CHAPTER 4-5 FSHN 322
1/69
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
70 Terms
Preterm pregnancy
Defined as delivery before 37 weeks of gestation.
Term pregnancy
Defined as pregnancy lasting between 38 to 42 weeks.
Post-term pregnancy
Defined as pregnancy lasting beyond 42 weeks.
Low birthweight
Infants who weigh less than 2500 grams at birth, often associated with preterm deliveries.
Preterm delivery
Delivery that occurs before 37 completed weeks of pregnancy.
nutritional Increasing risk
o Underweight and gain less than recommended
o Pre-pregnancy obesity
o Increased cholesterol, TG, FFA, markers of inflammation and oxidative stress
· Decreasing risk
o Use of multivitamin supplements and adequate folate intake
o 1-3 fish meals per week
o exercise
Infant mortality
The death of an infant before their first birthday.
Nutritional genomics
Study of how nutrition and genetics interact and how this affects disease risk.
Epigenetic modification
Changes in gene expression caused by mechanisms other than changes in the DNA sequence.
Fetal origins of adult disease hypothesis
Theory suggesting that environmental factors during fetal development may affect health later in life.
Dutch famine studies
Research analyzing health effects on individuals exposed to famine during gestation. • Decreased glucose tolerance
Famine exposure during early gestation
• Atherogenic lipid profile
• Increased BMI and CHD risk
Anabolic phase of pregnancy
The first 20 weeks where nutrient stores are built and fat is accumulated.
Blood volume expansion
increased cardiac output
buildup of fat, nutritent, and liver glycogen stores
growth of some maternal organs
increased appetite & food intake
decreased exercise tolerance
increased levels of anabolic hormones
Catabolic phase of pregnancy
The phase after 20 weeks when fat and nutrient stores are mobilized for fetal growth.
Mobilization of fat and nutrient stores
Increased production and blood levels of glucose, triglycerides, and fatty acids
Decreased liver glycogen stores
Accelerated fasting metabolism
Increased appetite and food intake declines near term
Increased levels of catabolic hormones
Placenta
o Hormone and enzyme synthesis
o Nutrient and gas exchange
o Removal of waste products from fetus
o Prevents passage of maternal red blood cells, bacteria, and large proteins

Human Chorionic Gonadotropin (hCG)
Maintains early pregnancy by stimulation estrogen and progesterone production by 2nd month
Progesterone
• Maintains implant
• Induces changes in uterine and gastrointestinal structure
• Stimulates Brest duct development
• Promotes Brest and uterine development
Estrogen
• Increases fat synthesis and deposition
• Protein synthesis
• Promotes breast and uterine development
Human Chorionic Somatotropin (hCS)
• Increases maternal insulin resistance
• Promotes protein synthesis
• Breakdown of maternal energy source
Leptin
• Regulates appetite and fat metabolism
• Weight gain
• Utilization of fat as maternal energy source
Glucose metabolism in pregnancy
Insulin insensitivity in the third trimester increases glucose availability for the fetus.
Protein metabolism in pregnancy
Accumulation of proteins occurs, with minimal nitrogen excretion.
Fat metabolism in pregnancy
First half: fat storage
Second half: fat breakdown
Calcium requirements in pregnancy
Pregnant women need additional calcium to support fetal skeletal development.
o Increased water volume and tissue synthesis requires increased sodium and other electrolytes
Sodium requirements in pregnancy
Increased sodium intake is necessary due to increased blood volume.
Pica
Craving for non-food items, often linked to mineral deficiencies.
Fetal growth classifications
AGA, LGA, IUGR, SGA - classifications based on growth parameters.
AGA
Appropriate for gestational age - 10th to 90th percentile.
LGA
Large for gestational age - above the 90th percentile.
IUGR
Intrauterine growth restriction - term for infants who are smaller than expected.
SGA
Small for gestational age - below the 10th percentile.
Postpartum weight retention
Women retaining more weight after delivery due to insufficient weight loss.
Caloric recommendations during pregnancy
Additional caloric intake of 340-452 kcal/day based on trimester.
+0 kcal/day for first trimester
+340 kcal/day for second trimester
+452 kcal/day for 3rd trimester

Carbohydrate needs in pregnancy
45-65% of daily calories should come from carbohydrates, with a minimum of 175g.
