PHYSIOLOGY UNIT 5
1/30
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
31 Terms
what does the somatosensory system do? 3 pts
the info of different sensations is captured by sensory receptors in the peripheral NS and sent through central pathways to different sensory processing info areas in the central NS
sensory signals begin when info reaches the CNS and sensory info is always encoded as electrical signals
the CNS must be able to identify 4 characteristics of sensory info
what are the four characteristics of sensory info that the CNS must be able to identify? 4 pts
type/nature of stimulus- the type of receptor determines the interpretations of sensory info regardless of the type of stimulus that caused that stiminulation of the receptor due to the receptor-stimulus association
location- encoded by receptive fields
intensity- determined by the frequency of action potentials
intensity- determined by the frequecy of action potentials
duration- encoded by how long the receptor is activated; tonic receptors keep firing as long as the stimulus persists
somatosensory receptors: elements involved? 6 pts
mechanoreceptors- react to mechanical stimuli e.g touch pressure, hearing, balance
thermoreceptors- detect changes in temp
nociceptors- react to painful stimuli e.g. tissue damage
photoreceptors- detect changes in light in the retina
chemoreceptors- detect changes in the chemical molecules in the mouth, nose, and internal fluids
osmoreceptors detect changes in the blood’s osmolarity
somatosensory receptors: location of stimulus? 3 pts
interoceptive receptors- found invisceral organs, blood vessels, etc and provide info regarding the internal envoronment of the body
proprioceptive receptors- found in the muscles, tendons, and joints, respond to stretch, tension, and movement, and generate conscious info about body position and movement
exteroceptive receptors- found in the body surface and are sensitive to stimuli from the external environment e.g. mechanoreceptors, nociceptors, thermoreceptors, photoreceptors
somatosensory receptors: transduction? 4 pts
receptors must encode the stimulus into an electrical signal
the stimulus activates the receptor which changes the membrane permeability to ions (graded potentials) reaching a threshold and triggering an AP in the sensory neuron
stimulus quality is encoded by the type and location of the receptor
stimulus intensity is encoded by the rate of APs and the number of receptors activated (larger receptor area = stronger stimulus)
somatosensory receptors: tonic (slow adapting) receptors? 5 pts
respond to the onset of the stimulus and keep sending signals as long as the stimulus exists
steady and sustain responses throughout the duration of the stimulus
provide spatial and temporal info about the stimulus e.g. size, shape, duration
allow for continous monitoring and adjustment of bodily functions
examples include baroreceptors found in the walls of blood vessels and sense blood pressure, nociceptors that detect pain, and proprioceptors that inform about body position
somatosensory receptors: phasic (rapidly adjusting) receptors? 4 pts
rapid discharge at stimulus onset then silence even if the stimulus persists
inform about changes in stimulation not steady states
adapt to a constant stimulus that decrease in response over time and allow receptors to sense new stimuli/changes in stimuli while filtering out continous stimuli
examples include olfactory receptors that detect olfaction and pancinian receptors involved in touch and vibration
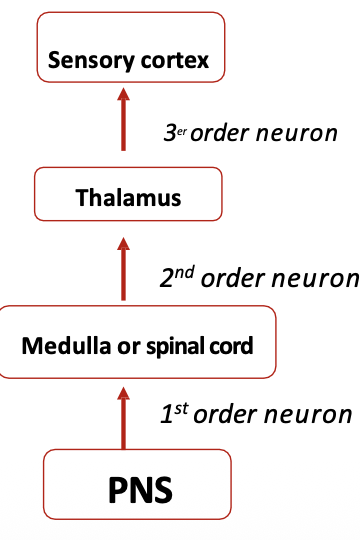
