2. adapted from quizlet: ryanef123 MMCP 9 - Diabetes/Renal (Dr. Xu)
1/151
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
152 Terms
(?) million people of all ages had diabetes in the US
40.1
describe cycle of diabetes mellitus
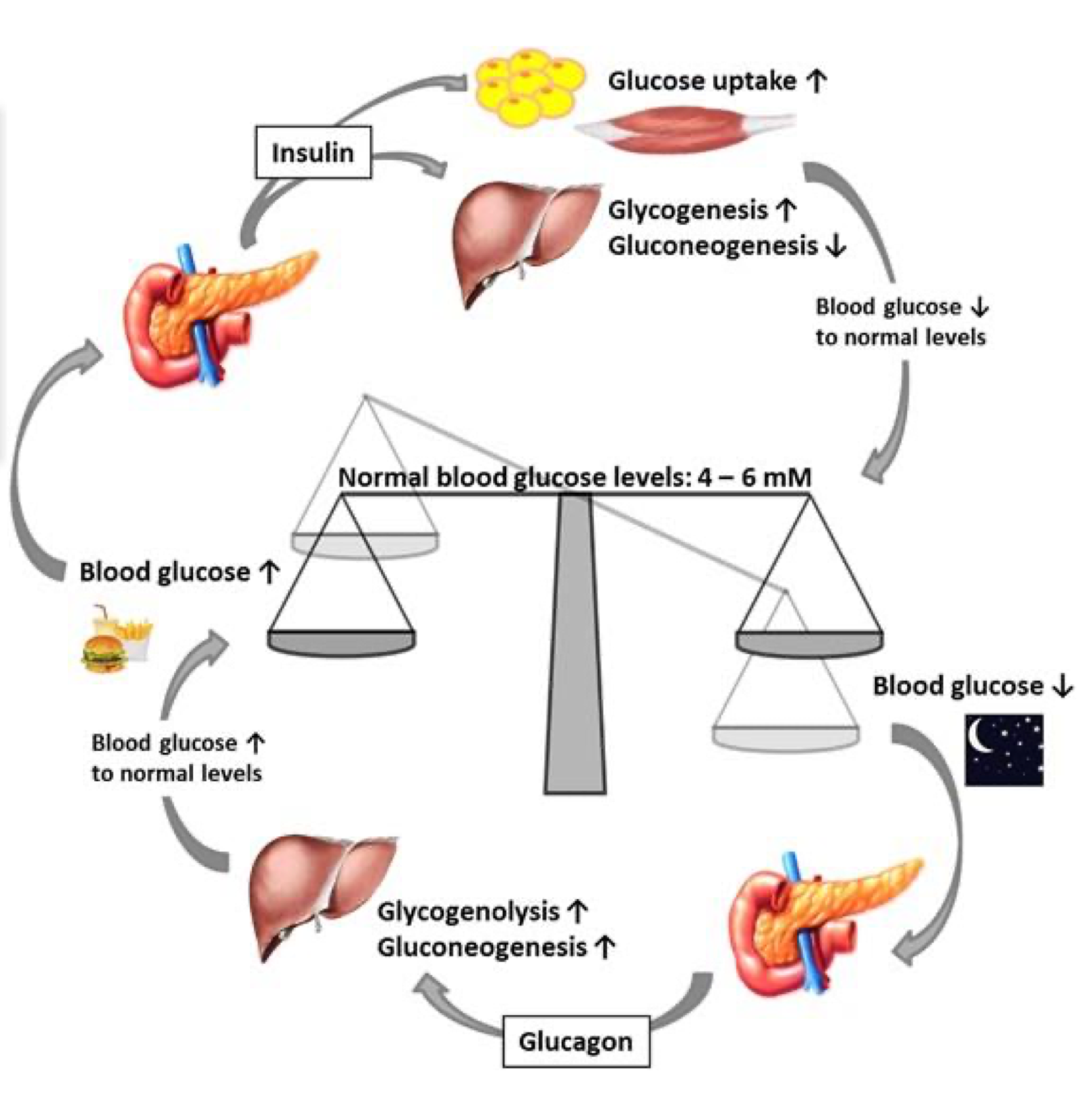
In normal function, when blood glucose is increased, what is released from the pancreas to decrease blood glucose?
