Unit 4
1/95
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
96 Terms
Which STIs are curable ?
Chlamydia , Gonorrhea and Syphilis
Which STIs are not curable but can be treated ?
HSV I , HSV II and HPV
Which STI is being described ?
most commonly reported
patients can be asymptomatic
curable
thin white or clear discharge (penile or vaginal ) is observed
dysuria
Chlamydia
A pregnant woman can give which STD to her baby during childbirth ?
Gonorrhea
What STI is being described ?
thick green or yellow discharge (penile or vaginal )
dysuria
swollen testicles
Gonorrhea
What complications of Chlamydia ?
Ectopic pregnancies , PID , infertility
What is Pelvic Inflammatory Disease (PID ) ?
caused by untreated chlamydia or gonorrhea - sx : pelvic pain , fever , chills
What are factors associated with an increased risk of developing chlamydia ?
being under the age of 25
having a new sex partner
having multiple sex partners
having a partner who is having sex with other people at the same time
having a sex partner with an STI
What are sx that are seen in women with chlamydia ?
Dysuria
abnormal / irregular menstrual cycles
spotting
PID
watery , clear or white vaginal discharge
what sx are seen in males with chlamydia ?
white watery or clear penile discharge
dysuria
penile pain
swelling of testicles (rare )
What tx and education is indicated for chlamydia ?
no sexual contact until 7 days after ABX are completed and sx go away
being tested for HIV and syphilis
what sx are seen in women with gonorrhea ?
painful or burning urination
thick green , yellow discharge
vaginal bleeding between periods
PID
what sx are seen in males with gonorrhea ?
burning when urinating
white , yellow or green discharge
painful or swollen testicles
HSV 1
presents as a round and irritated sore near the mouth
dx : with culture or lab test
lifelong viral infection ; not curable
transmitted through oral contact
HSV 2
presents as a round and irritated sore on the genital area
dx : culture or lab test
life long viral infection ; not curable
transmitted through sexual contact
Patient education on genital herpes
can be treated with daily immunosuppressants
condom use to prevent asymptomatic spreading since it is a virus
will be able to have children
What is the preventative vaccine for HPV ?
Gardasil 9
can be started at age 9 through 45
protects against cancers caused by HPV and genital warts
HPV
a non-curable virus with 80 different types that can cause cervical , anal , penile , vaginal or throat cancer
what is are the sx primary syphilis ?
starts with Chancre sores (large blisters) which heal on their own and virus becomes dormant
what are the sx of secondary syphilis ?
non-itchy rash on hands and feet with a fever
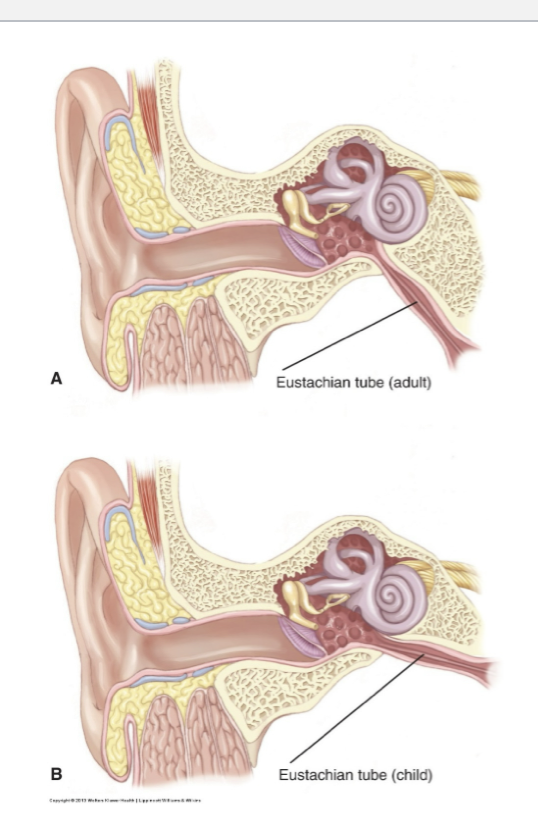
what is different in a child’s eustachian tube vs an adult’s ?
A child’s eustachian tube is shorter and flatter which makes it hard for any infectious fluid to drain
Why is bottle propping not ideal ?
Increases the risk of aspiration
Increased risk for ear infections bc milk can reflux into the eustachian tubes
decreases bonding with caregiver
what is acute otitis media (AOM)
acute infectious process of the middle ear that may produce a rapid onset of ear pain and possibly fever
also otalgia (ear pain )
toddlers will tug at their ears
what is otitis media with effusion (OME)
fluid in the middle ear space without signs and symptoms of infection
what is chronic otitis media with effusion
OME lasting longer than 3 months with perforation of the tympanic membrane (fluid escape through small hole)
what is otitis externa
inflammation of the external ear canal
what are the risk factors for otitis media ?
