Toxicology
1/83
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
84 Terms
History Must Include
Time, route, duration, and circumstances of exposure
Name and amount of each substance involved
Onset, nature, and severity of symptoms
First aid measures already taken
Medical/psychiatric history and occupation
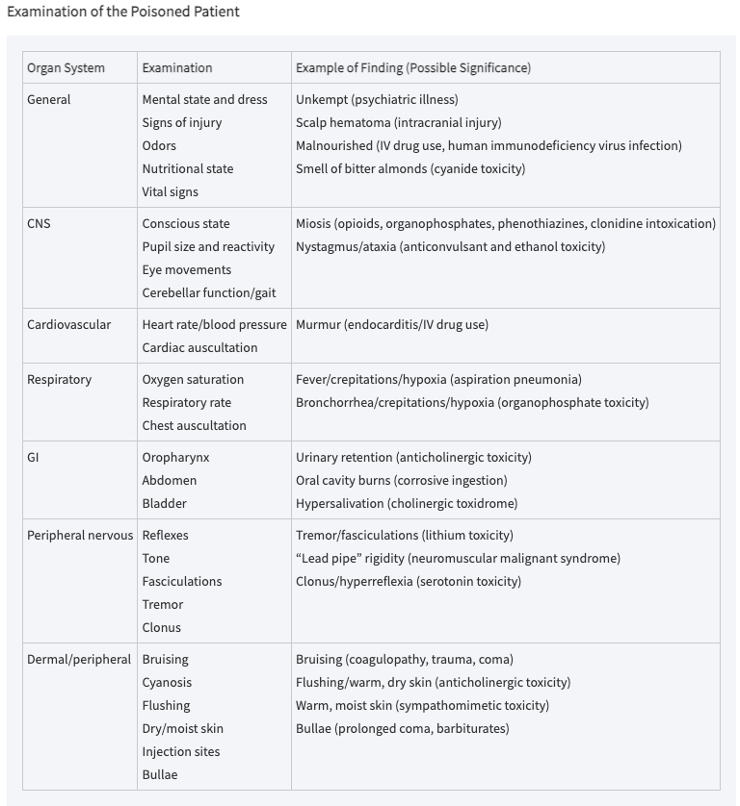
Physical Exam Focus
Vitals, cardiopulmonary system, neurologic status
Eyes: nystagmus, pupil size, reactivity
Skin: burns, color, warmth, moisture, puncture marks
Abdomen: bowel sounds, bladder size
Neuromuscular: dyskinesia, fasciculations, rigidity, tremors
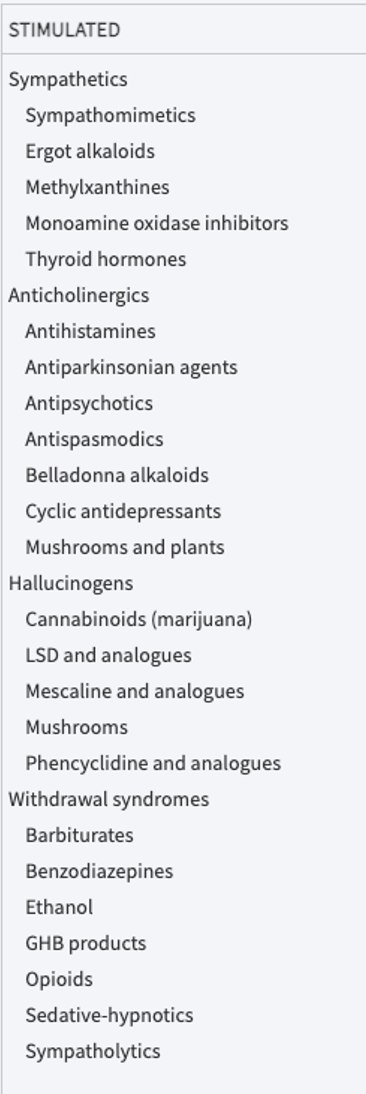
Stimulated State
Sympathomimetic/anticholinergic
Increased HR
Increased BP
Increased temperature
Mydriasis
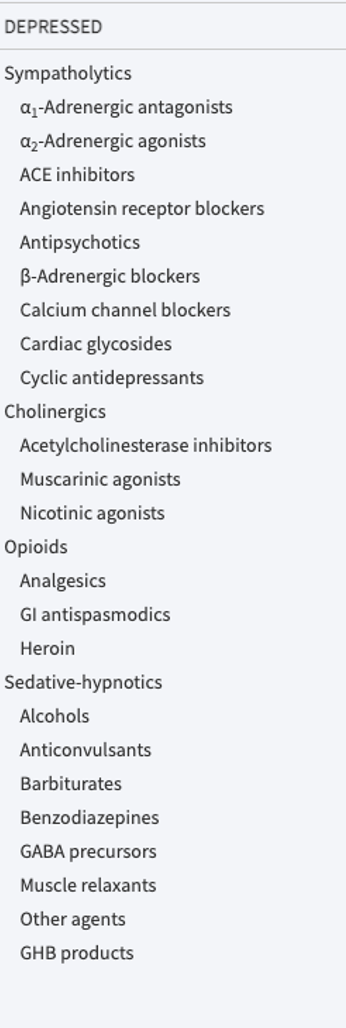
Depressed State
Opioids, sedatives, cholinergics
Decreased HR
Decreased BP
Miosis
Discordant State
Asphyxiants, CNS syndromes, AGMA inducers → mixed findings
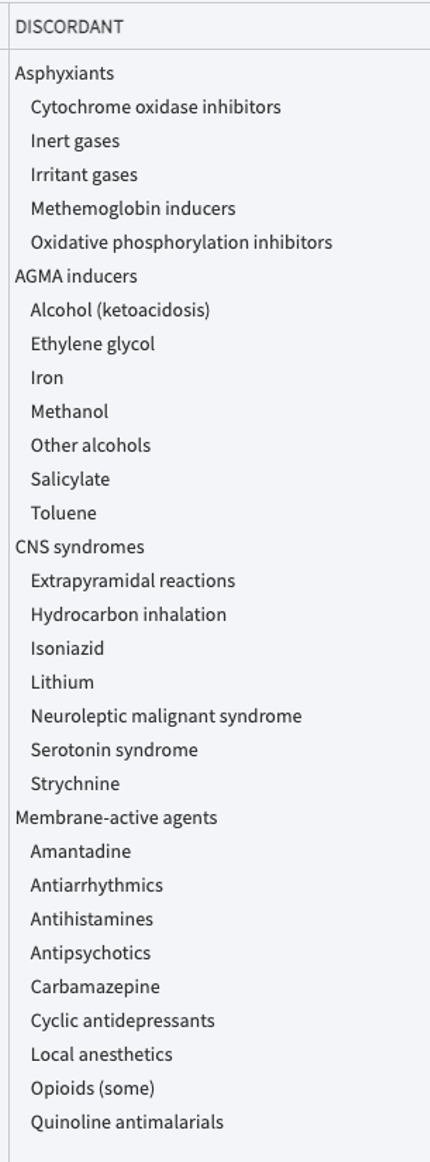
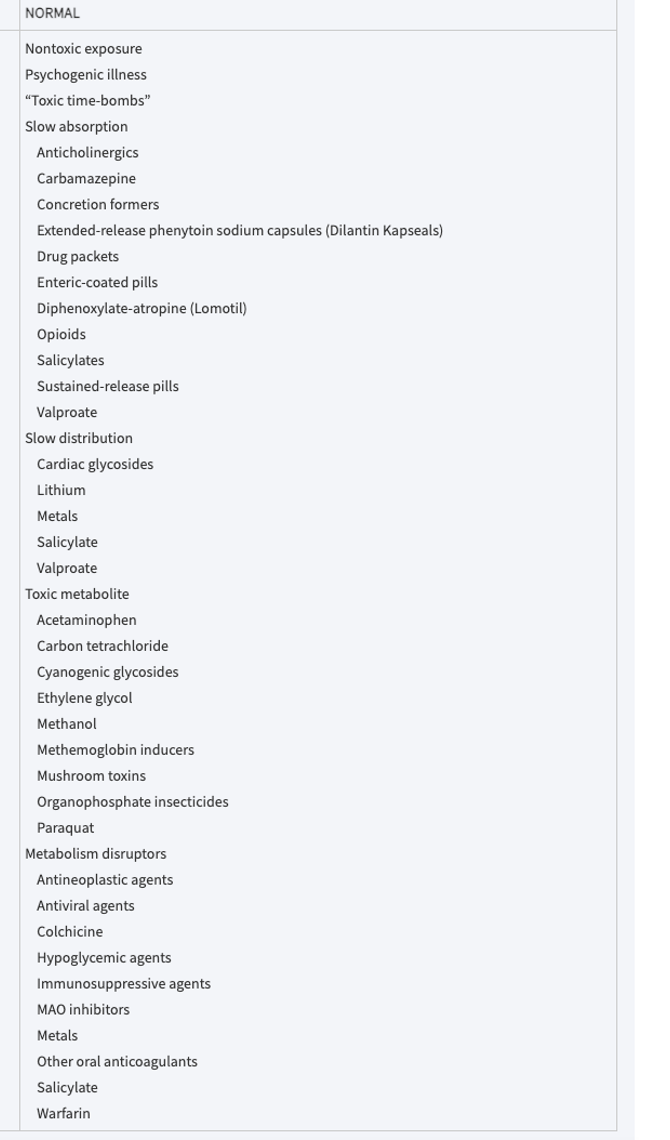
Drugs that have Normal Response
Qualitative Screening
Urine drug screen → confirms/rules out suspected poisoning
Obtain baseline ECG for any suspected cardiac toxin
Rapid qualitative tests for drugs of abuse may screen but not diagnose → most useful when
Unexplained coma
Seizures
Cardiac instability
Metabolic or respiratory acidosis
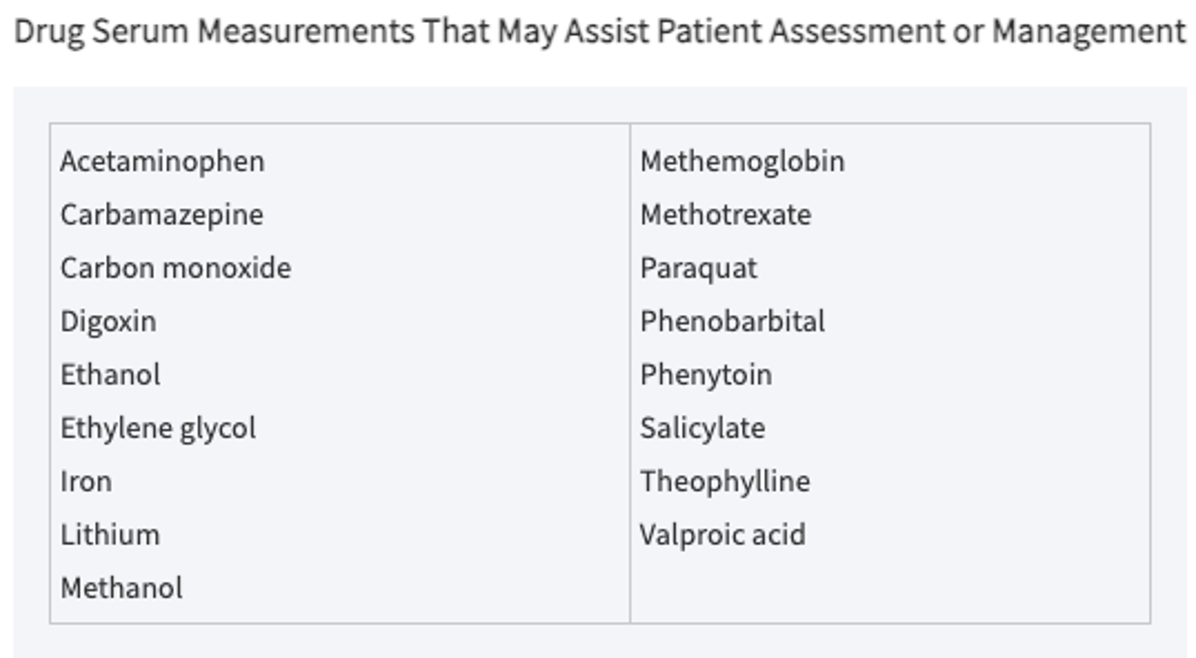
Quantitative Serum Levels
Guide clinical management for specific agents
APAP
Alcohols
Anti-convulsants
Barbiturates
Digoxin
Heavy metals
Iron and lithium
Salicylates
Antidote Trial
Resolution of altered mental status/abnormal vitals within minutes of IV antidote is virtually diagnostic (dextrose, naloxone, flumazenil)
Leading Overall Cause of Death from Poisoning
CO
Most Common Pharmaceutical Agent Implicated in Fatal Poisoning
Acetaminophen
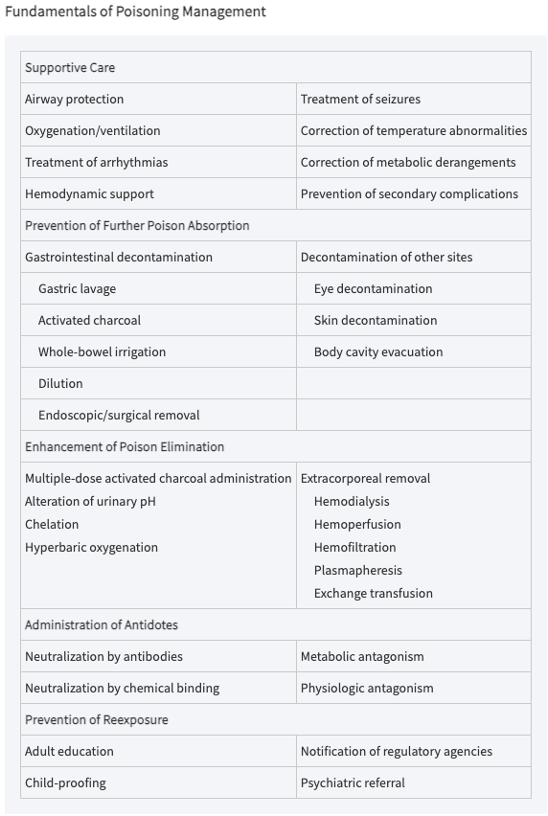
Pre-Toxic Phase
Before onset of poisoning
Decontamination is highest priority: assume the maximal potential toxicity
Most effective phase for decontamination
Toxic Phase
Onset → peak effect
Resuscitation is priority
IV access
O2 saturation
Cardiac monitoring
Consider decontamination, but less effective
Consider elimination enhancement
Resolution
Continued supportive care until clinical, lab, and ECG abnormalities resolve
Some agents may rebound from tissues
Things stored in fat
Airway and Breathing
Consider intubation for CNS depression or seizures (aspiration protection)
Mechanical ventilation for respiratory depression
ECMO for critically ill patients refractory to resuscitation
Hemodynamics and Rhythm
Hypotension unresponsive to fluids → vasopressors (epinephrine, NE)
SVT with instability → treat based on causative agents
Seizures/hyperthermia → benzodiazepines or barbiturates
