Endo 10 - Diagnosis (Dr. Monterio)⭐️
1/146
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
147 Terms
What are the 3 diagnosis objectives in endo?
- Reproduce the chief complaint
- Determine the cause
- Eliminate the cause
What is Step 1 in reaching an accurate endo diagnosis?
Establish chief complaint (subjective findings)
What is Step 2 in reaching an accurate endo diagnosis?
Review medical and dental history (subjective findings)
What is Step 3 in reaching an accurate endo diagnosis?
clinical exam (objective findings)
What is Step 4 in reaching an accurate endo diagnosis?
radiographic exam (objective findings)
What is Step 5 in reaching an accurate endo diagnosis?
diagnosis (assessment)
How should you record the patient's chief complaint?
- Write patients' own words ("I can feel my heart beating in my tooth")
- Listen to your patient!
- Ask why he/she is seeking dental treatment
T/F: Most medical conditions do not contraindicate the endodontic treatment but NEVER treat a stranger
True
What would the difficulty level be here according to the AAE Endodontic Case Difficulty Assessment Form and Guidelines:
- No medical problem (ASA Class 1*)
- No history of anesthesia problems
- Cooperative and compliant
Minimal difficulty
What would the difficulty level be here according to the AAE Endodontic Case Difficulty Assessment Form and Guidelines:
- One or more medical problem (ASA Class 2*)
- Vasoconstrictor intolerance
- Anxious but cooperative
Moderate difficulty
What would the difficulty level be here according to the AAE Endodontic Case Difficulty Assessment Form and Guidelines:
- Complex medical history/serious illness/disability (ASA Classes 3-5*)
- Difficulty achieving anesthesia
- Uncooperative
High difficulty
How often is the baseline blood pressure and pulse recorded?
Every visit
All of the following are included in what part of the history?
1. Does your patient present any medical disorder?
2. If so, is he/she compensated? Any recent complications?
3. Does he/she use medication for their systemic disease? Did he/she take it today?
4. Is he/she taking medications to relief their toothache?
5. Does he/she have any allergies?
6. Has he/she eaten in the last 3 hours?
Medical history
