biol 332 physiology exam 3
1/41
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
42 Terms
urinary system fx
excretion - removal of organic metabolic waste
water balance
electrolyte balance
conservation of valuable nutrients (glucose)
control of blood cell formation ( erythropoietin)
regulation of blood pressure (renin)
1 ml/min of urine production
structures of urinary system
kidney
ureter
urinary bladder
urethra
kidney functions
regulates extracellular fluid (plasma and intersistual fluid)
[] of waste product
[] of electrolytes
ph of plasma
nutrients and by products
glucose (C6 H12 O6) → cellular respiration → CO2 and H2O
lipids (CH3 CH2N COOH) → cellular respiration → CO2 and H2O
proteins (C H O N ) → CHO respirated but N urinated
types of byproducts
urea (15 ml/dl)
creatinine (1 ml/dl)
Uremia
increased levels of urea and creatinine in the blood
renal failure indicator
Blood urea nitrogen test (BUN test)
blood sample test measures nitrogen
renal failure if over 15 ml/dl
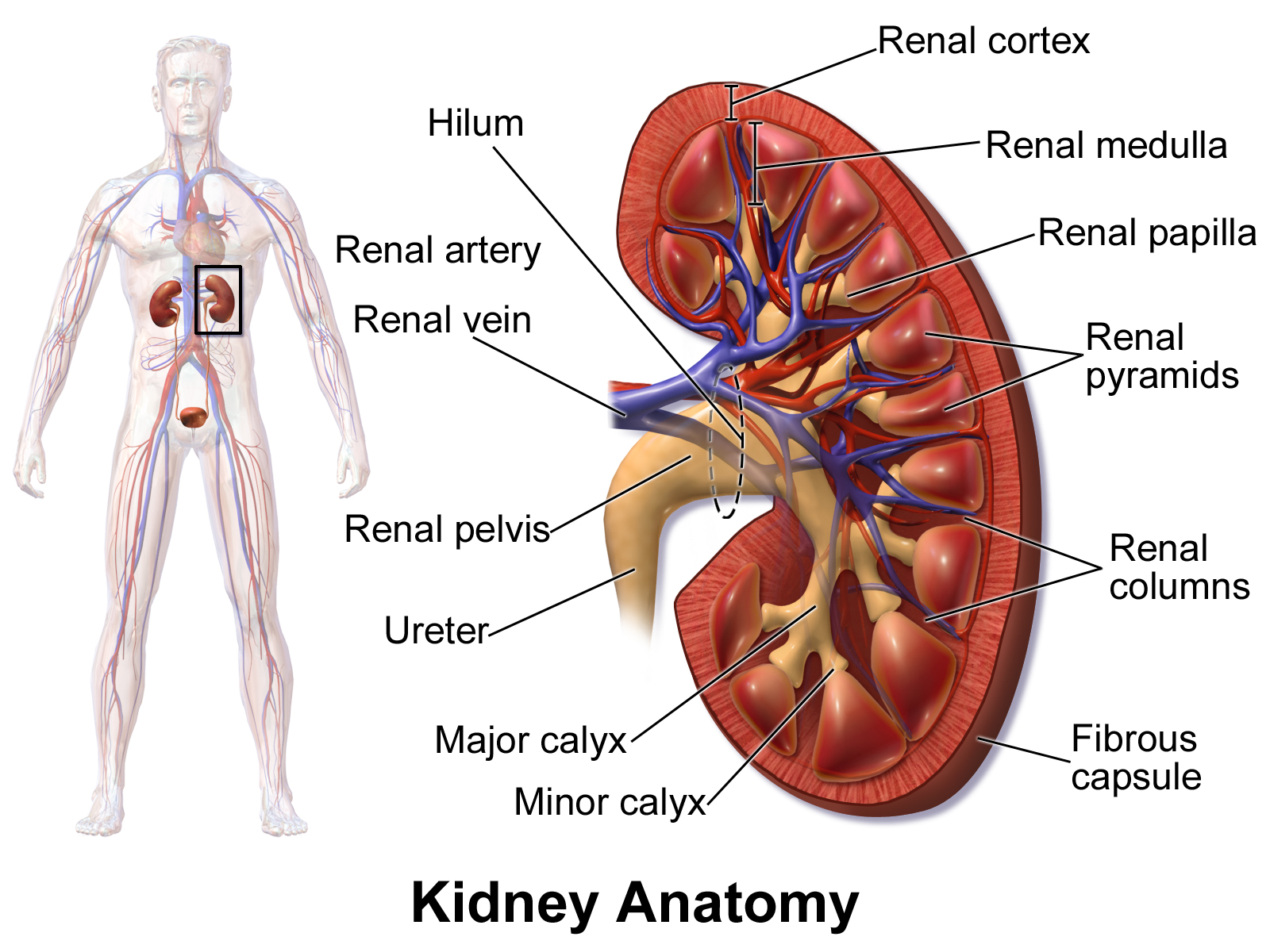
internal kidney structure
renal cortex - outer, granular red brown bc lots of blood flow
renal corpuscles - in cortex, gives granular shapes bc glomerolus balls
glomerulus - filters blood
medulla - inner
pyramids - striped bc lots of rubules tubules
columns - between renal pyramids
calyces - collects urine from renal tubes, minors connect into a major
pelvis - calyces connect and urine drains
ureters strx and fx
transport urine from kidneys to bladder
lined with smooth muscles for peristalsis (contract to push down)
connect to urinary bladder at an angle to prevent backflow
membrane flap at urinary bladder to further prevent backflow !
