N341 EXAM 3, part 2: Potassium/Calcium
1/56
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
57 Terms
Hydrogen
acid
moves into cell if basic, and out of cell if acidic --> hydrogen moves in and out to neutralize the body.
Potassium normal level
3.5-5.0 mEq/L
Potassium function
- cation (+ charge) in ICF
- must be ingested daily, body does not conserve it
function --> MUSCLES
- neromuscular function
- transmission of nerve impulses
- muscle contraction
- cell electrical neutrality
potassium diet sources
- chocolate
- dry fruits, nuts, seeds
- fruits: oranges, bananas, apricots, cantaloupe
- meats
- vegetables: beans, potatoes, mushrooms, tomatoes, celery
IC v EC potassium
high in IC, low in EC
H+ is low (neutral) in both
how does K+ and H+ move in acidosis
K+ out
H+ in
--> to make more basic
how does K+ and H+ move in alkalosis
K+ in
H+ out
--> to make more acidic
how does the body regulate potassium?
ingesion --> NEED 40-60 mEq of K+ per day (b/c body cannot conserve)
renal regulation --> excreted through kidneys (can't conserve, but can excrete extra w/ aldosterone when needed)
pH level --> K+ and H+ exchage to maintain balance
sodium-potassium pump --> pulls potassium in and out of cells against concentration gradient and osmosis
Hypokalemia
<3.5 mEq/L --> not enough potassium
Hypokalemia etiology/cause
inadequate intake of potassium --> usually d/t TPN, NPO, or alcoholism
excessive output --> intestinal fluids have alot of potassium
- suction
- lavage (washing stuff out)
- prolonged vomitting
- diarrhea
- fistuals
- laxitive abuse
- prolonged diaphoresis (potassium wasting)
- diuresis from newly implanted kidney
- osmotic diuresis (high urine glucose level)
- elevated aldosterone production --> conserving sodium, wastes potassium
- alkalosis --> potassium moves into cell)
What drugs cause hypokalemia?
- loop + thiazide diuretics --> waste potassium
- corticosteroids --> body conserves salt, loses potassium
- insulin
- some antibiotics
- laxatives --> lose potassium through GI
Insulin affect on potassium
treats hyperkalemia --> moves potassium into our cells (stashes it)
so BAD for HYPOkalemia
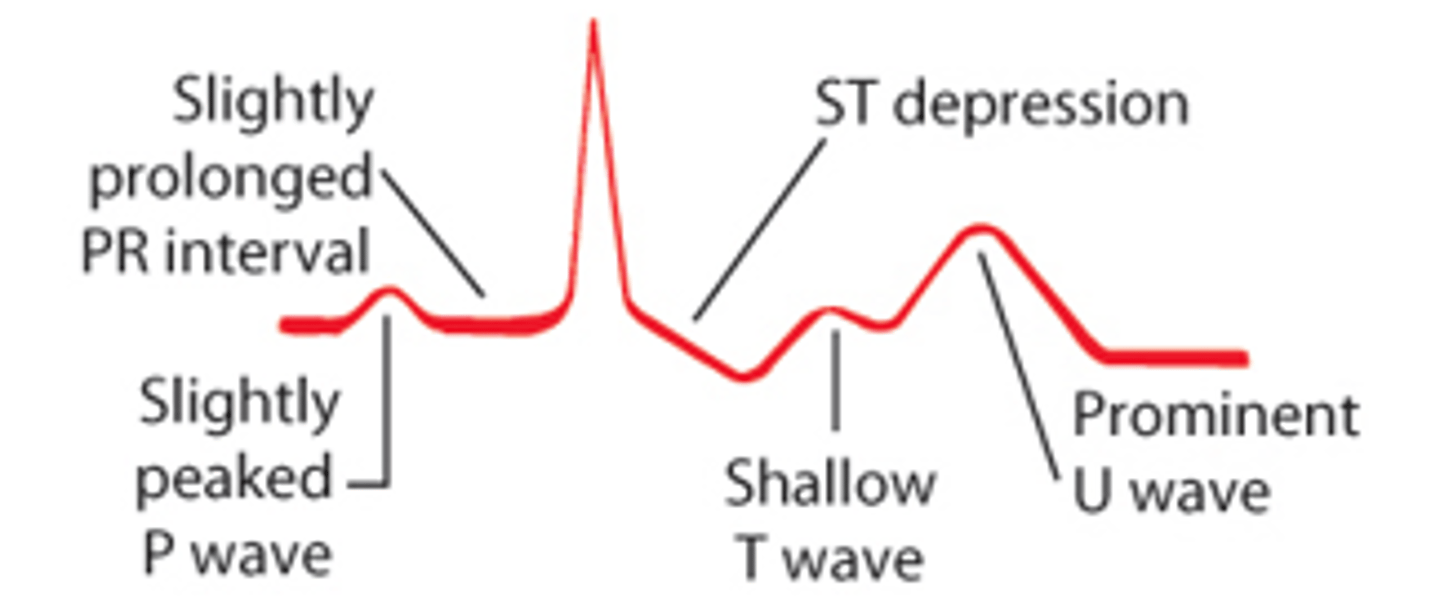
hypokalemia clinical manifestations
WEAK AND SLOW
Cardiac
- EKG changes --> heart muscles not depolerize/repolerize
- disrhythmias --> not contracting normal
- PROMINENT U WAVE
- irregular weak pulse
- orthostatic hypotension
muscular
- skeletal musle weakness
- paralysis
- rhadbdomyolysis --> we don't use our muscles, they break down
smooth muscle weakness (GI)
- constipation
- paralytic ileus
- anorexia
- N/V
hypokalemia diagnostic test result
- serum potassium level <3.5
- elevated pH and Bicarb levels
- slightly elevated serum glucose level
- characteristic EKG changes --> SHALLOW T WAVE and PROMINENT U WAVE
with hypokalemia the U wave is...
