Care of the Critically Ill Neurological Patient
1/32
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
33 Terms
Objectives
Describe the neurological assessment of a critically ill respiratory patient
Recognize and evaluate the major symptoms of neurological dysfunctions occurring in critically ill patients
Understand the diagnostic significance of CSF
Understand and differentiate the different arousal states and their designated outcomes
Key Terms
• Akinetic Mutism
• ALOC
• Brain Death
• Coma
• ICP
• Locked-In Syndrome
• Minimally Conscious State
• Persistent Vegetative State
• Mannitol
Assessment
• Review of Health History
• Review of Lab Data
• Visual Examination
• Physical Examination
• Pg 1976 (14th Ed. )
Assessment: Review of Health History
Events Preceding Onset of Symptoms
◦ Travel? Animal contact? Fall? Infection? Dental Problems? Food/Drugs ingested?
Progression of symptoms
◦ Initial Onset, Evolution of sx, Freq.?, Severity, Duration, Aggravation of sx Family History
◦ Stroke (AVM), DM, HTN, Seizures, Tumor, HA, Psych
Medical History
◦ DM, HTN, CV, Pulm., TB, Tropical Illness,
EARLY INTERVENTION IS KEY TO PREVENT
SECONDARY INJURY
Assessment: Review of Health History cont
Surgical History
◦ Neuro, ENT, Dental and Eye
Traumatic History
◦ MVA, Falls, Blow to head/neck/back, syncope
Allergies
◦ Drug, Food and Environment
Patient Profile
◦ Personal Habits, Illicit drugs, Alcohol, Place of residence, workplace, sleep patterns
Current Medication Use
◦ Nitrates, BP Meds, Herbals, Oral Contraceptives, Sedatives, Anticoagulants
Assessment: Review of the Lab Data CSF
Cerebral Spinal Fluid: Evaluated for 2 purposes
1. ___________________________
2. ___________________________
Normal: clear, colorless, no blood, <200mm H2O pressure, 0-5 WBCs, 50-75 mg/dL glucose, 15-50 mg/dL protein, lactate 10-20 mg/dL
Two life threatening risks associated:
1. Brainstem Herniation
2. Respiratory Arrest d/t
Assessment: Review of the Lab/Diagnostic Data
ABGs: PaCO2 and PaO2
PT, PTT, INR
CBC: Hgb and Hct, RBC, WBC
BMP: TCO2, Sodium, Potassium, LFTs
UA: infection?
CT vs MRI
Assessment: Review of the Visual Assessment
Level of Consciousness
1. Arousal or Alertness: Reticular Activating System and its connection to the thalamus and cerebral cortex
1. Ability to respond to noxious or verbal stimuli
1. Noxious Stimuli: trapezius pinch & Sternal Rub
2. Peripheral Stimulation: Nail bed pressure, Pinching inner arm or leg
2. Awareness
1. Content of consciousness is much more of a higher level of function (6 types)
1. Name, BD, Year, Place
2. Glasgow Coma Scale
Confusion
Impaired judgment and decision making
Disorientation
Disorientation to time, then place, then recognition
of self
Lethargy
Limited spontaneous movement or speech
Obtundation
Mild to moderate reduction in arousal with limited
response to environment
Stupor
condition of deep sleep or unresponsiveness from which the person may be aroused only by vigorous and repeated stimulation
Coma
no verbal response to the external environment or to any stimuli
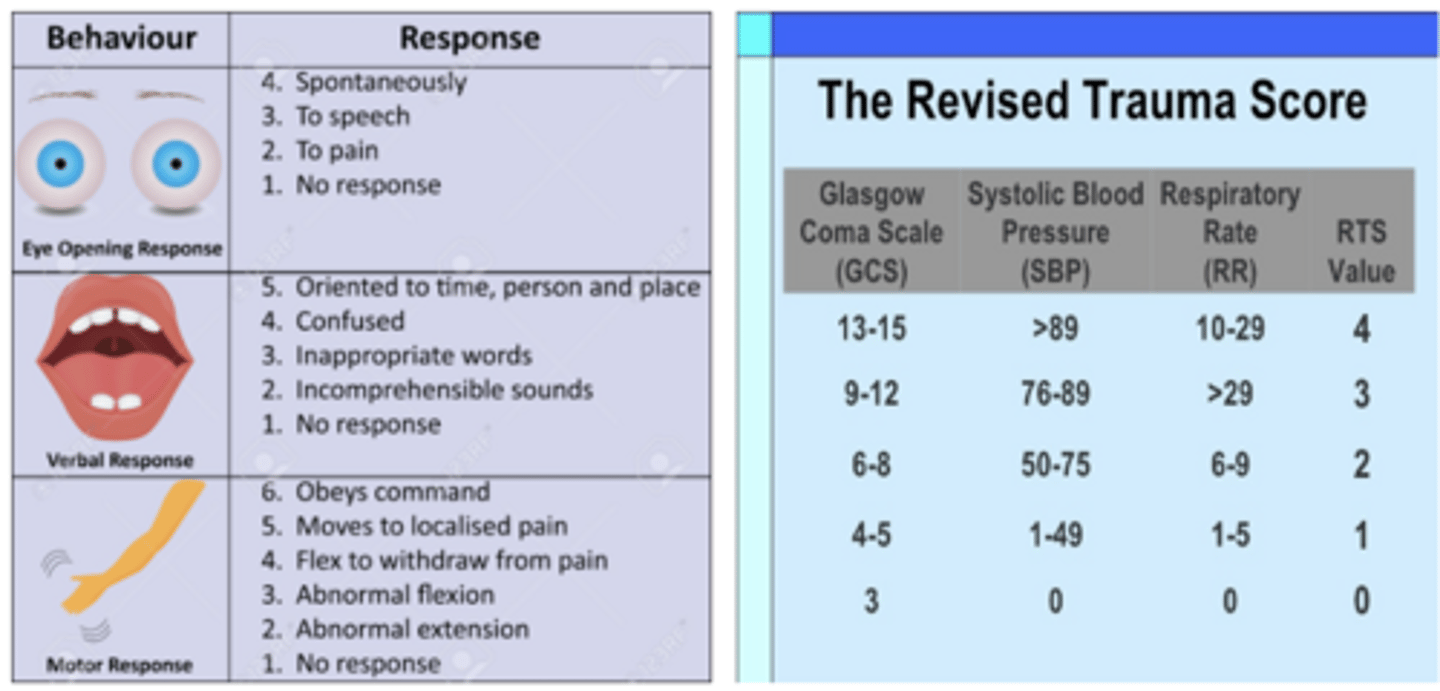
Glasgow Coma Scale vs Revised Trauma Score
pic
Persistent Vegetative State