The dental history is divided into 5 basic directions of questioning:
- Location (Can you point to the offending tooth?)
- Commencement (When did the symptoms first occur?)
- Intensity (How intense is the pain from 0 to 10?)
- Provocation and attenuation (What produces or reduces the symptoms?)
- Duration (“Do the symptoms subside shortly, or do they linger after they are provoked?")

This is most likely what?
sinus tract

This is most likely what?
swelling
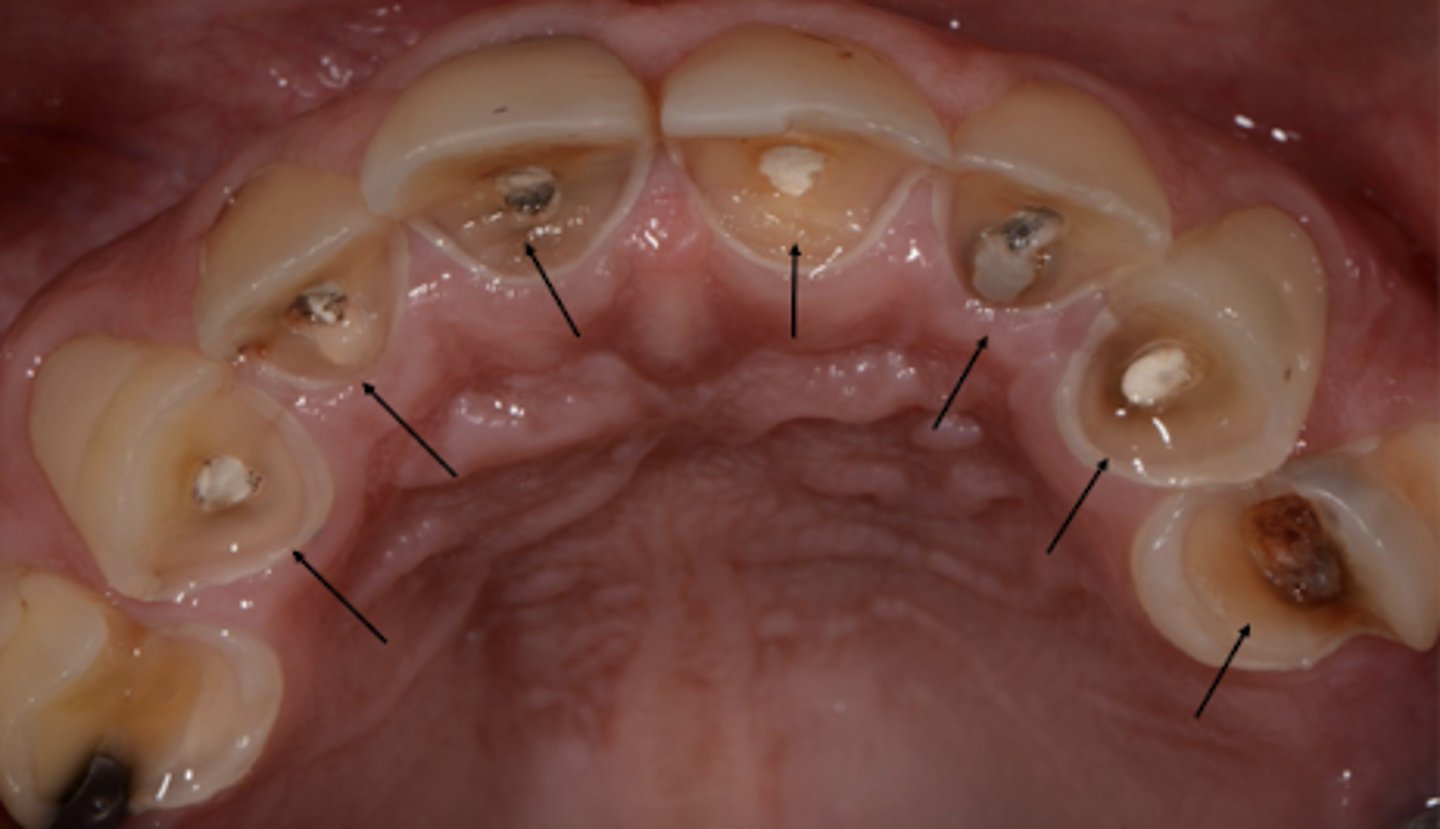
This is most likely what?
provisional restorations/exposed dentin

This is most likely what?
crown fracture/exposed dentin

This is most likely what?
caries

This is most likely what?
color alteration
Which is not a part of the armamentarium for diagnosis?
a) gauze pad
b) cotton pellet/roll
c) mirror
d) endo condenser
e) cotton pliers
f) explorer (regular and endo)
g) perio probe
h) endo ice
d (endo condenser)
All of the following are true when testing the teeth before endo diagnosis EXCEPT:
a) Patient is always the normality and the disease.
b) Test before what is normal to establish a baseline response
c) Always test the suspicious tooth first
d) Don't forget to investigate the opposing arch
e) Remember that these tests are comparison tests
f) Test the adjacent and contra-lateral teeth
c) Always test the suspicious tooth LAST
When should you test the suspected/problematic tooth?
last
Which teeth do you use as a comparison when doing pulp tests?
adjacent and contra-lateral
What are the four tests to evaluate the APICAL status of a tooth (pathology in the PDL)?
- Percussion
- Palpation
- Probing
- Mobility
Is testing the surrounding tissue an indication of pulp vitality or sensitivity?
No, it is not an indication
All of the following will give you information to reach an apical status diagnosis, EXCEPT:
A) Cold test
B) Percussion test
C) Palpation test
D) Perio probing
A) Cold test (that is for pulpal diagnosis, not apical status)
Which apical status test will help you identify detect swelling and bony expansions?
palpation test
Which apical status test includes the following?
- Soft Tissue Examination, palpation of the alveolar hard tissue (buccal and lingual)
- Apply firm digital pressure to the mucosa covering the roots and apices.