bigger --> takes longer to charge
hypokalemia treatment
Oral replacement
- food high in potassium
- potassium supplement --> drink w/ FULL glass of water, do NOT crush extended release
IV potassium replacement --> dangerous, but commin (impacts heart, cardiac arrest is possible)
IV potassium replacement
- high alert med
- dilute in compatible solution
- dose should NOT EXCEED 40mEq/L
- rates should NOT EXCEED 10-20 mEq/hr
- NO BOLUS or DIRECTLY FROM VIAL
- check serum potassium levels frequently
- irritating to tissue --> more PROXIMAL and LARGER VESSEL
hypokalemia nursing interventions
- monitor VS/BP every 15 minutes
- safety d/t weakness
- EKG monitor for U wave
- I/O --> diuretic may be contributing
- check for alkalosis --> ABG
- admin appropriate replacemnt therapy
hypokalemia and digoxin
MONITOR --> hypokalemia and digoxin can cause TOXICITY
hyperkalemia
> 5 mEq/L --> high potassium, less common, but DEADLY, cardiac arrest possible at any moment
hyperkalemia etiology/cause
increased intake of potassium --> not typical, but caused by SALT SUBSTITUTES
decreased potassium exretion
- renal failure
- low aldosterone --> not excreting potassium
injury --> when cell is injured, potassium is released (99% of potassium is in the cells)
- burns, infection, chemo, trauma
other causes
- acidosis --> pulls potassium out
- donate blood --> when nearing expiration, potassium rises (monitor K+ when giving blood products)
drugs that cause hyperkalemia
- beta blockers
- potassium sparing diuretics
- some anitibiotics
- ACE inhibitors --> suppress aldosterone
- NSAIDS --> suppress aldosterone
- chemo --> cells open/die
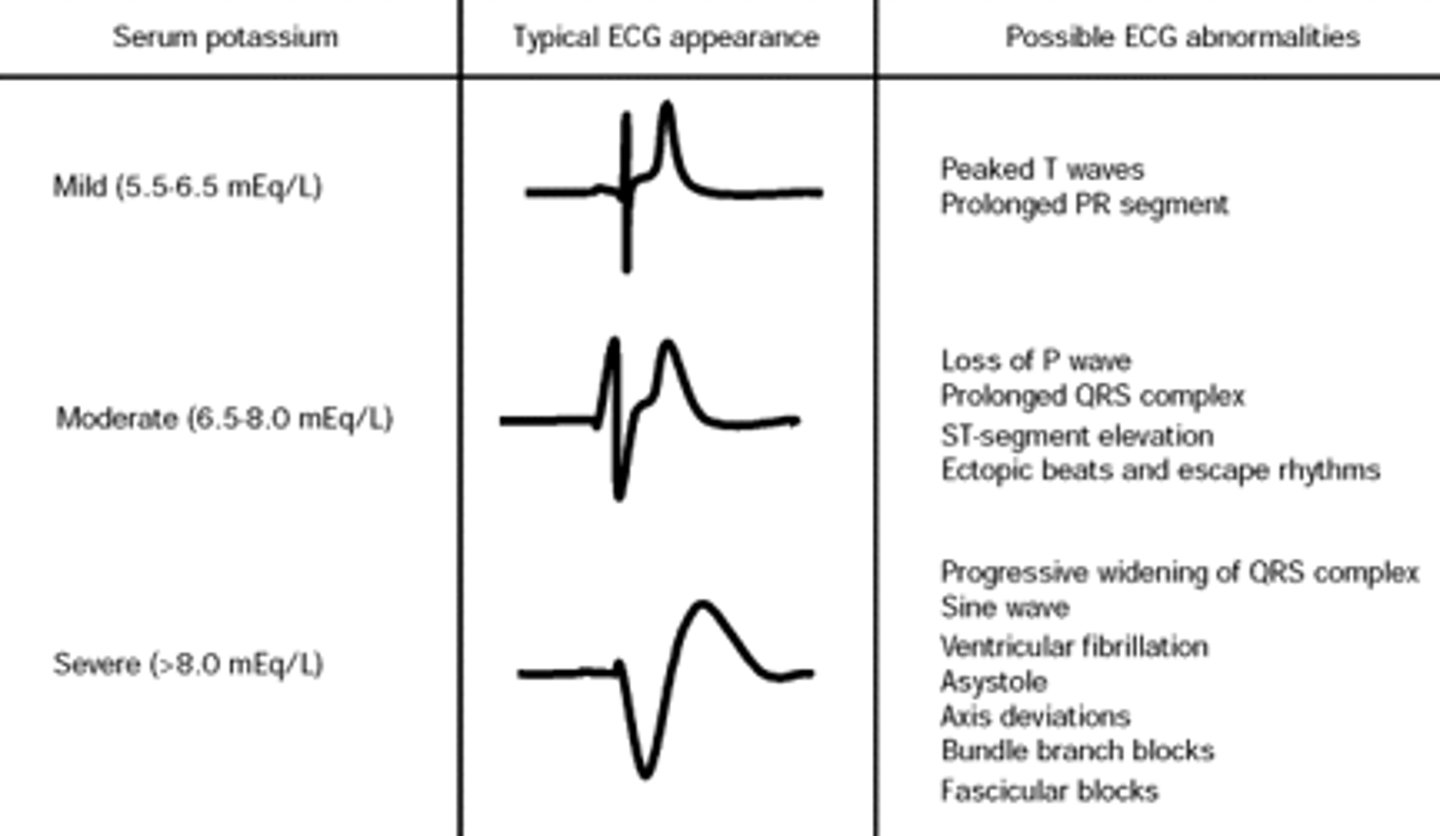
hyperkalemia diagnostics
- serum potassium level >5 mEq/L
- decreasd arterial pH --> K moves into cell and H moves out
- EKG abnormalities --> tall T wave
hyperkalemia clinical manifestations
effects heart, smooth muscle mostly
cardiac
- tall, peaked T wave
- ventricular arrhythmia and cardiac arrest
- slow HR
- slow BP
neuromuscular (slow, sluggish)
- muscle weakness
- paralysis