insulin
In normal function, when blood glucose is decreased, what is released from the pancreas to increase blood glucose?
glucagon
What cell secretes insulin, lowers blood glucose by promoting its uptake into cells?
beta cell
What cell secretes glucagon, which raises blood glucose by stimulating glycogen breakdown in the liver?
alpha cell
What cell secretes somatostatin, which inhibits the release of insulin and glucagon and slows digestive processes?
delta cells
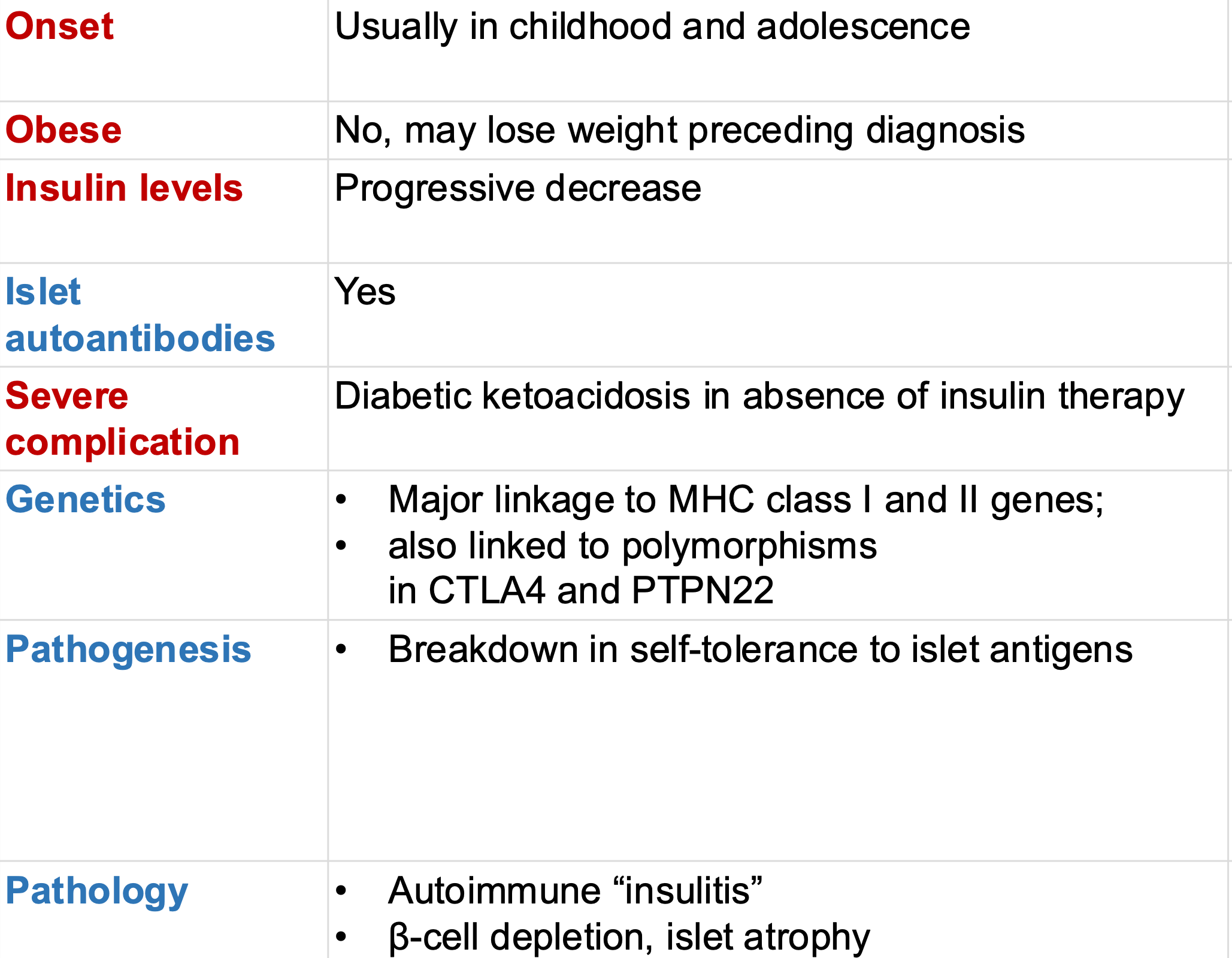
What type of diabetes?
