Pediatrics midterm (copy)
1/36
Earn XP
Description and Tags
studying time again :(
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
37 Terms
What is motor learning? (Not directly what? Requires what two things?)
Motor learning vs performance?
Permanent change from practice
Not directly observable
Requires repetition + engage
Performance is temporary while motor learning is longer lasting (neuroplasticity)
Watch over time: For example, a patient may walk better during therapy because you are giving verbal cues, providing manual assistance, or allowing repeated practice. That shows improved performance in the moment. To determine whether motor learning occurred, you would check whether the patient can still perform the skill later, such as at the next session or after several days, with fewer cues or no assistance.
Stages of learning:
What are the 3 stages of learning?
Feedback:
Intrinsic vs extrinsic feedback? KR vs KP?
Practice structures:
Blocked (specific) vs random? Massed vs distributed?
Stages of learning:
Cognitive
Needs higher level of cognition, understanding the nature of the task and developing strategies that can be used to carry the task out.
Associative
Can last days to weeks to months depending on the performer/intensity. Patients select the best strategy for the task and begins to refine that strategy.
Autonomous
Automaticity of the skill. Lower degree of attention required to preform skill (Ex: talking to someone while doing the task)
Feedback:
Intrinsic
Comes from various sensory systems. Involves the body’s own understanding of how we move: includes auditory, visual, and somatosensory feedback.
Extrinsic
Supplements intrinsic feedback. Shifts learner to use awareness of results.
KP (Knowledge of performance)
Feedback given from a task
KR (Knowledge of results)
Terminal feedback about the outcome of a movement in terms of movement goals (For instance telling a patent how high to step over something or using mirrors and force plates)
Practice structures
Blocked
practicing the same skill repeatedly before moving to another skill.
Random
Mixing different skills together in an unpredictable order. Most effective when used with skills that use different patterns of coordination.
Massed
Amount of practice time in a trial > amount of rest between trials. Work > rest.
Distributed
Amount of rest between trials ≥ amount of practice time in the trial. Rest ≥ work.
How can we encourage motivation in pediatric care?
What type of training is ideal of pediatric population?
Motivation: Use play and child centered activities
Task specific training: Practice real life tasks; functional goals MATTER!
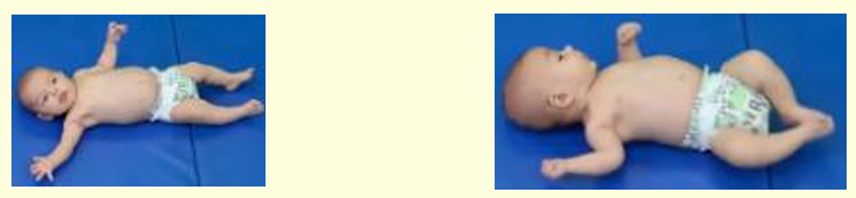
Neonate
Everything in this stage is controlled by?
What type of movements can we expect from the extremities?
What posture can be seen in this stage? Why?
What hours are newborns most likely to move in?
What type of objects are detected better in this stage? How about tracking? These stimulates what two things?
In this stage, the infant is mostly interested in what three things? What is vital during this stage?
Everything is controlled by gravity
Random extremity movements
Physiological flexion: elbows, hips, knees, and ankles
Fetal position
Newborns mostly move during wake/active hours
High contrast objects (black/white) are detected better, briefly tracking objects
Stimulates visual acuity and eye tracking
Mostly interested in eating, cuddling, caregiver attention
Auditory responses are vital→ be attentive/talkative
Neonate - Supine
LE:
What posture would be seen in the LE?
If hip flexors are tight, this will limit what motion? What about for hamstrings?
Dorsiflexion increased ROM to?
Hips have? (5)
LEs have? (6)
UE:
What posture would be seen in the UE?
Hand and mouth play will occur due to?
Head and vision
Why does rolling happen on accident?
Asymmetrical positions of head and neck is okay because?
______ tracks a toy (from their _____ to _____)
How far does the toy have to be? This helps mobilize what?
LE → physiological flexion (hip Flx, Abd, ER)
Tight hip flexors = limited extension; tight HS = limited knee extension
DF ↑ROM: ~60°
Hips have: medial femoral torsion, anteversion, bowing, coxa valga, shallow acetabulum
LE’s have: genu varum, tibia varum, tibial torsion, calcaneal varus, forefoot varus, ~metatarsus adductus
UE → Shoulder Add + ER, elbow flx, and forearm pronation
Hand to mouth play due to flexed elbow and rotated head
Head and Vision → Rolling happens by accident due to neck righting reaction and rooting reflex
Asymmetrical positions of head + neck is ok because of no midline control
Briefly tracks a toy (from their side to midline)
Needs to be 8-9 inches away
Mobilize head + neck by holding objects 8-9 inches away (using visual stimulation)

