Complex Patient Management
1/198
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
199 Terms
When should medical imaging be undertaken?
If clinical diagnosis is uncertain
When treatment has failed
Red flags
Guide management
Systematic Approach of an X-ray/Plain radiography
ABCS → Alignment, Bone, Cartilage, Soft tissue
Check patients details → name, side of body, date of xray
Consider clinical info → why do they require an x-ray?
Look at all images available → more than one view/compare
Bone and joint alignment → subluxation, dislocation, fracture
Bone cortex, texture & cortical outline → cortex = whiter
Joint spacing → degeneration
Soft tissue structures → swelling, joint effusion, myositis ossificans
Advantages & Disadvantages of Computed Tomography (CT)
Advantages:
Evaluation of bone and calcification
Can be reconstructed into 3D images
Disadvantages:
High amount of radiation
poor differentiation of soft tissues (muscle vs fat)
Limited ability to detect bone infiltration
Advantages & Disadvantages of Magnetic Resonance Imaging (MRI)
Advantages:
Avoids radiation
Excellence differentiation between tissue types
Useful for identifying red flags
Disadvantages:
Limitation apply to strong magnetic fields (e.g. metals)
Highly sensitive by not always specific
T1 Images → Hyperintensity with FAT
T2 images → Hyperextensibility with WATER and FAT
Contrast images → gadolinium contrast highlights tears
What are 7 core problems within a complex patient?
P M B M D N M
Pain
Muscle strength and ROM
Balance
Muscle length
Decreased exercise tolerance
Neurological
Mental health
What is the AOOTA Classification? (classify orthopaedic fractures and dislocations)
Bone Code (1 digit) – Identifies the bone:
1 = Humerus
2 = Radius/Ulna
3 = Femur
4 = Tibia/Fibula
5 = Hand
6 = Foot
7 = Spine
Segment Code (1 digit) – Identifies bone segment:
1 = Proximal
2 = Diaphysis (mid)
3 = Distal
Fracture Type (letter) – Indicates complexity:
A = Simple (extra-articular)
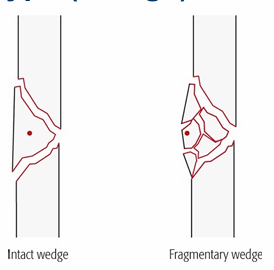
B = Wedge
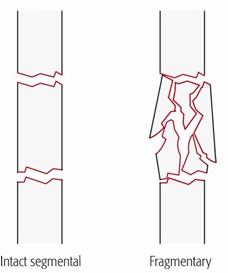
C = Multi-fragmentary
What are the 4 main causes of fractures?
Traumatic, pathological (disease), periprosthetic (mechanical weakness), avulsion (pulling)
Why is fracture classification important?
Ensures standardisation, consistent description, and reflects severity
What are the components of the AO/OTA alphanumeric code?
Bone → Location → Type → Group → Subgroup → Qualifications → Universal modifiers
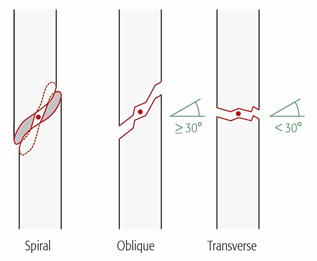
What are the simple fracture groups?
Spiral, Oblique and Transverse
What defines a wedge fracture?
a triangular piece of bone is created, usually because the bone has been compressed from one side; wedge may be intact or fragmentary
What defines a Multi-fragmentary fracture?
Many fracture lines and fragments; previously called “complex.”
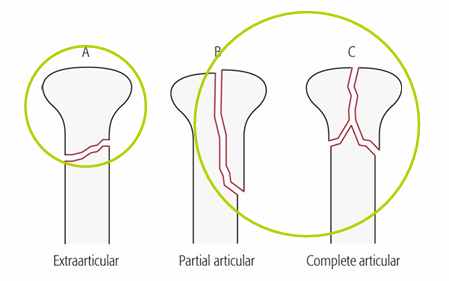
What are the three end‑segment fracture types?
