Exam 4
1/193
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
194 Terms
Definition of Crisis
Acute, time-limited event (4–6 weeks)
Client cannot cope using usual mechanisms
Client was previously mentally healthy
Key Concepts
NOT pathological → normal response
Personal perception matters
Outcome:
Growth OR
Psychological deterioration
Common Characteristics of Crisis
Sudden, unexpected event
Perceived as overwhelming or life-threatening
Loss of support/communication
Sense of displacement
Actual or perceived loss
Types of Crises
1. Situational (External)
Unexpected life events
Examples:
Divorce
Job loss/change
2. Maturational (Internal)
Developmental transitions
Require new coping skills
Examples:
Marriage
Retirement
3. Adventitious (Disaster)
Large-scale traumatic events
Examples:
Natural disasters (hurricane)
Crimes, war
Assessment- crises
Key Assessments
Suicidal or homicidal ideation (FIRST)
Client’s perception of event
Support system
Coping skills
Cultural/religious needs
Physical + Behavioral Findings
Disorganization
Anxiety/overwhelm
Poor problem-solving
Anger/aggression
Risk Factors- crises
Unresolved losses
Current stressors
Mental/physical illness
Fatigue or pain
Developmental stage
🔹 Protective Factors
Strong support system
Previous coping experience
Phases of Crisis
Phase 1
Anxiety ↑ → defenses activated
Phase 2
Defenses fail → disorganization
Trial-and-error coping
Phase 3
Severe anxiety/panic
Withdrawal or flight
Phase 4
Overwhelming anxiety
Possible:
Dissociation
Depression
Violence (self/others)
NURSING CARE (CRISIS)
PRIORITY INTERVENTIONS
Ensure safety first
Assess suicide/homicide risk
Assist with hospitalization if needed
🔹 Initial Nursing Actions
Identify problem
Take active, directive role
Help set realistic goals
Focus on short-term solutions
🔹 Therapeutic Communication
Stay with client
Maintain eye contact
Listen actively
Ask about:
Feelings
Event
Be:
Calm
Clear
Genuine
Avoid:
False reassurance
Nontherapeutic responses
🔹 Interventions
Reduce anxiety
Teach relaxation techniques
Teach coping skills
Encourage participation
🔹 Action Plan
Short-term
Realistic
Focused on crisis
🔹 Debriefing
Staff + client discussion post-crisis
Example:
Critical Incident Stress Debriefing (CISD)
Levels of Care- crisis
Primary Prevention
Prevent crisis
Teach coping skills
Secondary Prevention
During crisis
Focus on safety
Tertiary Prevention
Recovery phase
Rehab, outpatient care
Medications (Crisis)
Antianxiety:
Lorazepam, Diazepam
Antidepressants:
Paroxetine, Fluoxetine, Bupropion
Client Education- crisis
Use community resources:
Crisis hotlines
Support services
Follow-up care is essential
ANGER MANAGEMENT
Key Definitions
Anger:
Normal emotional response to frustration
Aggression:
Verbal/physical attack
Violence:
Intent to harm
🔹 Important Concept
Clients with mental illness are:
More likely to harm themselves than others
Causes of Anger
Underlying feelings:
Insecurity
Fear
Guilt
Rejection
Can be secondary to:
Depression
PTSD
Anxiety
Grief
🔹 Comorbidities
Depression
Substance use
Bipolar disorder
PTSD
Dementia
Personality disorders
Stages of Aggression
1. Preassaultive
Anxiety, tension
Verbal aggression
Hyperactivity
2. Assaultive
Violence occurs
May require:
Seclusion
Restraints
3. Postassaultive
Recovery phase
Debriefing
SECLUSION & RESTRAINTS
LAST RESORT ONLY
Use only if:
Client is danger to self/others
🔹 Legal Requirements
Provider order required:
Reason
Time limit
Type
Removal criteria
🔹 Monitoring
Face-to-face eval within 1 hr
Continuous monitoring (q15 min)
NEVER leave alone
🔹 Nursing Responsibilities
Check:
VS
Circulation
Skin integrity
Provide:
Fluids, food, toileting
ROM exercises q2 hr
Document EVERYTHING
AGGRESSION ASSESSMENT
Risk Factors
History of violence
Poor impulse control
Substance use
Psychosis (hallucinations/delusions)
Violent environment
🔹 Expected Findings
Pacing, restlessness
Loud/rapid speech
Clenched fists
Intense eye contact
Aggressive posture
Tachypnea
NURSING CARE (AGGRESSION)
De-escalation Key Actions
Respond quickly
Stay calm
Maintain control
Communication
Encourage verbal expression
Use:
Silence
Reflection
Active listening
Environment
Give personal space
Nonthreatening posture
Same eye level
Limit Setting
Clear, direct instructions:
“I need you to stop yelling…”
Offer choices
Explain consequences
Other Strategies
Physical activity (walking)
“Show of force” if needed (staff presence)
🔹 If Escalation Continues
Use medications
Prepare for restraints if necessary
POST-INCIDENT CARE
🔹 Client Debriefing
Discuss:
Triggers
Feelings
Correct misperceptions
