DSON Congenital Heart Disease Post Midterm
1/54
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
55 Terms
What are the types of acyanotic CHD? (7)
Coarctation of aorta
Cor Triatriatum
Ebstein’s Anomaly
Congenitally Corrected TGA (cc-TGA)
Partial Anomalous Pulmonary Venous Return (PAPVR)
Persistent Left Superior Vena Cava (L-SVC)
Dextrocardia
What does QP:QS measure/compare
compare the flow through the pulmonary valve with the flow through the aorta, should be exact same (equal to 1) except for shunts
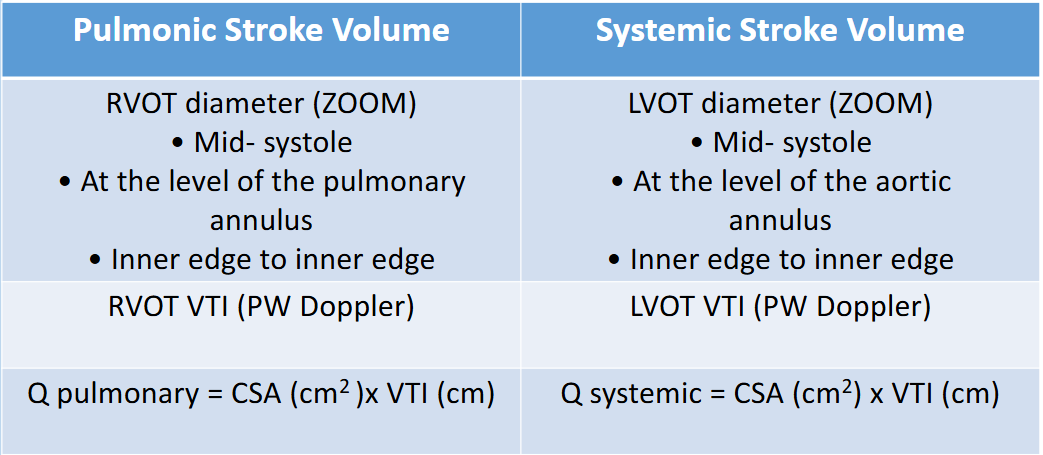
Q= flow= SV, SV =CSA x VTI
QP : Stroke volume at the pulmonary valve area
SV of pulmonary system = CSA of RVOT x VTI of the RVOT
QS : Stroke volume at the aorta valve area
SV of systemic circulation = CSA of LVOT x VTI of the LVOT
Describe QP/QS for normal, insignificant shunts, and hemodynamically significant shunts + Eisenmenger
normal heart: both sides equal, thus QP/QS = 1.0
insignificant shunts: travel left to right, thus lungs get more blood flow, QP/QS = > 1.0 - 1.5 <
hemodynamically significant shunt when QP/QS > 1.5
Eisenmenger shunt is reversed, thus QP/QS < 1.0
What are echo measurements for QP/QS
Describe what happens to QP/QS for Eisenmenger shunts
shunt ratio will drop, and eventually reverse direction (L to R becomes R to L)
Beginning stages → QP/QS lower than expected bc the shunt direction is starting to reverse
measured normal but visual assessment is not normal
Eisenmenger shunts → QP/QS <1.0 bc the shunt direction completely reverses (R to L, RAP > LAP)
systemic getting more blood than pulmonary, and patient will also be getting deoxygenated blood sent to the body
Describe what happens to QP/QS for PDA when calculated normal way
insignificant PDA: LA → LV/LVOT → Aorta → PA → LA → LV/LVOT = shunt missed RVOT and went LVOT twice (more blood)
QP/QS for insignificant PDA → < 1.0 if calculated normal way (looks like it signals for Eisenmenger’s)
significant PDA with Eisenmenger: RV → PA → Aorta → body = blood skips LVOT (less blood than RVOT)
QP/QS for Eisenmenger PDA → > 1.0 if calculated normal way
Describe the adjusted QP/QS calculations for PDA
in general, reverse the direction which you divide the numbers:
QP is measured at LVOT level
QS is measured at RVOT level
as a result:
insignificant shunts between 1-1.5
Eisenmenger shunts to be <1.0
Describe coarctation of the aorta
narrowing of the descending aorta in the areas of the ductus arteriosus (DA)
What is coarctation of aorta associated with? (2)
bicuspid aortic valve → most common
Turner Syndrome
Genetic condition in only females, leading to infertility, appears short stature with webbed neck
What are hemodynamic consequences: Coarctation of the Aorta (4)
Causes increased afterload → LVH
May have reduced flow to lower extremities
Systolic pressure higher in upper extremities
Development of collateral arteries to supply lower body
Role of Sonography for: Coarctation of the Aorta
best seen in SSN, look for shelf-like narrowing or tissue ridge extending to aortic lumen
CW Doppler for highest velocity→ Measure peak velocity and maximum pressure gradient across narrowing
PW walkdown to confirm coarctation, then CW to determine highest velocity (>2.5 m/s)
for severe: persistent pressure gradient across narrowing in systole and diastole
not severe: see step up only in systole
What are treatment options for: Coarctation of the Aorta (2)
infancy: prostaglandin to maintain ductus arteriosus patency (open, keep flow into PDA)
percutaneous, surgical repair in hemodynamically significant obstruction
