Treatment of feeding and swallowing difficulties in infants and children
1/46
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
47 Terms
Setting therapy goals
effective interventions need to target the cause of the problem (think about providing compensatory strategies but it’s most important to get rid of the root of the problem)
a thorough assessment is required to guide intervention
once the nature of the problem has been established, the treatment plan can be developed
Models of service delivery
providing therapy in different ways for different clients
Service delivery: location of services
inpatient: don’t get the patient for long, most important to make sure they have psychogically ability
outpaitent: client comes and sees the SLP
Service delivery: primary recipient of input
child: can work one-on-one w/ the child
parent or caregiver: parents can provide care for children
staff (eg. hospital, daycare, school)
Problem with parent or caregiver giving the intervention
sometimes kids don’t respond to their parents during intervention
Service delivery: members involved in sessions
individual: more attention on one client
group: social behavior learning, may not work for every child
Service delivery: frequency of sessions
Weekly or intermittently
intensive
consult only
Pediatric therapy focuses: swallowing and airway protections
thickened fluids
positioning
feeding equipment
pacing
modified foods
Pediatric therapy focuses: feeding and mealtime behavior
oral sensory-motor therapy
feeding utensils and equipment
behavioral feeding therapy
Use of thickened fluids
improves swallowing and airway protection
children with swallowing problems (dysphagia)
a. to slow the rate of fluid flow, thereby allowing more time to close the airway prior to the swallow. - flow rate will decrease
b. thickened fluids “hold together” better than thin fluids so are easier to control in the mouth
infants who display regurgitation
rational: thickened feeds may be less likely to be regurgitated from the stomach back to the esophagus
Considerations regarding thickening fluids
too thin → increased risk of aspiration
too thick → increased work of breathing → increased fatigue
Factors affecting the thickness of thickened fluids
type of thickening agent: 2 main types starch based and gum based
type of base fluid: water vs. milk vs. juice
amount of base fluid: how much base fluid vs. amount of thickener is not linear
temperature: get thicker at cooler temperature, stay thinner when warmer
standing time: overall fluids get ticker w/ time, don’t prep way ahead of time (even like 10 minutes)
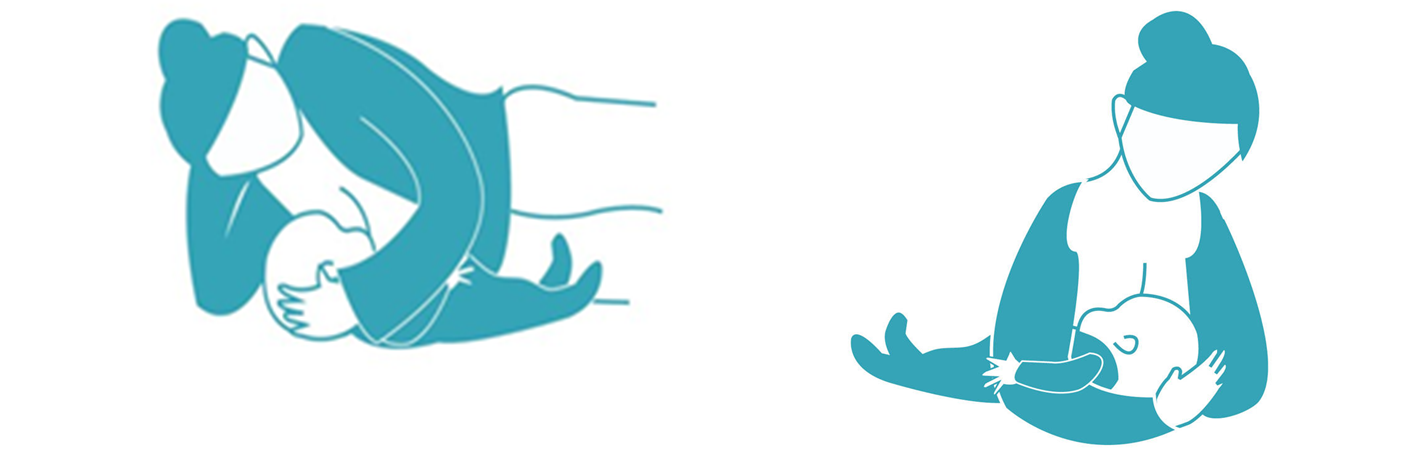
Positioning while breast feeding
because of the effects of gravity, fluids flow faster vertically than horizontally
positioning an infant in a more upright position versus a reclined supine position can slow the flow of feeds.
Position images