Phenytoin contraindicated in toxicologic seizures
Ventricular arrhythmias from TCAs → sodium bicarbonate
Anti-arrhythmics contraindicated in TCA dysrhythmia
Psychosis → haloperidol or ziprasidone
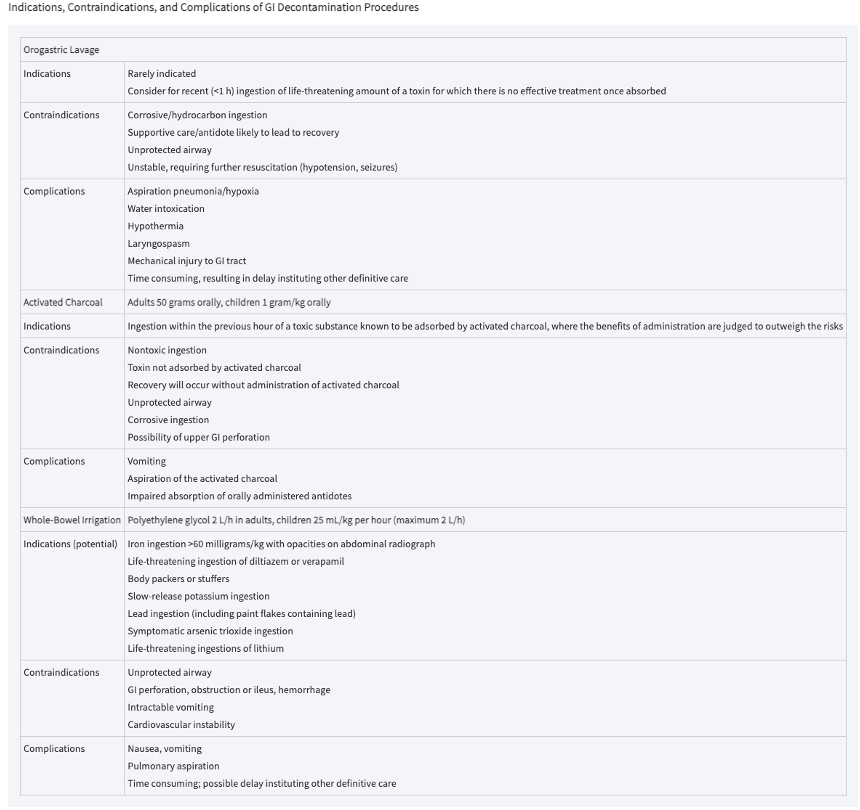
Activated Charcoal Mechanism and Efficacy
Absorbs ingested poisons within the gut lumen → charcoal-toxin complex evacuated in stool
Efficacy by time of administration
Within 5 minutes → 73% reduction in absorption
Within 30 minutes → 51% reduction
Within 60 minutes → 36% reduction
Activated Charcoal Not Effective For
Mineral acids
Alkalis
Highly dissociated salts
Corrosive agents → obscures endoscopy
Altered airway → aspiration risk
Multiple Dose Activated Charcoal (MDAC)
Repetitive oral dosing every 2-4 hours enhances elimination of already absorbed substances
Approaches efficacy of hemodialysis for:
Phenobarbital
Theophylline
Carbamazepine
Dapsone
Quinine
Contraindications
Ileus
Bowel obstruction
Hemodynamic instability
Cathartics
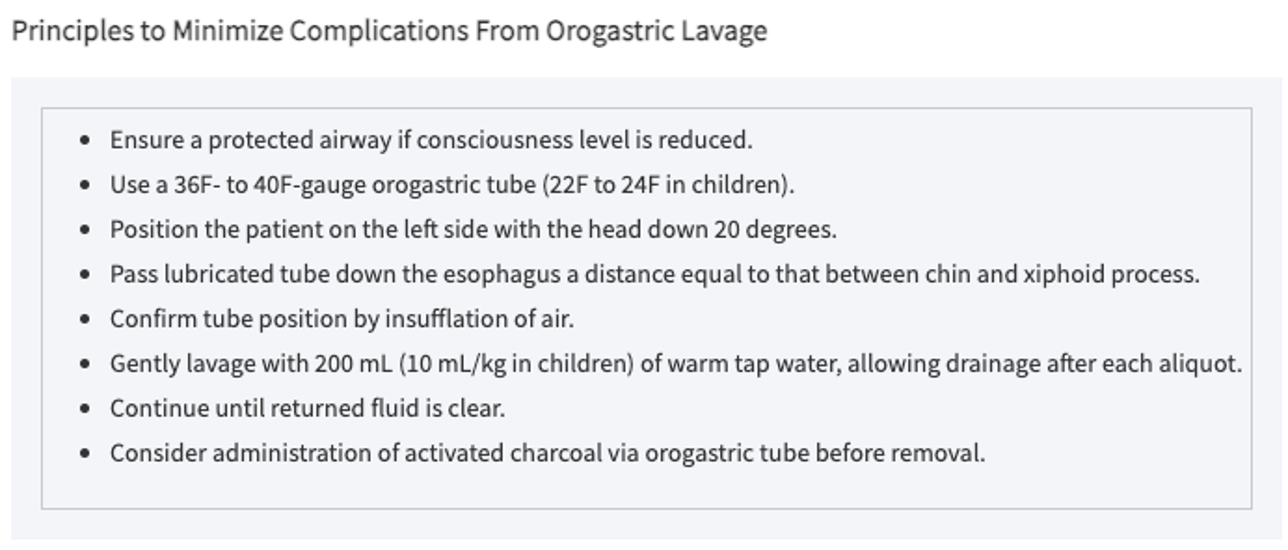
Gastric Lavage
Used for life threatening poisons not treatable with other methods (colchicine)
Patient position → Trendelenburg, left lateral decubitus
Put a bunch of fluid in and then flush it out
Efficacy
52% decrease in absorption within 5 minutes
16% decrease in absorption within 60 minutes
Not done often because it loses efficacy so quickly
Contraindications
Corrosives or petroleum distillates → risk for perforation/aspiration
Compromised/unprotected airway
Combative patients or those who refuse
Whole Bowel Irrigation
Ideal for: objects
Foreign bodies
Drug packets
Agents poorly absorbed by charcoal (heavy metals)
Use PEG electrolyte solution at 2L/hr PO or NG until rectal effluent is clear
Patient must be sitting upright
Contraindications
Bowel obstruction
Ileus
Hemodynamic instability
Compromised airway (aspiration risk): could potentially do for someone who is intubated
Syrup of IPECAC
No longer has role in poisoning management
Can cause electrolyte/cardiac toxicity
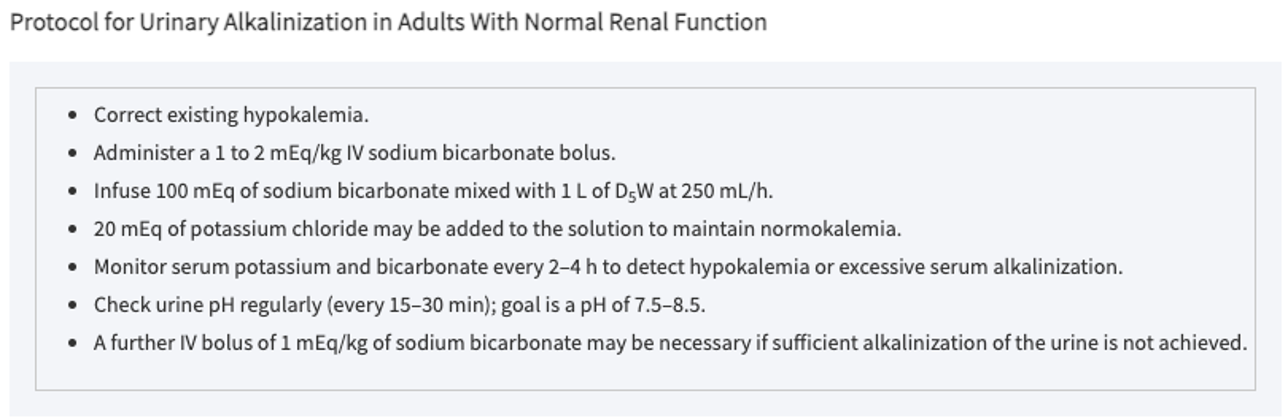
Urinary Alkalization
Goal
Urine pH > 7.5
Urine output 3-6 mL/kg/hr
Use IV NaHCO3
Ion trapping prevents renal reabsorption of acidic poisons (salicylates)
Contraindications
CHF
Renal failure
Cerebral edema
Monitor
Acid-base
Fluids
Electrolytes
Extracorporeal Removal
Most useful for:
Low molecular weight
High water solubility
Low protein binding
Small Vd
Indications
Carbamazepine
EG
Isopropyl alcohol
Lithium
Methanol
Theophylline
Salicylates
Valproate
Use when:
Deterioration despite aggressive supportive care
Dangerous blood levels
Renal failure
Other Techniques to Enhance Poison Elimination
Chelation
For elimination of heavy metals (deferoxamine, DMSA, BAL, EDTA)
Hyperbaric oxygenation
Can help to remove CO: consider for CO levels > 25%, LOC, pregnancy
