T5 - IE4 - Gastroenterology - Yamaki - Clostridium Difficile
1/124
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
125 Terms
C. diff
Clostridioides difficile
Clostridioides difficile is a ______-________ __________, strict __________
- gram positive bacillius [rod]
- (strict) anaerobe
Clostridioides difficile forms ________
- (forms) spores
Clostridioides difficile some are ______ producing
- toxin (producing)
A&B
Clostridioides difficile was discovered as a cause of _______________ ______ and ___________-__________ colitis
- pseudomembranous colitis
- antibiotic-associated (colitis)
Clostridioides difficile: ______-______ route transmission
- fecal-oral (route transmission)
Epidemiology of
Clostridioides difficile: accounts for _____-____% of cases of antibiotic-assoicated diarrhea
- 20-30(% of cases of antibiotic-assoicated diarrhea)
Epidemiology of
Clostridioides difficile: stool carriage of C. difficile reaches ___-_____%
- 16-35(%)
Occurs in community ~7 / 100,000 people
Epidemiology of
Clostridioides difficile: mortality
~14,000 people / year
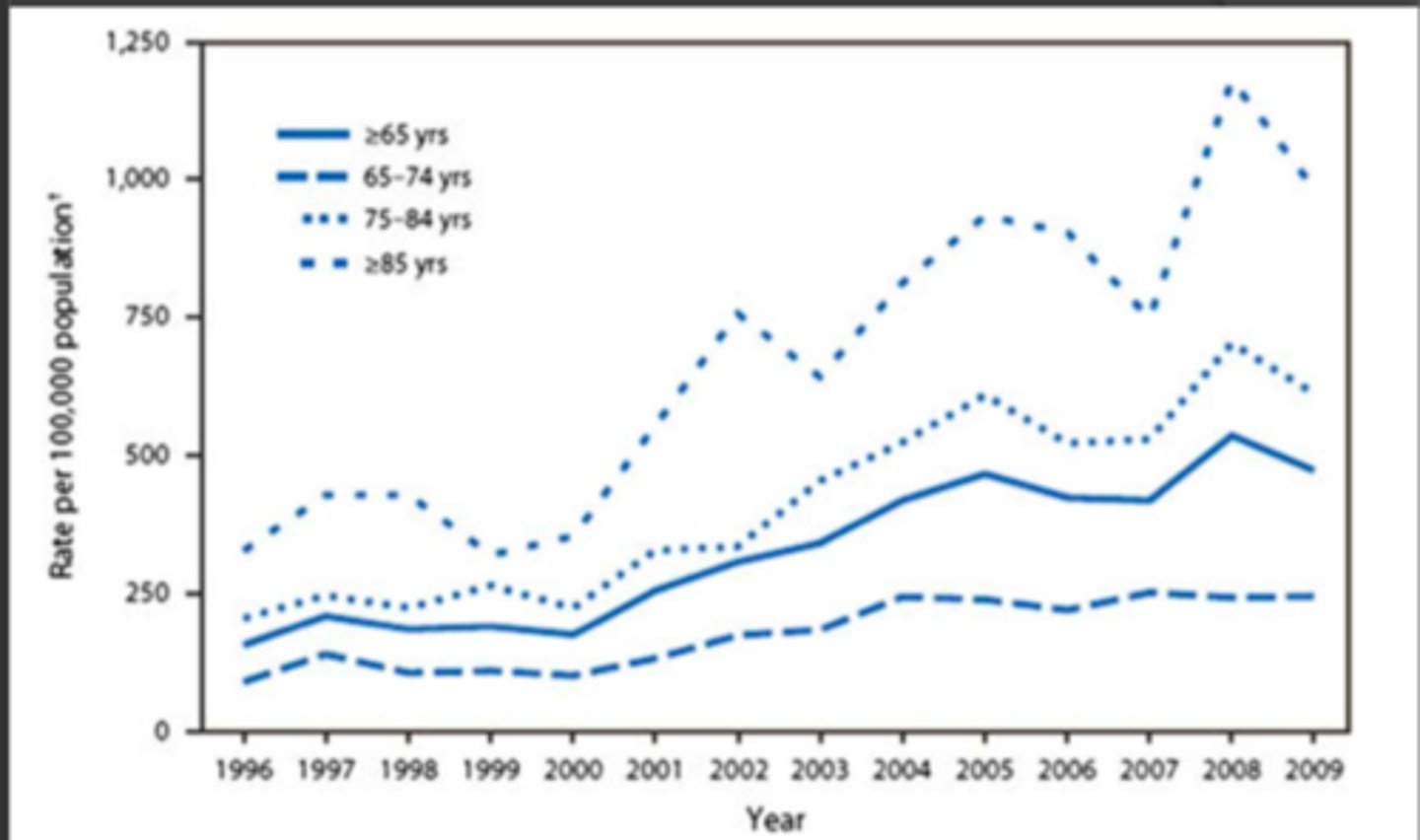
Epidemiology of
Clostridioides difficile: __________ rate amongst the elderly
- rising (rate amongst the elderly)
CDI
clostridiodes difficile infection
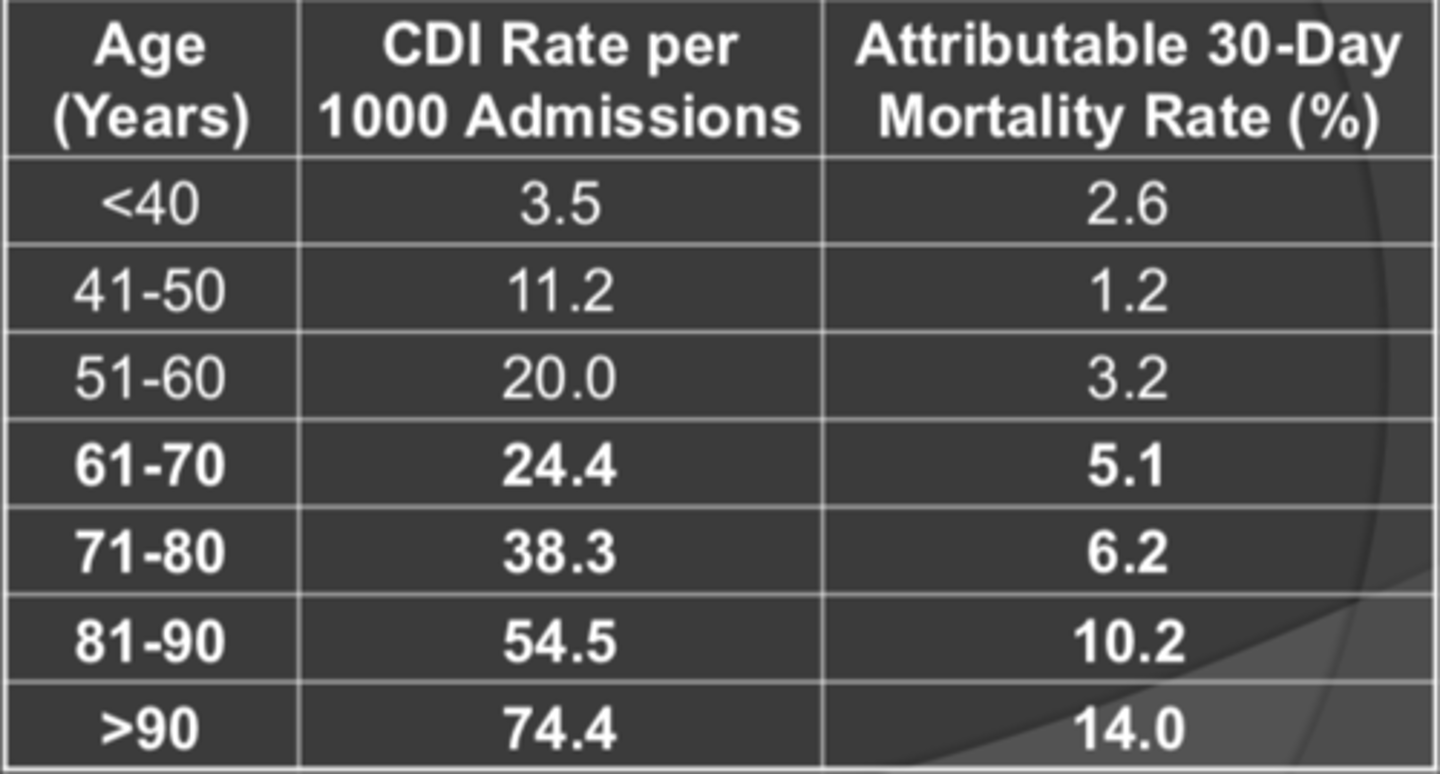
CDI rates and mortality increased with __________ ___________ _____
- (mortality increased with) increased patient age
CDI rates and mortality chart
older the patient, the higher the mortality in C Diff
Epidemiology of
Clostridioides difficile: in US, incidence continues to __________, as well as ________