GI (hyperactivity of smooth muscle)
- Nausea and diarrhea
hyperkalemia EKG changes
hyperkalemia treatment
life threatening --> detect/treat EARLY
restrict potassium intake --> limit oral and IV intake
promote potassium excretion
- diurectics
- kayexalate
- increased fluid intake (IF kidneys work)
- dialysis --> common
move potassium in cell
- insulin w/ glucose --> hides potassium until treatment is figured out
- treat acidosis w/ bicarb
protect the heart
- administer calcium gluconate
what does kayexalate do w/ hyperkalemia
causes p/t to poop out potassium
calcium gluconate use w/ hyperkalemia
cardiac protectant (calcium chill/relaxes heart + muscles) while you work to get potassium down
HIGH ALERT med
hyperkalemia nursing interventions
- monitor cardiac status w/ EKG
- monitor I/O's --> not excreting urine? likely the cause
- prepare to administer calcium gluconate
- prepare dialysis if no response to treatment (long-term fix)
Calcium level
8.6-11 mg/dL
calcium function
skeletal and heart muscle contraction.
- CALMS nerve cells (chills everything out)
- nerve impulse and transmission
- blood clotting
- building bones and teeth (99% stored there)
parathyroid hormone effects on calcium
promotes calcium resorption from the bones and teeth
- causes serum calcium to rise
- steals calcium from bones/teeth
- tell kidneys to conserve Ca and GI to absorb Ca
calcitonin effect on calcium
antagonizes parathyroid hormone --> when Ca is too high, tells it to stop
pH impacts on calcium
INVERSE relationship
High pH = Low Calcium
high pH (alkalosis) causes calcium to bind to albumin, lowering total available ionized calcium
phosphates relationship with calcium
INVERSE
- Ca binds to phophate
- high phosphate levels --> low Ca d/t binding
RENAL FAILURE causes high phosphate levels leading to hypocalcemia
magnesium and calcium
HYPOmagnesemia causes end organ reistence to PTH and decreaeed production of PTH reulting in HYPOcalcemia
calcium foods
- dariy
- leafy green vegetables
- whole grains
- tuna and salmon
- vit D
why is vitamin D important to calcium?