Dilution
Only used after corrosive ingestion (acid/alkali)
5 mL/kg water/milk
Do not use for other toxins → may increase absorption
Indications, Contraindications, and Complications of GI Decontamination Procedures
Fundamentals of Poisoning Management
Common Toxidrome’s
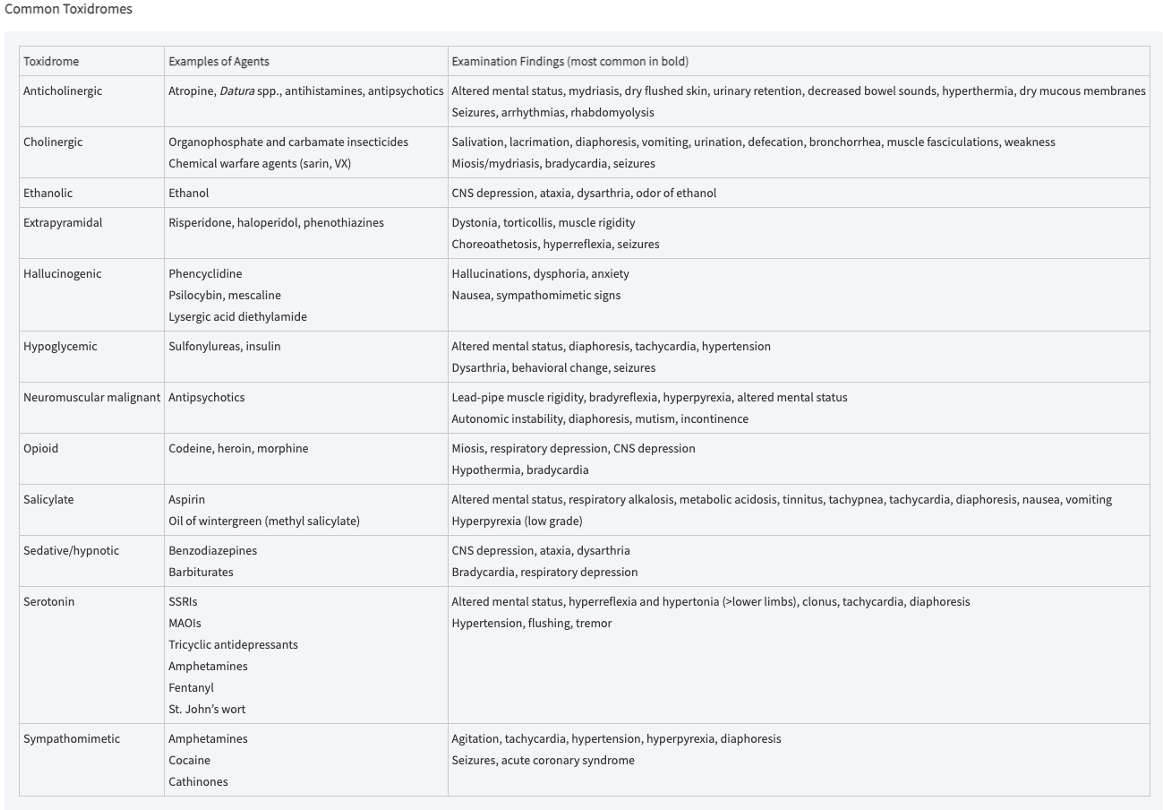
Anticholinergic Common Agents
Four A’s
Antihistamines
Antipsychotics
Antidepressants
Antiparkinsonian drugs
Atropine
Benztropine
Scopolamine
TCAs
Datura (Jimson weed)
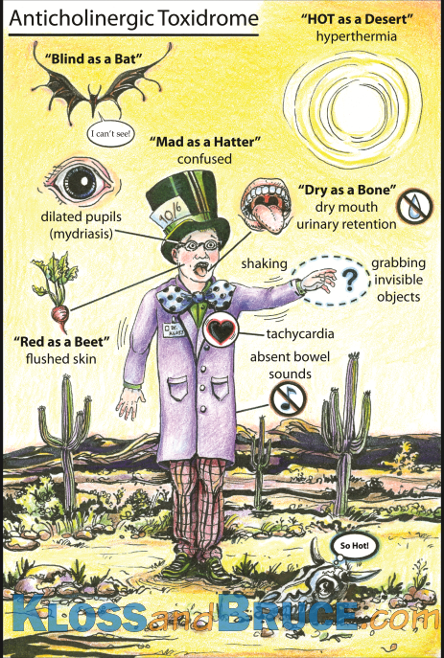
Anticholinergic S/S
Dry, warm, flushed skin
Fever
Dry mouth
Decreased bowel sounds, ileus
Urinary retention
Sinus tachycardia
Mydriasis/blurred vision
Delirium, restlessness, hallucinations → coma, psychosis, seizures
Mad as a hatter, dry as a bone, red as a beet, blind as a bat, hot as a hare, seizing like a squirrel
Anticholinergic Treatment
Benzodiazepines → first line for agitation
Physostigmine if benzodiazepines ineffective → inhibits acetylcholinesterase and more ACh competes for blocked receptors
Cooling measures
Cholinergic Agents and Mechanism
Agents
Organophosphates (malathion, diazinon)
Carbamates
Nerve agents
Some mushrooms
Absorbed via inhalation, gut, skin, mucous membranes: inhibits cholinesterase → excess ACh at muscarinic and nicotinic receptors
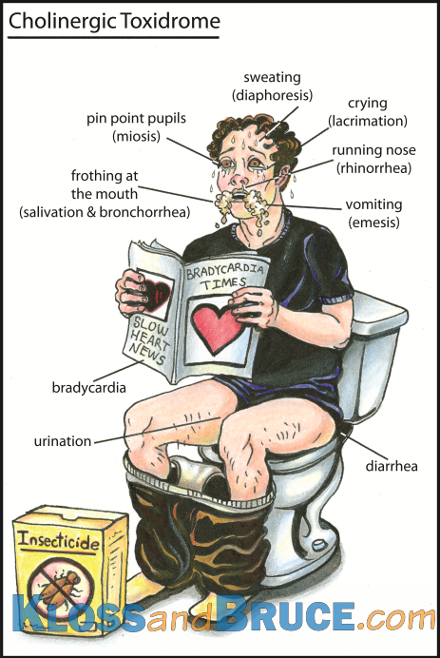
Cholinergic S/S
SLUDGE
Salivation
Lacrimation
Urination
Defecation
GI distress
Emesis
Killer B’s
Bradycardia
Bronchorrhea
Bronchospasm
Cholinergic Treatment
Decontamination: brush dry chemical before irrigation
Airway management
Activated charcoal
IV fluids
Atropine and 2-PAM (pralidoxime)
Atropine
Excellent BBB penetration
Dries secretions
Does not reverse paralysis
2-PAM
Reactivates AChE → reverses respiratory muscle paralysis
Poor BBB penetration
Both are needed → each covers what the other cannot
Sympathomimetic Agents
Cocaine
Amphetamines
MDMA
Methamphetmaine
Ephedrine
Pseudoephedrine
Sympathomimetic S/S
Anxiety
Agitation
Paranoia
Diaphoresis
Hyper-reflexia
Mydriasis
Piloerection
Distinguished from anticholinergics by:
Hyperactive bowel sounds and diaphoresis
Complications
HTN
Tachycardia
ICH
MI
Aortic dissection
Rhabdomyolysis
Sympathomimetic Treatment
Supportive measures: sedation with benzodiazepines, cooling
NO BB: unopposed alpha → HTN crisis
Cocaine ACLS modification
Increase epinephrine interval to 15-10 minutes
Avoid high dose epinephrine
Consider withholding in refractory V-fib
Sympathomimetic Clinical Pearl
Cocaine prevents NE re-uptake → giving exogenous epinephrine may worsen catecholamine excess
In cocaine overdose with V-fib, consider catecholamine excess as the cause before giving more epinephrine
TCA Mechanisms of Toxicity
Antihistamine → CNS sedation/coma