Describe Cor Triatriatum
a perforate membrane caused by failure of regression of an embryonic membrane
partitions the left or right atrium into two chambers
size of orifice that divides the atrium determines the severity of obstruction, symptoms, and age of presentation
large = asymptomatic/no obstruction of flow
small = have to squeeze harder, thus more severe
Compare Cor Triatriatum Sinister vs Dexter
Cor Triatriatum Sinister: divides the left atrium
symptoms similar to valvular mitral stenosis
Cor Triatriatum Dexter: divides the right atrium
extremely rare, and symptoms similar to tricuspid stenosis
How to differentiate Cor Triatriatum Sinister from supravalvular mitral ring in echo (2)
by relationship of membrane to LAA
Cor triatriatum is superior to LAA, and will be further away from MV annulus
Supravalvular is inferior to LAA, and will be near MV
assess membrane/orifice with colour and spectral Doppler:
if you see blood pooling before squeezing out, likely a cor triatriatum
Coumadin ridge in LA looks similar but the flow will be free flowing and only seen in PLAX
Describe Ebstein’s Anomaly
abnormality of tricuspid valve where there is apical displacement of the septal/posterior leaflets by AT LEAST 8mm (because its already naturally apical of MV)
What are consequences of Ebstein’s Anomaly (3)
Distortion and displacement of tricuspid leaflets
Atria-lization of RV→ some of the RV chamber become like an enlarged RA
Often severe amount of TR → amount determines hemodynamic consequences
severe TR → RA/RV dilation → can lead to RHF
Note: some people may not need treatment, others may need to surgery to replace the TV
Describe Congenitally Corrected TGA (cc-TGA)
Transposition of the great arteries, also known as L-TGA → aorta and pulmonary artery switched spots
Due to an error during first 8 weeks of fetal development, and exact cause is unknown (maybe genetics?)
Describe the blood flow in cc-TGA/L-TGA
blood flow maintained bc connections are switched twice, called double discordance → both atrioventricular (ventricles switched) and ventriculoarterial (great arteries attached to wrong ventricles)
circulation physiological normal but anatomy is abnormal, may be completely asymptomatic
blood goes into lungs to get oxygenated, while body still gets oxygenated blood
morphologic RV acts as systemic ventricle → has to pump blood to whole body
What are the associated lesions with cc-TGA (4)
VSD
Tricuspid valve anomalies
outflow tract obstruction (usually RVOT)
conduction defects
What are some long-term hemodynamic consequences of cc-TGA (3)
RV and TV are in systemic location, which is higher pressure than they were designed for thus overtime:
tricuspid regurgitation
RV failure bc cannot pump as well as LV = congestive heart failure
rhythm problems: heart blocks are common
What are some treatment options for cc-TGA
often only if they have associated defects such as VSD or RVOT obstruction
If needed:
heart failure medication
pacemaker (bc of heart blocks)
in severe cases:
“double switch surgery” which is rare
Describe Partial Anomalous Pulmonary Venous Return (PAPVR)
one or more(< 3), BUT not all (not 4), of the pulmonary veins are not connected to the LA → drains into wrong chamber (often RA)
they may be connected to systemic vein (SVC/IVC), RA, coronary sinus, and/or left innominate vein
Left sided pulmonary veins → may connect to coronary sinus and/or the left innominate vein
Right sided pulmonary veins → usually connect to RA, SVC/IVC
What are the hemodynamic consequences of PAPVR?