Reinforce support
Update care plan
🔹 Staff Debriefing
Evaluate response
Identify improvements
🔹 Documentation
Behavior before/during incident
Interventions used
Client response
Medications (Aggression)
First-Line (Common)
Atypical antipsychotics:
Olanzapine
Ziprasidone
🔹 Other
Haloperidol
Monitor for:
EPS
Neuroleptic malignant syndrome
🔹 Additional Options
SSRIs
Mood stabilizers (Lithium)
Benzodiazepines
family and community violence
Definition
Violence = abuse of power by a stronger person over a weaker person
Can occur:
Partner → partner
Parent → child
Child → parent
Caregiver → vulnerable adult
🔹 Key Concepts
Usually involves control, intimidation, or injury
Victims are often the least powerful
Occurs across:
All cultures
All socioeconomic levels
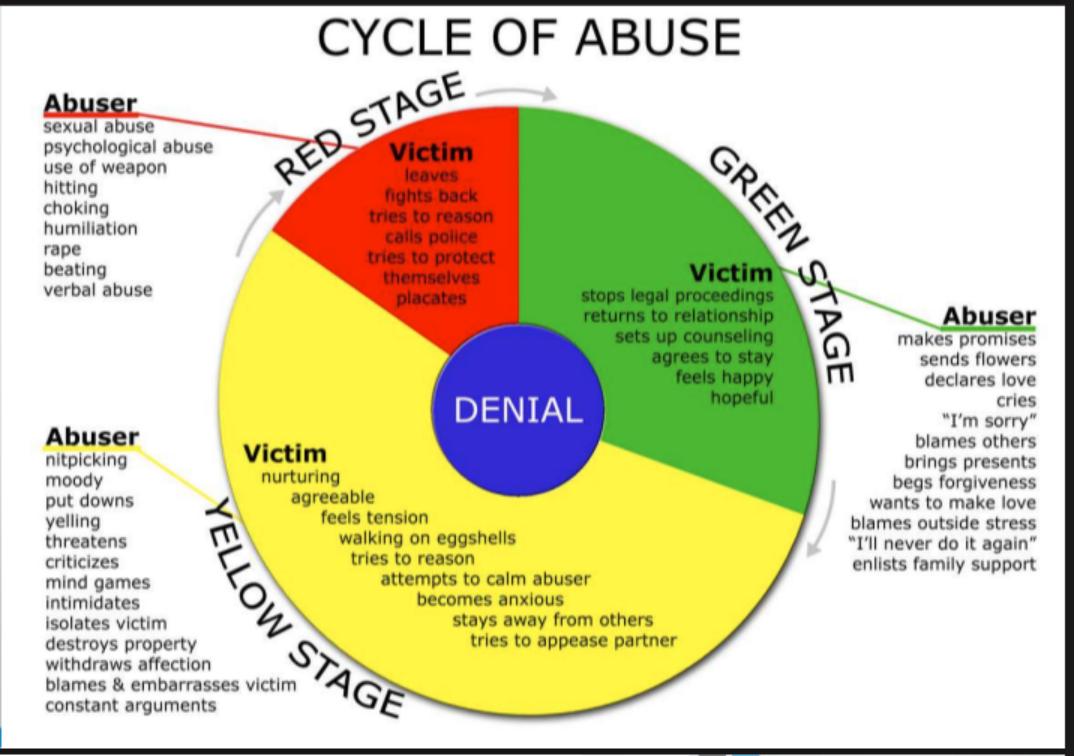
CYCLE OF VIOLENCE
1. Tension-Building Phase
Minor abuse:
Verbal abuse
Pushing/shoving
Victim:
Feels anxious
Accepts blame
Perpetrator:
May use substances
2. Acute Battering Phase
Most violent stage
Severe abuse occurs
Victim:
May try to hide injuries
May seek help
3. Honeymoon Phase
Perpetrator:
Apologizes
Promises change
Victim:
Feels hopeful
Forgives
🔹 Important Pattern
Cycle repeats
Time between episodes shortens
Violence worsens over time
TYPES OF VIOLENCE
Physical
Hitting, kicking, strangling
Shaken baby syndrome
🔹 Sexual
Non-consensual contact
Rape, incest, trafficking
🔹 Emotional
Humiliation
Threats
Intimidation
🔹 Neglect
Failure to provide:
Food
Emotional care
Education
Healthcare
🔹 Economic Abuse
Withholding financial support
Not paying bills despite having money
CHARACTERISTICS
🔹 Vulnerable Person (Victim)
Low self-esteem
Feelings:
Guilt, shame, helplessness
Protects perpetrator
Accepts blame
May deny severity
🔹 Perpetrator
Controlling, intimidating
Poor impulse control
Violent outbursts
Low self-esteem
Substance use history
Often history of being abused
RISK FACTORS (violence)
General
History of violence
Substance use disorder
Poverty
Mental illness + stressors
🔹 High-Risk Situations
Trying to leave relationship
Pregnancy (↑ violence risk)
Prior family violence
🔹 Children at Risk
Age < 4 years
Unwanted child
Disability or “different”
🔹 Older Adults
Dependent on caregiver
Poor health
Cognitive impairment
FAMILY VIOLENCE
Key Points
Most violence occurs within families
More likely toward:
Family members
Friends
NOT strangers
🔹 Important NCLEX Concept
People with mental illness:
More likely to harm themselves than others
ASSESSMENT
🔹 Nursing Approach
Ensure privacy
Be:
Direct
Honest
Nonjudgmental
Use open-ended questions
🔹 Legal/Ethical
Must inform client if reporting is required
🔹 Forensic Nurse Role
Collects evidence in:
Abuse
Sexual assault cases
AGE-SPECIFIC FINDINGS - violence
Infants Shaken Baby Syndrome
Intracranial hemorrhage
Findings:
Respiratory distress
Bulging fontanel
↑ head circumference
Retinal hemorrhage
ANY bruising < 6 months = suspicious
🔹 Children Suspicious Findings
Bruises:
Abdomen, back, buttocks
Burns:
“Glove” or “stocking” pattern
Cigarette burns
Fractures:
Spiral fractures
Multiple fractures
Bite marks
Head injury symptoms
🔹 Older Adults
Injuries inconsistent with explanation
Bruises, fractures, neglect
NURSING CARE- violence
PRIORITY
Mandatory reporting (ALL states)
Failure → legal consequences
🔹 Interventions
Document:
Objective + subjective findings
Treat injuries
Make referrals
🔹 Safety Planning
Identify triggers
Provide:
Safe housing options
Shelters
🔹 Crisis Intervention
Use during:
Family violence
Community trauma
COMMUNITY / MASS VIOLENCE
Examples
School shootings
Natural disasters
Terrorism
🔹 Interventions Early
Ensure safety
Provide psychological first aid
Reduce panic
Ongoing
Restore:
Sleep
Routine
Connect to:
Resources
Support systems
Critical Incident Stress Debriefing (CISD)
Group therapy after trauma
Includes:
Discussion of event
Emotional reactions
Coping strategies
SEXUAL ASSAULT
Definition
Any forced or pressured sexual activity
Includes:
Rape
Incest
Trafficking
Rape
Nonconsensual penetration
Crime of:
Power
Control (NOT passion)
🔹 Types
Stranger
Acquaintance (MOST common)
Date rape
Marital rape
Drug-Facilitated Assault
Substances:
GHB (“liquid ecstasy”)
Flunitrazepam (“roofies”)
Ketamine
RAPE-TRAUMA SYNDROME
Initial Phase Expressed
Crying, anger, hysteria
Controlled
Calm, numb, confused
🔹 Long-Term Effects
Guilt, fear, anxiety
Depression
Flashbacks
Sleep disturbances
PTSD
1 month after trauma
Symptoms:
Flashbacks
Hyperarousal
Avoidance
Acute Stress Disorder
3 days → 1 month post-trauma
Silent Rape Reaction
No disclosure
Signs:
Nightmares
Anxiety
Behavior changes
