DBB: 15 Barbiturates and benzodiazepines
1/53
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
54 Terms
what group do barbs and benzos fall into
sedative-hypnotics and anxiolytics
compounds that depress the CNS and behaviour (+ alcohol)
what do these all these have in common (besides being in the same group obvs)
they’re often used as ‘date-rape’ drugs
explain the symptoms that come with increasing the dosage
changing overall state of consciousness
alertness
relief from anxiety
sedation
sleep
general anaesthesia
coma
death
what is the foundational structure of all barbiturates
barbituric acid (1864)
what are the first developed barbs and what were they used for
barbital (1903)
phenobarbital (1912)
important sedatives, anticonvulsants and anaesthetics
barbs have similar effects - but how do they differ give examples
differ in their speed and duration of action (more their redistribution and metabolic pathways)
pentothal (ultrashort) - high lipid solubility, 30 min duration → intravenous anaesthesia
amytal (short) - moderate lipid solubility, 40 min duration → surgical anaesthesia
luminal (long) - low lipid solubility, 1hr+ duration → prolonged sedation/seizure control
what are some medical uses
sleep induction
anticonvulsant
anaesthetics
sedatives
alcohol withdrawal
anxiolytics
euthanasia
how are barbs abused
recreationally used as ‘downers’
desirable effects are very similar to alcohol (anxiety relief, loss of inhibition)
takes edge of other drugs like cocaine
what kind of barbs are more preferable to animals - what has to be considered during animal self administration of barbs
people and animals prefer more rapidly-acting barbs
have to be careful in experimentation as want to avoid animal taking too much - other wise they’ll be sedated and stop responding
what is a striking effects of barbs in experimentation
enhanced responding that has been suppressed by punishment
e.g. FR10 schedule food + VR15 electric shock (aka random shock) - creates a conflict schedules → increases responding, maybe because anxiolytic effects)
how do barbs effect sleep
initially helpful in getting to sleep (why it was thought to be beneficial)
with repeated use, reduction in both REM and SWS + harder to get to sleep
why might this be the case
because you get quite rapidly developing tolerance
why aren’t barbs prescribed for insomnia and anxiety anymore
too dangerous
rapid tolerance (dose escalation)
severe withdrawal (seizures)
low safety margin (like if you give higher dose, a dose that’s closer to sedation, anaesthetic effects - bad)
how were the therapeutics issues with barbs ‘resolved’
development of anxiolytics (benzos)
structurally different to barbs but have very similar effects
what is the base structure for all benzos
benzene ring - just different things attached to it
what are some of the first benzos brought to market