- increase
- (as well as) severity
Increased toxic megacolon, colectomy, refractory to therapy, relapse
Epidemiology of
Clostridioides difficile: in US, incidence continues to increase, as well as severity
Increased toxic megacolon
Increased colectomy
Increased refractory to therapy, relapse
Epidemiology of
Clostridioides difficile: now considered by CDC as a _______ _______ _______ threat
_________ _______ has the highest C diff rate in California
- MAJOR public health (threat)
- Orange County (has the highest C diff rate in California)
Epidemiology of
Clostridioides difficile - possible reasons for INCREASED CDAD incidence and SEVERITY
changes in underlying host susceptibility
changes in antimicrobial prescribing
new strain with increased virulence / resistance
changes in infection control practices
CDAD
Clostridium difficile-associated diarrhea
Epidemiology of
Clostridioides difficile - possible reasons for INCREASED CDAD incidence and SEVERITY:
Changes in underlying ______ ________ and _________ ______
- (underlying) host susceptibility
- antimicrobial prescribing
Epidemiology of
Clostridioides difficile - possible reasons for INCREASED CDAD incidence and SEVERITY:
New strain with __________ _________ / _________
- (New strain with) increased virulence / resistance
Epidemiology of
Clostridioides difficile - possible reasons for INCREASED CDAD incidence and SEVERITY:
Changes in __________ ________ practices
- infection control (practices)
Epidemiology of
Clostridioides difficile - BI/NAP1/027 strain