2 months
Biggest period of? (TEST QUESTION!)
Infant continues to practice what two things with the UE? (This is the number one goal of UE movement)
Fine motor control is still _______ during ________ movements.
Social behavior and language?
BIGGEST PERIOD OF ASYMMETRY (test qst)
Infant continues to open/close hands and practice reaching (still 1st goal of UE movement)
Fine motor control is still grasping during spontaneous movements
Same social behavior and language as one month
Visual preferences for humans
Moves in response to a voice
Vocalizes to caregivers smile and voice
2 months - supine
In terms of posture, what decreases?
Movements are?
Attempts to interact more with? What starts to come into play?
Head and vision:
Eye tracking from _____ to ______, and now can do what?
Greater degree of? This is directed by? Is chin tucking present?
This may stimulation what proprioceptors? This will in turn elicit?
UE:
Moving more into what two motions?
LE:
At rest, what motions can be seen but with more flexibility?
Actively, what movements can be seen?
Supine:
Less physiological flexion
Disorganized movements
Attempting to interact more w/ environment, swiping toys, + looking at facial expressions
Emotional intelligence coming into play
Head and Vision:
Eye tracking from side to midline and now back to side again
GREATER degree of head rotation, directed by visual attention (no chin tuck)
May stimulate neck proprioceptors which elicit ATNR (most evident in 2nd month)
↑ ATNR b/c ↑ mechanic receptors
UE:
moving more into Abd + ER
LE:
at rest: flx, abd, + ER (more flexible though)
actively: variety of LE movements (kicking alternatively or symmetrically)
2 months - Prone
Head:
Briefly lifts head how many degrees? The extension is? This is due to?
UE:
Begins to use arms to? Elbows are still?
LE:
Decrease in what two motions?
Decrease tightness in what two things?
Spine:
Increase in cervical and thoracic _____.
Prone
Head:
briefly lifts head ~45° with ASYMMETRICAL EXT. (no midline control still)
UEs
begins to use arms to push up in prone (elbows still posterior to shoulders)
LEs
decrease hip abd and ER
decrease hip flexion and HS tightness
Spine
increase in cervical and upper thoracic extension

3 months
Still cannot be?
Less _____ _____ noticed
Social behavior and language
Listens to?
Smiles purposely in response to?
To get attention, the baby will?
Crying decreases with? Why do they vocalize?
What about emotional intelligence?
Still cannot be left alone
Less head lag noticed
Social Behavior and Language:
Listens to voices → toys can sing/make noise
Smiles purposely in response to caregiver’s face or voice
Coos or cries to get attention
Crying decreases with adult contact; they vocalize to express displeasure
increased emotional intelligence

