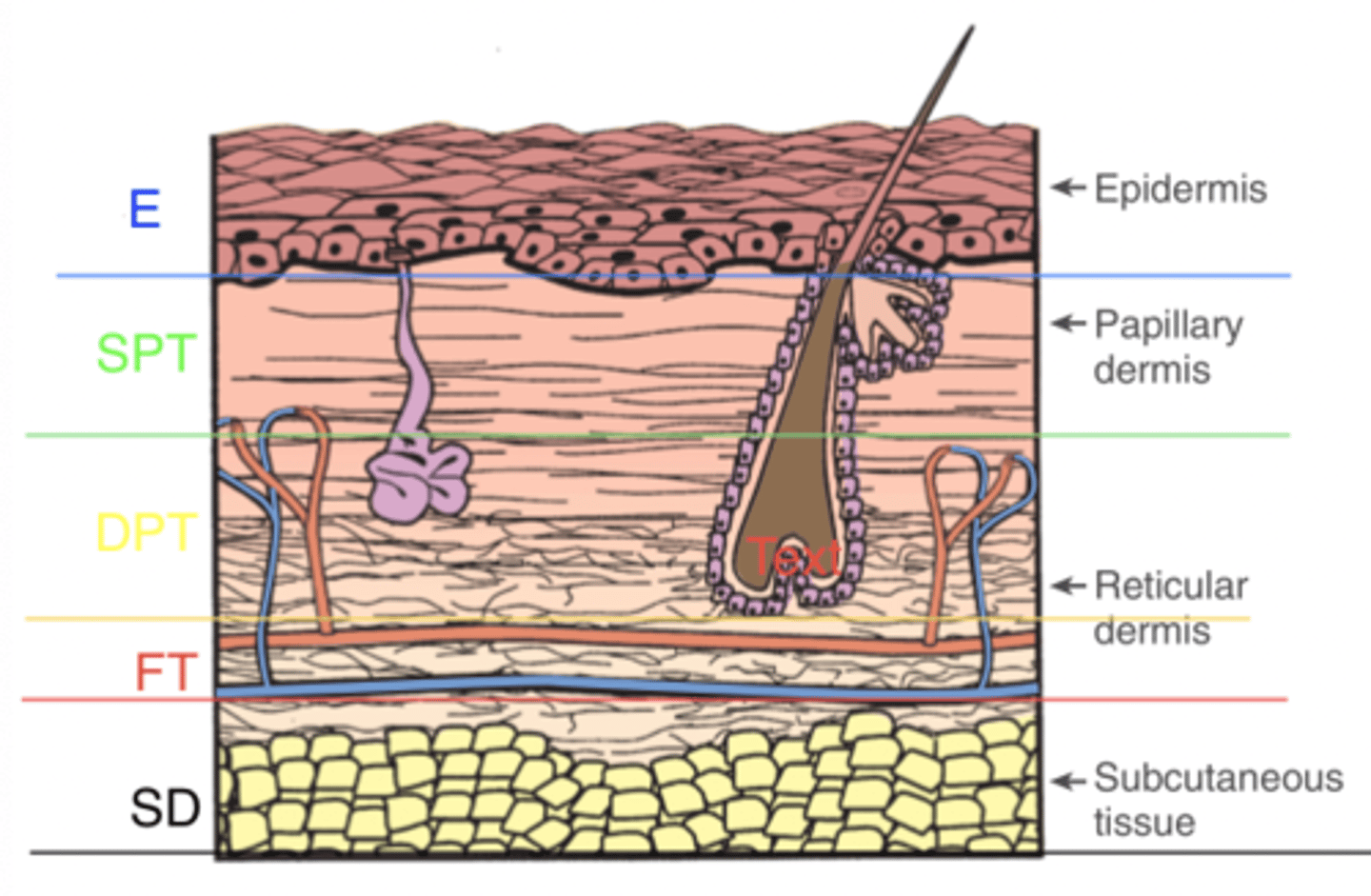
Subdermal burn (fourth degree) presentation
Charred, subcutaneous tissue evident, muscle damage
What burn wound classifications have spontaneous healing? Require skin grafts? Scarring?