somatosensory receptors: posterior/dorsal column pathway? 4 pts (1st→2nd→3rd from down to up)
involved in fine touch, vibration and proprioception
3rd order neuron has its soma in the thalamus and goes up to the first somatosensory cortical layer also associative cortex
2nd order neuron has its soma in the medulla O, its upper body as the cuneate nucleus and uits lower body as the gracile nucleus, decussates and synapses witth the 3rd order neuron in the thalamus
1st order neuron has its soma in the dorsal root ganglion, has sensory receptors (dendrites)
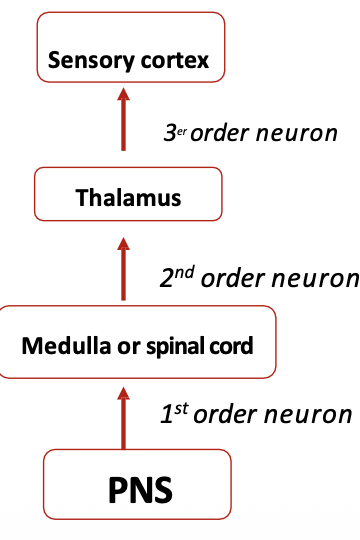
somatosensory receptors: spinothalamic tract? 4 pts (1st→2nd→3rd from down to up)
involved in pain, lateral temp, coarse touch and itching and pain in the anterior
3rd order neuron goes to the somatosensory and association cortex and has its cell body in the thalamus
2nd order neuron has its soma in the doral horn, decussates and synapses with the 3rd order neuron in the thalamus
1st order neuron has somatosensory receptors (dendrites), has its soma in the dorsal ganglion, and synapses with the 2nd order neuton in the spinal cord
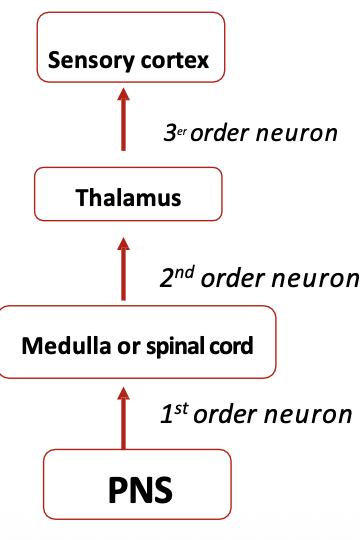
somatosensory receptors: trigeminothalamic tract? 4 pts (1st→2nd→3rd from down to up)
involved in mechanosensitive info of the face
3rd order neuron has its cell body in the thalamus and goes to the somatosensory primary and association cortex
2nd order neuron has its soma in the medulla O, decussates and synapses with the 3rd order neuron in the thalamus
1st order neuron has its soma in the trigeminal ganglion, synapses with the 2nd order neuron in the medulla O, its sensory receptors are in the face
somatosensory receptors: central nervous system (CNS)? 8 pts
1st order neurons collect and transmit sensory info to the CNS
the intergration of sensory info occurs in various structures:
ascending tracts- posterior dorsal and lateral spinal cord tracts
medulla O.
brain stem
thalamus- sensory info except olfactory is classified and directed to corresponding sensory cortex here
sensory cortex- primary and association
cerebellum- receives proprioceptive input for coordination
initial processing of sensory info encoded by the 3rd order neuron (thalamic); primary sensory areas (primary somatosnesory cortex, visual, auditory, insular cortex. and olfactory bulbs
interpretation of sensory info; association areas adjacent to primary sensory areas (auditory. visual, somatosensory)
primary somatosensory map (S1)? 3 pts
responsible for receiving the bulk of somatosensory inputs including touch, temp, vibration, pressure, and pain
second somatosensory cortex intergrates bilateral sensory input involved in tactil learning, object recognition by touch, and sensory memory
pathway- primary somatosensory cortex→ secondary somatosensory cortex→ projection areas e.g. amygdala or hippocampus
information intergration? 4 pts
sensory info is transformed into perception
the perceived stimulus is often different from the actual stimulus
our telencephalon is capable of filling in the info missing to create a complete picture, or transmlate a 2D drawing into a 3D shape
we perceive what our brain expects us to
cerebrum: synesthesia? 1 pt
a neurological condition in which stimulation of one sensory or cognitive pathway leads to automatic involuntary experiences in a second sensory or cognitive pathway
hypothesis behind what accounts for synesthesia? 1 pt
increased cross-talk between associative cortex areas specialized for different functions
cerebrum:disconnection syndromes?