Extra‑articular (A), Partial articular (B), Complete articular (C)
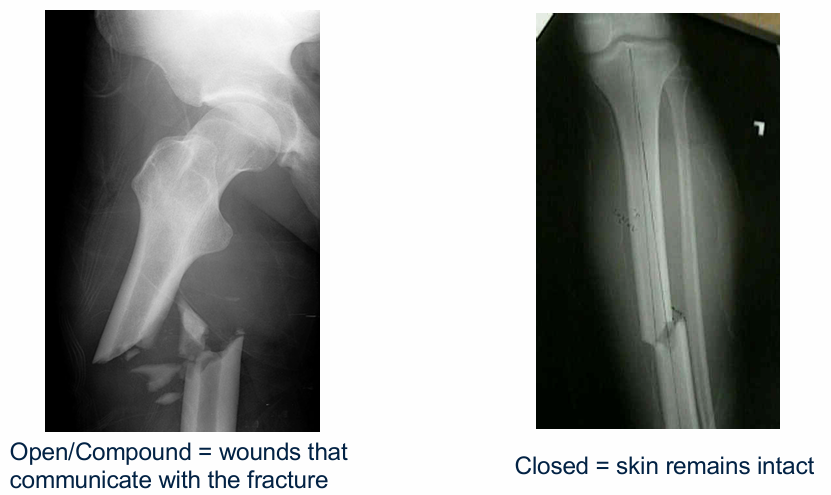
What is the difference between open and closed fractures?
Open fractures communicate with the external environment (e.g. femur poking through the skin)
What is an incomplete fracture?
Cortex not fully broken; includes greenstick, torus, buckle.

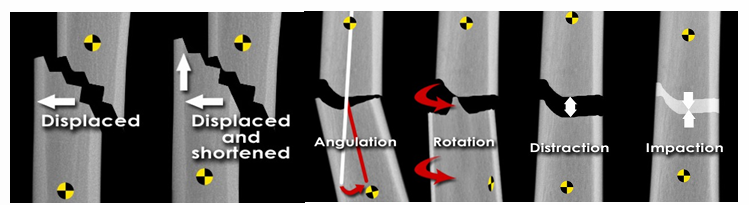
6 types of bone alignment
What is a scaphoid fracture?
What is a Colles fracture?
What is a Monteggia fracture?
What is a Jones fracture?
SF- FOOSH, most common
Colles - Distal radius fracture with dorsal displacement and angulation
Monteggia - Proximal ulna fracture + radial head dislocation
Jones - Fracture of the 5th metatarsal diaphysis
What is a Weber A fracture?
What is a Weber B fracture?
What is a Weber C fracture?
Weber A - Below syndesmosis; usually stable
Weber B - At level of syndesmosis; variable stability
Weber C - Above syndesmosis; unstable; requires ‘ORIF’
What is a Lisfranc injury?
Lisfranc - crush injury, gap between 1st & 2nd prox. MT heads
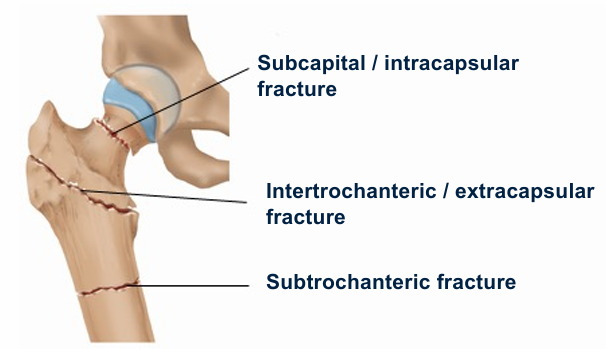
What are the three hip fracture regions?
Subcapital (intracapsular), intertrochanteric, subtrochanteric
Garden Classification System - 1 to 4
1 → Incomplete or impacted # → stable, best outcome
2 → Complete fracture, no displacement → less stable
3 → Complete fracture with partial displacement → unstable
4 → Completely displaced fracture → unstable, highest risk of disrupted blood supply
When is an ankle X‑ray required (Ottawa Rules)?
Pain in malleolar zone
Bony tenderness (medial/lateral)
Inability to weight bear
When is a knee X‑ray required (Ottawa Rules)?
Age ≥55
Inability to bear weight
Inability to flex to 90°
Patella or fibular head tenderness
When is a foot X‑ray required (Ottawa Rules)?