Spontaneous- epidermal and superficial partial thickness
Skin grafts- full thickness and subdermal
Scarring- Deep partial thickness, full thickness, subdermal
Insenate
without feeling
Electrical burns- least resistance to most resistance
Nerves
Blood Vessels
Muscles
Bone
Electrical burns- entrance vs exit wounds
Entrance- charred and depressed, smaller
Exit- Typically at ground site, appears like an explosion out of the tissue
Electrical burns- viable vs not viable tissue
Due to attacks of vascular walls, and unpredictability, days are required to determine what tissues will be viable
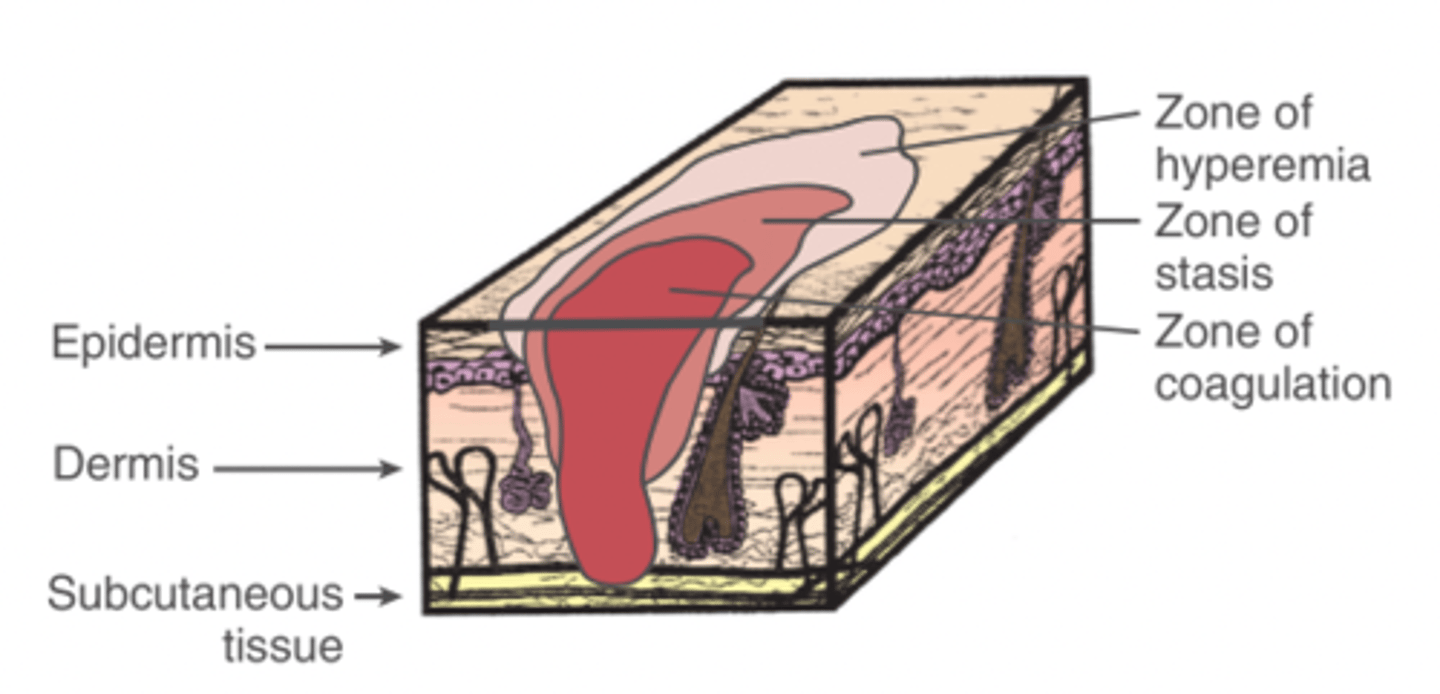
Zone of coagulation
The area of the burn that received the most severe injury with irreversible cell damage
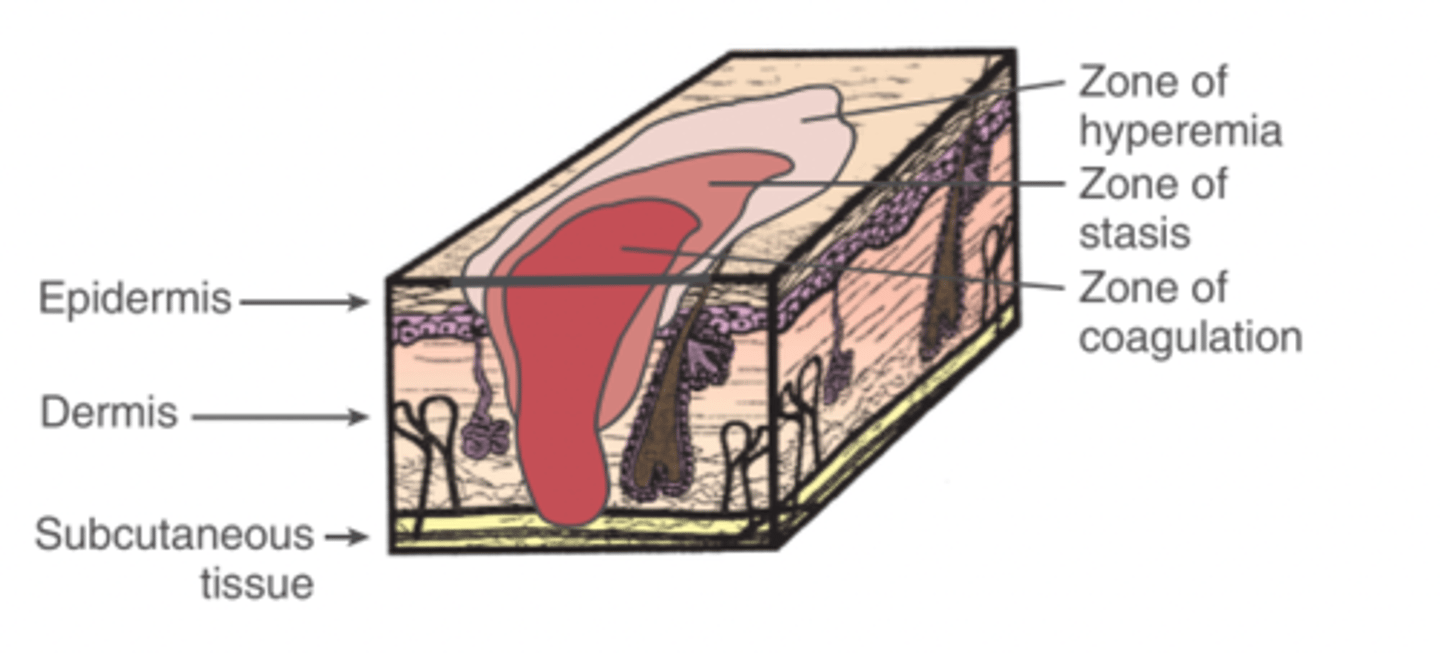
Zone of stasis
area of less severe injury that possesses reversible damage (may die in 24-48hrs without diligent treatment) and surrounds the zone of coagulation
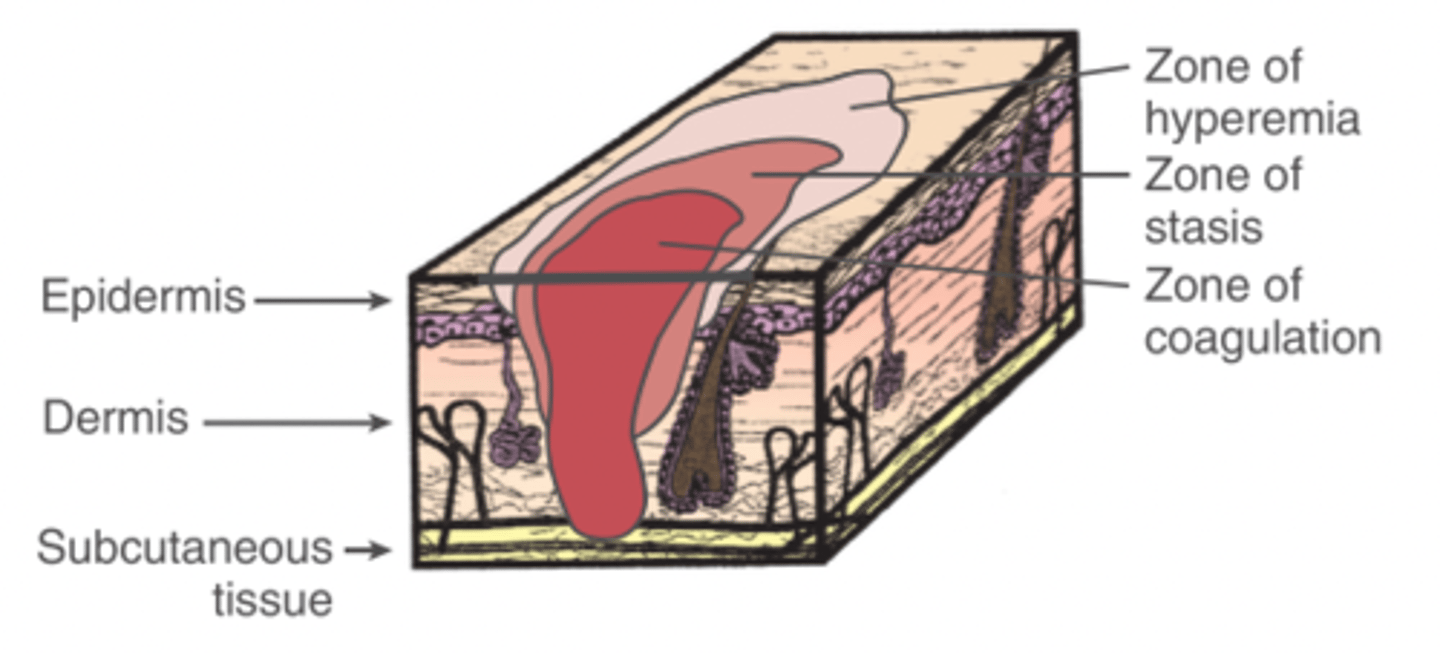
zone of hyperemia