Autoimmune β-cell destruction
Absolute insulin deficiency
Including latent autoimmune diabetes of adulthood (LADA)
type 1
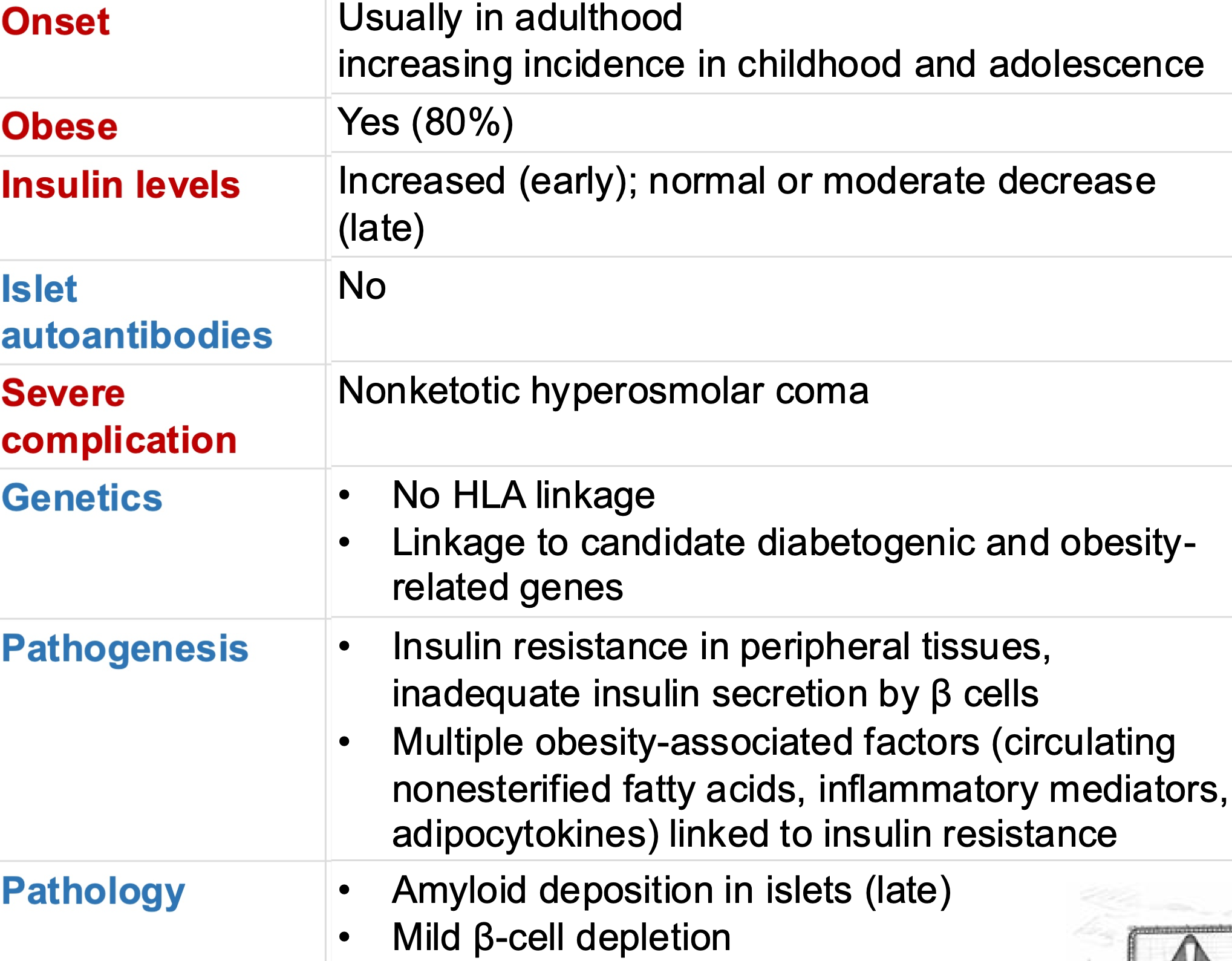
What type of diabetes?