NURSING CARE (SEXUAL ASSAULT)
PRIORITIES
Ensure safety
Provide nonjudgmental care
Assess for:
Suicide risk
🔹 Key Actions
Obtain informed consent
Use SANE nurse if available
Collect forensic evidence
🔹 Evidence Collection
Blood, swabs, hair, nails
Document:
Injuries (photos/body maps)
Client statements (verbatim)
🔹 Medical Care
Treat injuries
STI prophylaxis
Emergency contraception
🔹 Communication
Encourage expression
Do NOT ask “why”
Reinforce:
“This is NOT your fault”
🔹 Support
Contact support system (with permission)
Provide emotional support
CARE AFTER DISCHARGE
🔹 Interventions
Provide hotline numbers
Written instructions
Schedule follow-up
🔹 Therapy
Individual therapy
Group therapy
🔹 Important
Follow-up compliance is often LOW → emphasize importance
INTERPROFESSIONAL CARE- sexual assault
Includes
Case management
Social services
Legal system
Shelters
🔹 Additional Support
Parenting classes
Stress management
Problem-solving skills
substance use and addictive disorders
Overview
Substance Use Disorders (SUD):
Repeated use of substances → clinically significant impairment (within 12 months)
Substances include:
Alcohol, caffeine, cannabis
Hallucinogens, inhalants
Opioids
Sedatives/hypnotics/anxiolytics
Stimulants, tobacco
Behavioral (Process) Addictions:
Gambling, sex, shopping, social media, gaming
Key Characteristics:
Loss of control
Continued use despite problems
High relapse rate
Defense Mechanism:
Denial (VERY common)
“I can quit anytime”
🔹 Risk Factors
Genetics (family history)
Adolescents (immature judgment)
Chronic stress (low socioeconomic status)
Trauma (abuse, combat)
Low self-esteem
Poor coping skills
Few relationships or achievements
Risk-taking behaviors
🔹 Protective Factors
Strong family/social support
Positive self-esteem
Caregiver involvement
Community resources
Employment
🔹 Cultural Considerations
Higher alcohol use:
Some Native American/Alaska Native groups
Lower alcohol use:
Some Asian populations
Influenced by:
Alcohol metabolism
Cultural beliefs
Peer pressure
🔹 Assessment (Nursing History)
Use open-ended questions about:
Substance type
Frequency & pattern
Amount used
Age of first use
Work/school changes
Periods of abstinence
Withdrawal history
Last use
Review of Systems
Blackouts
Sleep issues
Weight changes
GI changes
Chronic pain
Stress
Desire to cut down
🔹 Special Populations Young Adults (18–25)
Highest use rates
Early use → ↑ risk of disorder
Pregnancy
Risks:
Prematurity
Low birth weight
Neonatal abstinence syndrome
Healthcare Workers
Risk due to:
Stress + access to drugs
Warning signs:
Overtime volunteering
Mood swings
Poor performance
Lying
Older Adults
↑ sensitivity to substances
Risks:
Falls
Confusion
Memory loss
Alcohol signs:
Incontinence
↓ self-care
Dementia-like symptoms
Polypharmacy ↑ adverse effects
🔹 Screening Tools
MAST – Alcohol
DAST / DAST-A – Drugs
CAGE – Alcohol perception
AUDIT
CIWA-Ar – Alcohol withdrawal
COWS – Opioid withdrawal
SBIRT – Early intervention
Substance Categories
Opioids (Heroin, Morphine) Effects
Euphoria, pain relief
Intoxication
↓ respirations ⚠ (can cause death)
Slurred speech
↓ LOC
Antidote
Naloxone
Withdrawal
NOT life-threatening
Flu-like symptoms:
Sweating, diarrhea, pain, insomnia
🔹 CNS Depressants Alcohol Intoxication
Slurred speech
↓ motor skills
Respiratory depression ⚠
Chronic:
Liver disease, pancreatitis
Withdrawal ⚠
Tremors, HTN, tachycardia
Seizures
🚨 Alcohol Withdrawal Delirium (Delirium Tremens)
2–3 days after stopping
MEDICAL EMERGENCY
Hallucinations
Severe HTN
Dysrhythmias
Death risk
Benzodiazepines / Barbiturates Intoxication
Sedation
Respiratory depression ⚠
Antidote
Flumazenil (benzos only)
Withdrawal ⚠
Seizures possible
🔹 Cannabis
Effects:
Euphoria, increased appetite
Risks:
Impaired motor skills (8–12 hrs)
Paranoia (high doses)
Withdrawal
Irritability, insomnia, anxiety
🔹 Stimulants Cocaine Intoxication ⚠
HTN, tachycardia
Chest pain
Seizures
Death
Withdrawal
Depression
Fatigue
Suicidal risk
Amphetamines
Similar to cocaine
Withdrawal
Depression, fatigue (NOT life-threatening)
🔹 Hallucinogens (LSD, PCP)
Effects:
Altered perception
Risks:
Panic, paranoia
Long-term
Flashbacks (HPPD)
🔹 Inhalants
Used by children/adolescents
Effects:
Dizziness, confusion
Respiratory depression ⚠
🔹 Caffeine
Intoxication (>250 mg):
Tachycardia, anxiety, insomnia
Withdrawal:
Headache, fatigue
🔹 Nicotine Effects
Relaxation
Long-term
Cardiovascular disease
Lung cancer
Withdrawal
Irritability
Cravings
Increased appetite
Nursing Care- substance use
Priority = SAFETY
Prevent injury
Seizure precautions
Monitor closely
🔹 Interventions