At least 175g
From:
• Whole grain products
• Fruits and vegetables
• Other foods that contain no added sugars
Protein needs in pregnancy
Recommended protein intake is 71g/day for tissue synthesis.
Needs to increase
71 g/day
Used for tissue synthesis (for baby)
Omega-3 fatty acids in pregnancy
300mg/day of EPA and DHA is recommended for fetal neural development.
• 1.4g/day
• Eicosapentaenoic acid (EPA) & Docosahexaenoic acid (DHA) are crucial for fetal neural development, and can be made from dietary ALA, but in low amounts (only 9% conversion of ALA to EPA/DHA)
o Must be obtained from diet
o From:
Cod liver oil
Fish oil (salmon, sardines, herring)
Folic acid requirements in pregnancy
600 mcg daily; 400 mcg from fortified foods.
· Orange
· Pineapple juice
· Papaya juice
· Dried beans
· Cereal
· Bread
· Pasta
· Rice
MTHFR C677T variant
Gene variant affecting folate metabolism, higher risk for neural tube defects.
Food safety considerations in pregnancy
o Pregnant women are more susceptible to foodborne infections
Listeria monocytogenes (spontaneous abortions and stillbirth)
o Avoid:
Raw fish
Oysters
Uncooked meat
Unpasteurized milk
Correctly store lunch meats and hotdogs
Raw meats
• Can be passed on from cats
Large, long lived fish
• Sharks
• Swordfish
• Tilefish
• Albacore tuna
• Bass
o Risks
Toxoplasma gondii (mental retardation, blindness, death)
Mercury (fetal neurotoxin)
Exercise recommendations during pregnancy
At least 150 minutes of moderate exercise per week.
Hyperemesis gravidarum
Severe nausea and vomiting during pregnancy.
Heartburn management during pregnancy
Eat small meals, avoid lying down after eating, limit acidic foods.
Constipation management during pregnancy
Increase dietary fiber and hydration; laxatives are not recommended.
Gestational diabetes (GDM)
Diabetes that develops during pregnancy, often managed through diet and exercise.
Risks associated with GDM
Increased risks of stillbirth, macrosomia, and early C-section.
Mean gestational age for twins
Twins average a gestational age of 37 weeks.
Mean gestational age for triplets
Triplets average a gestational age of 33-34 weeks.
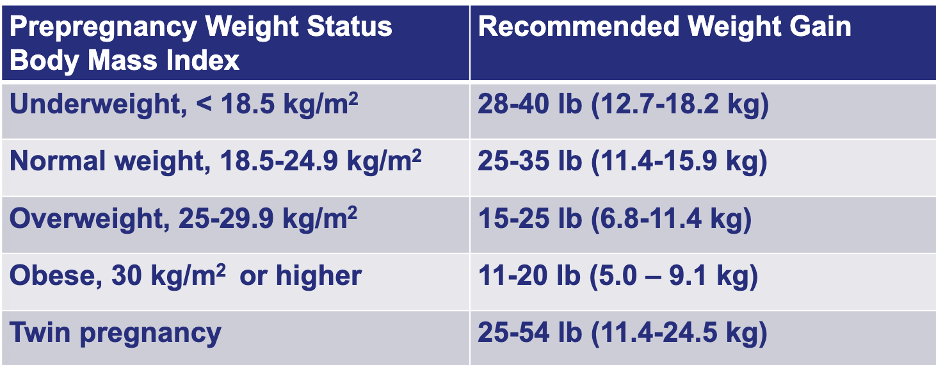
Weight gain guidelines for multifetal pregnancies
Recommended gain of 37-54 lbs for twin pregnancies.
Eating Disorders during pregnancy
Associated with risks such as low fertility and poor weight gain.