distinctions from typical C. diff strains
- hyper-production of Toxin A/B
- 3rd, binary toxin
- hypersporulation
- fluoroquinolone resistance
Epidemiology of
Clostridioides difficile - BI/NAP1/027 strain distinction from typical C. diff strains: _______-___________ of Toxin A/B
- Hyper-production (of Toxin A/B)
Epidemiology of
Clostridioides difficile - BI/NAP1/027 strain distinction from typical C. diff strains: 3rd, binary _______ and __________
- (3rd, binary) toxin
- hypersporulation
Epidemiology of
Clostridioides difficile - BI/NAP1/027 strain distinction from typical C. diff strains: ____________ resistance
- fluoroquinolone (resistance)
Disease pathogenesis of C. Diff figure
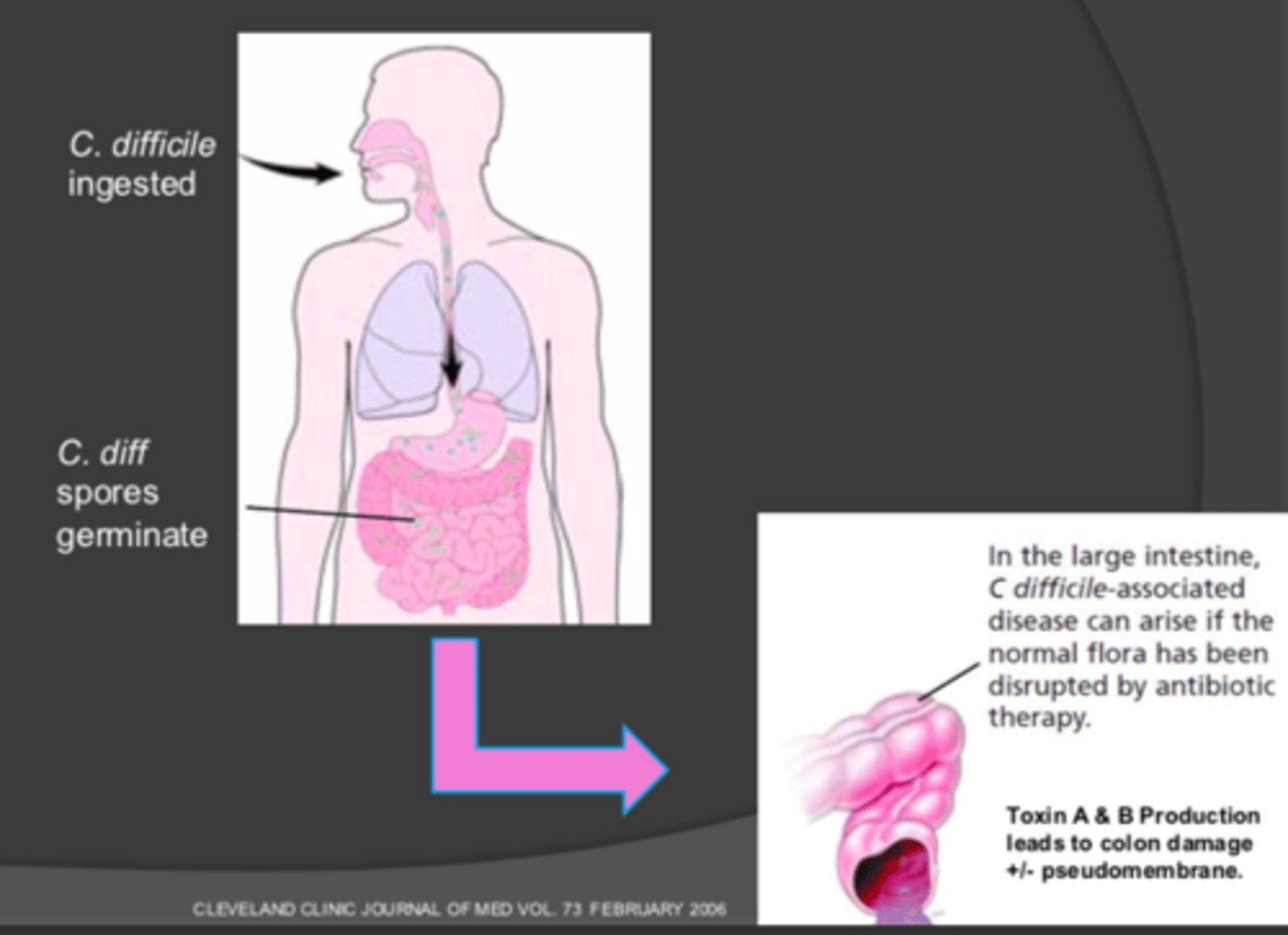
Disease pathogenesis of C. Diff: C. diff ingested -> C. diff spores ___________
- (spores) germinate
In the large intestine, C. difficile-associated disease can raise if the normal flora has been disrupted by antibiotic therapy
Toxin A & B production leads to colon damage ± pseudomembrane
Disease pathogenesis of C. Diff: In the large intestine, C. difficile-associated disease can raise if the normal flora has been ___________ by __________ therapy
- disrupted
- (by) antibiotic (therapy)
Toxin A & B production leads to colon damage ± pseudomembrane
Disease pathogenesis of C. Diff: Toxin A & B production leads to...
colon damage ± pseudomembrane
TcdA and TcdB
disrupt epithelial barrier, cause cell death and induce inflammation
Fulminant
occurring with great intensity; refers to severe pain with sudden onset
"Severe +"
