Liver & Renal Disease (Patterns of Abnormal Results, Signs of Deterioration & Affect of Impairment on Drug Choice)
1/28
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
29 Terms
Haemoglobin Reference Range (Men & Women)
Man = 130-170g/L
Woman = 120-150g/L
What is the most liver specific enzyme?
ALT (Alanine Aminotransferase)
Decompensated Liver Disease
Refers to a stage of chronic liver failure where the liver can no longer perform its normal functions leading to key clinical symptoms.
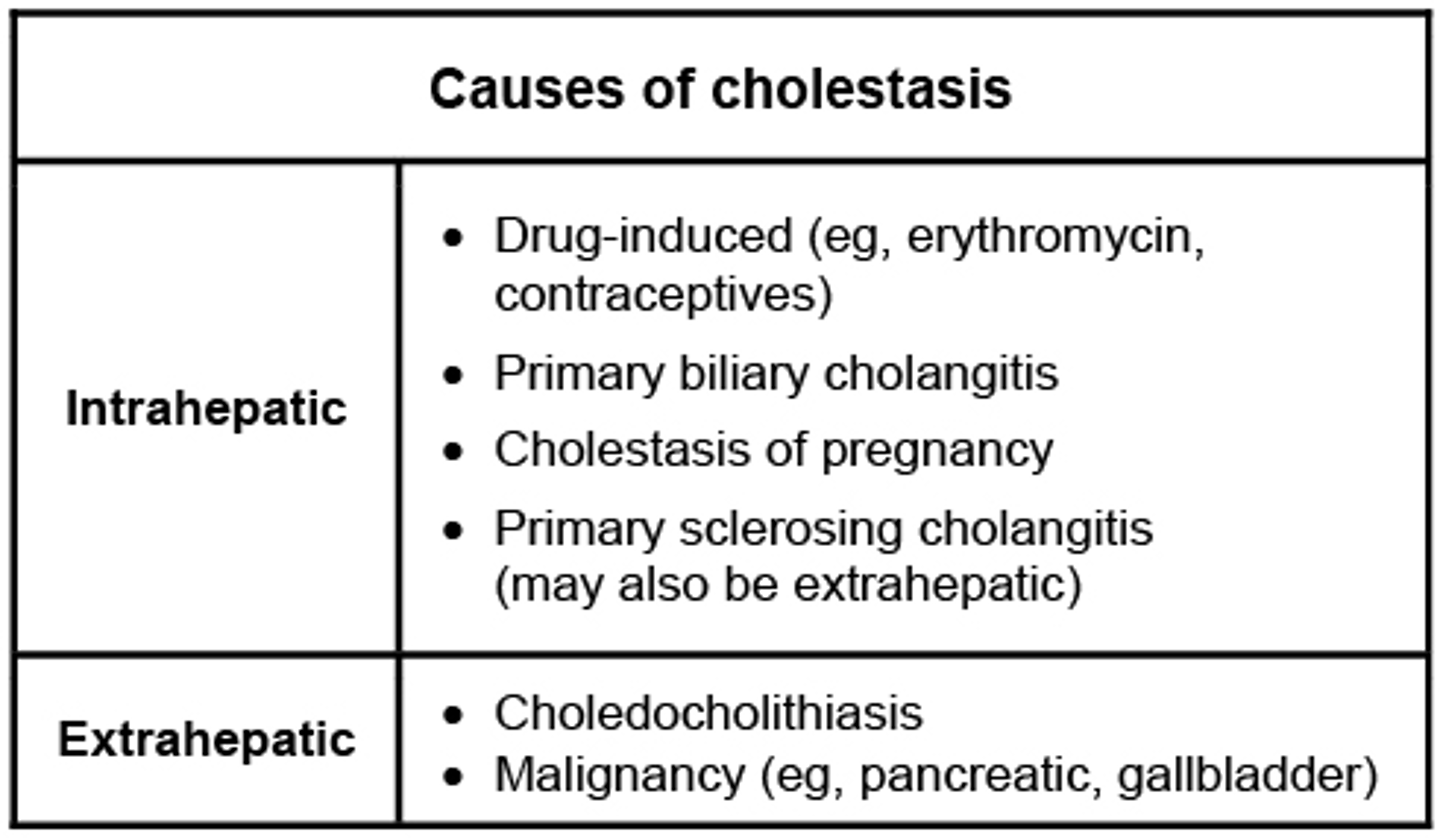
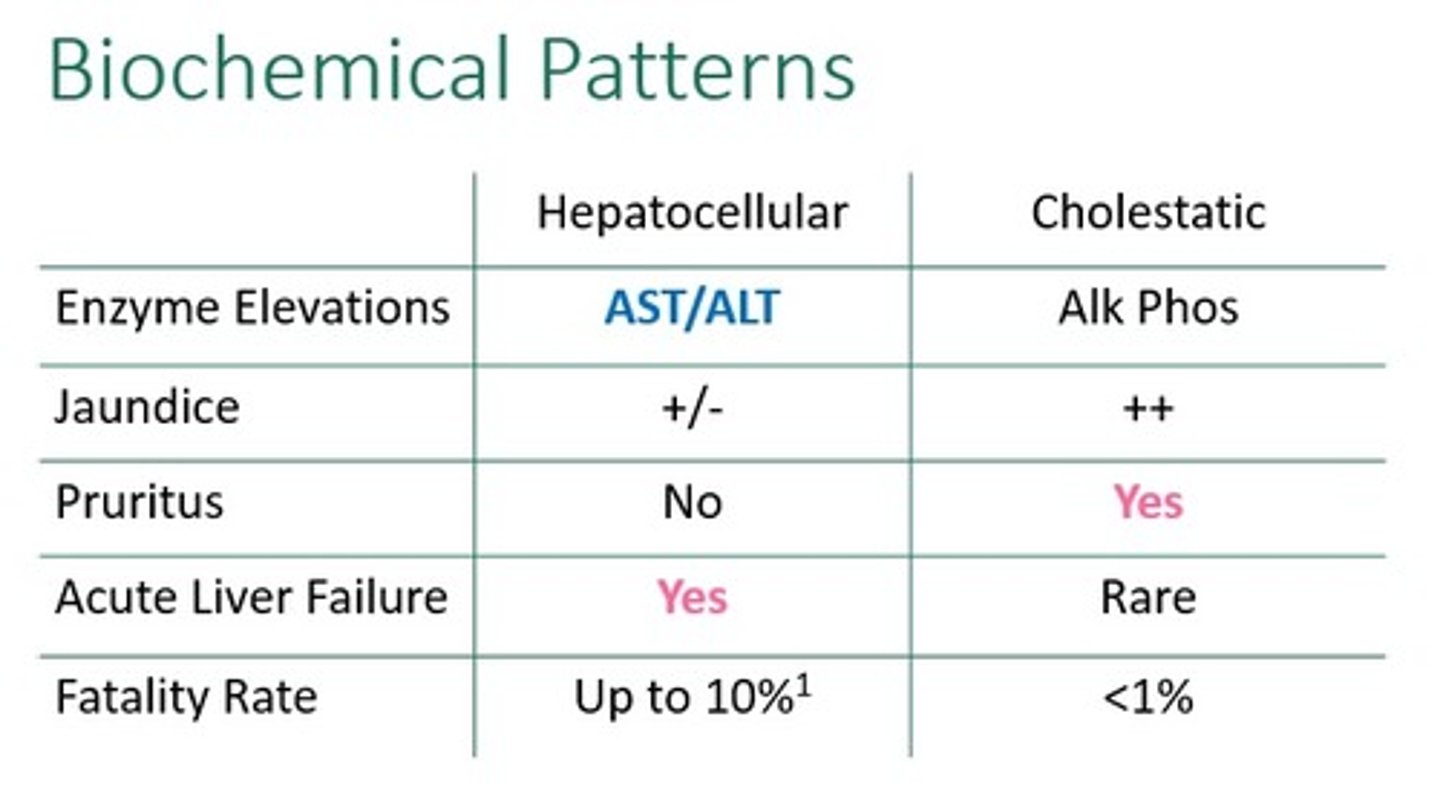
Cholestasis
Refers to a condition where bile formation/bile flow from the liver to the small intestine is impaired, leading to bile accumulation in the liver.