Low-stimulation environment
Frequent orientation
Monitor:
VS
Neuro status
Maintain:
Nutrition
Hydration
Administer meds for:
Withdrawal
Detox
Watch for covert use
🔹 Psychosocial Care
Nonjudgmental approach
Emotional support
Educate family (codependency)
🔹 Promote Recovery
Encourage:
Accountability
Coping skills
Emergency relapse plan
Refer to 12-step programs:
AA, NA, Al-Anon
Interprofessional Care
🔹 Therapies
CBT → change thinking/behavior
ACT → acceptance + commitment
Relapse prevention
Group therapy
Family therapy
🔹 Codependency
Family enables behavior
Example: covering up for client
Medications- substance use tx
Alcohol Withdrawal
Benzodiazepines (FIRST LINE)
Diazepam, Lorazepam
Prevent seizures
🔹 Alcohol Abstinence
Disulfiram
Causes severe reaction with alcohol ⚠
Naltrexone
↓ cravings
Acamprosate
↓ withdrawal discomfort
🔹 Opioid Use Disorder
Methadone
Replacement therapy
Buprenorphine
↓ cravings
Clonidine
↓ withdrawal symptoms
🔹 Nicotine Cessation
Bupropion
Nicotine replacement:
Gum, patch, spray, lozenge
Varenicline
↓ cravings
⚠ watch for suicidal thoughts
🔹 Antidotes
Naloxone → opioids
Flumazenil → benzodiazepines
Important Definitions
Tolerance: need more for same effect
Withdrawal: symptoms when stopping
Abstinence syndrome: severe withdrawal
Treatment Goals
Primary goal = Abstinence
Long-term recovery:
Behavior change
Coping strategies
Support systems
opioids
How Opioids Work: Opioids are prescribed for severe pain. They work by attaching to specific structures called opioid receptors located throughout the brain, spinal cord, and other body parts to dampen pain signals.
Other Effects: Beyond pain relief, these drugs impact the brain's reward pathway by triggering the release of dopamine, which creates feelings of euphoria or a "high." They can also physically affect the body by slowing down breathing and reducing intestinal movement, which commonly leads to constipation.
The Risks of Misuse: When taken as prescribed for short periods, these drugs are generally safe. However, using them in ways not intended—such as taking higher doses, using them recreationally, or sharing them—significantly increases the risk of serious health issues.
Tolerance, Dependence, and Addiction:
Tolerance: The body becomes less sensitive to the drug over time, requiring higher doses to achieve the same pain relief.
Dependence: The body adapts to the drug, leading to physical withdrawal symptoms when use is stopped.
Addiction: A chronic brain disease characterized by overwhelming cravings and the inability to stop using the substance despite harmful consequences.
Overdose: An overdose occurs when too much of the drug is consumed, potentially leading to confusion, unconsciousness, severe respiratory depression, and death.
Seeking Help: The video emphasizes that addiction is a serious condition and encourages anyone struggling with opioid use or those seeking information to consult their healthcare provider for professional support.
opioids and withdrawal
Why people use opioids: Opioids are powerful medications often prescribed for pain or used illegally (e.g., heroin). Beyond blocking physical pain, they produce a "rush" of pleasant feelings, which can lead to patterns of continued use.
What is withdrawal: It is the body's reaction to the absence of a substance it has become accustomed to over time. As a person uses more of the drug to achieve the same effect, the body's reaction to stopping the drug becomes more severe.
The physical sensation: While opioid withdrawal is not life-threatening, it is described as being extremely difficult to tolerate. Symptoms are often compared to a severe case of the flu and are essentially the opposite of the relaxed, pain-free state opioids provide.
Common symptoms include:
Agitation, anxiety, and being short-tempered.
Disrupted sleep patterns.
Physical discomfort, including sweating, trembling, goosebumps, and muscle aches.
The return of original pain, often felt more intensely than before.
Digestive issues like nausea, vomiting, or diarrhea.
The cycle of dependence: Because the withdrawal process is so painful, individuals may begin taking the opioid again simply to stop the symptoms, which often leads to a cycle of misuse and potentially opioid use disorder.
A path forward: The video emphasizes that recovery is possible. If someone is struggling with opioid use or withdrawal, they are encouraged to talk to a healthcare provider. Effective treatment programs exist to help manage withdrawal symptoms safely and support individuals in reducing or stopping their use of opioids.