syndromes that arise from damage or disruption in the associative areas of the brain
associative visual agnosia- impairment in recognition of objects caused by damage to the ventral (what) pathway
propospagnosia- impairment in recognizing people’s faces caused by damage or disconnection in the cortical region involved in face recognition
Alexia- not understanding written language depsite knowing how to read and seeing the letters
akinetopsia- inability to perceive motion
auditory agnosias- problem in the recognition of the auditory info that may affect environmental sounds
speech deafness- sounds are heard but meaning cannot be processed
amusia- affects musical perception and interpretation
musical amnesia- no recognition of songs and sounds
musical Alexia- inability to read music
musical apraxia= inability to play an instrument that was priorly known
somatosensory receptors: dermatome? 1 pt
areas of skin innervated by a spingle spinal nerve from a single dorsal root ganglion neuron that overlap so that injury to a dorsal root nerve does not result in complete loss of sensation in the area
sensory receptors: structure? 3 pts
neuron with free endings directly innervate the receptive field, conduct info such as coarse touch, temp, pain, and can be tonic or phasic
neurons with encapsulated endings are wrapped by a capsule of connective tissue that increases sensitivity (myelin)
specialized cell e.g. hair cells from the ear can be myelinated or non-myelinated
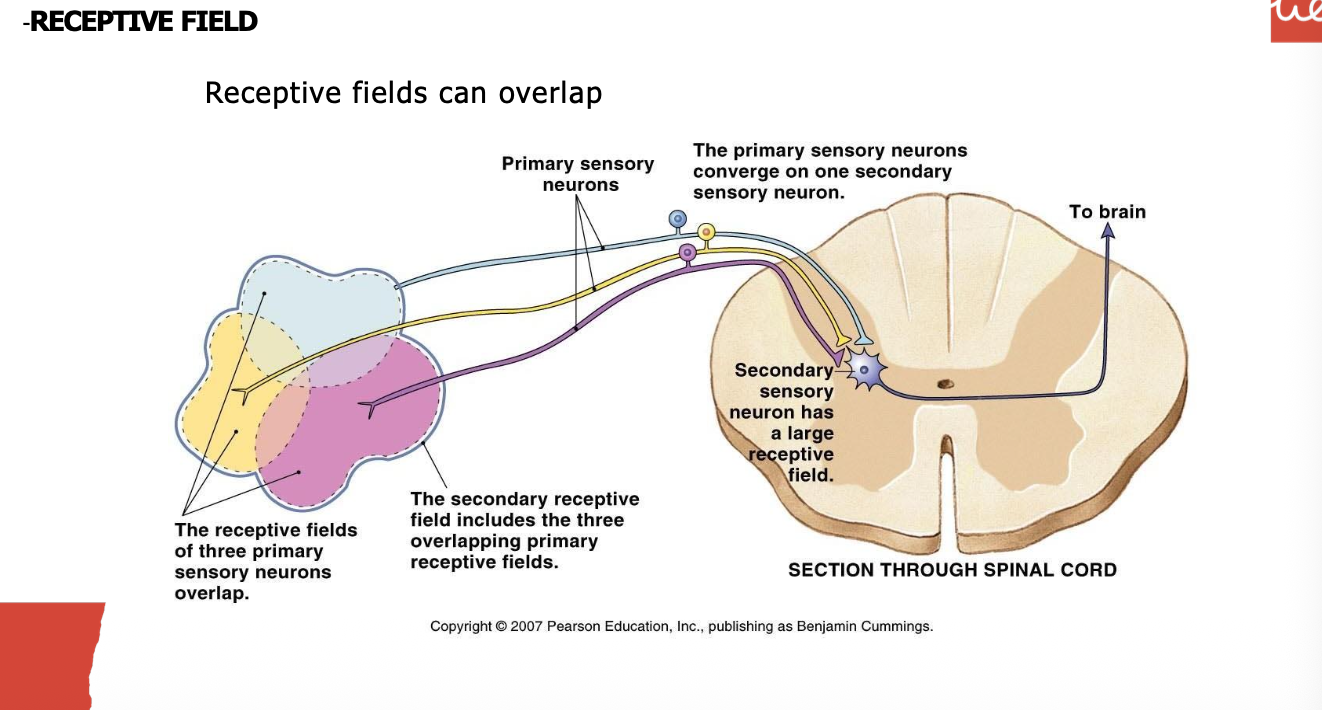
sensory receptors: receptive field? 6 pts
areas of the body that when stimulated activate the 1st order sensory neuron
individual receptive fields in close proximity can merge into a single large secondary receptive field
small receptive fields are found in more sensitive areas and secondary receptive fields are much smaller when there is less convergence
the diameter of the primary receptive field determines the sensitivity and ability of spatial discrimination; smaller receptive fields = higher densitiy of receptors= greater discrimination
lateral inhibition- increased stimulus precision through the inhibiton of neighbouring fields which focuses stimulation on the receptors found in the center of the field increasing the resolution and enhancing perception of the stimulus (used to sharpen the signal)
receptive fields in the finger overlap but info in the cortex is segregated
sensory receptors: touch and pressure encapsulated skin receptors? 10 pts
A. meissner corpuscles:
rapidly adaptive receptors (phasic, detect changes in the stimulus)
small receptive fields (high spatial resolution)
40% of the innervation of the hand
very sensitive to initial touch and the movement of very light objects on the skin
B. merkel cells:
slowly adapting receptors (tonic, spatial info from the stimulus)
very small receptive fields (very high spatial resolution)
free endings found in the epidermis
20% of the innervation of the hand
detect continous stimuli and are related to the static discrimination of shapes, edges, and textures
C. ruffini corpuscles:
slowly adapting receptors (tonic spatial info from the stimulus)
detect steady changes in skin shape e.g. skin stretching
D. pacinian corpuscles:
rapid adaptive receptors that detect changes in the stimulus
very large receptive fields e.g. entire finger (very low spatial resolution)
10-15% of the innervation of the hand
located deep in the dermis
insensitive to light touch but very sensitve to vibration and rapid changes in pressure e.g. when picking up and object
sensory processing: thermoreception? 6 pts
thermoreceptors are usually free endings with small receptive fields
activated by cold- temps below body temp; no longer stimulated if the skin in under 5 degrees
activated by heat- beyond 45 degrees nociceptors take cotnrol to avoid damage to the skin and underlying tissues
thermoreceptors are widely distributed through the skin btu are also in the hypothalamus and spinal cord to detect body temp