Intracellular modifications by TcdA & TcdB Figure
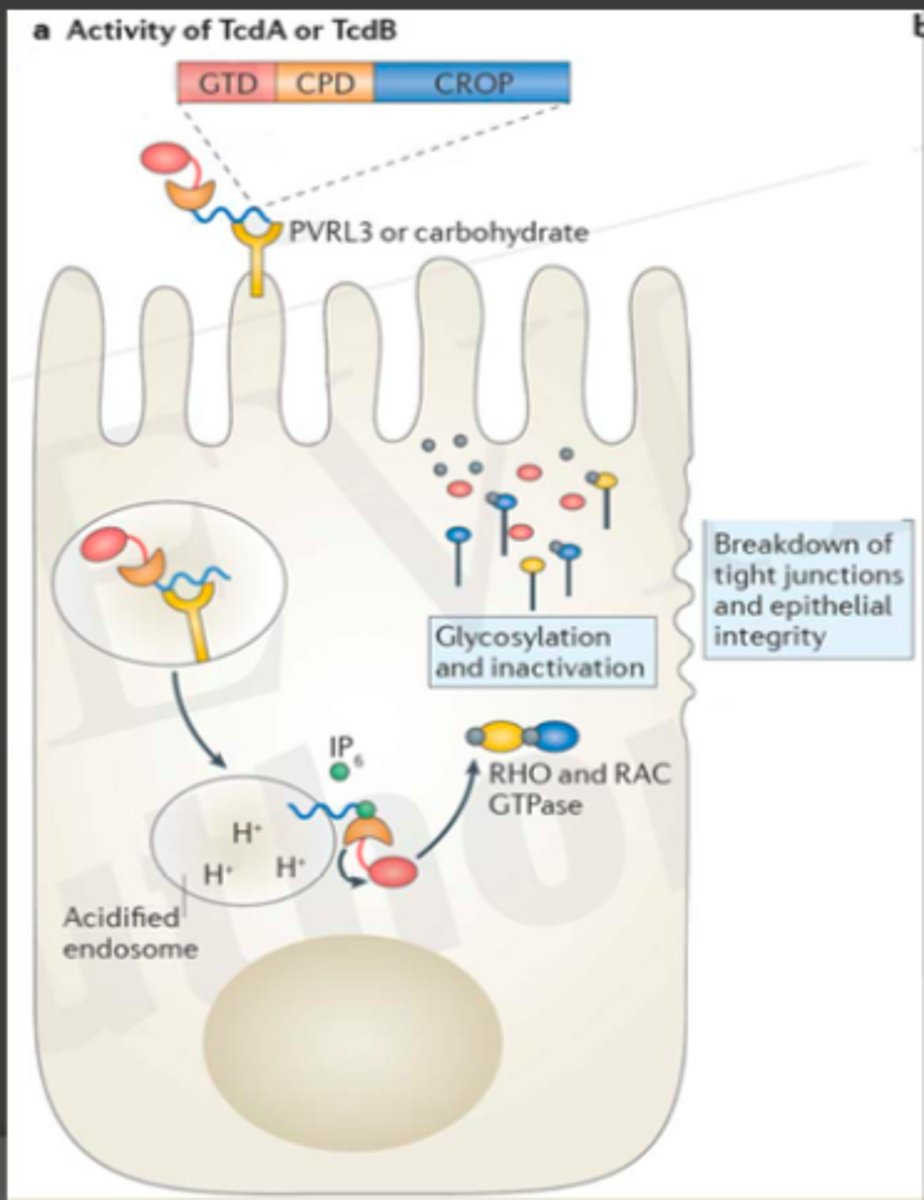
Intracellular modification by TcdA & TcdB
breakdown of tight junctions and epithelial integrity (toxins destroy epithelial cells)
glycosylation and inactivation
serum level increases and neutrophils in area which causes diarrhea
Risk factors for C. Diff
advanced age (≥ 65 years)
prior hospitalizations
resides in SNF
Prior C. Diff infection
Immunosuppression
Risk factors - MEDICATIONS
antibiotics
- clindamycin
- fluoroquinolones
- 3rd generation cephalosporins
- carbapenems
- long duration of therapy
proton pump inhibitors
prolonged corticosteroid use
chemotherapy
Risk factors - MEDICATIONS (antibiotics)
clindamycin
fluoroquinolones
3rd generation cephalosporins
carbapenems
long duration of therapy
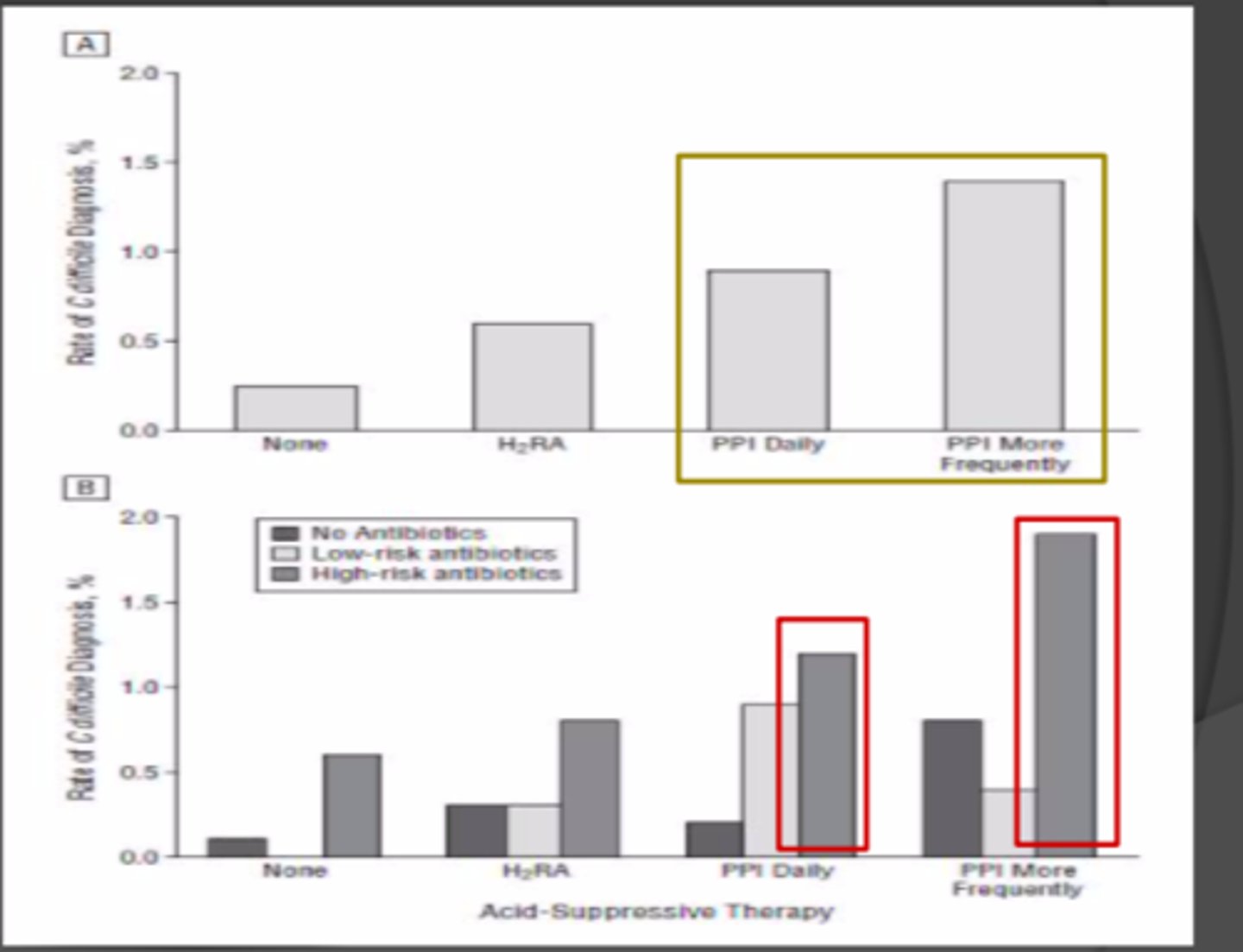
______ suppression and __________ lead to higher C. diff risk
- Acid (suppression)
- antibiotics (lead to higher)
Acid suppression and antibiotics with C. Diff Risk Chart
C. diff presentation - general signs and symptoms
Diarrhea ≥ 3 times a day
Cramps
fever
leukocytosis
inflammation on colonic biopsy
toxic megacolon
dehydration / electrolyte imbalances
ileus
obstruction of the ilium
Disease presentation of C. Diff chart
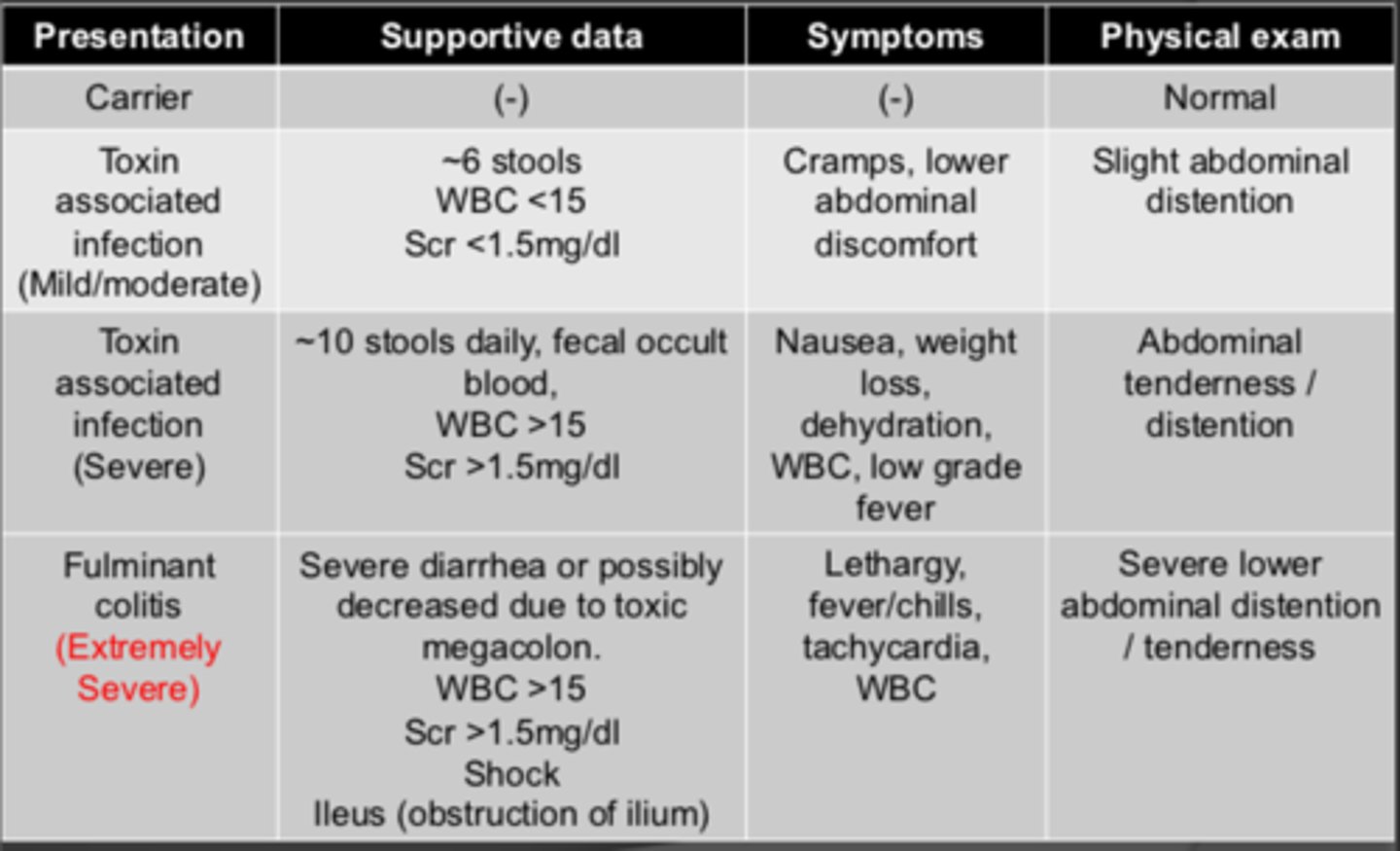
Disease presentation of C. Diff - mild/moderate toxin associated infection
supportive data:
- ~6 stools
- WBC < 15
- Scr < 1.5 mg/dL
symptoms
- cramps
- lower abdominal discomfort
physical exam
- slight abdominal distention