The area surrounding the zone of stasis that presents with inflammation, but will fully recover without any intervention or permanent damage
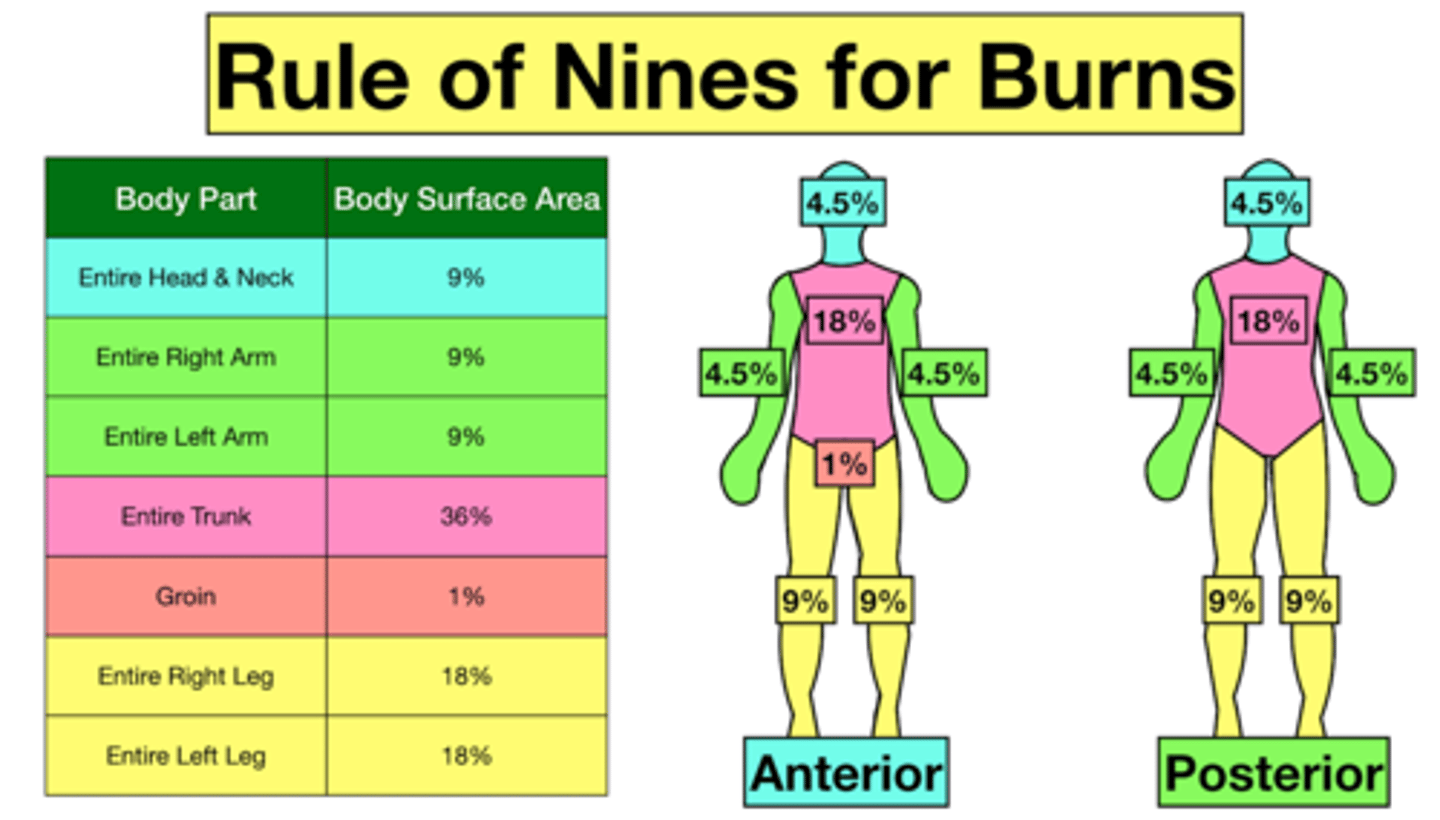
Rule of 9s
Calculations for assessing percentage of body surface burned.
Burn infection complication: what bacteria count constitutes infection and what is used to treat
10^5 bateria per gram of tissue
Systemic antibiotics
Burn pulmonary complication: signs of inhalation injury
facial burns, singed nose hairs, harsh cough, hoarseness, abnormal breath sounds, distress, sputum, hypoxemia
Burn pulmonary complication: diagnostic procedure
Bronchoscopy
Burn metabolic complication: what occurs
Metabolic rates increase rapidly with increase in TSBA burn, causing decrease in weight, decrease in muscle mass, negative nitrogen balance, decrease in energy stores
Burn metabolic complication: should room be kept warm or cool
Warm (86dgs F) to reduce metabolic rate
Burn cardiovascular complication: what occurs