vit D is needed to absorb Ca in the GI tract.
vit D deficient = hypocalcemia
hypocalcemia level
< 8.6 mg/dL
hypocalcemia etiology/cause
- hypoparathyroidism --> decreased levels of PTH, take calcium from bones/teeth
- hypoalbuminemia --> not as much Ca bound to albumin
- pancreaititis --> binds to fat
- magnesium imbalance
- hyperphosphatemia
- alkolosis
- malabsorption syndromes (cannot absorb) --> diarrhea, laxative use, low vit D, Crohn's
- intake issues --> alcoholics and breast-fed babies
- citrate in blood porducts
burns/sepsis --> tissue traps Ca
hypocalcemia drug causes
- anticonvulsants (phenobarbital and phenytoin) --> interfere w/ vit D metabolism
- loop diuretics (lasix) --> waste calcium
- calcitonin --> parathyoid hormone antagonist
- antibiotics
- phosphates --> low calcium, enema
hypocalcemia clinical manifestations
Neuromuscular
- tetany
- Chvostek's sign
- Trousseau's sign
- hyperactive deep tendon reflexes
- laryngospasm --> airway may not close, have airway cart around
- seizures
GI
- hyperactive bowel sounds
- abdominal cramps
CNS
- irritability
- confusion
- delusions
- convulsions
- anxiety
cardiac --> cannot push a ton of blood out d/t partial contractions
- hypotension
- cardiac arrest
- decreased myocardial contractility
- prolonged QT interval and risk for torsades de points (fatal arrhythmia)
renal
- oliguria --> low urine output
- anuria --> no urine output
tetany
involentary contractions of muscles
Chvostek's sign
tap over facial nerve
- see contraction of upper lip, nose, cheek
Facial muscle spasm upon tapping
Trousseau's sign
inflate BP cuff 20 mmHg above systolic.
- see flexed wrist, adducted thumb, extended fingers (hand/risk contract)
arm/carpal spasm
hypocalcemia diagnostic results
- total serum calcium below 8.6 mg/dL
- ionized calcium below 4.5 mg/dL
characteristic EKG changes
hypocalcemia treatment
acute hypocalcemia (symptomatic --> medical emergency)
- administer calcium gluconate or calcium chloride
chronic hypocalcemia
- vid D supplement and calcium-rich diet
- phosphate binder (lower phosphate level)
calcium gluconate
- high alert medication
- do not give IM --> muscle necrosis
- dilute IV calcium in dextrose 5% and water
- do not push IV calcium --> bradycardia, hypotension, and cardiac arrest (heart too chill)
- VESICANT
hypocalcemia nursing interventions
- airway cart, trach tray, ambu bag
- cardiac monitor --> EKG changes
- seizure precaustions (pads, suction, etc.)
- avoid overstimulation (quiet room, limit visitors, soft lighting)
hypercalcemia level
>11 mg/dL
hypercalcemia etiology cause
hyperparathyroidism --> producing PTH at high level, losts of Ca being pulled out of bone
- cancer --> tumors secrete PTH
- multiple fractures --> Ca leaks out
- immobilization --> Ca leaks out
- hypophosphatemia (not enough, too many free Ca)
- acidosis --> pH low, Ca high
hypercalcemia drug causes
- thiazide diuretics --> potentiate PTH
- antacids --> lots of Ca
- lithium --> compete w/ Ca
- Vit A and D --> absorb too much Ca
hypercalcemia clinical manifestations
(decreased neuromuscular irratibility)
Cardiac
- HTN
- dysrhythmia --> heart block (HR slow, forgets to beat) and cardiac arrest
neuromuscular
- decreased deep tendon reflex
CNS
- bizzare behavior
- coma
- lethargy
GI
- hypoactive bowel sounds
- constipation
renal
- polyuria --> decreased renal function
- kidney stones --> made of calcium
skeletal
- bone fractures/pain
hypercalcemia diagnostic results
- serum Ca >11 mg/dL
- ionized Ca >5.5 mg/dL
- digitalis toxicity
- X-ray revealing pathologic fractures
- characteristic EKG changes
digitalis toxicity
toxic drug effects from administration of digoxin
hypercalcemia treatment
- limit intake and flush out --> dietary, meds, IV infusion
- hydrate the p/t --> oral 3,000-4,000 mL per day, IV 0.9% saline
- loop diuretic (NO thiazide diuretics)
- dialysis (life threatening hypercalcemia)
- corticosteroids --> block bone resportion and GI absorption of calcium
- calcitonin --> stop parathyroid hormone
- biphosphates
- weight bearing activity --> force calcium back into bones
hypercalcemia nursing interventions
- cardiac monitor for arrhythmias
- assess for kidney stones (strain urine)
- I/O --> renal failure common