Disease presentation of C. Diff - mild/moderate toxin associated infection (supportive data): ___ stools, WBC ___ _____, Scr ___ ____ mg/dL
- ~ 6 (stools)
- (WBC) < 15
- (Scr) < 1.5 (mg/dL)
Disease presentation of C. Diff - mild/moderate toxin associated infection (symptoms)
cramps
lower abdominal discomfort
Disease presentation of C. Diff - mild/moderate toxin associated infection (physical exam)
slight abdominal distention
Disease presentation of C. Diff - severe toxin associated infection
supportive data:
- ~10 stools daily
- fecal occult blood
- WBC > 15
- Scr > 1.5 mg/dL
Symptoms
- nausea
- weight loss
- dehydration
- WBC
- low grade fever
Physical exam
- abdominal tenderness / distension
Disease presentation of C. Diff - severe toxin associated infection (supportive data): ____ stools daily, positive _______ ________ blood, WBC ___ _____, Scr ___ ______ mg/dL
- ~10 (stools daily)
- positive (fetal occult) blood
- (WBC) > 15
- (Scr) > 1.5 (mg/dL)
Disease presentation of C. Diff - severe toxin associated infection (symptoms)
Nausea
Weight loss
Dehydration
WBC
Low grade fever
Disease presentation of C. Diff - severe toxin associated infection (physical exam)
abdominal tenderness / distention
Disease presentation of C. Diff - FULMINANT colitis (extremely severe)
supportive data:
- severe diarrhea or possibly decreased due to toxic megacolon
- WBC > 15
- Scr > 1.5 mg/dL
- Shock
- Ileus
Symptoms
- lethargy, fever/chills
- tachycardia
- WBC
Physical exam
- severe lower abdominal distention / tenderness
Disease presentation of C. Diff - FULMINANT colitis (extremely severe) - supportive data: _______ diarrhea or decreased due to _______ _______