Pain in midfoot
Tenderness at base of 5th MT or navicular
Inability to weight bear.
How are dislocations coded in AO/OTA?
Distal bone number + “0” + region letter + [direction modifier]
What must always be checked after a dislocation?
Neurovascular status + post‑reduction x-rays
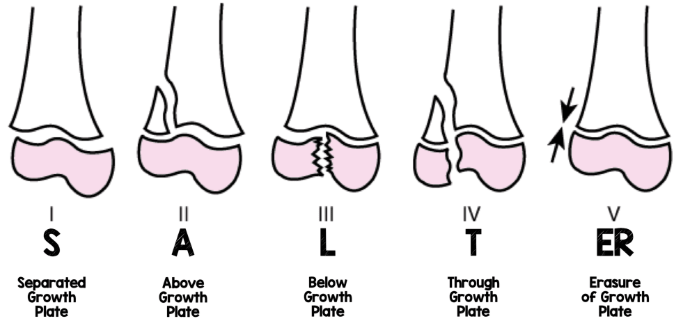
What is a Salter‑Harris II fracture?
Fracture through the growth plate of a child’s bone
What are the 6 core cardiorespiratory problems?
Respiratory failure
Increased work of breathing
Sputum retention
Loss of volume
Pain
Decreased exercise tolerance
What are the steps of the clinical reasoning cycle?
P C P P G A E R
Consider patient → Collect cues → Process info → Identify problems → Establish goals → Take action → Evaluate → Reflect
What information is essential in a pre‑op assessment?
Presenting condition
PMHx
Social & functional history
Investigations
Planned procedure
Special orders
Baseline respiratory status
Pain
What does the pre‑op physical assessment include?
Observation
Palpation
Auscultation
Cough
LL assessment
Special tests
What should be taught pre‑operatively?
Breathing exercises, circulation exercises, supported cough, bed mobility, transfers, post‑op exercises
What subjective info is gathered post‑op?
Pain
Cough
Shortness of breath
PMHx
Smoking
Social/functional history
Nausea
Dizziness
Drowsiness
P&N/numbness
What must be documented post‑treatment?
Distance mobilised
Assistance level
Tolerance
Effect
Adverse events
What problems does physio treat in ortho patients?
Pain
Decreased strength/ROM
Balance issues
Decreased muscle length
Decreased exercise tolerance
Neurological issues
What to look for in a pre-screening of a respiratory assessment?
Cough – Effective? Productive?
Observe RR – Work of breathing
Normal bi-basal expansion
Auscultation - Normal breath sounds
What to look for in a pre-screening of a circulatory assessment - DVT (5)
Commonly seen in the calf and assessed by looking for:
Swelling of the calf
Redness of the calf
Localised pain/tenderness
Increased temperature on palpation
Positive Homan’s sign (calf pain on passive ankle dorsiflexion
What are the 4 cardinal signs of Orthopaedic Musculoskeletal Assessment?
Mobility Level (Independence)
Range of motion
Muscle Strength
Balance
What are the 3 mobility classifications?
Assistance (hands-on)
Supervision (verbal cues only)
Independent
What are the 6 Signs and Symptoms: Post-surgical chest infection
SpO₂ <90% after 2 days
X-ray findings
Temp >38°C after day 1
Productive sputum
Abnormal auscultation
Increased white cell count
What are 3 common post‑op respiratory complications?
Atelectasis (reduced PaO2, FRC, lung compliance)
Chest infection
Hypoxemia
2 types of atelectasis?
Obstructive
Bronchial obstruction occurs and there is progressive collapse of the airways distal to the obstruction.
Non-Obstructive
Compressive (surgery; tumor; pneumothorax; hemothorax; abdominal content weight; pleural effusion)
Passive (loss of negative pressure in pleural space)
Adhesive (loss of pulmonary surfactant)
Cicatrizing (wound that leads to scarring).
What reduces mucociliary clearance?
Medications
Dehydration
High FiO2
Decreased cough
Pollutants
What are the routes of pain relief?