Insulin resistance and metabolic syndrome
A non-autoimmune progressive loss of adequate β-cell insulin secretion
type 2
What type of diabetes?
Diagnosed in the second or third trimester of pregnancy
Not clearly overt diabetes prior to gestation
gestational
what are some other causes of diabetes?
Monogenic diabetes syndromes: neonatal diabetes maturity-onset diabetes of the young (MODY)
Diseases of the exocrine pancreas
Cystic fibrosis
Pancreatitis
Drug or chemical induced
Glucocorticoid use
Treatment of HIV/AIDS
Post organ transplantation
Endocrinopathies
Infection
Genetic syndromes
Type 1
Type 2
MODY stands for what?
Maturity-onset diabetes of the young
What lab measures when hemoglobin becomes glycated/coated with glucose?
HbA1C
HbA1c reflects RBCs where?
bloodstream
what conditions can alter HbA1C levels?
Hemodialysis
Pregnancy
HIV treatment
Age, race/ethnicity
Anemia/ hemoglobinopathies
T/F: Patients can have only HbA1C testing done instead of regular blood sugar self-testing
False (in addition, not replacing)
A fasting plasma glucose of _____ mg/dL OR ____ mmol/L indicate diabetes
≥126 mg/dL , ≥7.0 mmol/L
An occasional plasma glucose of ____ mg/dl OR ____ mmol/L indicates diabetes
≥200 mg/dL , ≥11.1 mmol/L
An HbA1C greater or equal to ____% indicates diabetes
≥6.5%
An HbA1C from ____ % to _____ % indicates pre-diabetes
5.7-6.5
An HbA1C below ___% indicates no diabetes
≤5.7
After 2 hours of fasting, once glucose is consumed, below _____ mg/dL or ____ mmol/L indicates no diabetes
140 mg/dL, 7.8 mmol/L
After 2 hours of fasting, once glucose is consumed, between _____-_____ mg/dL or ____ - _____mmol/L indicates pre-diabetes
140-199 mg/dL, 7.8-11.0 mmol/L
After 2 hours of fasting, once glucose is consumed, greater or equal to _____ mg/dL or _____mmol/L indicates diabetes
200 mg/dL, 11.1 mmol/L

A 21-year-old female was referred to the dental center, complaining of halitosis and swollen and painful gums, which lasted 2 months. The patient has a history of diabetes, which was diagnosed around 11 years ago.
Are there any other questions you would like to ask the patient?
- When were you diagnosed with diabetes, and which type is it?
- How do you usually monitor your blood sugar levels?
- What medications are you currently taking for diabetes (or other conditions)?
- How often do you see your doctor? When was your last visit?
- Do you ever have episodes of very low or very high blood sugar?
- Do you ever find yourself disoriented, agitated, and anxious for no apparent reason?
- Do you have any other medical conditions related to your diabetes?

A 21-year-old female was referred to the dental center, complaining of halitosis and swollen and painful gums, which lasted 2 months. The patient has a history of diabetes, which was diagnosed around 11 years ago.