WBC: ___ _____; Scr ___ ____ mg/dL; shock and obstruction of ilium (________)
- severe (diarrhea)
- (decreased due to) toxic megacolon
- (WBC:) > 15
- (Scr) > 1.5 (mg/dL)
- ileus
Disease presentation of C. Diff - FULMINANT colitis (extremely severe) - symptoms
lethargy
fever / chills
tachycardia
WBC
Disease presentation of C. Diff - FULMINANT colitis (extremely severe) - physical exam
SEVERE lower abdominal distension / tenderness
Complications of C. diff
dehydration
- electrolyte imbalances
hypoalbuminemia
AKI
toxic megacolon or pseudomembranous colitis
sepsis
death
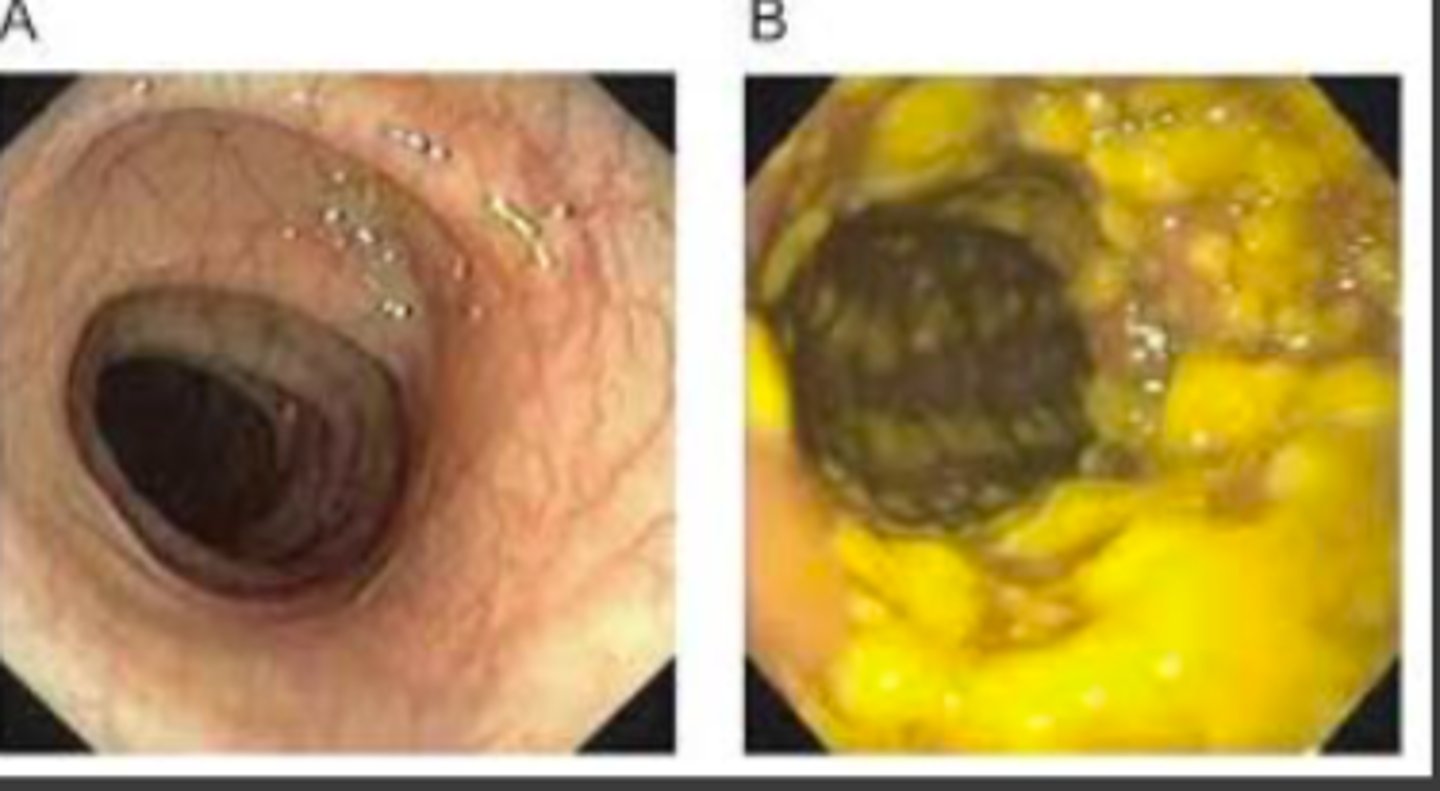
Pseudomembranous colitis figure
A: regular
B: pseudomembranous colitis
Toxic Megacolon X-Ray Figure

FT is a 67 y/o male with NKDA, that was admitted 3 days ago on 3/7/20 for CAP. Today (3/10) FT has had 8 bowel movements that were unformed. He also is complaining of abdominal pain and cramping. WBC were initially trending down (9.2k WBC yesterday), however today they increased to 14.3k and has a fever of 102.4F.
Labs today:
Na 139 mEq/L
K 3.8 mEq/L
Cl 102 mEq/L
Co2 18 mEq/L
BUN 26 mg/dL
Scr 1.1 mg/dL
WBC 14.3 k/cmm
Neut 79%
Bands 6%
Hgb 13.1 g/dL
Hct 43%
Put 230 k/cmm
AST 36 IU/L
ALT 22 IU/L
Alb 4.0 g/dL
T. bili 0.3 mg/dL
Glu 118 mg/dL
Ca 9.3 mg/Dl
Mg 2.1 mg/Dl
Current medications:
Atorvastatin 20mg q24h
Ceftriaxone 1g IV q24h
Azithromycin 500 mg IV q24h
Levofloxacin 500 mg IV q24h
Metoprolol succinate 50 mg q24h
Pantoprazole 40 mg q24h
What are signs/symptoms and risk factors for Cdiff?