similar to an ASD or VSD
R-side volume overload → RA and RV dilation
Dilation of PA
RV hypertrophy if longstanding shunt causes pulmonary hypertension
Anomalous connection of a single pulmonary vein to the right SVC may be an…
isolated lesion or in combination with a sinus venosus ASD
What are echo features of PAPVR (3)
Dilated right side
absence of obvious ASD or VSD
possibly a dilated coronary sinus
How else to confirm PAPVR?
echo helps, but cannot see outside of the heart structure so most likely will be confirmed by other forms of testing:
MRI
catheterization
OHS
Describe Persistent Left Superior Vena Cava (LSVC)
L-SVC is formed by confluence of the left jugular and subclavian veins, and descends inferiorly parallel to the RSVC in most cases
commonly enters coronary sinus, but may enter LA (rare)
very rare, but likelihood increased with patients with other CHD
most commonly associated with ASD
Describe the consequences of persistent LSVC
LSVC drains into RA via the coronary sinus, so likely no hemodynamics
coronary sinus may be dilated
What are some extra steps to confirm persistent LSVC?
injection of agitated saline or dextrose into peripheral left arm vein → opacification of coronary sinus
persistent LSVC may pose difficulties during cardiac catheterization and/or cardiac surgery
Describe the Dextrocardia echo scanning protocol (4)
Subcostal view, with POM 3’o clock as normal (left) → do not correct images
Apex pointing left, but heart is right = dextroposition
Apex pointing right, but heart is right = dextrocardia
Assess liver and great vessel location to see if they have situs inversus
Label images as “Dextro”
Perform PLAX, Apical windows with patient turning to right side instead
PLAX: align transducer in plane with heart, POM to base of heart (towards aorta and PA) → heart look same/normal on screen
PSAX: clockwise from PLAX → left and right will not be opposite from normal PSAX
A4C: transducer to apex, maintaining PSAX POM → left and right reversed on screen
A2C, A3C: counter clockwise from A4C as normal
SSN: in situs inversus only, the arch will be directed to the right shoulder instead of left
rotate transducer to align with structure, a SAX arch sweep will display this more accurately
Define cyanosis
blue skin tone caused by low blood oxygen
deoxygenated blood enters the systemic system (bypassing the lungs)
What are types of Cyanotic CHDs? (8)
Interrupted Aortic Arch
Total Anomalous Pulmonary Venous Return (TAPVR)
Tetralogy of Fallot
Double Outlet Right Ventricle (DORV)
Complete Transposition of the Great Arteries (d-TGA)
Truncus Arteriosus
Hypoplastic Right Heart Syndrome
Hypoplastic Left Heart Syndrome
Describe Interrupted Aortic Arch
very rare and low survivability
represents the most severe form of coarctation, narrowing to the point it completely closed off
lack of continuity between ascending and descring aorta
can occur anywhere within the arch
if PDA remains open, there will be some blood flow into the aorta via PDA, however it will be deoxygenated
What are other cardiac abnormalities associated with interrupted aortic arch? (5)
PDA
VSD
subaortic stenosis
bicuspid AoV
ASD
Describe hemodynamic consequences of interrupted aortic arch with no ASD versus with ASD
No ASD
upper body receives oxygenated blood
lower body received deoxygenated blood
incompatible with life
With ASD
ASD allows some mixed O2 blood in the RA, which eventually enters lower body, but still overall receive very low O2 content
with addition of PDA (still open) → can provide time for baby to live longer prior to surgery
Describe the prognosis of interrupted aortic arch
failure to treat will result in 90% mortality rate by 4 days old
Cause of death include:
if there is an associated ASD/VSD, excessive blood flow through the defect → severe RHF
if no ASD/VSD, death will occur if PDA closes naturally and no blood will enter lower body → organ failure
acute kidney failure will cause blood to become too acidic → death
Describe treatment options for interrupted aortic arch
prostaglandin given intravenously immediately after birth to avoid closure of the ductus arteriosus
surgical connection of the aorta through thoracotomy incision → preferably within 1st week of life
Describe Total Anomalous Pulmonary Venous Return (TAPVR) or TAPVC (Connection)
all 4 pulmonary veins have no connection to LA → no blood to the left side at all
drain directly or indirectly into RA
can occur with or without obstruction of the pulmonary veins
What are the 3 types of TAPVR, and are there different hemodynamics?