Antimuscarinic → anticholinergic syndrome (dry, tachycardic, confused)
Alpha adrenergic blockade → orthostatic hypotension
Na+ channel blockade
Widened QTS
Conduction delays
Contractility decreased
K+ channel blockade → QT prolongation
GABA antagonism → seizures
Serotonin uptake inhibition → serotonin syndrome
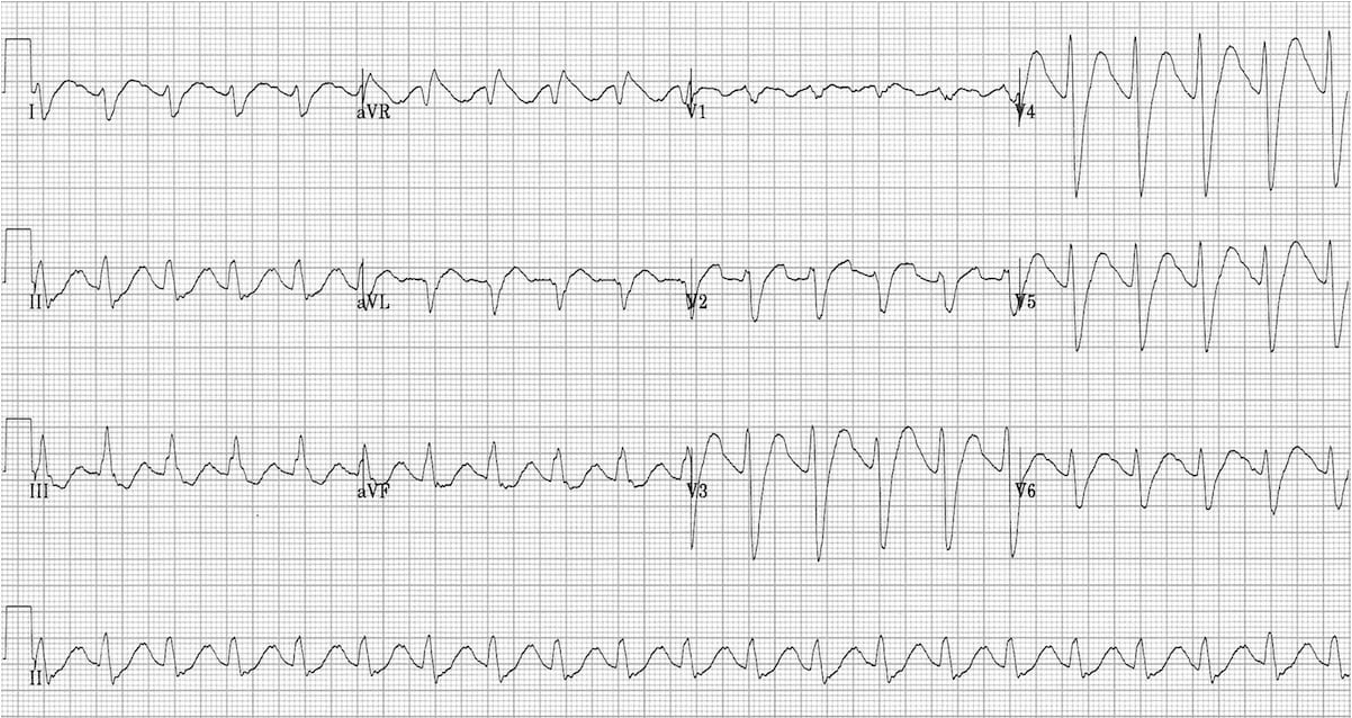
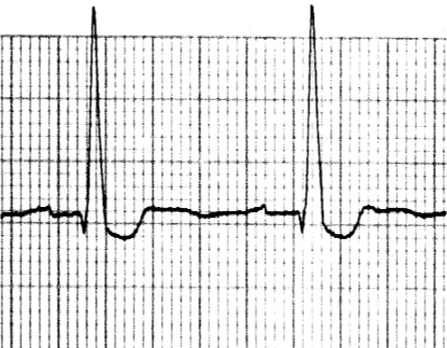
TCA EKG Changes
Sinus tachycardia
Rightward axis
Prolonged PR and QT
Widened QRS → worsens as toxicity increases
Terminal R wave (right bundle affected > left bundle)
TCA Treatment
Sodium bicarbonate
1-2 mEq/kg bolus → drip
Use if:
QRS > 100 ms
Rightward axis > 120 degrees
Hypotension
Benzodiazepines for seizures
Charcoal if alert
Dialysis ineffective due to large Vd
Antiarrhythmics contraindicated → can worsen dysrhythmias
MAOIs
Inhibits MAO → increase storage/release of epinephrine, NE, dopamine, serotonin, and tyramine
Tyramine reaction
Occurs when taking MAOIs with aged cheese, preserved meats, chianti wine, fava beans)
Causes severe HTN crisis
Treat tyramine crisis with phentolamine (alpha blocker) or nitroprusside
SSRIs
S/S
GI side effects (most common)
Sedation
Tremor
Tachycardia
QT prolongation and seizures → rare
Treatment
Supportive
NaHCO3 if QT prolonged
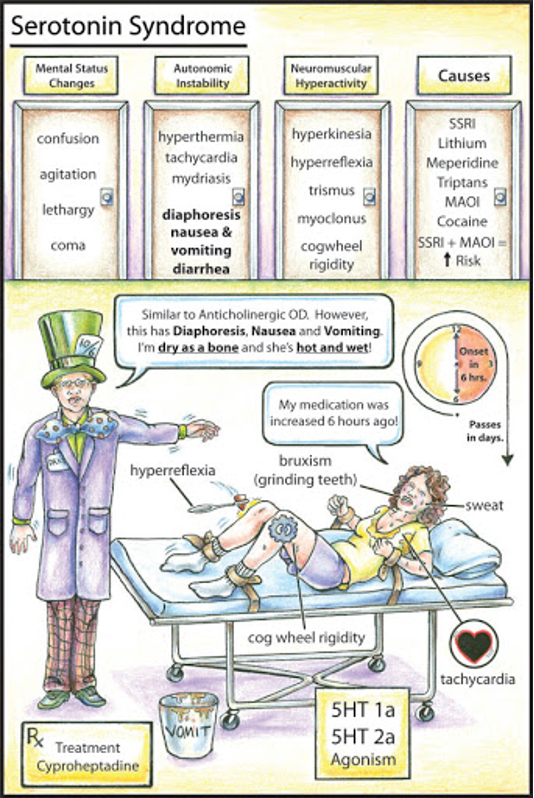
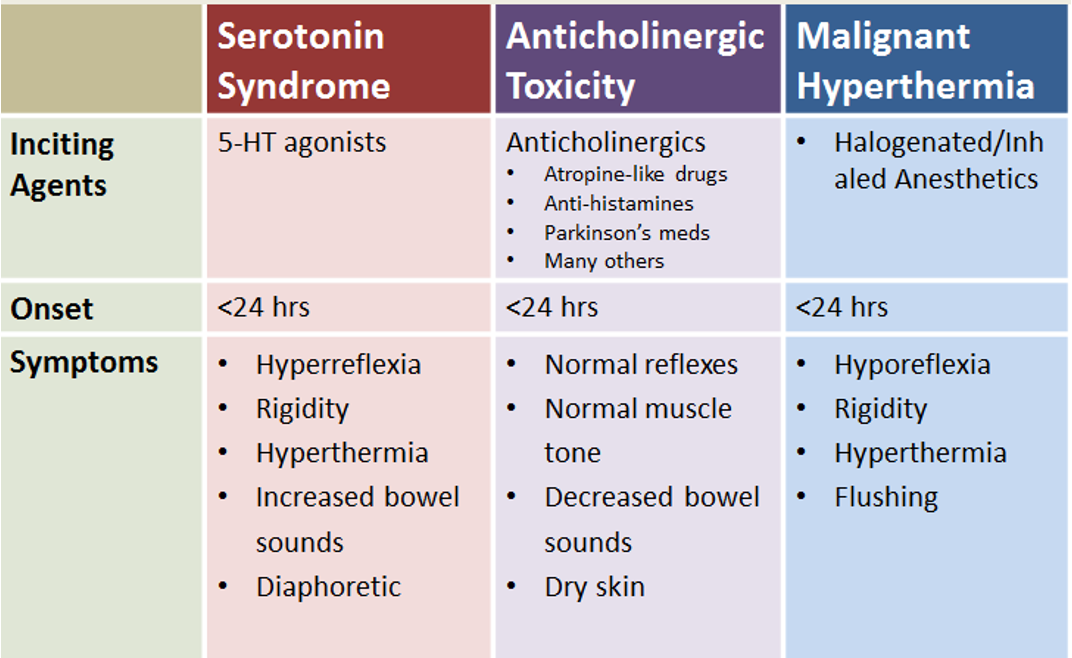
Serotonin Syndrome
Life threatening increase in serotonergic CNS activity from drug interactions, therapeutic use, or intentional OD
Classic triad
Altered mental status
Autonomic hyperactivity
Neuromuscular abnormalities (clonus, hyper-reflexia, lower extremity rigidity)
Treatment
Benzodiazepines for sedation
Cyproheptadine (serotonin antagonist) → more definitive
Serotonin Syndrome vs Anticholinergic Toxicity vs Malignant Hyperthermia
Atypical Antipsychotic Overdose
Less extrapyramidal effect than typicals
S/S
Sedation
Seizures
Temperature instability
Hypotension
Tachycardia
QT prolongation
Watch for NMS even at therapeutic doses
Treatment
Supportive
NaHCO3 if QT prolonged
Magnesium if TdP
NMS Diagnosis
Fever
Altered mental status
Leukocytosis
Tremors
Elevated CPK
Rigidity (lead pipe)
Caused by dopamine receptor blockade or rapid withdrawal of dopaminergic medications
NMS Treatment
Stop the offending agent
Cooling
IV fluids
NaHCO3 infusion
Dantrolene
Stops calcium leak from sarcoplasmic reticulum → controls hyperthermia and rigidity
Bromocriptine
Dopamine agonist to restore dopaminergic tone
Acetaminophen Toxicity Mechanism of Toxicity
Small doses → glucuronidation and sulfation
High doses → CYP450 saturates → NAPQI accumulates → depletes glutathione → covalent binding to hepatocytes → necrosis
Main organ injured → liver (may be fatal and could require transplant)
Acetaminophen 4 Stages of Toxicity
Stage 1 (0-24 hours) → N/V, weakness, fatigue