Addiction and the brain
Addiction works in the brain's reward system
The brain relies on the substance to feel normal which makes stopping difficult
The main neurotransmitter is dopamine
What is Substance Use Disorder
Substance use disorder is a pattern of substance use that causes problems or distress
Substance use disorder affects health relationships work or school safety daily functioning
It can involve substances such as alcohol prescription medications illegal drugs nicotine or tobacco
Substance addictions
Affect the brain and body in different ways
But they all impact safety judgment health and daily functioning
other addictions
There are many other addictions
Look at compulsive behaviors
Why this matters in nursing - addiction
Nurses care for clients with substance use disorder in many settings
Emergency Department medical surgical units behavioral health community and outpatient settings long term care maternal newborn care
The substance may be a part of the bigger picture
Substance use can affect safety judgment physical health mental health and treatment outcomes
Intoxication
Immediate effects of substance on brain and body
“under the influence”
Substance abuse
Over using
Tolerance
Takes more to feel the effects
Dependence
Body gets used to it
The five C's of addiction
Craving compulsion loss of control consequence coping
Withdrawl
How the body reacts when the substance is gone
Substance abuse is a complex health disorder
Can be impacted by genetics mental health trauma environment stress and early exposure
Risk factors of substance abuse
Risk factors don't guarantee addiction
Family history of addiction
Mental health disorders
Trauma or abuse
Peer pressure
early substance exposure
Poor support system
Stress poverty or unstable environment
Protective factors of substance abuse
Protective factors don't guarantee prevention
Supportive family or relationships
Positive coping skills
School or work success
Community support
Healthy self image
Access to resources and treatment
Warning signs and early clues for substance abuse
Frequent falls
Repeated ER visits
Poor medication compliance
Homelessness and instability
Anxiety irritability
Malnutrition
Mood or behavior changes
Decline in school or work performance
Poor hygiene or self care
Sleep or appetite changes
Weight changes
Tremors shakiness or sweating
Frequent injuries or accidents
missing appointments or poor follow through
Relationship legal or financial problems
Drug seeking behaviors
Nursing assessment substance abuse
Substance history
What's used how much and how often
Mood
Withdrawal symptoms
vital signs and level of consciousness
nutrition
Support systems
Safety
Falls injury suicidal self harm violent situation
make sure you know what they use when they last used if they're intoxicated or withdrawing if they're medically unstable or if they're safe
Therapeutic communication substance abuse
nursing approach
Be nonjudgmental
Use a calm respectful tone
Promote privacy and dignity
Ask open ended questions
use empathy
Explain what you are doing and why
Focus on safety and support not shame
“tell me more”
“ I'm here to keep you safe”
Alcohol use disorder
Can affect the brain liver GI system heart nutrition and safety
Will develop tolerance and dependence
withdrawal can become life threatening
s/s: Strong cravings for alcohol, Drinking despite harm to relationships, spending excessive time drinking, continuing despite worsening health, drinking in dangerous situations, failing responsibilities due to drinking, unsuccessful attempts to cut down, drinking more or longer than intended
CIWA
Measure acute alcohol withdrawal symptoms
at 48-72 hrs after alcohol withdrawal what s/s appears
Alcohol withdrawal delirium or delirium tremens
delirium tremens
Tremors shakiness anxiety irritability nausea and vomiting headache tachycardia hypertension confusion and seizures
delirium tremens: Life threatening emergency that requires immediate treatment and close monitoring
Monitor airway seizure precautions close vital signs monitoring medication support reduced stimulation keep room dark and quiet and safety precautions
disulfiram
for AUD
Inhibits alcohol metabolism
Can cause an alcohol reaction if drinking alcohol while on it
Can cause nausea vomiting flushing tachycardia and intense feeling of unwell
used to deter
Appropriate only if goal is abstinence of alcohol
Opioids and overdose
Heroin oxycodone morphine fentanyl and methadone
s/s: Drowsiness slowed breathing constricted pupils decreased level of consciousness
red flags: Unresponsiveness pinpoint pupils blue Gray skin or lips low heart rate or bradycardia and respiratory depression
worried about them stopping breathing
Opioid overdose emergency care
Maintain airway
support breathing
administer oxygen
Monitor vital signs
Prepare or administer naloxone or Narcan as prescribed
ensure patient safety
Monitor for return of respiratory depression
Might have to give Narcan again
stimulants sedatives and Co occurring disorders
stimulants
Cocaine methamphetamine
Agitation restlessness Tachycardia hyperactivity unable to sleep
sedatives
Benzodiazepines
Drowsiness slurred speech poor coordination
co-occurring disorders
Depression anxiety bipolar disorder or suicidal thoughts with alcohol use or substance abuse
lab tests for substance abuse or AUD
Blood alcohol level
Urine drug screen
Liver function tests (ALT, AST, bilirubin)
See how alcohol is damaging the liver
CBC
electrolytes
alcohol affects electrolytes
glucose
magnesium
kidney function
Organ damage dehydration malnutrition
Nursing interventions for AUD and substance abuse
airway breathing circulation
Frequent vital signs
Neuro and mental status monitoring
Monitor for withdrawal symptoms
Hydration and nutrition
Medication administration
Calm low stimulation environment
Reorientation as needed
Assist with self care and ambulation
Promote rest and sleep
Nursing safety precautions for AUD and substance abuse
Fall precautions
Seizure precautions
Frequent observation (1:1)
Safe environment
Patient education recovery and support for AUD and substance abuse
Effects of substance use on the body
Withdraw and relapse warning signs
Medication teaching
The importance of follow up care
support groups and treatment options
Healthy coping strategies
Sleep nutrition and hydration
Avoiding triggers when possible
Across the lifespan for AUD and substance abuse
pregnancy, neonates, children
harm fetal growth and development and lead to complications
Fetal alcohol spectrum disorders and neonatal abstinence syndrome
adolescents
Effects growth behavior learning development in adolescence
Developing brain especially vulnerable to poor decision making risk taking and long term addiction
older adults
Harder to recognize
Increased risk for falls and confusion
Polypharmacy
Adverse Childhood Experiences (ACEs)
The video tells the life story of a child growing up in a home filled with violence, neglect, substance misuse, and emotional instability. It uses the child’s perspective to show how Adverse Childhood Experiences (ACEs) shape development, health, behavior, and future relationships.
Early Childhood: Fear, Instability, and Emotional Harm
The narrator begins as a young child who feels constantly frightened by parental fighting, shouting, and physical abuse. They long for basic affection—a cuddle, a bedtime story—but instead experience rejection and fear. This chronic emotional insecurity becomes the foundation for lifelong consequences.
The child witnesses domestic violence, sees a parent struggling with alcohol misuse, and watches the other parent cry despite taking medication. There is little money for food, clothing, or toys. The child becomes accustomed to fear, which gradually transforms into anger.
Biological and Developmental Impact
Doctors in the video explain that these experiences are ACEs—traumatic events that alter the developing brain and stress-response system. Because of constant stress, the child’s brain does not learn to regulate emotions effectively. Their body remains in a heightened state of alert, making it harder to relax or heal. Over time, this increases the risk of chronic diseases such as cancer, heart disease, and diabetes.
The video emphasizes that while physical abuse hurts, the deeper and more lasting damage is internal and invisible—changes in brain wiring, stress hormones, and emotional regulation.