librium (1959) - still used for bipolar
valium (1963)
what are they widely used for
anxiolytics; sedatives (calm agitation, induce sleep);
anticonvulsants; treatment of alcohol withdrawal;
surgical sedation/amnesia (in combination with other drugs - since benzos cant really induce general anaesthesia unless at very high doses → more for pre surgical sedation)
what is its medical use
pathological anxiety
severe emotional distress
relief from agitation and alcohol
sedation (sleep-inducing)
pre-surgery sedation and amnesia
anticonvulsant
what determines benzo distribution in the brain
they’re all lipid soluble
depend partly on redistribution to others sites, but also metabolic pathways
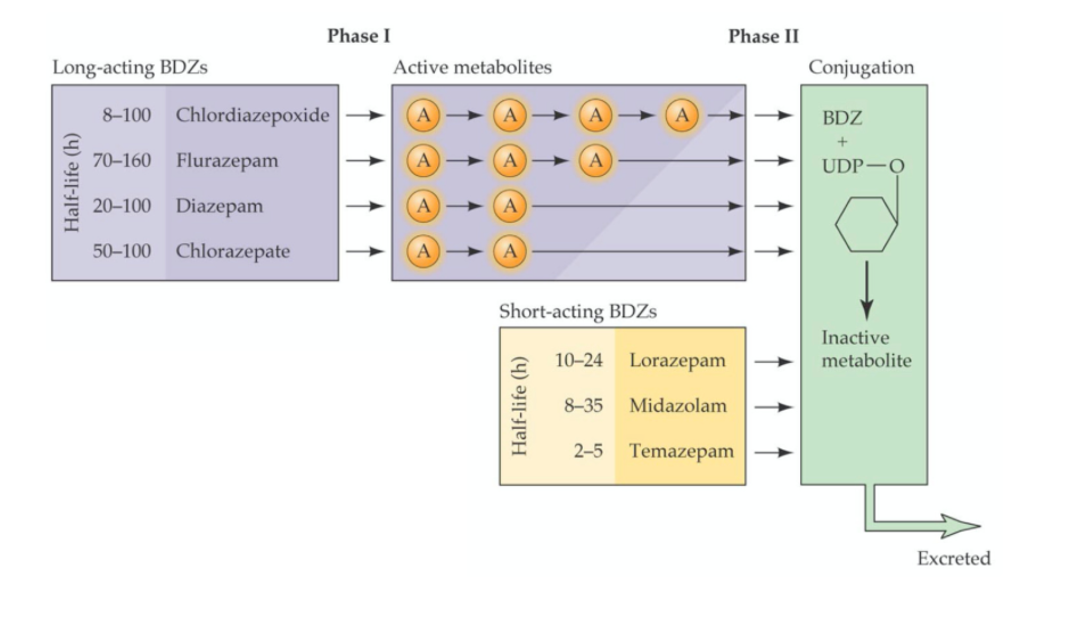
what do longer action benzos have
multiple active metabolite steps
give example of both a short acting and long acting benzo and how they’re metabolised
e.g. lorazepam (HL = 10-24hr) immediately metabolised into an inactive molecule
but chordiazepoxide (HL = 8-100hr) is metabolised into an active molecule → and then another active molecule - that keep having effects → until it becomes and inactive molecule
and then both are excreted
how would you use both these drug considering if they’re short or long acting
for someone have a one off panic attack, no history of anxiety → give lorazepam for example
versus someone with chronic anxiety → makes sense to give them chlordiazepoxide
compared to barbiturate, how are benzos safer
less tolerance
less severe withdrawal
higher TI
much harder to take a lethal dose of benzos (unless in combination with other CNS depressants)
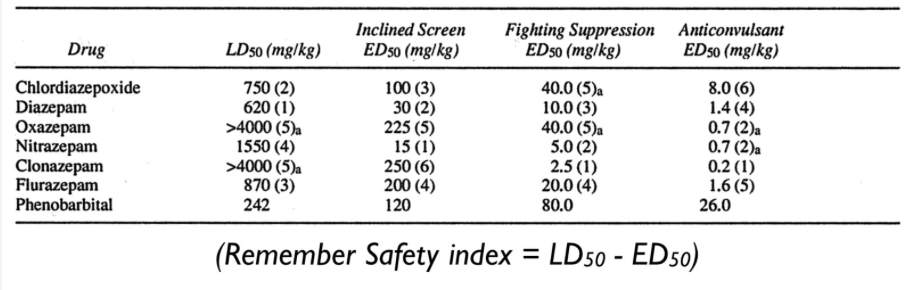
explain the study comparing safety index of benzos and phenobarbital
showed the difference when
inducing sedation incline screen test (if you’re sedated → you slip off)
suppression of fighting induced by foot shock
and blocking convulsion
the LD50s were ranked for each drug and when working out SI → phenobarbital was a lot lower in all cases
where can benzo abuse be seen
illicit use: when In combination with not other drugs
date rape drug cases e.g. rohypnol
in what ways does benzo dependence occur - what’s the best way to come off them
ween off - never cold turkey
withdrawal syndrome: milder form of alcohol, barbiturate withdrawal
persistent emotional disturbances, following withdrawal from even low doses of benzos - anxiety, tingly feelings, weight loss, oversensitivity to sensations
what’s another sedative hypnotic - how is it synthesised
GHB
synthesise by chemises looking for GABA replacement that would cross the BBB
also occurs naturally in the brain (small quantities)
GHB structure very similar to GABA
what are its effects - what drug does it resemble
subjective effects resemble alcohol: relaxation, social disinhibition etc. with some mild stimulant-like effects too
also a date-rape drug (pops up as a ‘club drug’)