Stage 2 (24-48 hours) → elevated LFTs, RUQ pain, decreased urine output
Stage 3 (72-96 hours) → liver function disruption, peak toxicity
Stage 4 (4-14 days) → recovery or progressive liver failure
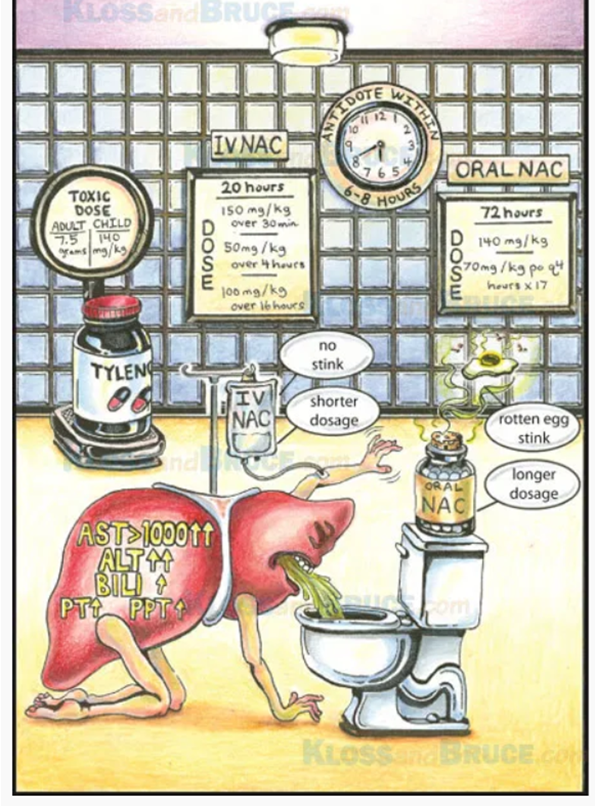
Acetaminophen Toxicity Treatment
Within 1 hour of ingestion and airway intact → activated charcoal
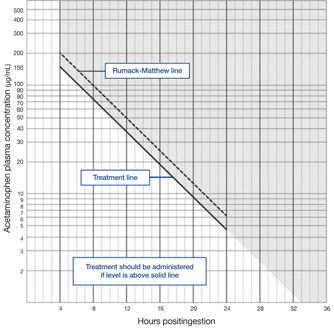
4 hour serum APAP level → Rumack-Matthew nomogram to assess hepatotoxicity risk
NAC (IV preferred)
Replenishes glutathione
Nearly 100% hepatoprotective if given within 8 hours
Monitor APAP levels and LFTs throughout
NSAIDs
More problematic in normal use than in overdose
Ibuprofen < 100 mg/kg usually benign
Ibuprofen > 400 mg/kg very toxic
S/S
Acute (within 4-6 hours) → visual changes, HA, seizures
Hypotension
Bradycardia
Anion gap acidosis
GI upset
Hyperkalemia, hypocalcemia, hypomagnesemia
Patient with borderline renal function → acute renal failure
Treatment
Activated charcoal and supportive care
Salicylates
Primary toxicity → uncouples oxidative phosphorylation
S/S
Early: respiratory alkalosis (from direct CNS stimulation)
Later: metabolic acidosis and respiratory alkalosis
Tinnitus
Hyperthermia
N/V
Altered mental status
Seizures
Treatment
Urinary alkalization (NaHCO3) → ion trapping in urine
If altered mental status, renal failure, serum level > 100 mg/dL → hemodialysis
Avoid acetazolamide → worsens acidemia
Digitalis Mechanism Presentation
Inhibits Na+/K+/ATPase → increase intracellular calcium → increases vagal tone and have bradydysarrhythmias
Narrow therapeutic to toxic margin
Digitalis S/S
Bradycardia
AV block
Frequent PVCs
Multifocal V-tach
Junctional escape
Yellow green halos
Dizziness and weakness
Flu-like symptoms
Toxic hyperkalemia
Digitalis Treatment
If < 2 hours after ingestion → charcoal
Severe bradycardia → atropine and pacing
Ventricular arrhythmia → phenytoin
Definitive treatment → digoxin specific FAB fragments
Sheep derived anti-digoxin antibodies bind free digoxin
Digitalis Key Points
Do not aggressively treat hyperkalemia in digitalis toxicity → Digibind will correct it as Na+/K+ pumps are restored
Slow diffusion and high Vd mean blood level may appear near normal in chronic toxicity
Acutely high levels may not appear very toxic initially → monitor closely
BB Overdose Presentation
Negative inotropy → hypotension
Negative chronotropy → bradycardia
Bronchospasm
Hypoglycemia
QRS widening
CNS: sedation, coma, seizures, psychosis
Sustained release → may delay symptoms 4h+ (toxic time bomb)
BB Overdose Treatment
Activated charcoal within 1-2 hours of ingestion
Trial of atropine (may not work)
Normal saline bolus and IV calcium (increase inotropy)
High dose insulin (100-120 units per hour) and glucose
Overcomes BB interference with insulin → glucose to myocytes