normal urine production rate
1 ml/min but not all become pee
oliguria
less than 1 ml/min urine
diuretics
increase rate of pee production
bp medication bc lower stroke volume
kidney stones
solidified calcium and acid salts (casts) forming stones
start in the kidney, and have to travel down the ureter and bladder and urethra
caused by oliguria, prevented by low salt intake and high water intake
hydronephrosis
really big kidney stones that get stuck in the urinary system, causing ureter and calyces to expand
unilateral- stone stuck in one ureter
bilateral - stone stuck in bladder
renal blood flow
1 L/min, ½ per kidney
from the 20% of blood that goes to kidneys from the 5 L/min of blood from heart
kidney vasculature structure (tracing)
renal artery - from aorta to kidney
segmental arteries → interlobar arteries (renal columns) → arcuate arteries (top of cortex) → cortical radiate arteries (interlobular) → microscopic afferent arterioles (1 mil per kidney)
all branching so its a lot of arteries
glomerulus
filter site for blood
fenestrated capillaries - lots of holes that are too small for cells like rbc to escape but fluid can be pushed out
filtration moves into other tubules system called nephrons
nephrons
system of tubules around the glomerulus
renal corpuscle - glomerulus + bowmans capsule, always in cortext, filter site, 180l fluid passes but no rbc released
filtrate out the glomerulus and picked up by bowsman capsute
afferent arterioles drain blood into glomerulus → fluid and solutes are pushed through the glomerulus and pushed into the bowmans capsule (ig like coffee filter) → remaining filtrate blood in glomerulus is drained by efferent arterioles
renal tubules - reabsorption and secretion site
provimal convulated tubule → loop of henle → distal convulated tubule → collecting tubule → collecting duct
compounds not filtered out of glomerulus/stay within capilaries
rbc
plasma proteins
these are the bigger cells in the blood
compounds that will be filtered out of glomerulus/leave capilaries
water
sodium
glucose
urea
creatinine
urorbin
most of these will be reabsorbed
glomerular hematuria
damaged glomerulus
blood come out of urine,
can cause anemia
non glomerular hematuria
blood from kidney stone, UTI, bladder cancer,
blood come out of urine,
can cause anemia
glomeular dmg test
dysmorphic rbc - glomerular
normal rbc - not glomemrular
proteinuria
dmg to glomerulus, plasma protein come out in urine
hypertension sign
cause edema
filter
blood pushed through glomerulus into nephrone
affects rbc and plasma proteins
reasborption
tubules back bloodstream
affects water, sodium, and glucose
178.5 L of filtrate reasbsorbed
secretion
taken from blood into tubule after filter
excretion
substance from blood, put into tubules, and eliminated
affects urea, creatinine, and urobilin
glomerular filtration rate
indicates how well kidneys work, between filtration and reabsorption
measuring ultra filtrate, h2o, na, glucose, urea, creatinine, urobilin
125 ml per minute
increasing gfr
increasin size of afferent artertionsm, more blood come in and more pressure
decreasing gfr
constricting size of afferent artertiones, decrease blood and less pressure
renal disease
gfr less than 60 ml/min
end stage renal disesae
less than 15ml/min gfr
build up of nitrogen waste in blood
end stage renal disease treatments
kidney transplant - new working kidneys put into body
dialysis - connected to machine and filters blood for you
death - urea or creatinine cannot be removed
water reabsorption site
proximal convoluted tubule - 80% mandatory water reabsorbed, depends on Na and Glucose
collecting duct - facilitated water reabsorption, regulated by the body depending on hydration levels given from the pituitary gland
more/less hydrated → less/more reabsorption → more/less extretion
sodium glucose co transporter
uptakes sodium and glucose and pumps in n out of cell
water follows sodium in n out of cell
anti diuretic hormone ADH
produced in hypothalamus
released from posterior pituitary gland
facilitates water reabsorption and less excretion
collecting duct
lumen - filtration flow site
apical - medial
basal - superficial with blood vessels
v2 receptor (vasopressin) - basolateral side, adh binds to it
v2 signal aquaporin - inserts on apical membrane, allows h2o to be absorbed
aquaporins
water channel proteins on the edges of vesicles
with adh → fuses with plasma membrane
without adh → pinches itself off back

flozin
diuretic
antagonize sglt 1 (blocked)
sodium and glucose will not be absorbed, water will not follow, and all be excreted instead
v2 antagonist
diuretics
antagonized v2 in the collecting duct
Aquaporins don’t bind, and vesicles cannot move to reabsorb water
anti anti-diuretic hormone (ethanol)
diuretics
treats hypertension/pulmonary edema → decrease blood vol and lowers bp
Suppresses ADH and does not facilitate water reabsorption → increase excretion (pee)