3 months - Prone
Head and neck:
May lift head ___ degrees to ____ degrees, in ______ with no _____. Tracking to how many degrees?
Eliciting what motion at the neck? This helps increase what and decrease what?
Due to head shifting, this will cause a lateral weight shift. How would this impact the UE?
Increased effect of ________ and ______ ______ reactions.
Because of the increase in what?
Increased head movement will increase what and help prep the baby for what motion?
A lack of labyrinthine receptors can lead to?
Spine:
Increase in spinal ____.
UE:
What can be seen in the forearms? This combined with _____ _____ and elbows aligned with _____ or in front of ______.
What movements can be seen in the fingers? This means we are starting to see what?
LE:
Asymmetrical or symmetrical?
Increase ______ at hips and knees.
Decrease in?
Ankles will begin to?
Head and Neck → lifts head ~45° to ~90° in midline w/ no bobbing + tracking to 180°
Eliciting chin tucks = increased visual tracking; decreased head lag
Head shifting will cause lateral weight shift; might shift to one arm b/c of ↑ head rotation
Increased effect of the labyrinthine and optical righting reactions
B/c of the increased eye tracking up to 180°
increased head movement = increased vestibular priming + prepping for ROLLING
A lack of labyrinthine receptors can lead to developmental loss of coordination and/or dizziness
Spine
Increased spinal extension
UE
forearm WB (propping) with shoulder ABD and elbows ALIGNED with shoulders or in front of shoulders
scratching movements with the fingers = starting to see release of flexion
LEs
symmetrical
increased extension at the hips and knees
- decreased ER
- Ankles begin to fluctuate between DF and PF

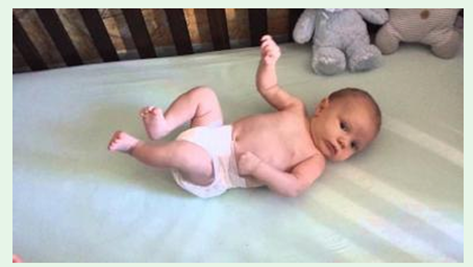
4 months - supine
Period of _____, ______ ______ of the head and hands.
What extremity movements are dominant?
Rolling from what position to what position is seen?
This rolling can be initiated by what two things?
What is the posture during the rolling?
LE
Hands to?
Kicking legs _____ or _____ (pushing)
What play can be seen?
Begins to use what two active hip motions? This indicates some?
Head and neck
What gaze develops with head flexion? This causes what activation?
UE
What bilateral pattern can be seen? During this pattern the forearm is in supination or pronation? wrist is in flexion or extension?
What coordination increases?
Spine
What posture is seen?
Trunk moves as?
Active anterior and posterior _____ _____ is seen (sagittal plane)
Side lying helps with what 5 things? This new position gives tons of?
Supine:
Period of symmetry, midline orientation of head and hands
Bilateral symmetrical extremity movements are dominant
ROLLING supine to side lying is seen
Initiated by head rotation or by an asymmetrical position of LE which causes a lateral weight shift
Flexed posture
LEs
Hands to flexed knees:
kicking legs symmetrically or reciprocally (pushing)
foot on foot play
BEGINS to use active hip add with hip flexion (some purposeful movement)
Head and Neck
downward gaze develops with head flexion (chin tuck activation)
UEs
bilateral REACHING pattern towards toys with forearm pronation + wrist extension
Increased hand-eye coordination
Spine
Flexed posture
Trunk moves as one unit
Active anterior and posterior pelvic tilting is seen (sagittal plane)
Side lying rib cage shaping, head shaping, new visual orientation, vestibular orientation, proprioceptive feedback. TON of sensory feedback

5 months
Social behavior and language
Laughs: laughs at? What else will the baby do now?
Excited about? Turns heads towards a?
Propped sitting
How long can the baby maintain this propped sitting? How does the baby maintain its balance? This sitting is also known as?
Social Behavior and Language:
Laughs; laughs at self in mirror (mirror therapy); laughs and babbles (blowing raspberries)
Excited about food; turns head towards a voice
PROPPED SITTING:
Can maintain propped for ~8 seconds
Maintains balance by propping UEs
AKA Tripod sitting