Adolescence: Coping Through Risk and Aggression
As the child grows into adolescence, they turn to smoking, drinking, and fighting as coping mechanisms. They describe these behaviors as attempts to manage overwhelming emotions shaped by their ACEs. Violence feels normal because it mirrors home life.
School becomes a place of conflict rather than learning. The narrator gets into fights, skips classes, and feels disconnected from teachers who seem indifferent. They also become a parent at a young age, repeating the pattern of early pregnancy seen in their own family.
Adulthood Without Intervention: The Cycle Continues
In adulthood, the narrator faces significant health problems—diabetes and the expectation of future cancer. They have never held stable employment and have spent time incarcerated. Their relationships are strained, and they acknowledge hating their partner and even their children. Some of their children grow up with ACEs as well, continuing the intergenerational cycle.
The narrator recognizes that their life trajectory was set early and that their children are likely headed down the same path.
A Second Possible Path: Early Support and Intervention
The video then rewinds to show how the narrator’s life could have unfolded differently with early support.
As a baby, nurses notice the mother is struggling and offer help, explaining how important early childhood experiences are. When neighbors report domestic violence, police check on the child and ask how they feel. The parents receive support, the fighting decreases, and the hitting stops. The child finally receives affection and bedtime stories.
At school, a teacher notices emotional and behavioral struggles and connects the child with help to manage feelings. These small but meaningful interventions change the child’s developmental path.
Adulthood With Support: Breaking the Cycle
In this alternate future, the narrator becomes an adult who is married, employed most of the time, and raising children without repeating the harmful patterns they experienced. Their children grow up ACE‑free, giving the next generation a strong chance of remaining ACE‑free as well.
Public Health Message: ACEs Are Common and Preventable
The video concludes with key statistics:
Nearly half of people in England and Wales experienced at least one ACE.
One in ten experienced four or more.
Reducing ACEs would dramatically lower rates of smoking, binge drinking, violence, and chronic disease. The narrator calls on doctors, nurses, teachers, police, firefighters, and especially parents to become ACE‑aware. Understanding ACEs helps prevent them and supports those who have already experienced them.
Adverse Childhood Experiences (ACEs): Impact on brain, body and behaviour
The video explains how a child’s earliest experiences shape the developing brain and influence lifelong health, behavior, and learning. It begins by establishing that genes provide the blueprint for brain development, but environmental experiences determine how that blueprint is expressed. Neural connections that are used frequently become stronger and more permanent, while those that are rarely used fade away. This interplay between nature and nurture forms the foundation for all future development.
Healthy vs. Harmful Early Experiences
The video distinguishes between different types of stress:
Positive stress: everyday challenges like meeting new people or starting daycare. These experiences help children build coping skills and resilience.
Tolerable stress: more serious events that can be buffered by supportive caregivers.
Toxic stress: frequent, chronic, or intense stress without caregiver support.
Adverse Childhood Experiences (ACEs)—such as abuse, neglect, exposure to domestic violence, parental mental illness or addiction, and poverty—fall into the toxic category. These experiences can lead to long‑lasting changes in learning, behavior, and health.
How Toxic Stress Affects the Body
The stress-response system is designed to activate during danger: heart rate rises, cortisol and adrenaline surge, and the body prepares for fight or flight. Normally, this system shuts off once the threat passes or when a caregiver provides comfort.
With ACEs, the stress system stays activated for long periods. Without supportive adults to help regulate emotions, the child’s body struggles to return to baseline. This prolonged activation:
Weakens the immune system
Increases vulnerability to infection and chronic disease
Disrupts normal brain development
Impact on Key Brain Regions
The video highlights three brain areas that are especially vulnerable to toxic stress:
Executive Function Center Responsible for planning, attention, problem‑solving, impulse control, and learning. Toxic stress disrupts its development, making it harder for children to focus, reason, and regulate behavior.
Emotional Center (the brain’s alarm system) Handles emotional processing and impulse control. Chronic stress makes this system overreactive, leading to emotional distress, heightened reactivity, and difficulty managing impulses.
Memory and Learning Center Supports memory formation and retrieval. Toxic stress interferes with learning and the ability to store and recall information.
As a result, children exposed to ACEs often show emotional dysregulation, impulsivity, learning difficulties, and increased risk for mental and physical health problems.
Epigenetics: How Experience Changes Gene Expression
The video explains that ACEs can influence gene expression through epigenetic mechanisms. Epigenetics does not change DNA itself but alters how genes function through chemical modifications.
The metaphor used is:
Genes = hardware
Epigenetics = operating system
Experiences such as stress, relationships, nutrition, and smoking can modify how genes are expressed. ACEs are associated with epigenetic changes affecting:
Stress response
Brain development
Cognition
Mental and physical health systems
Changes that occur early in development are more likely to be long‑lasting and may even be passed to future generations.
The Good News: Support Can Change Trajectories
Despite the risks, the video emphasizes that positive, supportive relationships at any stage of life can improve outcomes. Early intervention is especially powerful.
Warm, responsive caregiving—known as serve and return interaction—is highlighted as a key protective factor. This includes:
Eye contact
Responding to sounds, gestures, and emotions
Shared activities like reading and play
Programs that help caregivers strengthen these skills can prevent many negative outcomes associated with ACEs and build strong foundations for healthy development.
Protecting Our Elders: How to Spot and Stop Abuse
The video provides a clear, structured overview of elder abuse, emphasizing that it is a growing and often hidden problem affecting older adults across many settings. It defines elder abuse as any intentional harm, mistreatment, or neglect directed toward an elderly person, and stresses that it can take multiple forms—each with distinct warning signs and consequences.
Forms of Elder Abuse
The video outlines four major categories:
1. Physical Abuse
This includes any use of physical force—hitting, pushing, slapping, or improperly restraining an older adult. It also includes misuse of medications. Common indicators include unexplained bruises, cuts, fractures, or injuries inconsistent with the explanation given. Signs of neglect, such as dehydration or malnutrition, may also accompany physical abuse.