Nutrition recommendations for pregnant teens
Increased caloric, calcium, and vitamin D needs, similar protein as adults.
weight gain guidelines
o dSGA
disproportionally SGA
<10th percentile for gestational age
with normal length and head circumference
Skinny, wasted appearance, small abdomens, little body fat
Due to low maternal weight gain or poor nutrition in 3rd trimester
o pSGA
proportionally SGA
<10th percentile for weight, length,and head circumference
Small but normally proportioned
Likely due to long-term malnutrition in utero
postpartum weight retention
o Prevent by:
Pregnancy weight gain management programs
Weight loss of 1 to 2 pounds per month
Breastfeeding may facilitate weight loss but should not be promoted as an effective weight loss method
Linoleic acid (omega-6)
• 13g/day
• From plany oils
four types of hypertensive disorders during pregnancy
o Chronic hypertension
o Gestational hypertension
o Preeclampsia & eclampsia
o Preeclampsia & eclampsia
Oxidative stress
Platelet aggression, increased coagulation
Restricted blood flow
Hypertension
Insulin resistance
Increased FA TG cholesterol
Proteinuria
Pre-pregnancy and pregnancy diets high in plant foods and fiber tend do decrease while diets high in processed meats, drinks and salty snacks tend to increase the risk
Additional antioxidants
• No individual supplement has shown to be effective
Salt
• No restriction has shown to make change
Gestational hypertension
First occurs during pregnancy
Increased risk of later hypertension and stroke
Associated with maternal obesity and central adiposity
Recommendations
• Similar dietary recommendations to chronic hypertension
o Chronic hypertension
Diagnosed before pregnancy
Increased risk of preeclampsia, preterm, growth, retardation
Recommendations
• Follow hypertension related diet prescribed before pregnancy
• Salt restriction is NOT recommended but can be decreased if previously treated
the three main types of diabetes during pregnancy
o Gestational diabetes
o Type 2
o Type 1
Type 1
Blood glucose should be monitored closely
Management
• Dietary intake
• Exercise
• Insulin dose
• Ketones should be monitored
Type 2
Occurs in women who enter pregnancy with T2DM will need medical nutrition therapy and close monitoring
Management
• Good glucose control before pregnancy
• Time meals with glucose levels and insulin
• Minimize hyper OR hypo glycamia
• Monitor and adjust weight gain
• Manage carbs and include appropriate fiber, fruits, veg, unsat fats
o Gestational diabetes
In 2-12% of pregnancy, increases with maternal obesity
Outcomes in mother
• Early C section
• Shoulder dystocia
• Maternal death
• Increased risk of preeclampsia
• Increased risk of gestational diabetes, hypertensino, T2DM
Outcomes in newborn
• Stillbirth, spontaneous abortion, macrosomia (>10lbs)
• Congenital anomalies
• Increased risk of obesity, hypertension, T2DM, Hypoglycemia, Hypocalcemia
Treated through diet and exercise
• Assess diet and exercise habits
• Develop individualized diet and exercise plan
• Monitor weight gain and dietary intake
• Interpret blood glucose and urinary ketone results
• Follow up during pregnancy and postpartum
• Diet plan
o Whole grains
o Fruits
o Vegetables
o Unsat fat
o Decrease foods and beverages with simple sugars
o Monitor carb intake
o 3 meals and snacks with distributed calories
GM in mother
• Early C section
• Shoulder dystocia
• Maternal death
• Increased risk of preeclampsia
• Increased risk of gestational diabetes, hypertensino, T2DM
GM in newborn
• Stillbirth, spontaneous abortion, macrosomia (>10lbs)
• Congenital anomalies
• Increased risk of obesity, hypertension, T2DM, Hypoglycemia, Hypocalcemia
twin risks in mom
Hypertension and preelampsia
Anemia
GDM
Placenta previa
Kidney disease
Preterm delivery
C section
Fetal loss
twin risks in baby
Death
Congenital abnormalities
Respiratory distress
Cardiac dysfunction
Cerebral palsy
LBW
twin birth age & brithweights
37 weeks
5.4 lbs
triplet birth age & brithweights
33-34 weeks
4.0 lbs
nutritional recommendations for twins+
Balanced diet
Increase caloric needs (+450 cal a day)
Vitamin and minerals similar to when having one
risk with ED pregnancy
o Risks
Low fertility
Preterm labor
Spontaneous abortion
IUGR
Hypertension
Anemia
UTI
Poor weight gain
o Behavioral changes
o Ketosticks to help understand when they are not consuming enough food for healthy pregnancy
guidelines for pregnant teens
o Similar weight gain and protein as adults
o Increased caloric needs
o Increased calcium (+300 mg) and vitamin D needs
o Referral to food and nutrition programs