- Search for sensitive areas, that may indicate inflammatory process.
- Test the quadrant and compare right side and left side
Palpation
Which apical status test is initiated with a digital pressure then tap the incisal or occlusal surfaces with a blunt end of an instrument?
Percussion test
Which apical status test shows if there is or not inflammation in the periodontal tissue in the apical portion, not pulp vitality?
Percussion test
Once infection/inflammatory process has extended through the apical foramen into the PDL space and apical tissues, pain is localizable with what test?
Percussion test
T/F: For the percussion test in posterior teeth, you should test all the cuspids
True
Findings from which apical status test help differentiate between all of the following conditions?
- Occlusal premature contacts
- Apical disease
- Trauma
- Root cracks
Percussion test
After the percussion test, what is another test you can perform to test all cusps?
- Perform the bite test (tooth slooth)
- Occlusal test (marking paper)
What is the importance of percussion in Endodontic Diagnosis?
1. Valuable information about periapical status
2. The PDL is richly innervated by proprioceptive fibers, which makes it easier to localize where the pain comes from (once the infection/inflammation extended to the apical foramen into the PDL and apical tissue)
Which apical status test includes the following?
- Measurement of periodontal pocket depth (mesial, middle and distal aspects of both buccal and lingual sides) at least 6 points
- Isolated areas of vertical bone loss indicate endodontic origin
Periodontal probing
With a vertical crack, endo-perio lesion or excess of inter-proximal fillings, which clinical test can allow you to reach this differential diagnosis?
Periodontal probing
Which apical status test includes the following?
- Compromised periodontal attachment apparatus or the extension of inflammation in the periodontal ligament
- Pressure is applied in a facial-lingual direction and vertical direction and should be scored 0-3
Mobility test
Findings from which apical status test help differentiate between all of the following conditions?
- Acute or chronic physical trauma
- Occlusal trauma
- Parafunctional habits
- Periodontal disease
- Root fractures
- Extension of pulpal disease
Mobility test

Which test can reveal hidden decay or a fractured tooth, used for suspicion of cracks/fracture?
transillumination
How does the transillumination test work?
Teeth with fracture block the light, part of the tooth that is proximal to the light source will glow and areas beyond will not have light transmitted
Which test can methylene blue dye be used to determine the presence of crack in the surface of the tooth?
staining
What are the 2 sensitivity thermal tests to evaluate the pulpal status (responsiveness of pulpal sensory neurons) of a tooth?
- Cold test
- Electric Pulp Test (EPT)
T/F: you can administer a cold test whether the mucosa is wet or dry
False - clean, clear & dry tooth before cold test
Large cotton pellet made of a cotton roll and applied in the mid-facial of the tooth or crown that must be isolated and dry. Always test a normal teeth before. This is known as the ___________
cold test
what test is BEST for a pulpal diagnosis?
cold test
During the cold test, the patient reports sensation but disappears immediately upon removal of the stimulus. This is indicates ______
normal sensation/baseline response
During the cold test, the patient reports no response. This indicates ______
pulp necrosis (previously treated/previously initiated; other findings – trauma/calcification/open apex, etc)
During the cold test, the patient reports lingering/intensification of painful sensation after removal of the stimulus. This indicates ______
symptomatic irreversible pulpitis
During the cold test, the patient reports hypersensitivity to the cold but it does not linger. This indicates _________
reversible pulpitis
How do you instruct the patient during a cold test?
1 - Ask patient to raise hand when sensation is felt, then remove the stimulus
2 - Ask patient to lower hand when sensation ends - count the seconds that the sensation lasts
- Establish a baseline tooth before testing suspicious tooth
What test is used to cross-check when cold test is not reliable and functions by producing a pulsating eletrical stimulus?
Electric Pulp Test (EPT)
What can be used as a conducting medium for EPT?
toothpaste
For anterior teeth, the EPT probe is located in what third of the crown?
incisal
For posterior teeth, the EPT probe is located in what third of the crown?
middle
Which test includes the following?