Eustachian tube dysfunction , recurrent upper respiratory infections , passive smoke (tobacco ) , # of previous ear infections , day care attendance
clinical cues of otitis media
fussiness or inconsolable crying (especially when lying down )
pulling at ears
verbalized ear pain (otalgia )
fever up to 104 or higher
rolling head from side to side
loss of appetite ; refusal to feed
lethargy
fluid draining from ear
swollen lymph nodes
Diagnostic evaluation of Otitis media
fast onset of sx
visual inspection of tympanic membrane
may look dull , bulging or red with visible pus
immobile eardrum of inspection of canal
what are complications of otitis media ?
most common is hearing loss —> gradual decline or deficit
expressive speech delay
tympanosclerosis (ear drum scarring )
perforation of ear drum
intracranial infections (meningitis )
sx management of Otitis media
kids under 6 mo will be given abx doesn’t matter if its bacterial or viral at this age
over 2 mo w/o severe sx will be monitored
sx of uncomplicated lower uti ( bladder or urethra)
fever , vomiting , diarrhea , nocturia , hesitancy , frequency and dysuria
sx of complicated upper uti (kidneys or ureters)
can be asymptomatic or be septic
high fever
cold , clammy or pole skim
disorientation or difficult to arose
what can be a key sx of a UTI in an infant ?
jaundice
sx of uti in infants and children
fever , irritability , tachypnea , vomiting , poor po intake , grabbing diaper , bed wetting , blood in urine
What are some risk factors for a UTI
female
diabetic
pregnancy
gout
any condition that can cause obstruction , urine stasis or foreign body insertion
what are factors that contribute to UTI in older adults
cognitive impairments , frequent use of antimicrobial agents , multiple chronic medical conditions , immunocompromised , low fluid intake or excessive fluid loss
what are risk factors for pyelonephritis?
recurrent utis and urine back flow
What does acute pyelonephritis lead to and what is the tx
leads to inflammation of kidneys and possible abscesses . it causes atrophy and destruction of glomeruli
Tx : two week course of abx
what does chronic pyelonephritis lead to and what is the tx
leads to kidney scarring and progressively lowers kidney function
Tx: long term IV abx
what are potential complications of pyelonephritis ?
end stage renal disease , HTN or renal calculi
What class is amoxicillin ?
penicillin
what are adverse effects of amoxicillin ?
anaphylaxis and furry tongue
what are nursing considerations for amoxicillin?
check for allergies to cephalosporins as there is a high cross sensitivity between both classes
what class is ceftriaxone ?
cephalosporin
what are the adverse effects of ceftriaxone ?
disulfiram - like reaction with alcohol
causes pt to become nauseous , vomit or experience a HA after alcohol consumption
what are nursing considerations for ceftriaxone ?
Do not give if pt is allergic to penicillin , these drugs have a high cross sensitivity as they are both beta lactams
what education should be given to a patient taking ceftriaxone ?
do not drink alcohol during the entire course of abx and for 12 hrs after the last dose
what class is doxycycline ?
tetracycline
what are adverse effects of doxycycline ?
bicycle in sun
photosensitivity (severe sunburn risk )
tooth discoloration ( permanent yellow/brown stains in kids )
what are nursing considerations for doxycycline ?
do not give to pregnant women or kids under 8
do not give with dairy , antacids or iron
these bind to drug and stop absorption
what class is gentamicin ?
aminoglycoside
what are adverse effects of gentamicin ?
ototoxicity (irreversible hearing loss or tinnitus)
nephrotoxicity ( kidney damage )
what are nursing considerations for gentamicin ?
check peak and trough levels : narrow therapeutic window , trough needs to be drawn 30 min before next dose
monitor urine output : let provider know if under 30 ml/hr
monitor BUN and CR
Red man syndrome
Red rash from rapid IV administration of gentamicin or vancomycin
sx : hypotension , flushing and itching

what class is vancomycin ?
glycopeptide
what are the adverse effects of vancomycin ?
otoxicity : irreversible tinnitus and hearing loss
nephrotoxicity : kidney damage
red man syndrome
what are nursing considerations for vancomycin ?
narrow therapeutic window → check peaks and troughs
closely follow infusion rate instructions
what class is ciprofloxacin ?
fluoroquinolone
what are adverse effects for ciprofloxacin ?