Glucagon
Increase cAMP → increase intracellular calcium → improved contractility
Pre-medicate with anti-emetics (high dose glucagon causes severe N/V)
Lipid emulsion therapy
Lipid sink for highly lipophilic BBs (propranolol)
Catecholamines → epinephrine most effective
Pacing if refractory (do not need long term therapy because drug will eventually be eliminated)
CCB Overdose Presentation
Most deadly cardiac drug → most cardiovascular drug deaths in U.S
Verapamil and diltiazem → bradycardia, hypotension, AV block
More of the heart affects in addition to hypotension
Amlodipine → vasodilation, reflex tachycardia
Does not really work on the heart and more on the vasculature
All can cause:
Complete heart block
Cardiovascular collapse
Hyperglycemia and acidosis (blockade of pancreatic insulin release)
Pulmonary edema
Altered mental status
Onset delayed up to 12 hours with SR formulations
CCB Overdose Treatment
Mainstay → calcium
High dose insulin and glucose
Trial of atropine and 0.9% NS
Glucagon
Adrenergics (epinephrine)
Whole bowel irrigation for sustained release formulation
< 2 hours → charcoal
Gastric lavage considered within 1 hour given high toxicity
Pacing if refractory (do not need long term therapy because drug will eventually be eliminated)
Diuretics Overdose
Thiazides and loop diuretics in overdose can cause:
Hypotension
Hyponatremia, hypokalemia, hypocalcemia
Metabolic acidosis
Mechanism of excreting too much fluid
Treatment
0.9% NS and electrolyte replacement
Pressors if fluid unresponsive for acute hypotensive phase (NE)
Do frequent labs
Most diuretics last around 12 hours → very self limiting
ACE-I Overdose
S/S
Hypotension
Hyperkalemia
Treatment
Largely supportive
0.9% NS
Pressors if needed
Monitor kidney function long term because the can be nephrotoxic
Cyanide Poisoning Mechanism and Sources
Inhibits cytochrome c oxidase → cells cannot use O₂ → anaerobic metabolism → lactic acidosis
Sources:
Combustion of wool/rubber/silk
Industrial use
Apricot/cherry pits
Jewelry manufacturing
Cyanide Poisoning S/S
Headache
HTN
Tachycardia
Seizures
Coma
Bitter almond odor
Pulmonary edema
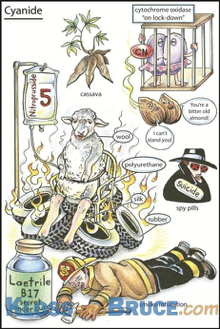
Cyanide Poisoning Treatment
Supportive care + 100% O₂
Three antidote strategies:
Direct cyanide binding — hydroxocobalamin (cyanokit) is 1st line
High dose vitamin B12
Directly binds cyanide → forms cyanocobalamin → renally excreted
May cause transient reddish discoloration of skin, plasma, urine, and mucous membranes — expected and not harmful
Preferred over nitrite/thiosulfate in victims with concomitant CO poisoning (avoids methemoglobin formation)
Methemoglobin induction
Amyl/sodium nitrite (ferric Fe³⁺ binds cyanide)
Sulfur donors
Sodium thiosulfate (rhodanese → thiocyanate)
CO Poisoning Exposure