Slower Acting
Oral (paracetamol, tramadol)
Subcutaneous narcotic (morphine)
Intramuscular narcotic (morphine)
Faster Acting
Intravenous - (morphine, fentanyl)
Continuous Acting
Epidural (ropivocaine, fentanyl)
Nerve Block - continuous infusion or local infiltration in theatre
Patient Controlled - Intermittent
Patient Controlled Analgesia - PCA
Operative Anaesthetic
Spinal (wears off 3-4 hours post surgery)
General (associated with respiratory complications - atelectasis…)
Intensive Therapy Unit (sedatives)
Neuromuscular blocking agents
Time to action (5-30minutes) - plan your treatment times around this where possible
What is the physio approach to decreased exercise tolerance?
Early mobilisation
Sit out of bed
Short walks
Self‑care
Exercise testing
Aerobic/anaerobic/strength training
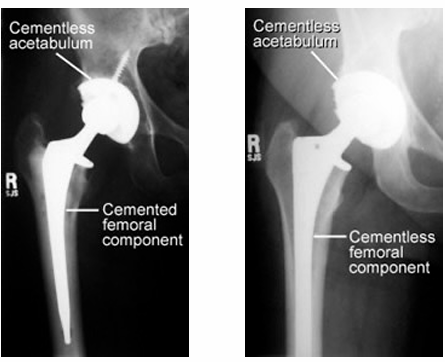
Operation Type - Total Hip Replacement, Prosthesis & Management
Most commonly used prosthesis:
Metal on polyethylene – ball is metal, socket is plastic or plastic lined (polyethylene)
Ceramic on polyethylene – ball is ceramic, socket is plastic or plastic lined (polyethylene)
Ceramic on ceramic - ball is ceramic, socket is ceramic lined
Ceramic on metal - ball is ceramic, socket is metal lined
Day 0 → hip ROM, bridging, bed mobility
Day 1 → mobilize out of bed, rollator
Day 2 → sitting 30 mins initially depending on symptoms
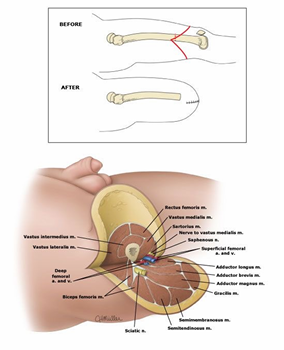
THR - 2 approaches + their advantages/disadvantages and complications
Posterior - Most common, easiest for surgeon
dislocating position - flex more than 90, FADIR
Anterior + Anterolateral - more difficult for surgeon,
dislocating position - forced extension + ADDER
Complications → sciatic nerve damage, DVT, re-dislocation, infection, loosening of components
Operation Type - Birmingham Hip Resurfacing
Femoral head is trimmed and shaped, and covered with a metal cap → preserves patient own bone
Goals: indep. mobility, home exercise program, stairs & car

Operation Type - Arthroscopic Knee Surgery
Performed through small portals to allow an irrigation cannula, a fibre optic viewer and light source, and surgical instruments into the joint.
Meniscectomy: meniscus removed (partially or total)
Meniscal repair: only if located in periphery of meniscus as adequate blood supply for healing
Chondroplasty: removal or repair/smoothing of cartilage
Ligament repair and replacement: e.g. Anterior Cruciate Ligament reconstruction
Arthroscopic Knee Surgery - 3-way patella realignment
Tibial tuberosity transfer
Removing the tibial tuberosity medially
Lateral release
Releases tight lat. retinaculum + vastus lateralis
Medial Plication
folding/tucking/tightening of medial structures
Operation Type - High tibial osteotomy (knee)
Proximal part of the tibia is cut and realigned to change how weight is distributed through the joint.
Factors: under 65, not overweight, 90deg flexion, non-smoker, higher activity level
Total Hip Replacement - Post Op. Management
Day 0 or 1 - hip ROM, quad exercises, bridging, bed mobility as aim, get out of bed on un-affected side
Day 1 Sitting - 30 minutes initially
Day 2 - progress ROM/strength, balance exercises, stairs, car transfers
Operative Type - Total Knee Replacement
Femoral and tibial metal component with a polyethylene spacer
Gold standard for OA patients
Post-op → analgesia, nerve blocks, pain busters
Goals → knee flexion, indep. mobility, single leg reach
Day 0-1 Exercises/Mobility - quad exercises, flee flexion, mobilization, out of bed un-affected side, sitting allowed 30 mins, ice
Operative Type - Uni-compartmental knee replacement
Procedure similar to TKR, however only one compartment is replaced (medial, sometimes lateral or patellofemoral)
other compartments must be healthy
Operative Type - ACL Reconstruction + Indication
Indications: Significant functional disability due to instability
Synthetic grafts (carbon fibre)
Allografts (cadaver tendon donation)
Autografts (hammys tendon)
Operative Type - Toe deformity surgery
Procedure: Osteotomy (cutting & replacing bones) of 1st Metatarsus Valgus
What are 4 examples of fracture complications?