- Should be applied on the tooth adjacent to a pulp horn
- Tooth isolation is essential
- When the patient feels a tingling or warm it should be removed
Electric Pulp Test (EPT)
When do you suspect the presence of disease during EPT?
When the numeric readings on the EPT differs SIGNIFICANTLY from readings obtained from a control tooth
(However, in most cases, response is scored either present or absent)
If you reach a max. reading on EPT, what is the probable diagnosis?
necrotic pulp
What type of test is a cold test?
Thermal
What type of test is EPT?
Elelctric
What nerve fiber do both cold and EPT target?
a-delta
Can a cold test be done on a restoration/crown?
Yes
Can an EPT test be done on a restoration/crown?
No - only tooth structure, but can be done on crown for cold test
Are either of the cold-test or EPT reliable on trauma/immature teeth?
No
Which pulp test causes osmotic changes inside the dentinal tubules?
cold
What tooth surface is the EPT test used on?
Buccal
Which pulp test causes ionic changes inside the dentinal tubules?
EPT
We perform heat test only when patient complains of pain when hot. What are three ways we can administer a heat test?
- Hot instrument
- Instrument friction
- Gutta percha (Use lubricant to keep GP from sticking to tooth)
What nerve fiber does the heat test target?
C fibers
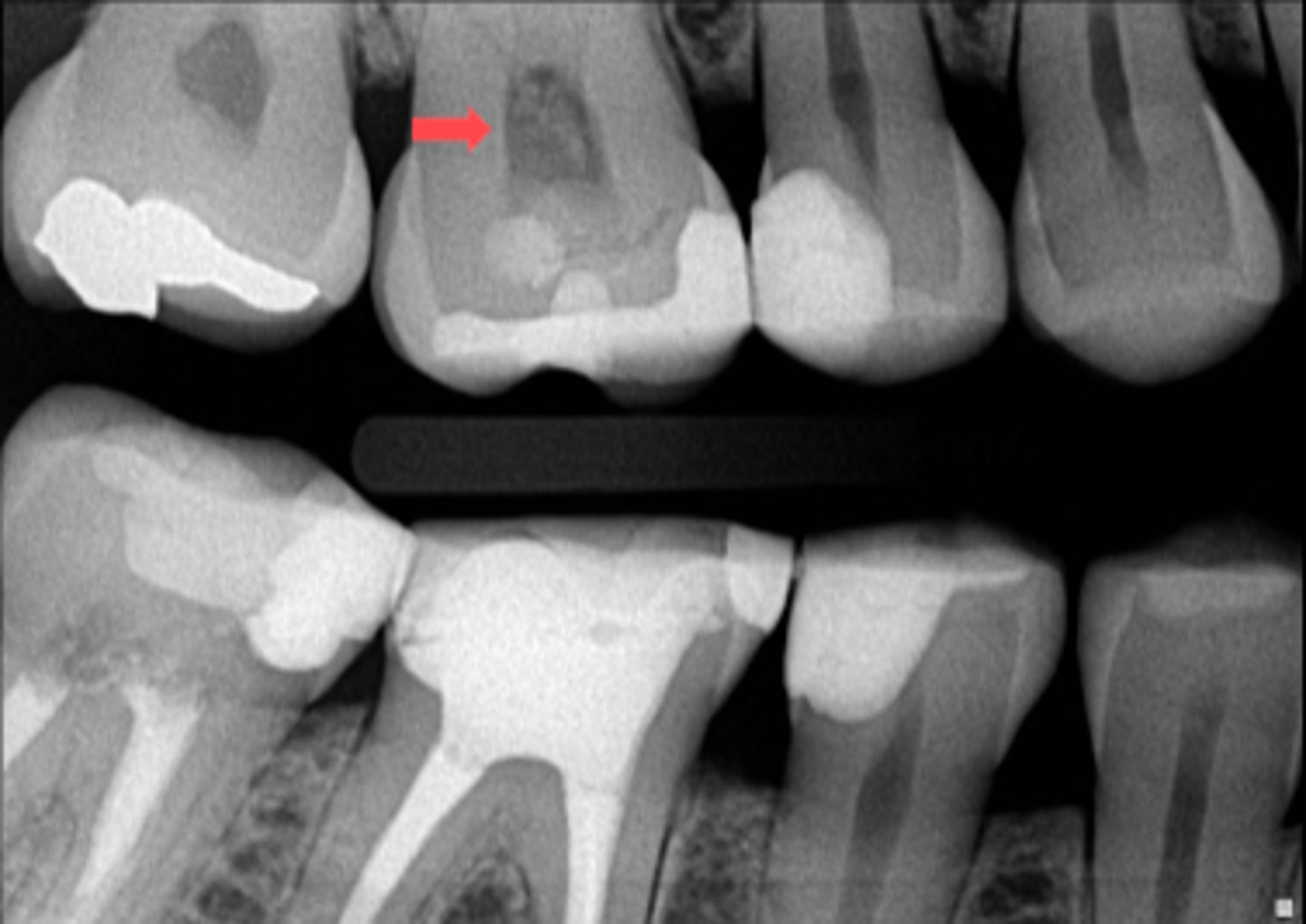
ID the abnormality in the radiograph:
pulp stones
Which test?
- It's an invasive irreversible test.
- Only used when all other test methods are inconclusive.
- Patient is not anesthetized to perform this procedure.
- If the patient reports pain, the procedure is terminated and the tooth is restored.
- If no sensation is felt, RCT is indicated.
Cavity test
Which test?
- When pulp testing is inconclusive and patient does not know if pain comes from maxilla or mandible.
- The injection is administered to the most posterior tooth in the quadrant of the arch that may be suspected, starting from the distal sulcus.
- The anesthesia is administered in an anterior direction, one tooth at a time.