heat receptors start perceiving high temp when the skin surface rises above 30 and are most stimulated at 45 degrees; beyond this pain receptors take control
cold receptors start perceiving loq remp when the skin surface drops below 35 and are most stimulated when the skin surface is at 25 degrees; no longer stimulated below 5 dehrees
sensory processing: pain? 4 pts
perception of pain has specfic pathways and receptors
nociceptors- sensory afferents responsible for transmitting pain and have free nerve endings
equal at different temperatures after the pain threshold is surpassed (45 degrees)
increase of the number and frequency of APs with temp over 45 degrees
pain? 5 pts
can be separated into an early perception of first sharp pain and second a later duller and burning sensation
Ab fibers:
early perception of acute pain
small myelinated fibers
phasic/rapidly adjusting
mechanosensitive and mechanothermal
C fibers:
more diffuse and burning sensation
small unmyelinated fibers
tonic/slow adapting
polymodal nociceptors- mechanical thermal chemical
pain modulation: pain gate theory? 3 pts
transmission of nerve impulses from affernt fibers to 2nd order neurons in the spinal cord is modulated by a gating mechanism in the dorsal horns
activation of mechanoreceptors modulates the transmission of nociceptive info to higher centers
interaction in the local circuits of the dorsal horn reduce the sensation of sharp pain
pain modulation: descending pathway and local circuits? 3 pts
in higher nuclei (periaqueductal gray, raphe nucleus, locus coeruleus) there are descending neurons that modulate/inhibit active neurons in the dorsal horn of the spinal cord
these neurons activate local circuits and cause the release of inhibitory molecules that modulate the pain signal decreasing it
pain modulators- enkephalins, endorphins, dynorphin, cannabinoids, norepinephrine, serotonin
pain processing: alterations? 7 pts
peripheral sensitization- activation thershold of the peripheral nociceptor is lowered by the nociceptor itself through inflammatory molecules in the tissue causing pain to be perceived with greater intensity after and injury
central sensitization- occurs due to an excitability of 2nd order neurons in the dorsal horn of the spinal cord
hyperalgesia- exaggerated pain response to a normally painful stimulus due to sensitization
allodynia- induction of pain by an innocuous stimulus/in the absence of a stimulus often dur to central sensitization
neuropathic pain- occurs when both peripheral and central sensitization persist after an injury heals
paresthesia/dysesthesia- abnormal sensation e.g. tingling burning or itching in reponse to touch than can be central or peripheral
phantom limb syndrom- sensory perceptions in a limb that has been amputated
causes of phantom limb syndrome? 4 pts
reorganization of the somatosensory cortex
activity in adjacent areas activates neurons priorly represnting the lost limn
interpreted by the brain as sensations in the missing limn
CNS origin and usually disappears afterr the reorganization of the circuits (plasticity)
what is referred pain? 1 pt
pain perceived in the skin or muscle even though the source is visceral e.g. heat pain being perceived as skin pain in the left arm and chest for men or in the jaw or back for women
how does referred pain occur? 1 pt
visceral nociceptors share the same dorsal root ganglion and segment of the spinal cord with the fibers that come from skin nociceptors which causes the brain to misinterpret the pain as coming form the skin
parallel pathways of pain? 2 pts
response to pain is multifactorial
sensory discriminative aspects- processing of sensory info
affective motivational aspects- unpleasant feeling, fear, anxiety, autonomic activation
sensory processing: proprioception? 3 pts
mechanoreceptors that provide info about the position of the limbs and other parts of the body in space
golgi tendon organ- detects changes in muscle tension
muscle spindles- detects changes in muscle length