BLACK box warning : achilles tendon rupture
QT prolongation : can cause cardiac arrhythmias
what are nursing considerations for ciprofloxacin ?
monitor pt for tendon pain / inflammation
ask if hx of myasthenia graves (can worse muscle weakness)
take any multivitamins , antacids (tums ) or dairy products 2 hrs before or after this med
what class is azithromycin ?
macrolide
what are the adverse effects of azithromycin ?
hepatotoxicity (liver damage )
contraindicated in pts that are lactating
what are nursing considerations for azithromycin ?
monitor liver function tests (LFT)
do not give to patients that are lactating
what is clotrimazole ?
a topical anti-fungal
what is nystatin ?
a topical or oral anti-fungal
what are three main priorities of abx administration ?
culture before first dose of abx
monitor for allergies
monitor for s/s of secondary infections like c. diff or oral candidacies
what is the peak level
highest concentration of abx in blood
too high kidney will die
is drawn 1 ½ hr after administration
what is the trough level
lowest concentration of abx in blood
too low bacteria grows
is drawn 30 min b4 next dose
Healthcare associated MRSA
associated with invasive procedures or devices like surgeries , IV tubing or artificial joints
spread by HCW touching ppl with unclean hands or by ppl touching unclean surfaces
Community associated MRSA
starts as a painful skin boil
spread by skin to skin contact
ppl at risk are high school wrestlers , childcare workers or ppl that live in crowded conditions
what are s/s of MRSA
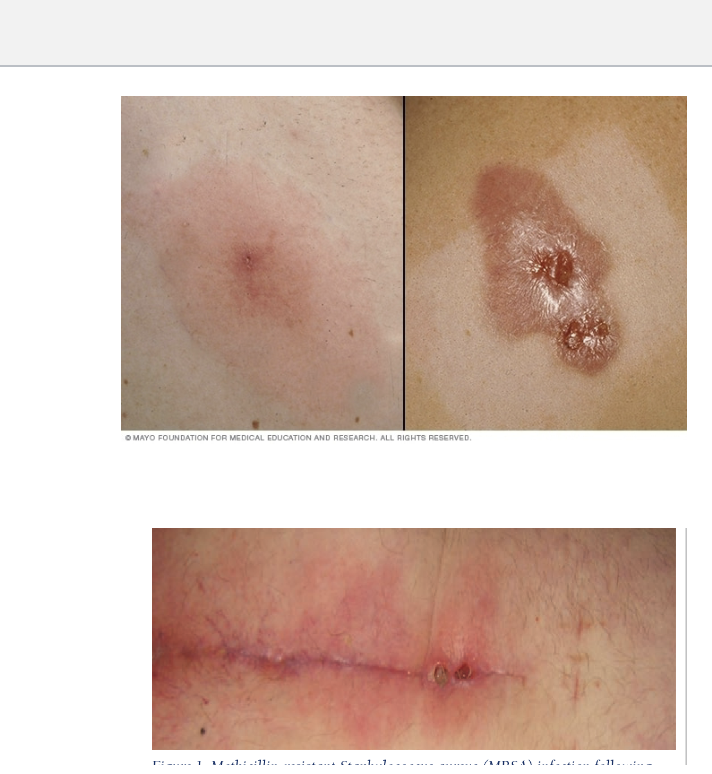
Starts as swollen, painful red bumps that may resemble pimples or spider bites.
Lesions can feel warm and may contain pus.
fever
progresses to deep, painful boils.
what is the cause of bacterial meningitis?
caused by bacteria (meningococci and pneumococci )
what is the cause of viral (aseptic )meningitis ?
caused by viruses such as
enteroviruses (echovirus or coxsackievirus )
measles , mumps , herpes virus , HIV , varicella or influenza
Bacterial meningitis pathophysiology
Bacteria enter CSF → multiply
Release toxins → inflammation
↑ Blood brain barrier permeability
WBCs + bacteria → pus
Brain swelling + ↑ ICP → headache
brain is covered with a layer of pus
commonly seen in school age children to adults
viral meningitis pathophysiology
Virus infects meninges
Mild inflammation
No pus
↓ ICP compared to bacterial
Symptoms less severe
s/s of meningitis
Will be the same regardless if viral or bacterial
fever , HA , drowsiness, nuchal rigidity , photophobia , poor feeding , n/v , neck pain
positive kernig and brudzinski signs
seizures , weak cries
flat / bulging fontanels
rash → late stage
how do you differentiate between the manifestations of viral and bacterial meningitis ?
Patients with viral meningitis will appear less ill
sx appear suddenly with bacterial
sx come on gradually in viral
How is meningitis treated in babies if we are unable to obtain a CSF sample ?