Avascular necrosis
Joint instability
Delayed union of fracture site
Complex Regional Pain Syndrome (CRPS)
Physio role in trauma surgeries? (5)
Joint mobilisation
Exercises
Walking aids
Pain management
Swelling management
Surgical Management - Open Reduction External Fixation (OREF)
Stabilised using an external fixator

4 Causes of Hip Fractures
Simple fall - direct blow to the hip
Trip and fall - rotational force
Spontaneous - pathological
Traumatic fall - MVA, skiing etc
(Displaced) or (Undisplaced)
Clinical Features of a Hip Fracture (displaced vs undisplaced)
Displaced
pain
limb shortened / externally rotated
unable to weight-bear
Un-displaced
pain
no change in limb orientation
can sometimes weight-bear
sometimes difficult to pick up on → Xray
Hip Surgical 4 Management Types
Garden I & II → Cannulated screws (un-displaced)
Garden III & IV → Hemiarthroplasty (displaced)
Intertrochanteric → dynamic//compression/Richards hip screw
Subtrochanteric → pin & plate
1’s or 2’s a pin or screw, 4’s or 3’s a hemi-arthroplasty
Signs and Symptoms of Post-op Delirium
Decreased attention
Disorganized thinking
Irrelevant speech
Disturbed sleep cycle
Disorientation
Memory impairment
Difference between Trauma vs Elective surgeries + management
Trauma surgery is urgent and performed in emergencies, while elective surgery is planned and scheduled in advance for non-urgent medical issues
Trauma Management: Prioritize life over limb, stabilize spine early, prevent complications
Elective Management: Optimize patient before surgery, minimize complications, early rehab, restore QOL
TSJR: Total Shoulder Joint Replacement Indications and Contraindications
Metal ball with stern + plastic socket in same anatomical shoulder layout
Indications:
Affecting sleep or ADLs
Glenoid cartilage degeneration
Post. humeral head subluxation
Contraindications:
Deltoid dysfunction
Active infection
RC arthropathy
Brachial plexus palsy
RTSJR: Reverse Total Shoulder Joint Replacement Indications, Appropriate for and Post-op Physio
Humerus becomes the socket and ball in inserted into the glenoid
Indications:
RC tear arthropathy (joint condition)
Rheumatoid arthritis
3- and 4-part fractures
Appropriate for:
More than 70 years old
sufficient glenoid bone stock
low functional demand
intact axillary nerve
Post-op Physio:
Chest circulation exercises + ice
Mobilize out of bed early
Sling until week 6
No WB through shoulder
PROM flex 90deg, max 120deg → no extension + ER
TSR → needs rotator cuff
RTSR → used when rotator cuff is NOT working
Rotator Cuff Repair
Full vs partial thickness / traumatic vs spontaneous
Candidates: Age, size of tear, limited activity, cooperative
Procedure →
Arthroscopically or open, goal is to reattach good quality tendon to the bone. A grove is created in the normal attachment site and sutures draw the end of the tendon securely into the grove to heal
Post Operation: Day 1 up to 6 weeks
Arm supported in a sling for 6 weeks
Pendulum exercises, scapula stabilization, re-education and pain relief
Post Operation: 6-12 weeks
Pain free arcs, pendulum, abduction active assisted 90deg, IR/ER
Post Operation: 12-16 weeks
Strengthening RC muscles, plyometrics, neuromuscular control, sport-specific activity
Subacromial Decompression (SAD) Indications, Procedure and Post-Op
Indications:
Conservative measures failed
Procedure →
Procedure to increase the space available for structures that pass under the acromial arch
Reshaping of acromion, ligament release, bursa removal etc
Post Operation:
Arm supported in sling but removed ASAP
Day 1: neck/scap/elbow/hand movements, education, icing, no abduction 3-6 weeks depending on Drs orders
Anterior Stabilization/Shoulder Reconstruction Indications, procedure and Post-op
Indications:
Acute dislocation or recurrent instability
Bankart lesion repair OR Hillsachs lesion repair
Procedure:
Bankart → Arthroscopically reattachment of the anterior-inferior labrum to the glenoid
Fixes the cause of instability
Hillsachs → Compression defect in posterolateral humeral head
Fixes the effect of dislocation
Post Operation:
avoid stressing the repaired structures until fibrous healing occurs at 6 weeks.