Selective anesthesia
For an endo diagnosis, how many and what type of radiographs should you take?
1 PA/ 1BW (for posterior teeth)
1 PA (for anterior teeth)
(Always use sensor positioning devices, ex: ring device; at least 2 straight/shifted - mesial or distal or vertical angulation)
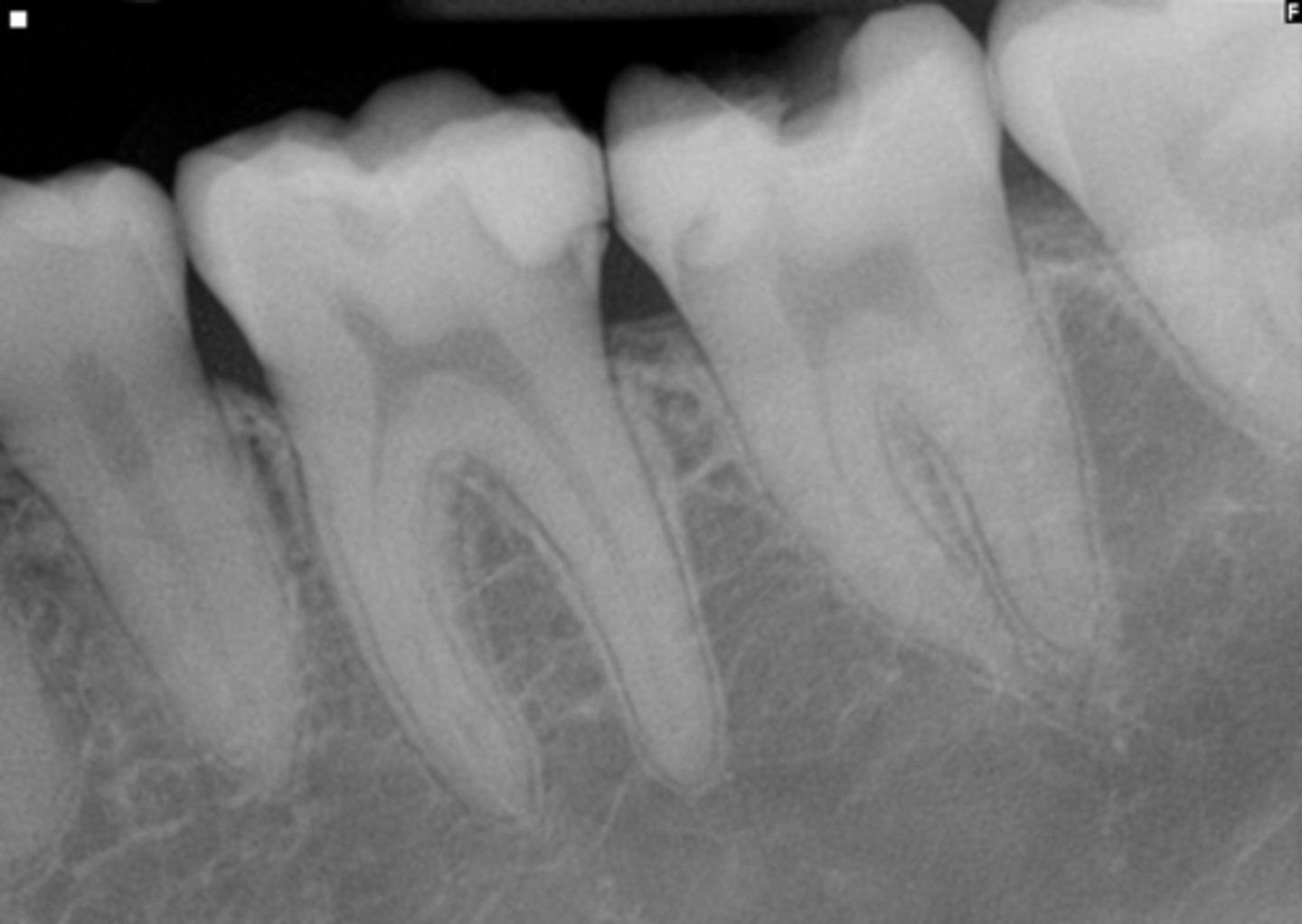
ID the radiographs:
- Pulp chamber size
- Inter-proximal excess
- Pulp stones
Bitewings
ID the radiographs:
- Examination of the entire tooth
- View of the periapical tissues
periapical radiographs
ID the radiographs
- Evaluation of caries, existing restos & previously initiated therapy
- Excellent projection to assess periodontal tissue
- Accurate representation of coronal pulp anatomy
Bitewings
ID the radiograph
- Recommended in trauma cases to rule out fracture of teeth and alveolus
Panoramic radiographs
ID the radiograph:
- Dimensionally accurate view of tooth and surrounding structures
CBCT

What does this show on the tooth?
Cracks
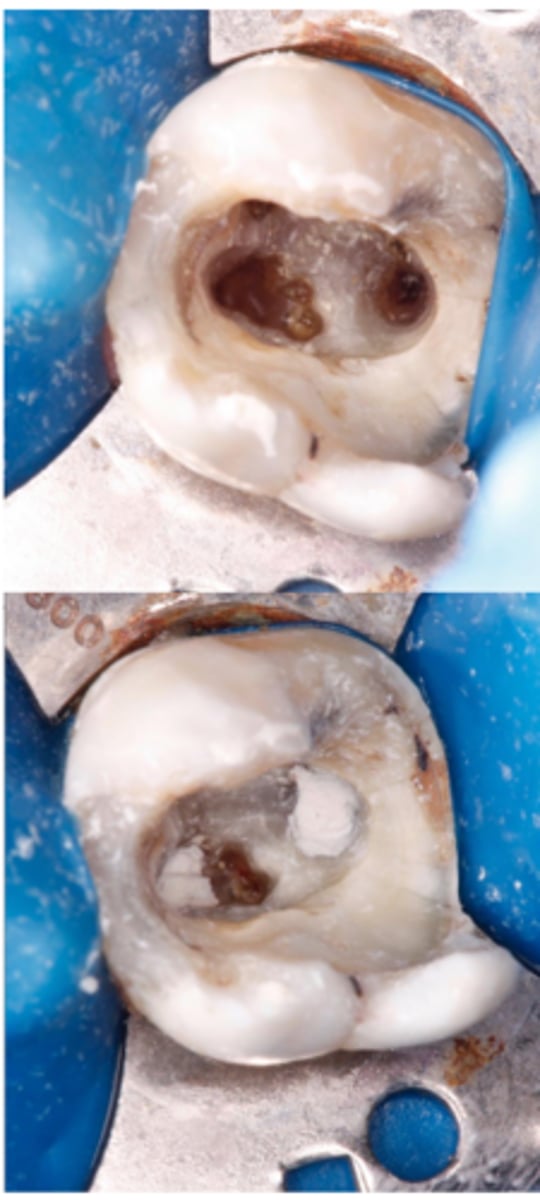
What does this show on the tooth?