2. Emotional or Psychological Abuse
Emotional abuse involves behaviors intended to intimidate, control, or degrade an older adult. This may include threats, humiliation, manipulation, or isolation. Warning signs include depression, anxiety, withdrawal from social activities, sudden behavior changes, sleep disturbances, appetite changes, or difficulty concentrating.
3. Sexual Abuse
Sexual abuse includes any non‑consensual sexual contact, inappropriate touching, coercion, or forcing an older adult to engage in sexual acts. Signs may include genital injuries, bleeding, sexually transmitted infections, or abrupt personality changes such as increased aggression or agitation.
4. Financial Abuse
Financial exploitation involves the unauthorized or illegal use of an older adult’s money, property, or assets. Red flags include sudden changes in bank accounts, unexplained withdrawals, transfers to unfamiliar individuals, missing belongings, or unexpected changes to wills, powers of attorney, or financial documents.
👥 Who Is Most at Risk?
While anyone can experience elder abuse, the video highlights several factors that increase vulnerability:
Social isolation
Cognitive impairment, such as dementia
Physical dependence on others for daily care
Living in long‑term care facilities
Living with family members who misuse drugs or alcohol
These conditions can reduce an elder’s ability to recognize abuse, report it, or escape harmful situations.
🧭 Preventing Elder Abuse
The video emphasizes that preventing elder abuse requires community awareness and proactive involvement. Key strategies include:
1. Educate Yourself
Understanding the types of abuse and their warning signs is the first step in recognizing when something is wrong.
2. Build Relationships and Reduce Isolation
Regularly checking in on older family members, neighbors, and friends helps build trust and reduces the isolation that often enables abuse.
3. Speak Up and Report Concerns
If abuse is suspected, the video urges immediate reporting to appropriate authorities such as local law enforcement or Adult Protective Services.
4. Support Independence
Encouraging older adults to stay active and engaged helps maintain their autonomy and reduces vulnerability.
5. Ensure Caregivers Are Qualified and Respectful
Whether care is provided by professionals or family members, caregivers should be properly trained and committed to treating older adults with dignity.
🧩 Final Message
The video concludes by stressing that preventing elder abuse is a shared responsibility. Families, communities, professionals, and government agencies must work together to create safe, supportive environments for older adults. Through awareness, vigilance, and compassionate action, elder abuse can be identified early—or prevented altogether.
Child Abuse: Skeletal and Cutaneous Findings
The video provides a comprehensive overview of skeletal and cutaneous (skin) manifestations of physical child abuse, focusing on how to recognize, evaluate, and differentiate abusive injuries from medical conditions that may mimic them. It is designed to equip pediatric healthcare providers with the knowledge needed to identify red flags, conduct appropriate diagnostic workups, and fulfill their responsibilities as mandated reporters.
📊 Epidemiology and Scope
Child maltreatment is a widespread issue in the United States, with 4 million referrals annually. The highest rates occur in children under one year old, and nearly five children die every day from abuse. Among all forms of maltreatment:
75% are cases of neglect
17% involve physical abuse
8% involve sexual abuse
This video focuses specifically on physical abuse, particularly fractures and skin injuries, which are among the most common clinical presentations.
⚠ Risk Factors for Abuse
Risk factors fall into three categories:
Child-related factors
Prematurity
Chronic illness
Developmental or physical disabilities
Behavioral or emotional challenges
Caregiver-related factors
Young parental age
Substance or alcohol misuse
Mental illness
Unrealistic expectations of child behavior
Environmental factors
Poverty
Unemployment
Low educational attainment
Social isolation
Single parenthood
Presence of an unrelated adult male in the home
History of intimate partner violence
The video emphasizes that child abuse crosses all socioeconomic, racial, cultural, and religious groups—no child is immune.
🩺 Clinical Red Flags
The most important indicator of possible abuse is a history that does not match the injury. Providers must assess whether the explanation is consistent, developmentally plausible, and appropriate for the child’s abilities.
Other red flags include:
Delayed medical care
Multiple injuries in different stages of healing
Escalating severity of events
Inappropriate caregiver affect
Recent stressors or triggering events
In infants and toddlers, up to 20% of fractures are caused by abuse.
🦴 Skeletal Findings Common but nonspecific fractures
Long bone fractures
May occur accidentally or abusively
Fracture pattern helps determine mechanism
Transverse: direct blow
Buckle: axial compression
Spiral: twisting force
Highly specific fractures for abuse
Especially concerning in children under one year:
Classic metaphyseal lesions (CMLs)
Also called bucket handle or chip fractures
Caused by twisting/pulling forces
Posterior rib fractures
Often from forceful squeezing of an infant’s chest
These injuries require significant force and are rarely accidental.
🩹 Cutaneous (Skin) Findings
90% of physically abused children present with skin findings, and sometimes a single bruise is the only sign.
Concerning bruise patterns
Bruises in protected areas: torso, ears, neck, genitals, buttocks
Bruises in non‑ambulatory infants (“those who don’t cruise rarely bruise”)
Patterned injuries suggesting an implement:
Handprints
Bite marks
Loop marks from cords or belts
The video stresses that you cannot accurately date a bruise based on color.
Burns
Accidental burns: irregular, asymmetric
Intentional immersion burns: symmetric, sharply demarcated, uniform depth
Often involve lower limbs, perineum, or “glove and stocking” distribution
Thermal burns may mirror the object used (e.g., cigarette, iron)
🔍 Diagnostic Workup
A thorough evaluation must distinguish accidental injuries, abusive injuries, and medical mimics.
Conditions that mimic abuse
Rickets
Frayed metaphyses, osteopenia, bowed legs
Osteogenesis imperfecta
Blue sclera, Wormian bones, family history
Bleeding disorders
Easy bruising, abnormal bleeding history, family history
Laboratory evaluation
Bone health labs: calcium, phosphorus, alkaline phosphatase, vitamin D, PTH
CBC, platelets, coagulation studies
Von Willebrand testing
Factor VIII and IX levels
Imaging
Skeletal survey for all children under two with suspected abuse
~21 radiographs covering long bones, skull, spine, ribs, pelvis, hands, feet
High sensitivity with low radiation exposure
🛡 Management and Reporting
The first priority is medical stabilization. Next steps include:
Notifying the hospital’s child protection team
Reporting to Child Protective Services (mandated in all states)
Contacting law enforcement when required
Conducting a social evaluation
Evaluating siblings for possible abuse
Referring families for support with substance use or intimate partner violence
Medical students are also mandated reporters.