FT is elderly (67 y/o), 8 bowel movements (unformed)
- abdominal pain / cramping
- WBC increased to 14.3k
- febrile
Meds (risk factors):
- ceftriaxone (3rd generation)
- pantoprazole
- levofloxacin
Bristol stool chart
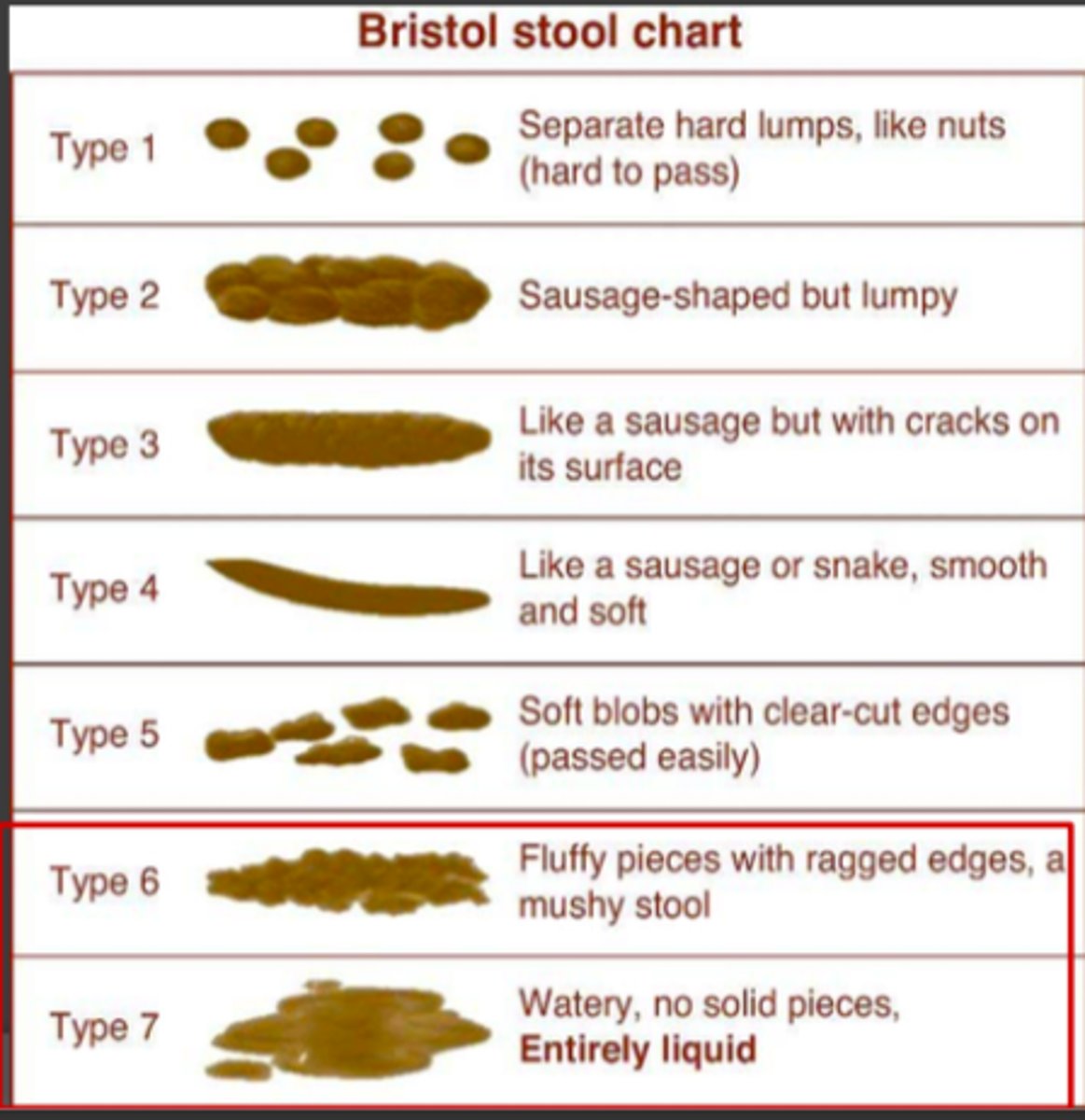
Diagnosis - bristol stool chart for C. diff
Stool sent for lab testing if ≥ 3 type 6 or 7 stools
Type 6
- fluffy pieces with ragged edges, a mushy stool
Type 7
- watery, no solid pieces, entirely liquid
Diagnosis - bristol stool chart for C. diff: stool sent for lab testing if ___ ___ type 6 or 7 stools
- ≥ 3 (type 6 or 7 stools)
Diagnosis - Bristol stool chart for C. diff: stool sent for lab testing if ≥ 3 type ___ or ___ stools
- 6
- 7 (stools)
Bristol Stool Chart - Type 6
fluffy pieces with ragged edges, a mushy stool
Bristol Stool Chart - Type 7
watery, no solid pieces (entirely liquid)
Diagnosis - Bristol stool chart for C. diff: also note that these patients should present without being on _________ or ______-_________
- (without being on) laxatives
- tube-feeding
Laxatives and tube-feeding will have type 6 or type 7 presentation
Diagnosis for C. Diff should not be made on lab tests alone, but needs to consist of the ________ ______ ______ including additional patient objective data
- entire clinical picture
e.g., WBC, PE, symptoms etc.
Diagnosis for C. Diff Lab Testing
PCR for toxigenic genes (high sensitivity, high specificity)
Gold Standard: Cytotoxin assay (high sensitivity, high specificity)
Diagnosis for C. Diff Lab Testing - PCR for toxigenic genes - highly sensitive but ONLY detects ______________, cannot distinguish between ________ infection and __________ carriage
- (ONLY detects) colonization
- (cannot distinguish between) active (infection)
- asymptomatic (carriage)
Cytotoxin assay is the GOLD standard
Diagnosis for C. Diff Lab Testing - GOLD standard
Cytotoxin Assay
May take several days for results
Diagnosis for C. Diff Lab Testing - GOLD standard: cytotoxin assay may take ___________ days for results, requires _______ _________ ________
- several (days for results)
- (requires) tissue culture facility
Diagnosis for C. Diff Lab Testing - PCR for toxigenic genes, results are _________
- (results are) rapid
However, cannot distinguish between active infection and asymptomatic carriage; more expensive than ELISA so needs criteria prior to testing
Nurse sends a stool sample to microbiology lab for C. difficile testing
What are the results needed in PCR and ELISA to confirm C. diff?