Day 1 → Active elbow ROM in IR, passive shoulder flexion to 90deg and no ER
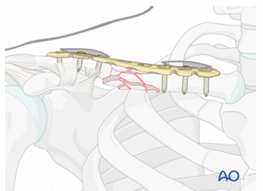
Clavicle ORIF - Compression Plate Indications and Post-OP
Indications:
shortening & displacement more than 2cm
shoulder pathology + neurovascular repairs needed
Post Operation:
Sling 1-2 weeks, NWB 6 weeks, PROM, resistance from 6wks
Humerus ORIF Indications and Post-op
Indications:
Unacceptable deformity or risk of displacement
Post Operation:
Weeks 0 - 3
Immobilization and/or support for 2-3 weeks, pendulum exercises, gently assisted motion, avoid external rotation for first 6 weeks
Weeks 3 -9
Active-assisted forward flexion and abduction, gentle functional use week 3-6, gradually reduce assistance during motion from week 6
Week 9 onwards
Add isotonic, concentric, and eccentric strengthening exercises, treat joint stiffness if any present
Distal Biceps Tendon Repair - Indications and Post-op
Indications:
Biceps tendon avulsion
Young active patients
Needs to be repaired within 3 weeks of injury
Post -Op:
Immobilisation in broad arm sling/full arm cast 6 weeks
Slow return to full range of motion then strengthening at 6 weeks
Olecranon Open Reduction Internal Fixation (ORIF) - Bridge Plate Indications and Post-op
Indications: Unstable displaced #
Post Operation:
Could be immobilized for a couple of days for pain, commence AROM as pain tolerates, resistance exercises commence at 4-6wks after confirmation of healing, nil loading elbow 6-8wks
Radial Head - ORIF or Arthroplasty Indications and Post-Op
Indications: Displaced or unstable # (ORIF) OR Irreparable # (Arthroplasty)
Post Operation:
Could be immobilized for a couple of days for pain, commence AROM as pain tolerate, resistance exercises commence at 4 6wks after confirmation of healing, nil loading elbow 6-8wks
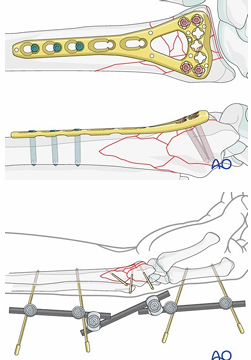
Radial and Ulna shaft ORIF Indications and Post-op
Indications: Displaced closed #’s
Post Operation:
Cast 6 weeks, commence AROM and strengthening post cast removal
Compartment Syndrome Indications and Post-op
Incidence: <30% forearm #s, higher incidence in crush injuries
Procedure: Fasciotomy, often left open for a few days until swelling subsides then repaired
Indications:
Unrelenting, worsening pain more than expected for the injury, numbness and tingling in fingers, colour change of limb, pressure changes in limb
Post Operation: Casting to allow soft tissue to heal
Wrist, Hand & Finger ORIF
WRIST:
Indications: Displaced or comminuted #’s
Post Operation: Cast 6 wks, commence AROM and strengthening post cast removal
HAND/FINGER:
Compression plate simple # + K-wire banding post avulsion #
Carpal Tunnel Release Indications and Post-op
Indications:
Severe carpal tunnel syndrome with sensation loss and pain
Post Operation:
Cast/splint 10-14 days, stitches removed 10-14 days post, gentle ROM commences, pain free movement commence wrist strengthening
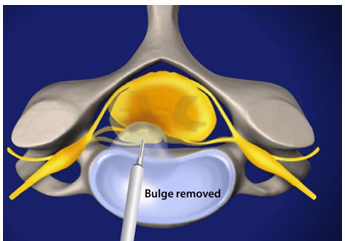
Discectomy/Microdiscectomy Indications, Contraindications and Post-op
Removal of part or complete herniated disc impacting on spinal nerves