hemodynamics are the same for all 3 types
Supracardiac: pulmonary veins drain into the SVC → above heart
Infracardiac: pulmonary veins drain into the portal vein, IVC, or ductus venous → below heart
Cardiac: pulmonary veins drain into coronary sinus
Describe hemodynamic consequences of TAPVC with no septal defects or PDA versus with ASD or VSD or PDA
No septal defects or PDA
Blood go to pulmonary veins → IVC → RA → mix blood → PA → oxygenation → pulmonary veins: never pass left side
no blood in left side AND to body → incompatible with life
With ASD or VSD or PDA
Shunts will go from right to left because the RAP > LAP
Blood will mix in the RA and go two routes:
→ RV → PA → lungs
→ LA → LV → body
allow mixed blood to enter left side, which gives enough time for baby to go into surgery
mixed blood is not sufficient for long term, still not enough oxygenated blood
RA and RV volume and pressure overloading → pulmonary hypertension
What are some treatment options for TAPVC
palliative/relief care:
atrial septostomy until corrective surgery is performed
corrective:
anasotomosis of common pulmonary vein to left atrium
closure of ASD
What is the prognosis of TAPVC?
post surgery prognosis is excellent
Describe the Tetralogy of Fallot
most common cyanotic lesion, comprised of 4 cardiac abnormalities:
Overriding aorta (sit directly over both RV and LV):
aorta override ventricular system
VSD
large subaortic defect that extends from right and non-coronary cusps of the aortic valve superiorly to the membranous septum inferiorly
RVOT obstruction and/or Pulmonary Stenosis → symptoms determining factor/ hemodynamic severity
muscular obstruction usually beings at crista supraventricularis and extends to pulmonary valve annulus, which is often hypoplastic (underdeveloped)
RVH
caused by RVOT obstruction or pulmonic stenosis
RVH may become stiff and eventually fails
When is Tetralogy of Fallot diagnosed
usually during infancy, but if severity of defects is minor, may go unnoticed for years
What are some risk factors for Tetralogy of Fallot (bc unknown cause)
viral illness during pregnancy, such as rubella
alcoholism during pregnancy
poor nutrition during pregnancy
mother older than age 40
parent who as Tetralogy of Fallot
presence of down syndrome or DiGeorge syndrome
What are hemodynamic consequences of Tetralogy of Fallot
baby will be blue/cyanotic because oxygen going to the body does not carry enough oxygen
blood from RA → RV cannot go to PA due to RVOT obstruction, and some goes to LV from the VSD → mixed blood, with low oxygenated content will go to the rest of the body
What are some signs and symptoms of Tetralogy of Fallot
cyanosis
SOB
Loss of consciousness
clubbing of fingers and toes
poor weight gain
irritability
What happens to patients with untreated Tetralogy of Fallot
survival to adulthood is rare → only 2% to age 40, most will die by age 20
underdeveloped, weak, easily tired due to low oxygen circulation
decreased oxygenated blood through coronary arteries leads to cardiac dysfunction and fatal ventricular arrhytmias
What are some treatment options for Tetralogy of Fallot, what are the 2 types of surgical options?
surgical repair is recommended between ages of 3-11 months, options include Rastelli Procedure or Intracardiac Repair:
Intracardiac Repair:
Patch the VSD
PV repair or replacement
Surgically widen the pulmonary artery to reduce RVOT obstruction
Rastelli
Role of sonography for Tetralogy of Fallot
may be first person to diagnose this disease, if the severity of pulmonary stenosis is very minor bc most blood can get to PA → asymptomatic \
Assess the following:
degree of PS
VSD → hold size
other complications (RVH, RVF) or congenital defects
RV pressure overload → “D” in PSAX
Post-surgery follow up echos, and assess for the following:
residual shunting across VSD patch
PV area, and flow through PA
any complications