Following a detailed interview, we gained a thorough understanding of the patient's diabetes……She also had stage 4 renal disease and gout.
Now, back to our comfort zone…… what are you going to do for the oral examination?
- D0150
- Perio assessment
- Take X-Rays
In diabetes-associated periodontal disease, periodontal microbiota plus ______ activation leads to exaggerated and sustained inflammation and impaired repair resulting in enhanced periodontal tissue breakdown
RAGE
What type of relationship do diabetes and periodontitis have?
Bidirectional
People without DM but with periodontitis have a _______ level of HbA1C, and exhibit a _______ chance of developing prediabetes and diabetes
higher, higher
Among DM patients, periodontitis was significantly associated with _____ glycemic control and more complications
poorer
T/F: Studies show that HbA1C levels in people with T2DM was reduced after periodontal treatment
true

A 21-year-old female was referred to the dental center, complaining of halitosis and swollen and painful gums, which lasted 2 months. The patient has a history of diabetes, which was diagnosed around 11 years ago.
What are some managament considerations?
- SRP performed over four visits within 1 week
- Systemic antibiotics (consisting of amoxicillin 500 mg and metronidazole 500 mg, BD for 7 days, were prescribed at the fourth visit)
- Twice daily rinsing (with 10 mL of 0.2% chlorhexidine was prescribed for 3 months)
What are 5 systemic chronic complications associated with diabetes?
- Vascular structures (Arterioles, Capillaries, Medium/Large vasculature)
- Retinopathy
- Nephropathy
- Neuropathy
- Foot ulcers
T/F these are all management techniques of diabetes
- Individualize goals
- Adjusted based on patient's age
- Duration of diabetes
- Presence of comorbidities
- Diabetic complications
- Hypoglycemic risk
true
What is the general goal HbA1C for most patients with type 2 diabetes?
<7% !!!
(for most nonpregnant adults without severe hypoglycemia)
What is the goal blood glucose for most patients with type 2 diabetes?