explain the study looking at tolerance to the behavioural effects of GHB
mice given 200mg/kg GHB for 14 days
locomotor activity measured 30-60 minutes following each dose
found:
initial decreased locomotor activity compared to control
over the two weeks increased - highlighting tolerance
why might this have been the case
sedative effects (maybe anxiolytic effects - less anxious in environment so doesn’t run)
what receptors does GHB act on
agonist at two types of GPCRs
low-affinity agonist at GABAb receptors (appears to be critical for most behavioural effects)
what do GABAb receptor knockout mice show
do not display the typical behavioural responses to GHB (particularly sedative-hypnotic effects)
what were early thoughts about mechanism of action for these types of drugs (alcohol, benzos, barbs)
have such widespread sedative effects - thought to affects several neurotransmitters
many transmitter systems implicated
nonspecific membrane effects
potentiation of GABA effects
what was discovered in 1977 concerning benzo binding sites
concentrated in newly evolved structures (cortex, hippocampus, amygdala)
correlate with anxiolytic effects
closely related to GABAa receptor sites
what does a coronal slice showing sedative-hypnotic drug effects
you see binding in a lot of places but not everywhere
lots of binding in hippocampus, but not the whole of it
widespread but selective nonetheless
what is GABA - its importance in the brain
most important inhibitory NT in the adult, vertebrate brain
found throughout the brain in high concentrations
synthesised from glutamate
how is GABA synthesised
glutamate inside the cell is converted into GABA by enzyme glutamic acid (decarboxylase)
glutamate → GABA (done through regular excitosis)
GABA is then stored in vesicles transported by vGATs - vesticular GABA transporter
which is then released through conventional mechanisms likes excitosis to then bind GABA to receptors
is now taken back up into the same cell through transporters to be converted back to glutamate
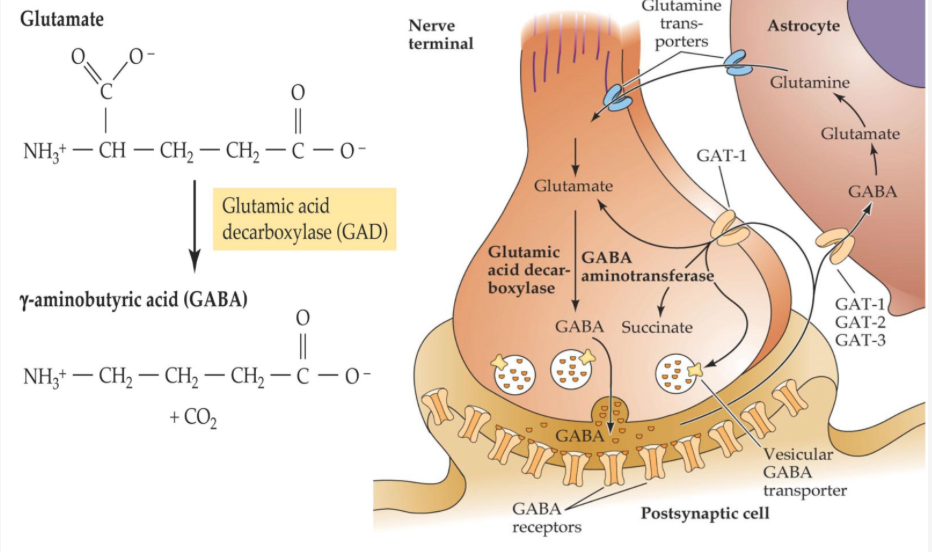
what do astrocytes have to do with this process also
not just GABA being taken back up into the presynaptic cell
it also has a process where its taken up by astrocytes which convert it to glutamate → and then transported back to the cell to be resynthesised into GABA again
explain the 2 types GABA receptors
GABAa and GABAb
both post synaptic and presynaptic (GABAa mostly ‘post’ and GABAb mostly ‘pre’)
GABAa (and GABAc) - ionotropic receptors (ligand gated Cl- channels)
GABAb - metabotropic receptors (G-protein-coupled)
how many subunits do GABAa receptors consist of
5 - they surround a central pore (Cl- ion channel)
how many ‘types’ of GABAa subunits have been identified
as of 2008 - 18 different types
most GABAa receptors have 2alpha +2beta + a (gamma/theta)