Leading overall cause of death from poisoning
Poorly ventilated heating systems, confined spaces
Inhaled colorless, odorless gas
Think: groups of people with similar complaints
CO Poisoning S/S
CO has 240× greater affinity for Hgb than O₂ and drastically outcompetes oxygen
Early:
Headache
N/V
Poor concentration
Tachypnea
Progressive: confusion, lethargy, coma
Late: cherry-red skin (unreliable finding)
CO Poisoning Diagnosis
ABG/VBG co-oximetry
SpO₂ unreliable → falsely normal
Pulse oximetry measures the percentage of hemoglobin that is bound to something: can’t differentiate between oxygen and CO
CO Poisoning Treatment
High-flow, high-concentration O₂
Reduces CO half-life from from around ~5 hours (room air) to ~1 hour
Hyperbaric O₂ therapy:
Indications
CO level >25%
Loss of consciousness
Neurologic signs
Pregnancy (due to complications that can arise)
High levels and pressure of oxygen to decrease the half life and eliminate it quicker
Caustic Substance Ingestion Acids vs Alkalis
Acids → coagulation necrosis with significant injury at exposure sites
Alkalis → liquefaction necrosis and allows for tissue transforms to viscous liquid with more wide spread tissue damage
Both can damage mouth, esophagus, and GI tract
Industrial >> household strength
Strong acids may be worse than strong alkalis for GI injury
Caustic Substance Ingestion S/S
Facial burns
Oral/throat pain
Dysphagia, odynophagia
Drooling, dysphonia (damage around vocal cords), hoarseness, stridor (can cause angioedema and localized swelling)
Abdominal pain, N/V
Respiratory distress
Most symptoms from local effects caused by caustic ingestion
Caustic Substance Ingestion Treatment
Safety first
PPE
ABCs because high risk for hoarseness, stridor, dysphonia, and significant local edema → at risk for losing airway
Dilution with water/milk → only thing that we can use dilution for
Caustic skin/eye → copious irrigation
Early endoscopy
Surgical intervention if needed → if they have significant damage and a perforation, need OR for intervention
NO activated charcoal (obscures endoscopy)
NO NG tube (tissue damage risk: may risk creating a perforation)
NO neutralization
Steroids to prevent stricture:
Significant esophageal or tracheal damage and heals → can form strictures
Controversial and likely unhelpful
Hydrocarbon Poisoning Presentation
Gasoline, kerosene, lighter fluid
May be ingested, inhaled, or dermally absorbed (large amount on skin for prolonged period of time)
Pulmonary:
Wheezing
Dyspnea
Hypoxia
Pneumonitis
CNS:
Headache
Dizziness
Slurred speech
Ataxia
Coma
Cardiac dysrhythmias
Peripheral:
Foot/wrist drop
Numbness and tingling
Hydrocarbon Poisoning Treatment
Personal safety + PPE first
Support and ABCs
Decontaminate patient
Nothing by mouth — NO activated charcoal