<110 mg/dL
What is the goal HbA1C for Healthy adults, short diabetes duration, long life expectancy, low hypoglycemia risk—if safe?
<6.5%
What is the goal HbA1C for Frail adults, significant comorbidities, cognitive/functional limitations, limited life expectancy, or high treatment burden?
~8%
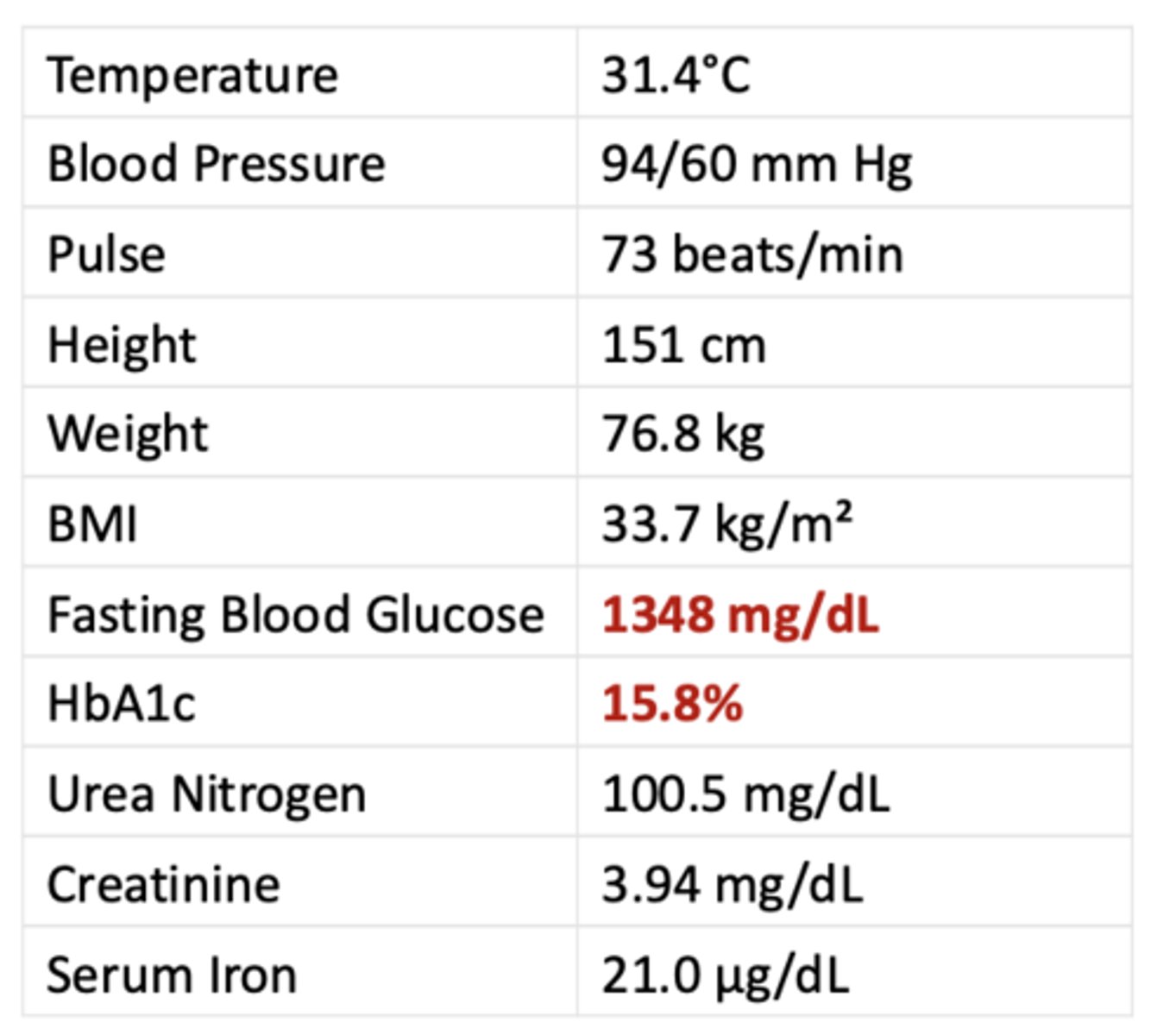
HPI
- A 64-year-old woman with type 2 diabetes was admitted to the hospital due to loss of
consciousness.
- Upon arriving at the hospital, she presented with hypothermia and hypotension, with abnormal serum glucose level and renal function.
PMH
- Hypertension
- Dizziness
What happened to this patient?
Hyperosmolar hyperglycemic status
The amount of insulin required to prevent lipolysis is _____ of that required for glucose utilization
1/10
Metformin is what classification of medication?
biguanides
Glipizide is what classification of medication?
sulfonylureas
Repaglinide, Nateglinide are what classification of medication?
meglitinides
Pioglitazone, Rosiglitazone are what classification of medication?
thiazolidinediones
Acarbose, Miglitol are what classification of medication?
alpha-glucosidase inhibitors
Dapagliflozin, Canaglifozin are what classification of medication?
SGLT2 inhibitors
Dulaglutide, Liraglutide are what classification of medication?
incretin mimetics (GLP-1 receptor agonists)
Pramlintide is what classification of medication?
amylin mimetics
Sitagliptin, Saxagliptin are what classification of medication?
DPP-4 inhibitors
This is the MOA of what diabetes drug?
Limit liver's ability to release sugar; improve cells' sensitivity to insulin
Biguanides (Metformin)
This is the MOA of what 2 diabetes drugs?
Trigger the release of insulin from the pancreas
- Sulfonlyureas (Glipizide)
- Meglitinides (Repaglinide, Nateglinide)
This is the MOA of what diabetes drug?
Improve cells' sensitivity to insulin; limit liver's ability to make and release sugar
Thiazolidinediones (Pioglitazone, Rosiglitazone)
This is the MOA of what diabetes drug?