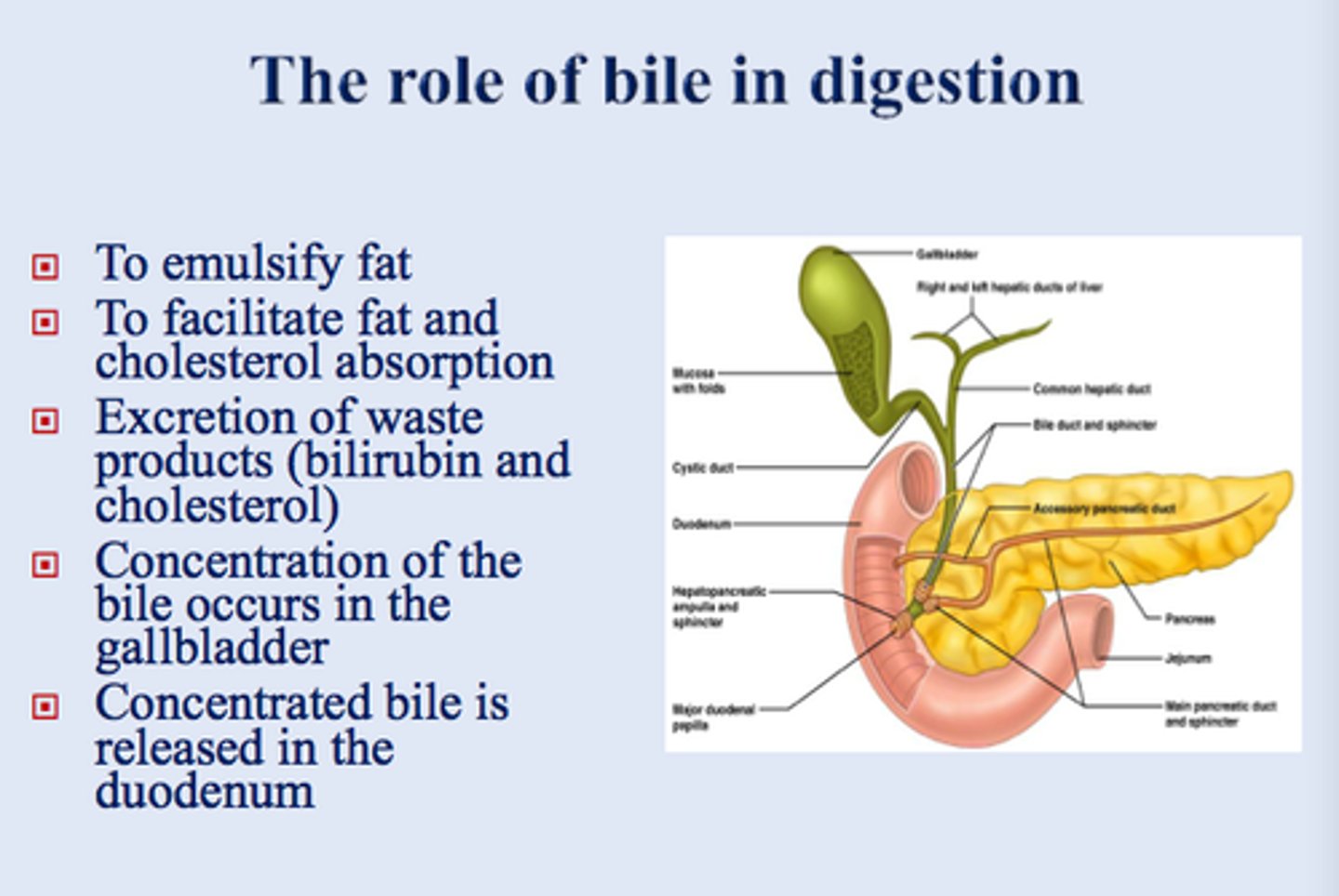
Role of Bile
1. Absorption of Fat-Soluble Vitamins
2. Excretion of Bilirubin and Cholesterol.
3. Fat Digestion.
3 Drugs that Cause Cholestasis
1. Co-amoxiclav
2. Flucoxacillin
3. Oral Contraceptive Pill
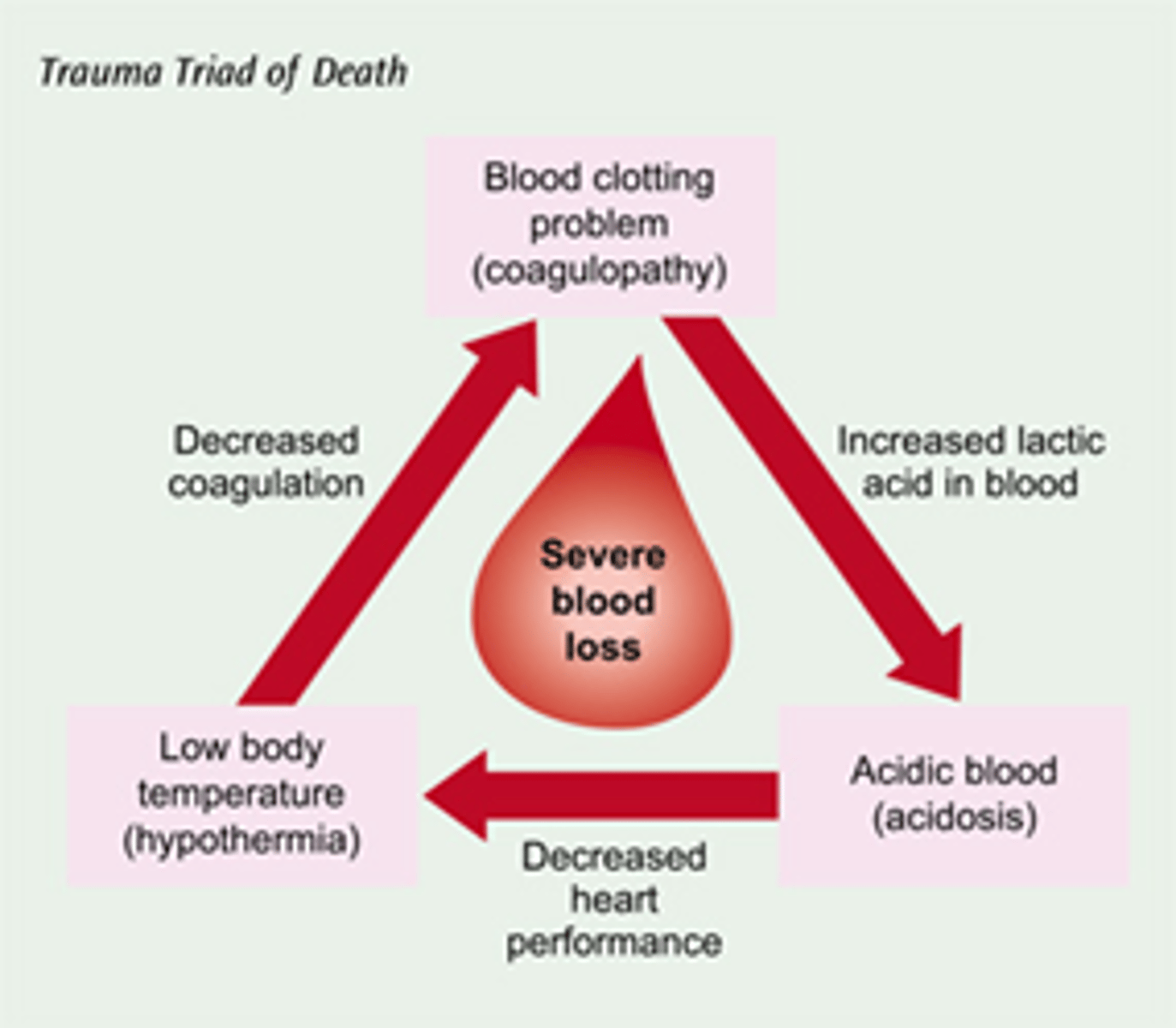
What fat-soluble vitamin is needed for coagulopathy?
Vitamin K
Coagulopathy
A condition where the blood's ability to clot is impaired, leading to excessive bleeding or excessive clotting.
Hepato-cellular Injury raises which Liver Enzymes?
ALT and AST
Hepatocytes are damaged and enzymes leak into the blood.
Cholestatic Injury raises which Liver Enzymes?