NEVER induce vomiting — lethal aspiration risk
Aspiration causes severe lung damage — be prepared to manage airway aggressively
Iron Toxicity Presentation
Most ODs in young children → initially asymptomatic but acute cases can be fatal
Moderate toxicity: 20–60 mg/kg elemental iron
Iron toxic to GI tract → GI upset within 6 hours is nearly universal with toxic dose
Five stages of toxicity
GI → apparent recovery → systemic toxicity → hepatic failure → GI scarring
Iron Toxicity Diagnosis
X-ray abdomen → may visualize iron tablets
Negative plain film does not rule out ingestion
Iron Toxicity Treatment
Antiemetics
IV fluids
Deferoxamine
Binds iron → vin rosé urine when active (stop when urine color clears)
Oral for mild toxicity
IV for severe/systemic
Charcoal NOT effective for iron
Gastric lavage <1 hour if toxic ingestion
Whole bowel irrigation can limit absorption
Ethanol Toxicity S/S
Slurred speech
Nystagmus
Disinhibition, CNS depression, poor coordination
Peripheral vasodilation → ↓BP, ↑HR
Level 400–500 mg/dL: fatal respiratory depression (especially for non-drinkers)
Chronic alcoholics may tolerate surprisingly high levels and have no symptoms
Is the most common cause of osmolar gap:
Osmolality = (2×Na+) + (glucose/18) + (BUN/2.8) + (EtOH/4.6)
Ethanol Toxicity Treatment and Work Up
Supportive
D5NS is fluid of choice
Young patients have risk of hypoglycemia
Ethanol does NOT bind to charcoal
Evaluate for co-ingestions, trauma, and infection
Subdural hematoma
Aspiration pneumonia
C-spine injury
Thrombocytopenia
Elimination rate:
Non-drinkers: 15–20 mg/dL/hr
Alcoholics: 25–35 mg/dL/hr (withdrawal symptoms quicker)
Isopropyl Alcohol
Rubbing alcohol: 2× potent and 4× longer than ethanol
Metabolized to acetone — fruity/ketone breath without ↑glucose
Causes osmolar gap but NO anion gap acidosis
GI: hemorrhagic gastritis
Treatment:
Supportive
IV fluids
PPI
Hemodialysis for very large amounts
Methanol
Windshield washer fluid, sterno, moonshine
ADH → formaldehyde → formic acid → inhibit mitochondria
Toxicity develops over 12–30 hours (latent period)
'Snowstorm vision', optic neuritis, blindness
TIME = EYES
Treatment:
Correct acidosis
Fomepizole or ethanol to compete for ADH
Hemodialysis
Folate
Ethylene Glycol
Antifreeze: lethal dose ~2 mL/kg
ADH → glycolic acid + calcium oxalate
Stages
Stage 1 (<12 hours): CNS depression, seizures
Stage 2 (12–24 hours): cardiac toxicity, hypocalcemia
Stage 3 (24–72 hours): acute renal failure, ATN
TIME = KIDNEYS
Treatment:
Calcium gluconate
Fomepizole or ethanol for ADH
Hemodialysis
Pyridoxine + thiamine
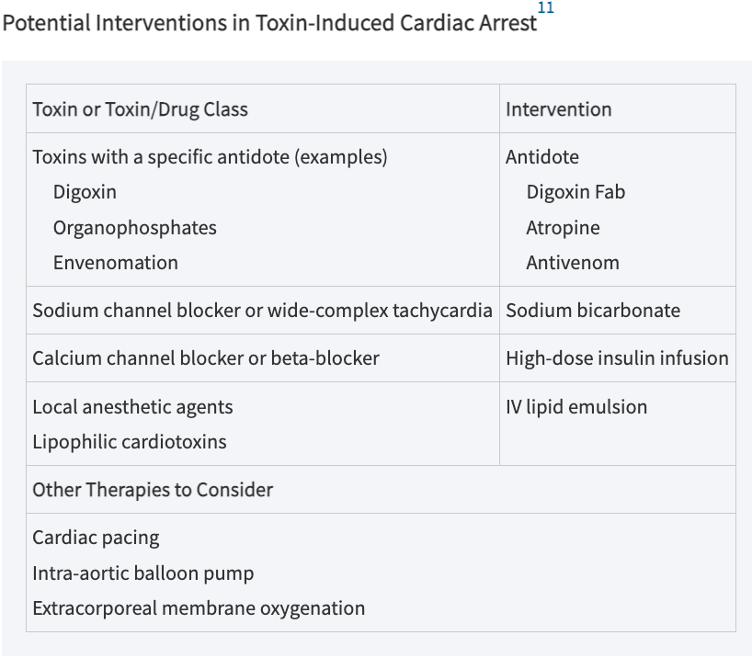
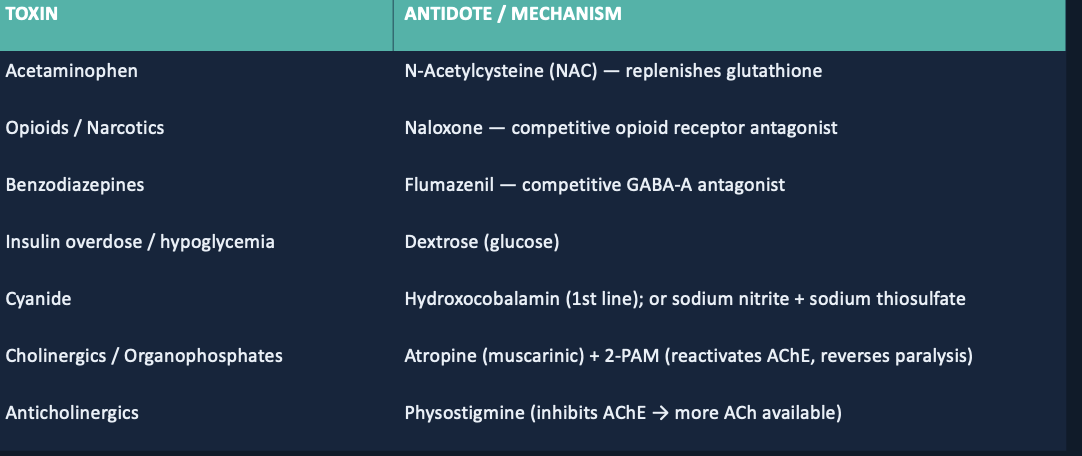
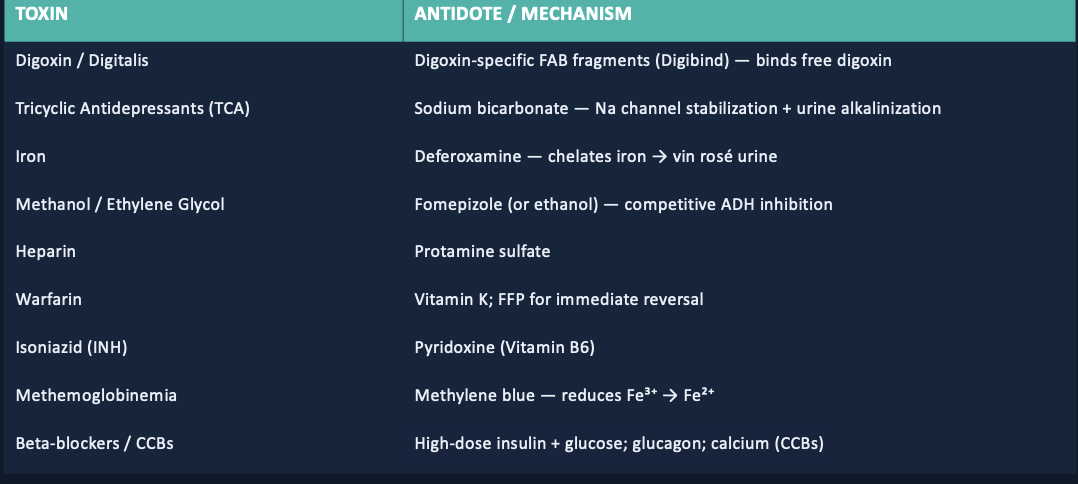
Antidote Pairs
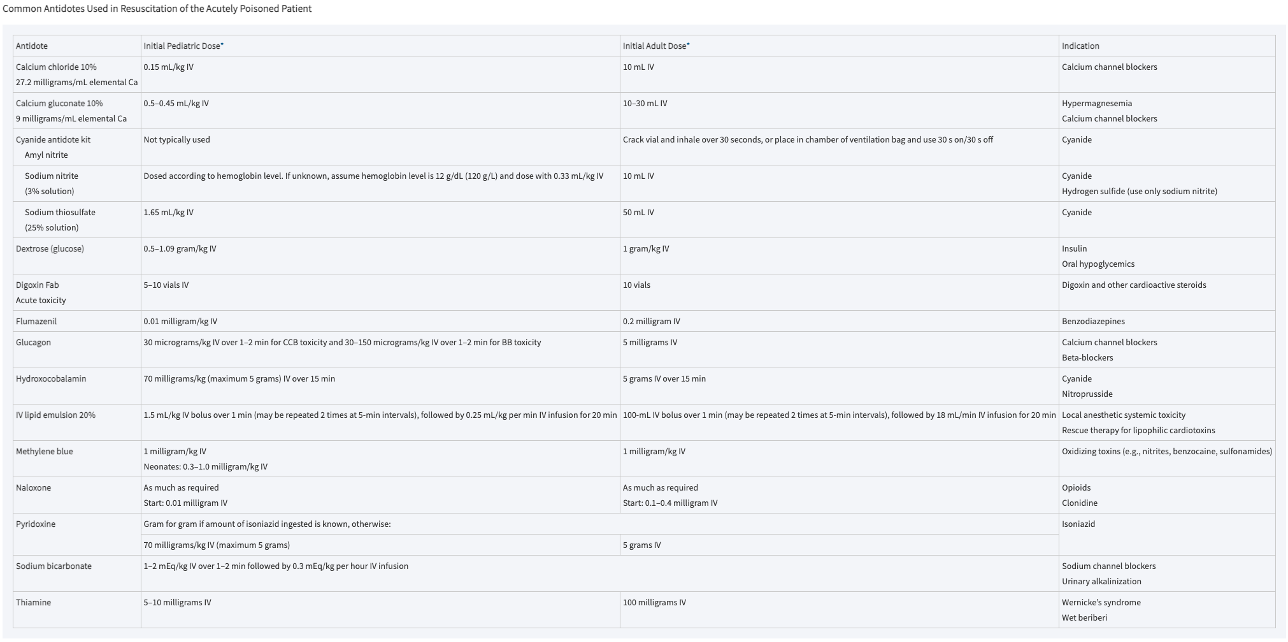
Potential Interventions in Toxin Induced Cardiac Arrest