Perforation

What does this show on the tooth?
Sinus tract
What are the two steps after clinical and radiographic examination to get to the correct diagnosis?
- Pulp diagnosis
- Periapical diagnosis
Pulp or apical diagnosis?
- Previously treated
- Previously initiated therapy
Pulp diagnosis
Pulp or apical diagnosis?
- Condensing osteitis
Apical diagnosis

ID the pulpal diagnosis:
- Pt has no symptoms
- Cold test: 1-2 seconds
- No intra-oral findings
normal pulp
AAE Terminology definition:
A clinical diagnostic category in which the pulp is symptom-free and normally responsive to pulp testing.
normal pulp

ID the pulpal diagnosis:
- CC: "My tooth hurts when I drink cold or eat sweets"
- Cold test: Hypersensitive non lingering (2-3 sec)
- Radiograph shows defective restoration
reversible pulpitis
AAE Terminology definition:
- A clinical diagnosis based on subjective and objective findings indicating that the inflammation should resolve and the pulp return to normal
(Pain not spontaneous it is triggered by stimuli A-delta fiber activation)
reversible pulpitis
What are five causes of reversible pulpitis?
- Caries
- Exposed dentin
- Defective restoration
- Recent restoration
- Scaling/root planning
What is the treatment and prognosis for reversible pulpitis?
- Tx: Remove source of irritation
- Prognosis: follow up
The pulp tissue is compromised in its ability to respond to external irritants because it's enclosed in a noncompliant environment, and it lacks collateral circulation. What will happen if the pulp is not treated?
The disease will progress to a certain point that the pulp tissue is incapable of healing

ID the pulpal diagnosis:
- Patient reports no symptoms
- Cold test: Hypersensitive non lingering (2-3 sec)
- Radiograph shows very deep caries into the pulp chamber
asymptomatic irreversible pulpitis
AAE Terminology definition:
- A clinical diagnosis based on subjective and objective findings indicating that the vital inflamed pulp is incapable of healing.
- Additional descriptors: no clinical symptoms but inflammation produced by caries, caries excavation, trauma
- Left untreated can become symptomatic or necrotic
asymptomatic irreversible pulpitis
What is the treatment for asymptomatic irriversible pulpitis?
- RCT
- Extraction
What is the difference between reversible pulpitis and asymptomatic irriversible pulpitis?
deep caries
ID the pulpal diagnosis:
- CC: "My tooth hurts randomly, I can't even touch it"
- Cold test: Hypersensitive lingering (30 sec or more)
- Radiograph shows very deep caries into the pulp chamber
symptomatic irreversible pulpitis

AAE Terminology definition:
- A clinical diagnosis based on subjective and objective findings indicating that the vital inflamed pulp is incapable of healing.
- Additional descriptors: lingering thermal pain, spontaneous pain, referred pain
symptomatic irreversible pulpitis
What is the diagnosis?
- Pain relievers don't work
- C-fibers activation (dull, throbbing pain)
- Pain is spontaneous/unprovoked
symptomatic irreversible pulpitis
What can cause symptomatic irreversible pulpitis?
- Deep restorations/caries reaching the pulp
- Fractures/cracks
- Crown prep close to pulp
- Pulp exposure