ALP and GGT
Bile is not flowing properly due to a intra-hepatic or extra-hepatic obstruction typically caused by gallstones or biliary obstruction.
Which Parameters in a Blood Test are Abnormal in a Liver Failure?
INR, Albumin and Bilirubin
INR is raised and leads to coagulopathy where the blood's ability to clot is impaired.
Albumin is decreased leading to decreased oncotic pressure causing fluid to build up in tissues, e.g., ascites.
Bilirubin is raised due to hepatocytes being damaged or cholestatic issues.
Serum Urea Range
2.5 - 7.8 mmol/L
Signs of Reduced Renal Function in Blood Tests
Serum Creatinine, eGFR and Urea
- Serum Creatinine is raised meaning there is reduced kidney filtration.
- eGFR is decreased.
- Urea is raised meaning reduced excretion of toxins.
Urea
A waste product of protein metabolism, produced in the liver and excreted by the kidneys, they reflect renal excretion and hydration status.
A patient presents with vomiting and poor oral intake. Blood tests show:
Urea: 18 mmol/L (↑)
Creatinine: 90 µmol/L (normal)
eGFR: >90 mL/min
What is the most likely explanation?
C. Pre-renal dehydration
*In dehydration, urea rises disproportionately because it is reabsorbed with water, while creatinine remains normal.
3 multiple choice options
Which pattern is most consistent with intrinsic renal impairment?
D. ↑ Urea and ↑ creatinine together
*Intrinsic kidney damage reduces filtration, causing both urea and creatinine to rise.
3 multiple choice options
A patient taking gentamicin develops rising blood results over 48 hours:
Creatinine: 85 → 150 µmol/L
Urea: 7 → 15 mmol/L
What is the most likely diagnosis?
B. Acute kidney injury
*Rapid rise in creatinine and urea suggests AKI, particularly with nephrotoxic drugs like gentamicin.
3 multiple choice options
Low urea levels may be seen in:
A. Liver Failure
3 multiple choice options
Which blood test pattern suggests post-renal obstruction?
C. ↑ Urea and ↑ creatinine with fluctuating values
*Obstruction causes back-pressure on the kidneys, impairing filtration and raising both markers.
3 multiple choice options
Which finding best suggests a pre-renal cause of abnormal renal blood tests?
C. Urea rises more than creatinine
*Increased urea reabsorption in dehydration leads to a high urea-to-creatinine ratio.
3 multiple choice options
A patient has the following results:
Urea: ↑
Creatinine: ↑
Potassium: 6.2 mmol/L
What is the most urgent concern?
A. Cardiac Arrhythmias
*Hyperkalaemia is the most dangerous complication of renal failure due to arrhythmia risk.
3 multiple choice options
How does Hepatic Impairment affect Drug Handling?
1. Reduced metabolism = Drugs are broken down more slowly, plasma levels increase and half-life is prolonged.
2. Reduced First Pass Metabolism = Oral drugs may have much larger bioavailability with small doses having large effects.
3. Reduced Albumin = More "free" drug when there is less albumin because less protein binding can occur.
Dosing Principles in Liver Impairments
1. Prefer drugs that are renally excreted.
2. Prefer drugs with short half-lives to prevent the risk of accumulation.
3. Avoid highly hepatically metabolised drugs.
How does Renal Impairment affect Drug Handling?
1. Reduces Renal Excretion = Metabolites accumulate and so does the risk of toxicity.
2. Half-Life Increases = Drug stays in the body for longer and steady state is reached more slowly.
Dosing Principles in Kidney Impairment
1. Prefer drugs that are hepatically metabolised,.
2. Adjust doses for renally excreted drugs.
3. Avoid nephrotoxic drugs.
General Rule for Liver & Kidney Impairments
Start low, go slow, monitor closely - or avoid.
What drugs MUST be avoided in Liver Impairment and Why?
Sedatives
- Hepatic metabolism is impaired and drugs that rely on the liver (especially sedatives) are cleared slowly, their half-life is prolonged and drug levels accumulate, even at normal doses.
- Sedatives further suppress CNS functions, mask early warning signs and can trigger encephalopathy in a previously stable patient.
- Protein binding changes increase free drug in liver failure. Albumin is low and sedatives are often highly protein bound resulting in higher free (active) drug concentrations. Toxicity occurs even if total drug levels look “normal”.