Slow the body's ability to break down starches and some sugars
Alpha-glucosidase inhibitors (Acarbose, Miglitol)
This is the MOA of what diabetes drug?
Limit kidneys' ability to reabsorb sugar, increasing sugar excretion in urine
SGLT2 inhibitors (Dapagliflozin, Canagliflozin)
This is the MOA of what diabetes drug?
Stimulate insulin release as blood sugar rises; may be combined with other therapies
Incretin mimetics/GLP-1 receptor agonists
(Dulaglutide, Liraglutide)
This is the MOA of what diabetes drug?
Help regulate blood sugar; slow gastric emptying; used with insulin shots
Amylin mimetics (Pramlintide)
This is the MOA of what diabetes drug?
Stimulate insulin release as blood sugar rises; limit liver’s glucose release
DPP-4 inhibitors (Sitagliptin, Saxagliptin)
Which two diabetes drugs target Liver, muscle, adipose tissue?
- Biguanides (Metformin)
- Thiazolidinediones (Pioglitazone, Rosiglitazone)
Which two diabetes drugs target pancreatic beta cells only?
- Sulfonylureas (Glipizide)
- Meglitinides (Repaglinide, Nateglinide)
Which diabetes drug targets the small intestine (brush border enzymes)?
Alpha-glucosidase inhibitors
(Acarbose, Miglitol)
Which diabetes drug targets the renal proximal tubules (kidneys)?
SGLT2 inhibitors (Dapagliflozin, Canagliflozin)
Which diabetes drug targets the Pancreatic beta cells, brain, stomach?
Incretin mimetics/GLP-1 receptor agonists (Dulaglutide, Liraglutide)
Which diabetes drug targets the Brain (satiety centers), stomach?
Amylin mimetics (Pramlintide)
Which diabetes drug targets Pancreatic beta cells, liver?
DPP-4 inhibitors (Sitagliptin, Saxagliptin)
Hyperosmolar hyperglemic status (HHS) or diabetic ketoacidosis (DKA)?
Glycogenolysis and gluconeogenesis
HHS
Hyperosmolar hyperglemic status (HHS) or diabetic ketoacidosis (DKA)?
Ketone body production
DKA
Hyperosmolar hyperglemic status (HHS) or diabetic ketoacidosis (DKA)?
Most commonly affects people with type 1 diabetes
DKA
Hyperosmolar hyperglemic status (HHS) or diabetic ketoacidosis (DKA)?
Most commonly affects people with type 2 diabetes
HHS
Hyperosmolar hyperglemic status (HHS) or diabetic ketoacidosis (DKA)?
Develops quickly (within 24 hours)
DKA
Hyperosmolar hyperglemic status (HHS) or diabetic ketoacidosis (DKA)?
Develops slowly (days to weeks)
HHS
Hyperosmolar hyperglemic status (HHS) or diabetic ketoacidosis (DKA)?
- Blood sugar level: Usually above 250 mg/dL.
- Urine or blood ketones Present.
- Blood pH level 7.3 or lower.
- Serum bicarbonate (mEq/L) 18 or lower
- Mortality rate about 1% to 8%.
DKA
Hyperosmolar hyperglemic status (HHS) or diabetic ketoacidosis (DKA)?
- Blood sugar level: Usually above 250 mg/dL.
- Urine or blood ketones Trace or none.
- Blood pH level higher than 7.3
- Serum bicarbonate (mEq/L) higher than 18
- Mortality rate about 10% to 20%
HHS
Uncontrolled hyperglycemia and high glucose levels in saliva can lead to what oral manifestation?
Candidiasis
Uncontrolled hyperglycemia and high glucose levels in saliva can lead to accumulation of glycosylation products which increases what?
Candida colonization and adhesion
Uncontrolled hyperglycemia and high glucose levels in saliva can lead to (increased/ decreased) neutrophil function and chemotaxis
decreased
High or low salivary pH has these effects?
