MLS BB advanced final
1/284
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
285 Terms
Whats a phenotype?
Observable trait, trait that is expressed
Whats a genotype?
Genetic makeup, genes that are present but cannot be expressed
What does heterozygous
2 of same gene, different copies (Hh)
What does homozygous mean?
2 identical copies of same gene (HH or hh)
Size of IgG
50,000
Size of IgM
900,000
Does IgG cross the placenta
Yes
Does IgM cross the placenta
No
Optimal temperature of IgG
Body temp, 37 degrees
Optimal temperature of IgM
RT, 4-25 degrees C
Is IgG clinically significant?
Yes
Is IgM clinically significant?
No, except ABO
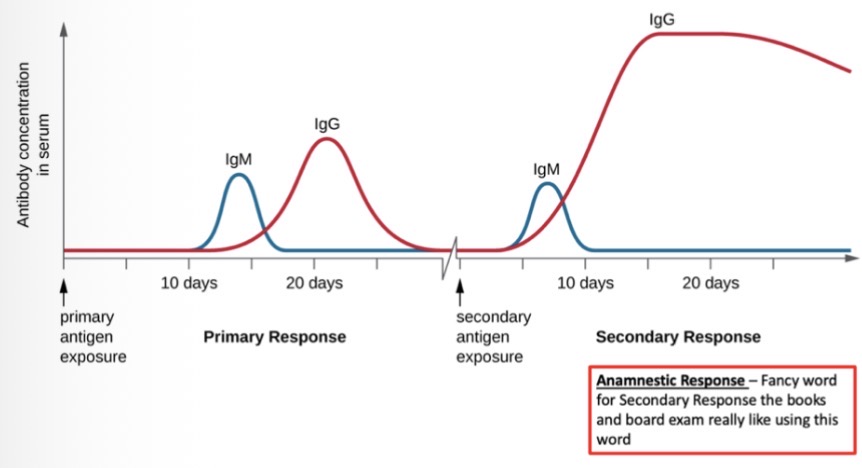
Appearance of IgM and IgG antibodies- primary and secondary
What is Landsteiner’s rule?
If the antigen is present on RBCs, the corresponding antibody will be absent from serum, if the antigen is absent then the antibody will be present
Type O has what ABO antibodies in their plasma?
Anti A and anti B
Type A has what ABO antibodies in their plasma?
Anti-B
Type B has what ABO antibodies in their plasma?
Anti-A
Type AB has what ABO antibodies in their plasma?
No antibodies
What is the universal blood type for RBCs?
O neg
What is the universal blood type for plasma?
AB neg or AB pos
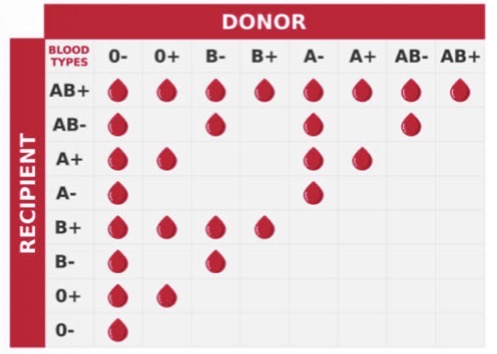
ABORh compatibility for red cells
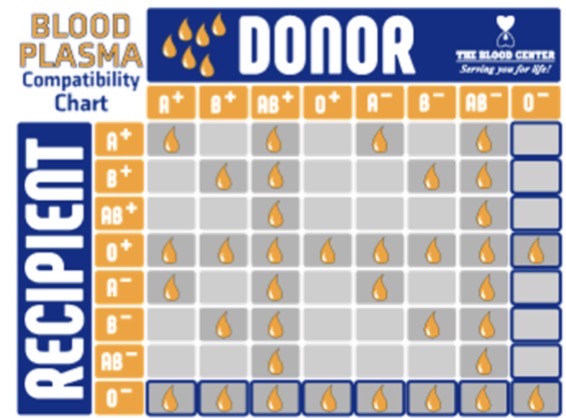
ABO compatibility for plasma
Whats the amount of H antigen on the red cell by blood type- From most H to the least amount of H antigen
O>A2>B>A2B>A1>A1B
What are the reactions in an ABORh front type and back type in Bombay blood type?
Pos for all Anti-A, Anti-B, anti-o, and anti-H
What are the antibodies a Bombay patient make?
A,B,O,H,AB
What is the genotype for HH, Hh, and hh?
hh
What blood is given for transfusion for Bombay patients
Only Bombay people
What the amount of H on the red cells?
None
How do you tell subgroup A2 from A1?
Use diluted extract of Dolichos Biflorus agglutinates A1 but not A2 RBCs
How to transfuse subgroup A2?
Use Type A unless Anti-A1 is present, then use type O or A2
Why is lectin used for subgroup A2?
They are saline extracts of seed react with specific carbohydrates on RBC membrane?
What are the reagents in front type?
Anti-a, anti-b, anti-d (antigen)
What are the reagents in the back type?
A1 cells, B cells (antibody)
What are check cells and when are they used?
Check cells are known reactive cells that are added if there is AB pos, to check if the reagents are reacting correctly instead of only providing positive results
What do check cells prove?
Prove that the reagent is working effectively
What is an elution?
Removes antibodies from red cell membrane
What is an adsorption?
Removes antibodies from plasma or serum
When can we NOT perform an auto adsorption?
If the patient has had a recent transfusion in the past 3 months
What is the Fisher-Race nomenclature of R0 (Weiner)
Dce
What is the Fisher-Race nomenclature of R1 (Weiner)
DCe
What is the Fisher-Race nomenclature of R2 (Weiner)
DcE
What is the Fisher-Race nomenclature of RZ(Weiner)
DCE
What is the Fisher-Race nomenclature of r (Weiner)
dce
What is the Fisher-Race nomenclature of r’ (Weiner)
dCe
What is the Fisher-Race nomenclature of r” (Weiner)
dcE
What is the Fisher-Race nomenclature of ry (Weiner)
dCE
What phenotypes contain the G antigen?