faster b/c of more angled milk jumps back of throat quicker

slower
Positioning laying down
by positioning a infant side-lying position versus a supine position may also SLOW the flow of feeds
for older children, encouraging a chin-tuck position for airway protection and avoiding neck extension while drinking can slow the flow of drinks
feeding equipment for infants
aim: to slow the flow of fluids
for infants:
-slow-flow nipples: one hole, give more reaction time
-nondrip nipples: as soon as they stop sucking there’s no drip
feeding infants: for older children
slow the flow of fluids
-straw
-cut-out cups
Pacing
intentionally slowing things down during feeding by imposing breaks during feeding and drinking to interrupt the flow of fluids
Pacing for infants
for infants: the feeder may actively impose breaks to allow the child to swallow and catch his or her breath
Pacing for older children
it can be done based on infant cues or on a schedule
may prompt the child to take a break from drinking by using verbal cues or by manually controlling the cup
Swallowing Maneuvers
many of the therapeutic strategies used with adults may not be possible with young children
Main reason: they do not have the cognitive skills to understand or follow detailed instructions or the self-awareness to voluntarily control movement of anatomic structures
Some therapeutic strategies may be possible to elicit with positioning change or modeling (chin tuck, head turn)
generalization is limited
Modified foods
by 2 to 3 years of age, most children have the oral skills to eat most solid foods
some children with developmental delay and neurologic impairment may require modified food textures beyond this age
- special considerations:
developing motor skills
developing cognitive ability
Oral Sensory-Motor Therapy (OSM)
Aim: to modify the child’s current oral motor skills and sensory processing ability in relation to eating and drinking
mostly applied for preterm infants
insufficient evidence exists regarding the effectiveness of OSM therapy
Example of commercial OSM programs: MORE program, the beckman protocol, and the Talk Tools approach
The main criticism: lack of specificity in OSM programs
Feeding utensils and equipment
Easier for younger kids than older kids
a variety of feeding utensils and equipment are available commercially
special feeding equipment:
teething toys
oral stimulation toys (pacifiers, teething rings, gum brushes, vibrating oral toys)
mouth toys (tubing for chewing, bite blocks, tongue depressors, oral blow toys)
Shape of nipple: Normal vs. Orthodontic nipple
orthodontic nipple: requires less muscle strength b/c nipple is thinner
slows rate of overall feed
Flexibility of nipple: latex and silicone
silicone nipple: firmer harder to suck milk
latex nipple: softer and easier to compress, require less effort
Length of nipple: long vs. short
Long: beneficial for cleft palate and reaches further back requiring less work needed
Flow rater: slow, medium, fast nipples
BIGGEST FACTOR
Size and number of holes
faster slow can overwhelm a baby
Slow: recommended: requires more work from child
medium: 3-6 months (6 holes)
fast: 6+ months (9 holes)
Bottle feeding: some nipples are designed for restricted flow
flow type (restricted flow or nondrip nipple)
Pressure release valves: (e.g. one-way valves/tube or air release holes): help them save energy later

Outcome to consider when comparing bottle nipples:
volume taken during bottle feed
duration of bottle feed (minutes)
rate of bottle feed intake (mL per minute or oz per minute)
incidence of physiologic abnormalities during bottle feeds
number of breaks needed during bottle feeds
infants fussing or refusal behaviors during feeds
number of bottle feeds taken per day
time take to transition from first oral bottle feed to exclusive oral feeding
Behavioral Feeding Therapy
Goals:
increasing desirable mealtime behavior
decreasing undesirable mealtime behavior
improving adequacy of dietary intake from food versus supplements
improving dietary variety
maintaining or improving growth
reducing parent stress
Operant Conditioning
Change behavior directly
designed to improve feeding difficulties and increase oral intake through specific prompted food goals and a reinforcement system
top-down driven approach caregiver is guiding the feeding and reinforcing the behavior
take a bite → get a reward
Systematic desensitization
change child’s relationship
designed to improve feeding difficulties and increase oral intake by exposing children to a range of food in play-based activities, which become gradually more challenging
bottom-up, exposure therapy, help child become more comfortable and regulated
learning to self-regulate around food
Operant Conditioning: antecedent Prompt
verbal prompt
visual prompt
physical prompts
Operant conditioning: consequence for desirable behaviors
spontaneous social reinforcement
specific verbal reinforcement
object reinforcement
Operant conditioning: consequences for undesirable behavior
preventing escape
verbal redirect
withholding attention
withholding reward
Operant conditioning: primary outcome measures
volume consumed
reduction of undesirable behaviors
Operant Conditioning: size of group
usually individual, as it is difficult to provide contingent reinforcement to multiple children at once
Systematic Desensitization: Antecedent Prompt
modeling
Systematic Desensitization: consequences for desirable behavior
spontaneous social reinforcement
Systematic Desensitization: consequence for undesirable behavior
withholding attention
verbal redirect, if needed
Systematic desensitization: primary outcome measures
variety (number) of foods consumed, level of interaction with food
Systematic Desensitization: size of group
may be individual
often in group format, extra participants adds to the amount of modeling and spontaneous social reinforcement to which the child is exposed
Measuring therapy outcomes: feeding skills
oral skills
swallow safety
variety of foods texture consumed
variety of food types consumed
number of foods and fluids consumed across key food groups
self-feeding skills
mealtime duration
mealtime behavior
Measuring therapy outcomes: diet
work w/ dieticians
nutritional adequacy from oral diet (overall energy intake, intake of key nutrients)
Measuring therapy outcomes: growth
change in weight
weight for height and body mass index
Measuring therapy outcomes: social factors
parent-child interaction
parent stress
parent satisfaction
child satisfaction