- Favors the growth of candida growth
- Triggers the extracellular phospholipase and acid proteases
- Increase yeast adhesion
Low
What can cause tissue response to injury to diminish and hyposalivation in DM patients?
Candidiasis
Which of the following is not an oral complication associated with DM?
A) Xerostomia and hyposalivation
B) Dental Caries
C) Diabetic sialadenosis
D) Deep bacterial infection
E) Delayed wound healing
D - Should be deep fungal infection
Which of the following is not an oral complication associated with DM?
A) Neuropathy
B) Taste disturbance
C) Lack of caries
D) Burning mouth syndrome
E) Oral adverse events from medications
C) Lack of caries
What do all of these cause in diabetic patients?
- Salivary gland dysfunction (Mitochondrial dysfunction, Nitric oxide pathway impairment)
- Osmotic diuresis/dehydration:
- Neuropathy
- Medication-Related Xerostomia
Dry mouth

ID the condition:
- A rapidly progressive, angioinvasive fungal infection.
- Clinical Presentations of rhino-orbital-cerebral mucormycosis include: facial pain, periorbital edema, black eschar, cranial nerve palsies
Mucormycosis
ID the condition:
- Significantly reduced salivary calcium and increased alkaline phosphatase in participants with DM
- Children with T1DM had significantly lower salivary pH and higher counts of Lactobacilli
- Cariogenic diet and poor plaque control
- Reduction in saliva production
Diabetes and caries
This is the patho-physiology of what diabetes-related oral disease?
Accumulation of advanced glycation end products (AGEs) in periodontal tissues, decreased renewal of periodontium and defective local immune regulation
Periodontal disease
This is the patho-physiology of what diabetes-related oral disease?
Infection with Candida species resulting from salivary dysfunction, hyperglycemia and abnormal immune function
Oral candidiasis
This is the patho-physiology of what diabetes-related oral disease?
Progression of periodontal disease exposing root surface and reduced salivary flow rate predispose to enamel hypomineralization and caries formation
Root caries
This is the patho-physiology of what diabetes-related oral disease?
Ischemic damage to pulp tissues diabetes- related vascular damage
Pulp necrosis and periapical abscess
This is the patho-physiology of what diabetes-related oral disease?
Diabetes-related vascular dysfunction and decreased immune function
Delayed wound healing/infection s/p surgery
What is the treatment/prevention for periodontal disease in patients with DM?
- Risk assessment
- Dental check-ups
- Nutrition intervention
- Periodontal therapy
What is the treatment/prevention for oral candidiasis in patients with DM?
Anti-mycotic drugs (nystatin, miconazole)
What is the treatment/prevention for root caries in patients with DM?
- Fluoride
- Restorative procedures
- Glycemic control
What is the treatment/prevention for pulp necrosis/periapical abscess in patients with DM?
- Endodontic treatment
- Control of DM
What is the treatment/prevention for delayed wound healing/infection in patients with DM?
- Antibiotics
- Good glycemic control
For acute oral infections, non-insulin controlled patients may require _______ and a consult with a physician is indicated
insulin
For acute oral infections, insulin controlled patients may require _______ and a consult with a physician is indicated
increased dose of insulin
For patients with brittle diabetes or receiving high insulin dosage, what should be performed if a patient has an acute oral infection?
Culture taken from infected area for antibiotic sensitivity testing
For patients with brittle diabetes or receiving high insulin dosage with an acute oral infection, what 2 steps must be taken?
Culture sent for testing, antibiotic therapy initiated
If a patient with brittle diabetes/receiving high insulin dosage and responds poorly to the first antibiotic, what do you do?
Use more effective antibiotic based on sensitivity results
T/F: For an acute oral infection in a DM patient, the infection can be treated by standard methods (Warm intraoral rinses Incision and drainage Pulpotomy, pulpectomy, extractions, antibiotics)
True