🌱 Prevention and Long‑Term Impact
Pediatricians play a crucial role in:
Recognizing early “sentinel injuries”
Providing anticipatory guidance during developmental stress points (e.g., toilet training)
Building long-term supportive relationships with families
Advocating for evidence‑based prevention programs
The consequences of physical abuse extend far beyond immediate injuries. Survivors have higher rates of:
Depression
Conduct disorders
Substance abuse
One study found 80% of abused 21‑year‑olds met criteria for at least one psychological disorder. Nearly one-third of abused children later abuse their own children, perpetuating the cycle.
what is trauma
Trauma is a deeply distressing or disturbing experience that overwhelms a person's ability to cope
Trauma can affect physical health mental health emotional regulation relationships and the sense of safety and trust
types of trauma
acute trauma: A one time event like an assault rape accident or disaster
chronic trauma: Repeated or ongoing trauma like an abuse neglect or domestic violence
complex trauma: Multiple or prolonged traumatic experiences often beginning in childhood
Common trauma responses
emotional/psychological: Fear anxiety depression shame guilt hypervigilance
physical/behavioral: Sleep issues chronic pain self harm substance use dissociation withdrawal
What is interpersonal violence
Intentional use of power control intimidation or force against another person
May include physical abuse emotional or verbal abuse sexual abuse financial abuse neglect or abandonment and stalking or intimidation
Types of interpersonal abuse
Physical abuse: Hitting slapping kicking choking burning
Emotional/psychological abuse: Threats humiliation control intimidation isolation
Sexual abuse: Unwanted or forced sexual activity
financial abuse: Controlling money stealing restricting access to funds
neglect/ abandonment: Failure to provide basic care safety or supervision
Who is at higher risk for interpersonal abuse
Children, older adults, pregnant individuals, people with disabilities, individuals with mental illness or substance use disorders, people who are socially isolated or financially dependent, LGBTQ plus individuals, Individuals with a history of trauma
Common characteristics of an abuser
Need for power and control, manipulation, jealousy or possessiveness, isolation of the victim, blaming others and the person being abused or minimizing abuse, lack of remorse, threats or intimidation, history of violence, substance misuse or poor impulse control
cycles of abuse
Why victims may not leave abusive situations
Fear of retaliation or death, financial dependence, children or custody concerns, emotional attachment or hope for change, shame or embarrassment, isolation from support systems, housing or transportation insecurity, trauma bonding
Domestic violence/intimate partner violence
May include physical violence sexual violence psychological abuse stalking reproductive coercion and financial control
Can occur in dating relationships marriage former partner relationships and all genders or relationship types
Indicators of neglect
Poor hygiene or dirty clothing
malnutrition or dehydration
untreated injuries or medical problems
frequent absences from school or appointments
inadequate supervision
unsafe living environment
developmental delays
pressure injuries or poor skin care
lack of needed medications or equipment
Indicators of sexual abuse
physical: Bruising bleeding pain or injury to genital or anal areas, torn or bloody underclothing, recurrent STIs, pregnancy in a child or adolescent
behavior: Fearfulness, withdrawal, sexualized behavior, regression, self harm, avoidance
Survivor presentation
A survivor may
minimize or deny abuse
appear fearful or withdrawn
avoid eye contact
be anxious or hypervigilant
have low self-esteem shame guilt PTSD depression or substance use
return to the abusive relationship
incest
Sexual abuse involving a family member or close relative
Especially traumatic because it involves violation of trust and safety, secrecy and fear, possibly a long duration, guilt confusion and loyalty conflict
possible effects of incest
Anxiety or depression, PTSD symptoms, self-harm, shame or secrecy, difficulty trusting others, sexual boundary issues, dissociation, eating disorders or substance use, relationship difficulties
Sexual assault
Any unwanted sexual contact or behavior without consent
Includes forced sexual contact attempted rape coercion drug facilitated assault assault by known or unknown individuals
Nursing priorities after sexual assault
Ensure immediate safety
Provide privacy and emotional support
Believe the survivor
Assess injuries
Explain options clearly
Preserve evidence if appropriate
Offer STI and pregnancy prevention resources
Refer to forensic services available
Sex trafficking
Use of force fraud or coercion to exploit a person for commercial sex acts
Victims may include children and adolescents runaway or homeless youth people with trauma histories individuals with substance use disorders people who are isolated or dependent on others
Red flags for sex trafficking
Accompanied by controlling person
cannot speak freely
no control of ID money or phone
frequent STIS or pregnancies
tattoos or branding
malnutrition injuries or exhaustion
fearful submissive or coerced answers
inconsistent story
multiple hotel and address changes
ACEs (Adverse childhood experiences)
Potentially traumatic events that happened before age 18
Examples include physical emotional or sexual abuse neglect witnessing domestic violence household substance use or mental illness parent separation or incarceration
ACE scoring
each yes = 1 point → Higher the score equals higher long term health and psychosocial risk
0 = no reported ACE
1-3 = some increased risk
4 or more = Significantly increased risk
ACE score is not a diagnosis it is a risk indicator
Nursing assessment
Assess privately
Look for injuries in different stages of healing
Observe for fear withdraw poor eye contact or hypervigilance
Notice if another person answers for the patient
Ask direct calm non judgmental questions
Consider patterns not just one isolated finding
What to ask and what to avoid
helpful
Do you feel safe at home
Has anyone hurt threatened or controlled you
Has anyone made you feel afraid
avoid
Why didn't you leave
Are you sure
Asking in front of the suspected abuser
Making promises you cannot keep
Mandatory reporting
Nurses are mandatory reporters for suspected abuse involving children older adults and vulnerable/dependent adults
Follow state law and facility policy, report suspicion not proof, Document objectively, and Prioritize safety