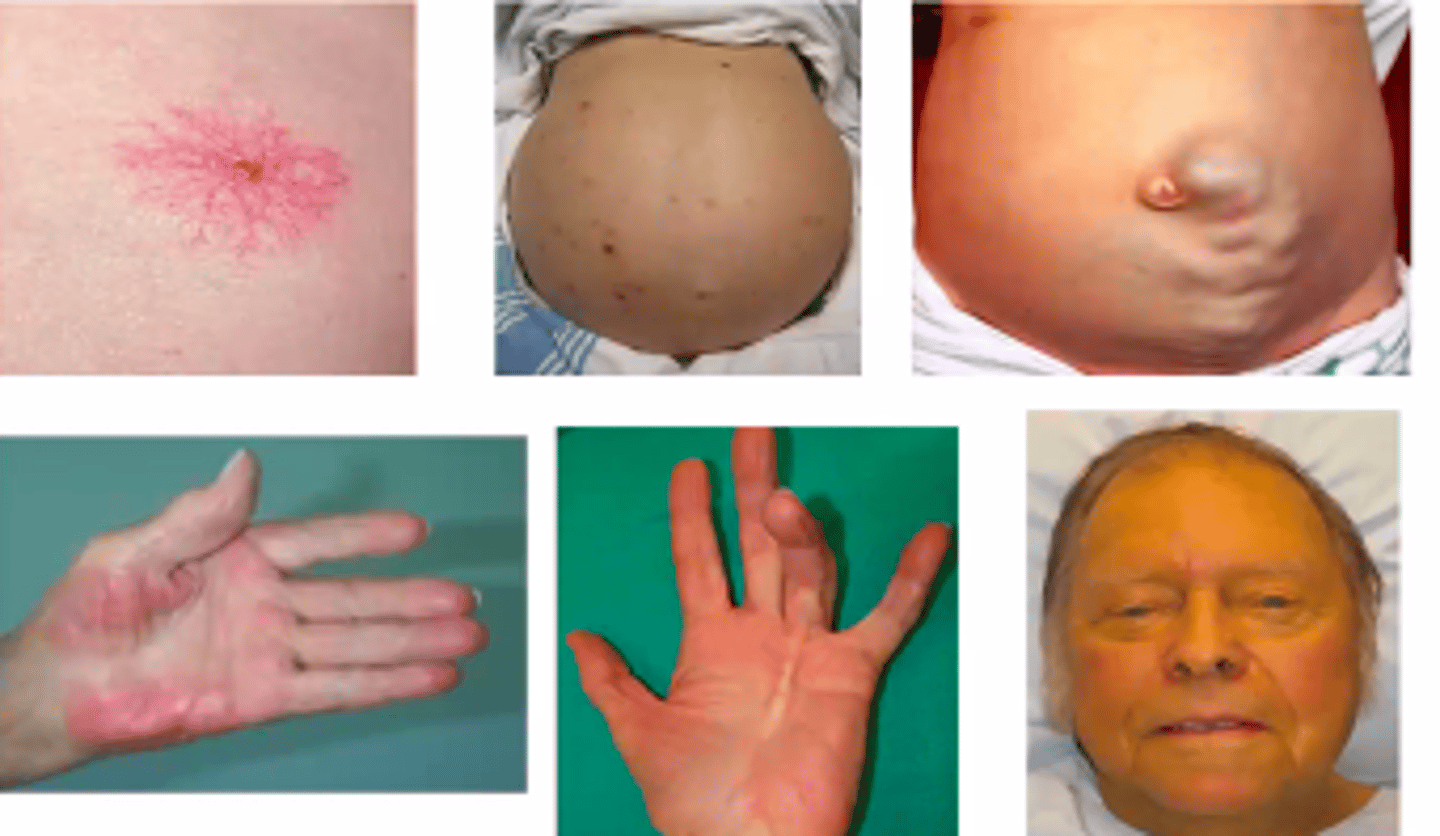
Clinical Features of Decompensated Liver Disease
1. Jaundice
2. Hepatic Encephalopathy
3. Variceal Bleeding
4. Ascites
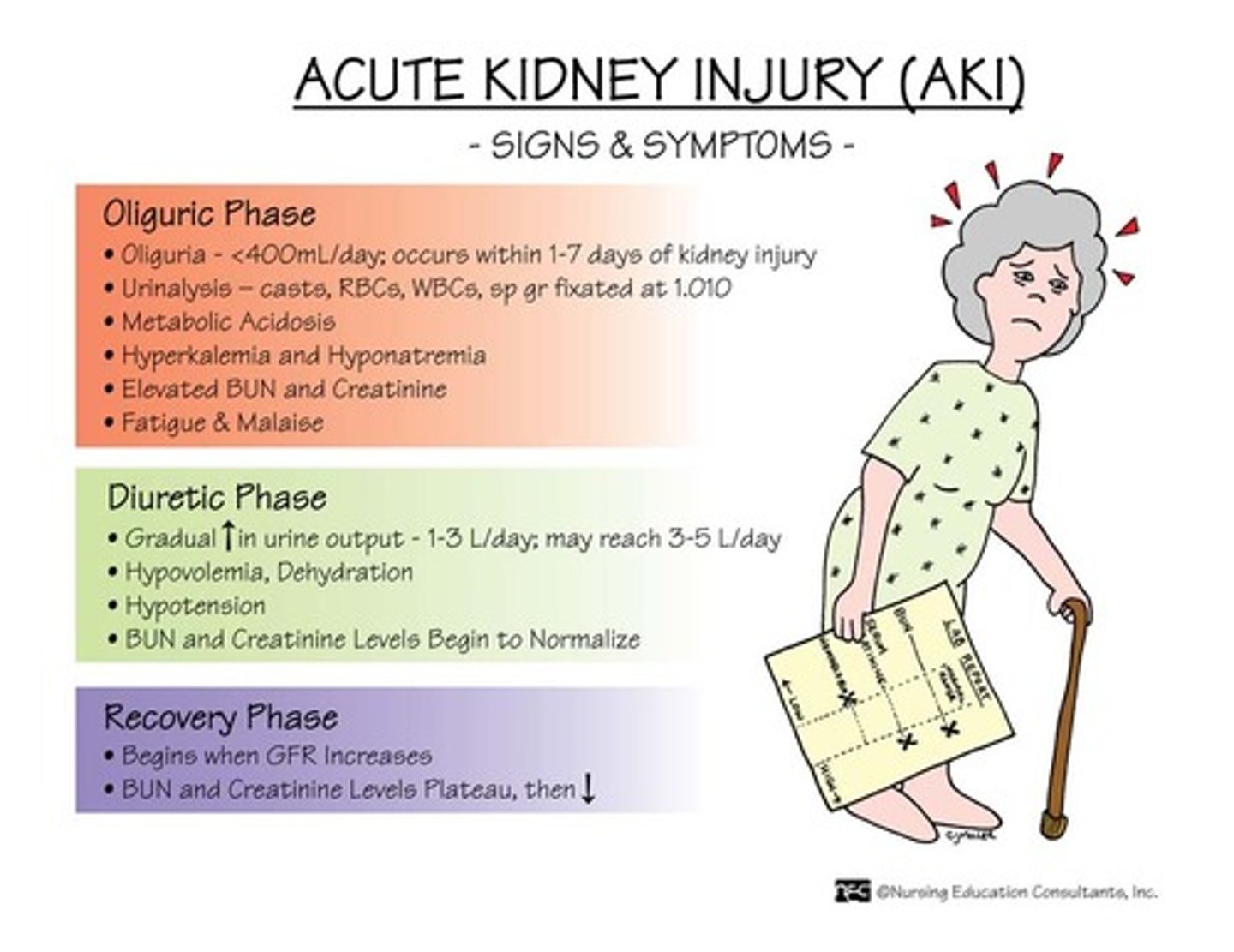
Clinical Features of Deterioration in Renal Disease
1. Oliguria (Reduced Urine Output)
2. Fluid Overload/Peripheral Oedema (Kidneys cannot excrete Sodium and Water)
3. Electrolyte Disturbances (Particularly Hyperkalaemia with Arrhythmias and Palpitations)
4. Uraemic Symptoms (Accumulation of urea and toxins resulting in confusion and itching)