PCR testing - Toxin A/B (+)
ELISA testing - Toxin A/B detected
If GENE is there (PCR TEST) does not mean toxin is there, so ELISA is sometimes used
Vancomycin PO
VANCOCIN
Oral vancomycin bioavailability is __________, thus it sits in the intestine to treat ____ _________
- (bioavailability is) low
- (sits in the intestine to treat) C. Difficile
Thus, low absorption and does not need renal adjustment UNLIKE IV vancomycin
Oral vancomycin has ______ ________ due to low bioavailability and does _____ _______ renal adjustment unlike IV vancomycin
- low absorption (due to low bioavailability)
- NOT need (renal adjustment)
No need for monitoring
Initial episode of C. diff (non-severe / mild-moderate treatment) - first line
Vancomycin PO (125 mg QID or NGT for 10 days)
Fidaxomcyin 200 mg PO BID for 10 days
(initial episode non-severe)
Initial episode non-severe is the same as SEVERE except DO NOT use second-line agents
Initial episode of C. diff (non-severe / mild-moderate treatment) - second line
Metronidazole 500 mg Q8 PO for 10-14 days
Initial episode of C. diff (severe treatment)
ONLY first-line used
Vancomycin PO 125 mg QID or NGT for 10 days
Fidaxomycin 200 mg BID for 10 days
(same as first line non-severe, however non-severe may use second line as alternative)
Initial episode of C. diff (FULMINANT / SEVER COMPLICATED)
Vancomycin 500 mg PO QID or by NG tube
- if ileus, consider adding rectal instillation of vancomycin (500 mg in ~100 mL NS)
IV metronidazole 500 mg Q8H should be administered together with ORAL or RECTAL vancomycin, particularly if ileum is present
First recurrence of C. diff treatment: use a ____________ ________ and __________ vancomycin regimen if a standard vancomycin regimen was used for initial episode
- prolonged tapered
- pulsed (vancomycin regimen)
e.g., 125 mg vancomycin QID for 10-14 days, then BID per day for 1 week, QD for a week, then once for every 2 to 3 days for 2-8 weeks
First recurrence of C. diff treatment
prolonged tapered and pulsed vancomycin
OR
fidaxomicin 200 mg BID for 10 days if vancomycin was used for initial episode
OR
vancomycin 125 mg QID for 10-14 days if metronidazole was used for the initial episode
Prolonged tapered and pulsed vancomycin treatment
125 mg QID for 10-14 days
then...
BID for 1 week
then...
QD for 1 week
then...
every 2 or 3 days for 2-8 weeks
First recurrence of C. diff treatment: may use the __________ ______ and _______ vancomycin regimen
- prolonged tapered
- pulsed (vancomycin regimen)
First recurrence of C. diff treatment: if vancomycin was used for initial episode may use __________ ______ mg ________ for ____ days
- Fidaxomycin 200 (mg)
- BID
- 10 (days)
First recurrence of C. diff treatment: if metronidazole was used for initial episode use...
vancomycin 125 mg QID for 10-14 days
Second or subsequent recurrence of C. Diff
Tapered and pulsed vancomycin regimen
OR
vancomycin 125 mg QID PO for 10-14 days FOLLOWED by rifaxmin 400 mg PO TID for 10 days
OR
Fidaxomcyin 200 mg PO for 10 days
OR
Fecal Microbiota Transplantation (FMT)
FMT
fecal microbiota transplant
Second or subsequent recurrence of C. Diff - vancomycin + rifaximin regimen
vancomycin 125 mg QID PO for 10-14 days
FOLLOWED by rifaxmin 400 mg PO TID for 10 days
Primary treatment (1st line) - Vancomycin (VANCOCIN - PO - NO IV)
used for mild / moderate / severe infections and recurrent infections
Primary treatment (1st line) - Vancomycin (VANCOCIN - PO - NO IV) dosing
125 mg PO q6H for 10 days, can give higher dose (250 mg)
In severe, patients give 500 mg
Primary treatment (1st line) - Vancomycin (VANCOCIN - PO - NO IV): has ________ absorption so there is ____ _______ for monitoring levels
- poor (absorption)
- no need (for monitoring levels)
Primary treatment (1st line) - Vancomycin (VANCOCIN - PO - NO IV): Other non-PO option
500 mg in approximately 100 mL NS per rectum Q6H as a retention enema
fidaxomicin
DIFICID
Primary treatment (1st line) - Fidaxomicin (DIFICID - PO) is also used for _______ / _________ / _______ infections and _________ infection
- mild / moderate / severe
- recurrent (infections)
Similar to Vancocin
Fidaxomycin is superior for recurrent infections than initial treatment
Primary treatment (1st line) - Fidaxomicin (DIFICID - PO): superior for ___________ infection
- recurrent (infection)
Rather than initial treatment
Primary treatment (1st line) - Fidaxomicin (DIFICID - PO) _______ ________ spectrum
- very narrow (spectrum)
Primary treatment (1st line) - Fidaxomicin (DIFICID - PO) dosing
200 mg PO q12h for 10 days
Alternative treatment (2nd line) - Metronidazole is used in _______ / _________ CDI
- mild / moderate (CDI)
Alternative treatment (2nd line) - Metronidazole (IV/PO) dosing
500 mg PO q8h for 10-14 days (if patient cannot TAKE vancocin or fidaxomicin)
NO longer first line
Alternative treatment (2nd line) - metronidazole (IV/PO) for SEVERE infection / fulminant colitis
Give 500 mg IV q8H WITH
vancomycin 500 mg PO q6h or 500 mg enema 6qh
Bezlotoxumab
ZINPLAVA