complete unawareness of self or surrounding environment and complete loss of cognitive function
Akinetic Mutism
severe disturbance in behavioral drive; limited to eye
opening and visual tracking
Minimally Conscious State
demonstrates minimal defined behavioral evidence of self or environmental awareness; following simple commands, manipulating objects, yes/no responses
Locked-In Syndrome
complete loss of spontaneous movement, except eye movement
Assessment: Physical Examination
Level of Consciousness
◦ GSC
◦ Appraisal of Awareness
◦ Evaluation of Arousal
Pupillary Function
◦ Control of Eye Movements
◦ Corneal Reflex
◦ Corneal Integrity
◦ Dolls Eyes
◦ Pupil Size
◦ Which cranial nerve?
Motor Function
◦ Muscle size, tone and strength
◦ Right vs Left
◦ Abnormal motor responses
◦ Posturing/Reflexes
◦ Decorticate vs Decerebrate
◦ Babinski
◦ Grasp
Doll's Eyes Phenomenon
Normal response—eyes turn together to side opposite from turn of head.
B. Abnormal response—eyes do not turn in conjugate manner.
C. Absent response—eyes do not turn as head position changes.
Oculovestibular Reflex: Caloric Ice Water Test
A. Normal response—conjugate eye movements.
B. Abnormal response—
dysconjugate or asymmetric eye movements.
C. Absent response—no eye movements.
Assessment: Physical
Respiratory Function : cerebrum, brainstem and metabolic processes
◦ ABGs
◦ Respiratory Pattern
◦ Airway Status
◦ Cough, Gag, Swallow
◦ Vent Assessment and Management
Vital Signs
◦ Blood Pressure
◦ Systemic HTN
◦ Heart Rate and Rhythm
◦ Cushing Reflex
◦ THIS IS A LATE SIGN!
◦ Systolic HTN, bradycardia, abnormal RR
◦ Pulse Pressure
◦ Fever
◦ ICP and CPP * other slide
Intracranial Pressure (ICP)
Normal Range: 0-10, can be 15 mmHg
Measured in lateral ventricles In patient's
◦ Catheter is placed into the cranium through a burr hole under local anesthesia to monitor ICP, and possibly drain excess CSF.
Monroe Kelli Hypothesis
Causes:
High: _____, __________, __________, __________
Low: __________. __________, _______, _________
Monroe Kelli Hypothesis
Nursing Management of ICP
Maintain level at Ventricles (tragus-notched part of ear)
Maintain proper alignment in bed
Maintain pressure level ordered in chart
Reduce controllable variables that elevate ICP
Baseline and serial neuro assessments
Temperature Q4H
Vitals Q1H
ABGs
Appearance of CSF
Monitor for Infection
Monitor Waveform
Cerebral Perfusion Pressure (CPP)
Cerebral Perfusion Pressure (CPP)
(CPP = MAP − ICP).
Guidelines recommend a CPP in the range of 50 to 70 mmHg
Hand-off SBAR The Conscious Patient
◦ 1.
◦ 2.
◦ 3.
◦ 4.
◦ 5.
Hand-off SBAR The Unconscious Patient
◦ 1.
◦ 2.
◦ 3.
◦ 4.
◦ 5.
Mannitol
Classification:
MOA:
Nursing Considerations:
HyperTonic Saline
Classification:
MOA:
Nursing Considerations:
Mannitol IV (0.5 to 1 gm/kg)
Increases serum osmolarity and draws free water into vasculature
Blood less viscous so improves cerebral blood flow
Onset in a few minutes
Osmotic diuretic so will also lead to volume depletion
3% saline (2-5 ml/kg)
Can also be given as a continuous drip
Hyperosmolarity leads to decreased blood velocity and improved cerebral blood flow
Does not have diuretic effect
Preferred if not hemodynamically stable