what do these differences mean
question comes in - are there different drug effects at different receptors
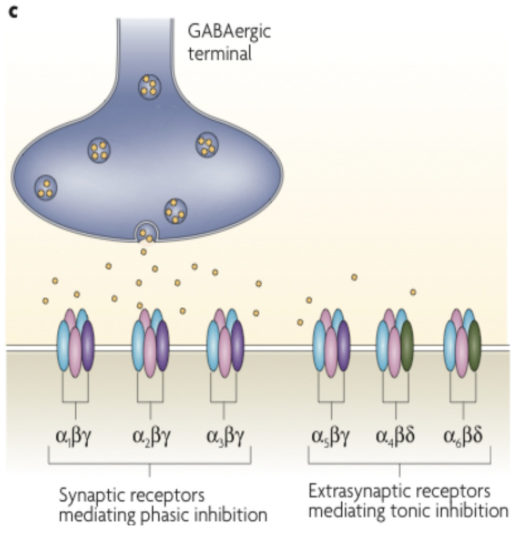
where are these different subunit combinations found - what does it mean
found in different parts of the brain - even on the same neuron (just in different locations)
e.g alpha(1,2,3) beta gamma → synaptic receptors mediating phasic inhibition
e.g alpha5 beta gamma + alpha(4,6) beta theta → extrasynpatic receptors mediating tonic inhibition
what’s a GABAa receptor agonist
muscimol
what’s a GABAa receptor antagonist - how does it work
bicuculline
blocks the effects of GABA not the effects of benzo/barbiturates
because benzo/barbiturates bind to a different site separate from the GABA binding site
explain - how most drug act as non-competitive antagonists
since they compete for the same site as GABA bu they do change the effect of GABA (in order to inhibit cells)
what do all sedative-hypnotics appear to do to GABA
enhance the ability of GABA to cause chloride influx through GABAa receptors
cell becomes more negative → inhibition
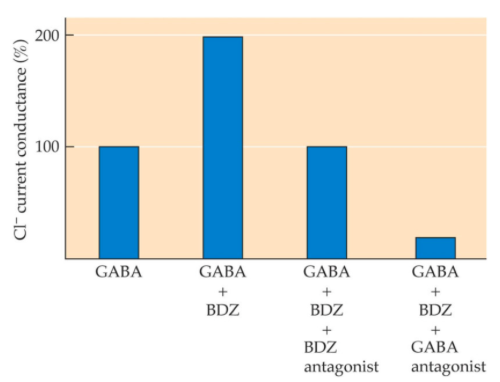
so explain this image - are barbiturates the same
benzos dont do much by themselves they are influencing the effect of GABA - cant do anything without GABA
barbiturates seem to have some effects by themselves by again its primarily their influence on changing the gate to allow more Cl- influx
give an example of what GABA + benzo/barbiturates on GABAa channels
in the presence of GABA + diazepam → GABAa channels open more frequently than with GABA alone
in the presence of GABA + phenobarbital → GABAa channels stay open for longer than with GABA alone (barbiturate may also have some direct agonist effects)
do similar things but in different ways
what about a binding site for alcohol
we don’t know yet
why does the GABAa receptor have benzo binding sites?
endogenous ligands for the benzo binding site
steroid metabolites of progesterone and deoxycorticosterone
may regulate anxiety at times of stress e.g. childbirth
so the suggestion that this may indulge in this pathway that regulate through the benzo site sort of stress responses and potentially in childbirth
how can you test the behavioural effects of benzos separately
generate knock-in mice with point mutations of the benzos binding site, in specific GABAa alpha subtypes
these mice are then selectively insensitive to benzo effects
what receptor subunits are requires for the sedative effects and anxiolytic effects
sedative effects - require alpha1 containing receptors (also a3 - as they're located in recticular activating systems - related to more general states of awareness)
anxiolytic effects - require alpha2 containing receptors → so alpha2 is a very attractive target for drug development (because a2 receptors are specifically located in the limbic regions - striatal regions)