Indications:
Spinal Cord compression, Cauda equina, spinal nerve root compression, radiological imaging, failure of non-operative treatments
Contraindications: NIL
Post Operation: Indep mobility, indep ADLs, limited lifting/flexion
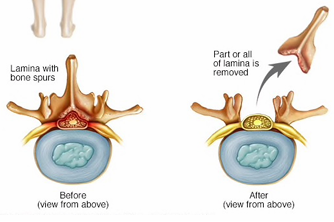
Laminectomy Indications, Contraindications and Post-op
Removal of the lamina to enlarge the spinal canal to relieve pressure on the spinal cord or nerves
Indication: Spinal stenosis or radiculopathy
Contraindications: Instability
Post Operation: Indep mobility, indep ADLs, limited lifting, 70-80% positive outcomes
Complications: Spondylolistheses
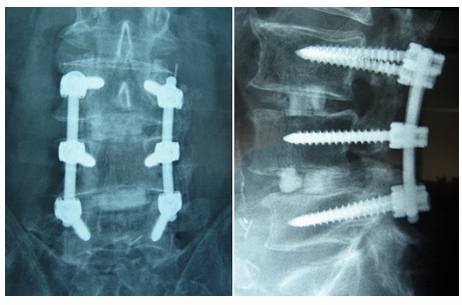
Fusion (Operation) Indications, Contraindications and Post-op
Fuses 2 or more vertebral bodies together, to restrict spinal motion and remove the source of mechanical back pain to relieve symptoms
Indication:
Trauma, tumor, segmental degeneration, spondylolisthesis, spondylolysis, deformity, DDD, recurrent disc herniation
Contraindications: Severe deconditioning/multimorbidity
Post Operation: Indep mobility, indep ADLs, limited lifting
Complications: Pseudoarthrosis (poor/incorrect bone fusion)
Corrective Surgeries + 5 types of procedures
Indication: Fixed deformity, stability of spine is compromised, neurologic deficit
Procedures:
Osteotomy
Decompression
Fusion
Rods – Magec Grow rod, Shilla Procedures
Vertebral body stapling
What to do when you suspect a spinal injury?
Immobilize on rigid board (start spinal rules)
Apply rigid collar
Protection is priority, Detection is secondary
Think about MOI, suspect in all unconscious patients, presence of red flags, beware the “distracting injury"
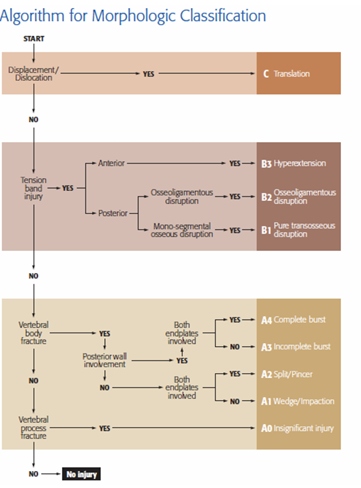
Algorithm to follow if a spinal injury is suspected
→ Displacement/dislocation
→ Tension band injury
→ Vertebral body fracture
→ Vertebral process fracture
Cervical Fracture causation, care + 3 types
Common in: 18–25-year-old males (80%)
Caused by: Head injury, high energy trauma, MVA
Care: Assume & immobilize until cleared, Needs neuro examination
Type A→ Bone injury only
Type B → Tension band/ligamentous injury
Type C → Translation Injury
What are the Canadian C-spine rules?
Age ≥ 65 years
Dangerous mechanism:
Fall > 1 m / 5 stairs
Axial load (e.g. diving)
High-speed MVC, rollover, ejection
Motorized recreational vehicle
Bicycle collision
Paresthesia’s in extremities
What are the 5 Cervical managements?
A0 - Minor injury → stable, conservative management (Soft collar)
A1 - Wedge compression fracture → stable, usually conservative (brace, physio)
A2 - Split (pincer) fracture involving both endplates → potential instability, often still conservative but monitor closely
A3 - Incomplete burst fracture (one endplate + posterior wall) → unstable risk, may need surgery depending on neurology/alignment
A4 - Complete burst fracture (both endplates + posterior wall) → unstable, higher risk to spinal cord → often surgical stabilisation
From A0 → A4, there is increasing structural damage and instability, shifting management from conservative → surgical.