Rapid fluid shift to interstitial, requiring fluid replacement therapy and significant edema
Burns and heterotrophic ossification
Uncommon complication following burns, but increases with increased TSBA burns
Burns and neuropathy: peripheral neuropathy and local neuropathy causes
Large TSBA burns can cause peripheral neuropathy that typically resolves over time
Local neuropathies result from compression bandage too tight, poor fitting splints, prolonged poor positioning
Common contracture for anterior neck burn
Flexion
Common contracture for shoulder-axilla burn
Adduction and IR
Common contracture for elbow burn
flexion and pronation
Common contracture for hand burn
Claw hand
Common contracture for hip and groin
Flexion and adduction
Common contracture for knee
Flexion
Common contracture for ankle
Plantarflexion
Critical burn classification
10% of body with 3rd dg burns and 30% with 2nd degree
Moderate burn classification
2-10% with 3rd dg burns and 15-30% with 2nd degree
Minor burn classification
Less than 2% with 3rd dg burns and less than 15% with 2nd dg
Hypertrophic scar
Raised scar that stays within boundary of burn
Keloid scar
Raised scar that extends beyond boundaries of original burn
Hypotrophic scar
flat & depressed below surrounding skin
Allograft
use of tissue from another person
xenograft
a graft from another species
Biosynthetic graft
combination of collagen and synthetics
Cultured skin
laboratory grown from patient's own skin
Autograft
skin graft from a person's own body
Split thickness graft
a skin graft that contains only a superficial layer of the dermis in addition to the epidermis
Full thickness graft
a skin graft that contains the dermis and epidermis
Autolytic dressings
use of moist dressings such as hydrogels or hydrocolloids to help remove eschar
Surgical or sharp debridement
excision of eschar using sterilized surgical instruments
Enzymatic debridement
using topical substances that break down dead tissue
Mechanical debridement
Physical removal of debris by irrigation, hydrotherapy or wet-to-dry dressing application