R0, R1, R2, Rz, r’, ry
What phenotypes can make anti-G?
r, r”
Why would a patient who is dce/dec transfused with dCe/dCe red cells, make both Anti-D and Anti-C
The donor cells has C and G-antigen, so it mimics having D antigen thus making Anti-D
What is RHD responsible for and what do they need to be expressed?
Codes for D antigen→ people who have deletion of this gene or have defective RHD genes do not express D antigen and they are D neg
What is RHCE responsible for and what do they need to be expressed?
Codes for C, c, E, e→ all on same protein, difference between big and little one is one amino acid
What is RHAG responsible for and what do they need to be expressed?
Codes for rhAg antigen on chromosome 6→ important in expression of Rh antigens and RhAg is needed to express DCcEe antigens
What antibodies could an Rhnull patient make?
All antibodies because no Rh antigens (anti-C, anti-E, anti-c, anti-e, anti-D)
What antigens is Rh6 (f) directed against and what Weiner genotype would these antigens occur?
ce R0 or r
What antigens is Rh7 directed against and what Weiner genotype would these antigens occur?
Ce R1 or r’
What antigens is Rh22 directed against and what Weiner genotype would these antigens occur?
CE Rz or ry
What antigens is Rh27 directed against and what Weiner genotype would these antigens occur?
cE R2 or r”
Is big K high or low prevalence?
Low, 9%
Is little k high or low prevalence?
High, 99.8%
Is Kpa high or low prevalence?
2%
Is Kpb high or low prevalence?
High, 99.9%
Is Jsa high or low prevalence?
Low, <0.1%
Is Jsb high or low prevalence?
High, 100%
Why do blood bankers say “Kell Kills”
Kell Kills because anti-K causes a unique form of hemolytic disease of the fetus/newborn. Anemia associated with anti-K induced HDFN can be deVere because the antibody suppresses erythropoietin by attacking immature K-pos red cell precursors in the bone marrow
Which Duffy phenotype that has protection against malaria?
Fya and Fyb negative protects against malaria
Do the Duffy antibodies demonstrate dosage?
Yes
Can Duffy antibodies cause HDFN or hemolytic transfusion reactions?
Yes
Are Duffy antigens enhanced by enzymes
No, they are destroyed by enzymes (ficin)
Can Kidd antibodies cause HDFN and hemolytic transfusion reactions?
Yes
What transfusion reaction are the Kidd antibodies famous for causing?
Delayed hemolytic transfusion reactions because the antibody activity disappears quickly between both in vitro and vivo
Is Kidd enhanced by enzymes?
Yes
Does Kidd demonstrate dosage?
Dosage dependent, strength of reaction depends on number of antigen sites
Are Lewis antibodies clinically significant?
No
Does Lewis cause HDFN or hemolytic transfusion reactions?
No, rare hemolytic transfusion reactions
In which conditions do you see a decrease or loss of the Lewis antigens on the red cells?
Pregnancy, cancer, infectious mononucleosis, severe alcoholic cirrhosis, alcoholic pancreatitis, viral or parasitic infection
What would be in the secretions and on the red cells of someone who has this genotype Le, Se, BO, H?
Lea, Leb, A, B, H / ABH Le(a-b+)
What would be in the secretions and on the red cells of someone who has this genotype Le, sese, BB, H?
Lea / B/H Le(a+b-)
What would be in the secretions and on the red cells of someone who has this genotype lele, Se, AA, H?
A, H / A Le(a-b-)
What would be in the secretions and on the red cells of someone who has this genotype lele, sese, AB, H?
No secretions / AB Le(a-b-)
Is this MNS blood group enhanced by enzymes?
No, destroyed by enzymes
Are the M and N antibodies IgM or IgG?
50-80% are IgG but react at room temp
Are the M and N antibodies considered clinically significant?
Rarely, unless reactive at 37 degrees C
At what phase do the M and N antibodies react?
Immediate spin because they react at room temp
Are the S, s, and U antibodies IgM or IgG
Anti-S and anti-s = IgG (some IgM), anti-U = IgG
Are the S, s, and U antibodies considered clinically significant
Yes
At what phase do the S, s, and U antibodies react?
AHG at 37 degrees C
Are anti=I, anti-HI, anti-i considered clinically signficant?
They’re all very rare
What disease is associated with anti-I, anti-HI, anti-i?
Cold hemagglutination disease (CHAD CAD)
Anti-big I can be seen in people who have what infection?
Some autoimmune disorders and hemolytic anemia, mycoplasma pneumoniae, and anti-I, viral infections (ABV or CMV) show rare anti-I
Anti-little i can be seen in people who have what infection?
Anti-little i = infectious mononucleosis
Is anti-Le IgM or IgG?
IgM but occasionally IgG→ optimal at room temp, immediate spin
Is anti-Le clinically significant?
Not clinically significant
Can anti-Le cause HDFN or hemolysis?
Not clinically significant
Is dosage seen in Anti-Le?
No dosage seen
Is anti-K IgG or IgM?
IgG but rare IgM→ react at AHG and 37 degrees C
Is anti-K clinically significant?
Not clinically significant
Can anti-K cause HDFN and HTR?
Can cause severe HDFN and HTR
Do you see dosage in anti-K?
Dosage dependent
Is anti-Kpa IgG or IgM?
IgG→ AHG and 37 degrees C
Is anti-Kpa clinically significant?
Yes