What are the 3 Thoracolumbar Type Classifications?
Type A → Compression Injuries
Type B → Distraction Injuries
Type C → Translation injuries
What are the 3 Subaxial Type Classifications?
Tupe A → Compression Injuries
Type B → Tension Band Injury
Type C → Translation Injuries
Physio management - Braces and Surgery
Braces
usually mobilized WBAT the day of brace application
Lying → standing through side lying
Educate: injury & expectations, warnings re-brace, doning and doffing brace, ADL’s, avoid heavy lifting/jumping/sustained flexion for 6 weeks
Surgery
usually mobilized WBAT Day 1 post-op
lying → standing through side lying and perching is recommended
Educate: injury & expectations, ADL’s, avoid heavy lifting/jumping/sustained flexion for 6 weeks
^ Both require MDT referrals
What are 3 major causes of limb amputation?
Peripheral Vascular Disease
Diabetes
Trauma
What are the 3 amputation types?
Primary → performed as the initial treatment, usually when a limb is severely damaged or diseased (e.g. poor blood supply or infection) and cannot be saved
Secondary → after attempts to preserve the limb have failed (e.g. after surgery or treatment complications), so the limb is removed at a later stage.
Traumatic → Occurs at time of injury
Transtibial Amputation (TTA) technique
Most common = Burgess technique
Posterior flap is made from lateral and medial gastrocnemius and some soleus muscle
Flap fixed anteriorly by sutures
Also referred to as “Below Knee Amputation” (BKA)
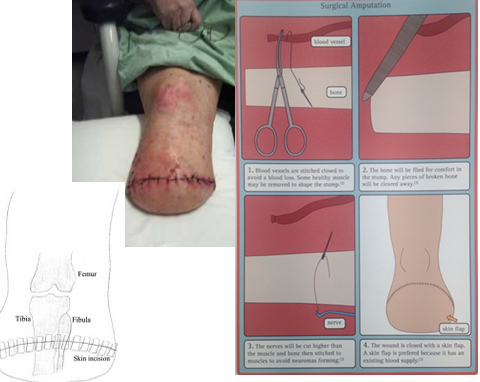
Transfemoral Amputation (TFA) technique
“Fish mouth” incision
Myopexy of posteromedial musculature to shape stump
Scar line sits at the base of the stump
Also referred to as “Above Knee Amputation” (AKA)
Physio acute care Principles of an amputation/stump - Standard + Stump Management
Standard Post-op Care:
Circulation exercises of other limb
Sit out of bed early post-op
Check bloods and vitals
Stump Management:
Suture splitting
Swelling, itching, inflammation
Early prosthetic fitting
Amputation: Stump pain & Phantom pain
Stump Pain → from wound healing, requires good pain control
Phantom Pain → pain that is felt in a limb that has been amputated → 20-50% patients describe it as crushing, toes twisting, burning, tingling, cramping
What are 4 example causes of ongoing stump pain?
Infection
Muscle contractures
Neuromas (nerves cut in operation)
Bony spurs at the cut end of bone
2 Advantages & 2 Disadvantages of Removable Rigid Dressings (RRD) in stump care
Advantages → Reduced oedema and shapes the stump
Disadvantages → Can be heavy & specialist required for application
Needs to be applied in theatre and to be worn for up to 2 weeks (progress to shrinker socks)
2 Advantages & 2 Disadvantages of Bandaging and Shrinker socks in stump care
Advantages → Washable and easy to don/doff
Disadvantages → May slip off and slower healing
Bandaging → 2-4 days post-op once pain allows
Shrinker socks → 7-10 days when conical shape is forming
Bandaging guidelines for Stumps/amputations
Check stump first, dressing over wound
All bandage turns should be diagonal (not spiral) to avoid tourniquet (figure 8 dressing)
Never restrict blood flow = reduced circulation
Should be applied with extended knee
Graduated pressure, firm at end of stump, apply pressure on upwards turns.
Re-apply every 4 hr
No pins to secure, use only tape
Worn 24/7