Will need to be treated as if it were bacterial meningitis
what cues of mengitis are not typically present in children under 12-18 months
nuchal rigidity , brudzinski , kernig
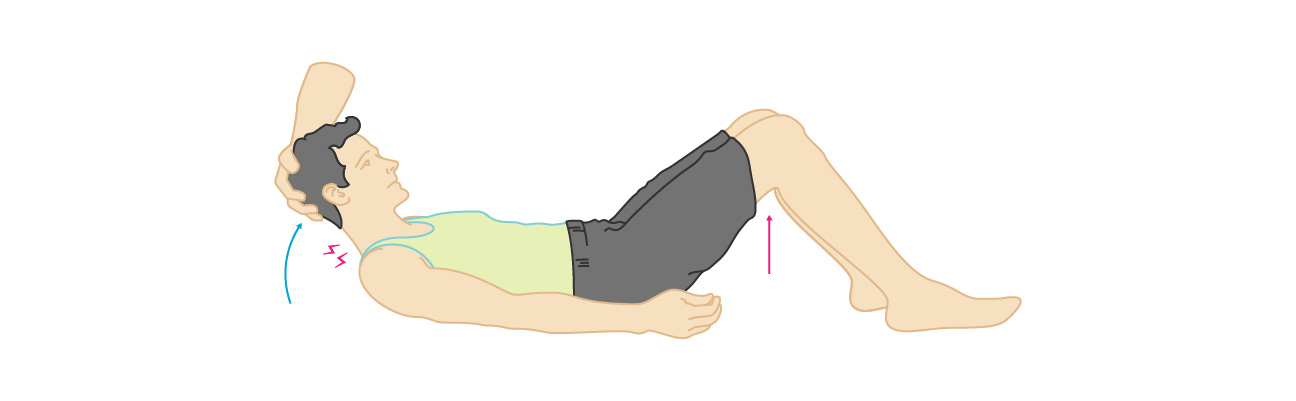
What is a positive brudzinski sign
Severe neck stiffness that causes pt’s hips and knees to flex when their neck is flexed
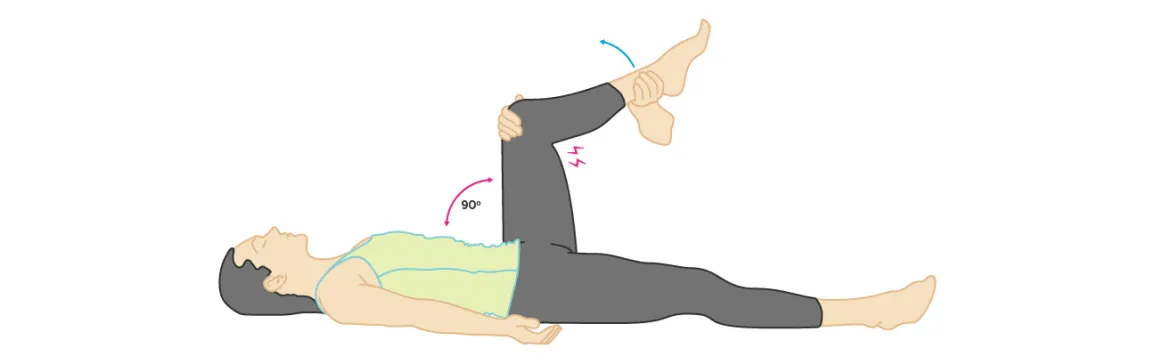
what is a positive kernig sign
severe stiffness of hamstrings causes an inability to straighten the legs when the hip is flexed to 90 degree’s
What will children do as meningitis progresses and what is that position called ?
Opisthonos postion to avoid flexing the neck
The child will hyperextended their neck to relieve pain

what CSF results should we except in bacterial meningitis ?
elevated —→ csf pressure , wbc ,neutrophils
decreased → glucose
positive bacterial culture
cloudy color
what is a definite diagnostic test to distinguish between viral or bacterial meningitis ?
Lumbar tap
what CSF results should we expect in viral meningitis
normal → CSF pressure , Glucose
normal / slightly elevated → wbc , protein
negative bacterial culture
clear or slightly cloudy color
Nursing management for bacterial meningitis
medical emergency
contact and droplet isolation
IV abx (7-21 days )
control temp
control or prevent seizures
hydration (over hydration can increase output and positon changes )
dark room
corticosteroids to lower inflammation
Nursing management for viral meningitis
Symptom management
antipyretics
hydration
side lying in dark quiet room
can be managed at home
tx is 3-10 days
What is sepsis ?
A life-threatening organ dysfunction caused by infection
what is SIRS (systemic inflammatory response syndrome ) ?
a body wide inflammatory response that can be infectious or non infectious
SIRS criteria
Temp: > 38 or < 36 celsius
HR : > 90
RR : > 20
WBC
AMS