6 months - supine
Before talking about supine, what type of sitting would be seen in this month and why?
Supine:
For hands and feet play, hand to feet is now?
What type of play facilitates rolling?
Maintains and recovers balance with?
Pelvis off the surface shows good?
Rolls from what position to what position and vise versa?
This is initiation with what two things?
Controls weight shifting with what two things?
Has mastered what movements in supine and prone?
RING SITTING with wide BOS (b/c still has lack of control in abs)
Supine:
Hands to Feet play → now contra-lateral hand to feet
Transverse play facilitates rolling!
R UE to L LE play
Maintains + recovers balance with legs lifted in supine
Pelvis off the surface showing good abdominal strength
Rolls supine → prone and prone → supine
Initiated with flexion + dissociated LE
Controls WS with abdominals + NWB leg
Has mastered antigravity movements in supine + prone

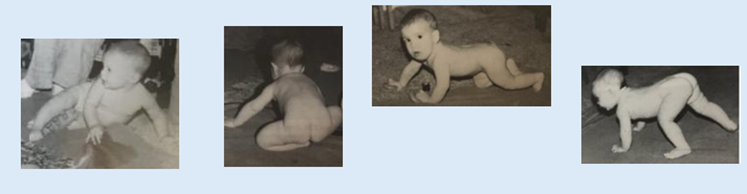
7 months - floor transitions
What education can you give to the caregivers?
Floor transitions
What position does the baby rarely stay in (red flag otherwise)?
Rolling out of what position? Baby has to be doing what two things?
For sidelying, the baby will dissociate UE or LEs? Plays in low or high sidelying?
For quadruped, Rocking anterior to posterior:
can be a primer for?
Initially the movement is what and may cause what?
Later the movement becomes what and this means a decrease in?
What spinal curve can be seen initially and will decrease with repetition and practice?
Quadruped transitions:
Baby can go from ____ to quadruped or ______ to quadruped.
Required the ability to dissociate UE or LE?
Increase in what control?
Increase in ____ and proximal ____/____ strength.
What is bear crawling?
Education for caregivers: crib now needs to be lowered. Baby proof house! Objects need to be secured
Floor Transitions:
Rarely stays in Supine (RED FLAG OTHERWISE)! Rolling out of supine! Baby has to be moving and transitioning
Side lying: dissociates LEs and plays in high side lying
Quadruped → (may have started @ 6 months). Rocking A/P:
Primer for crawling
Initially, large movements, perhaps falling over
Later, finer more controlled, decrease falls
Lumbar lordosis is present initially and decrease with repetition/practice
Quadruped Transitions:
Prone into quadruped or sitting into quadruped
Required ability to dissociate LEs
increase weight shift control
increase trunk and proximal hip/GH strength
Bear Crawling → transitions from quadruped postures into bear (pushing butt up)
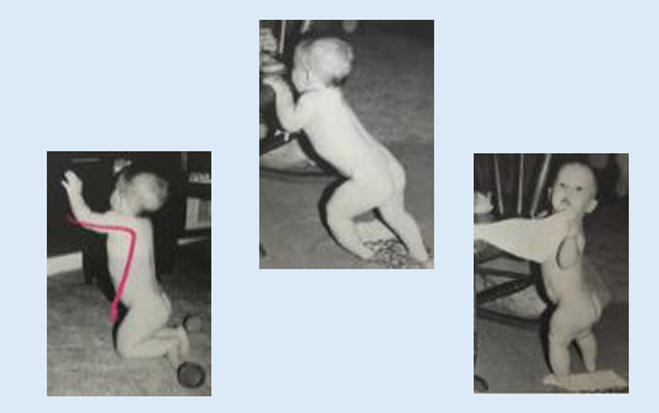
Month 7 - Standing transitions
For pulling to stand, this movement relies heavily on? What positions can the baby do pull to stand from?
For standing at furniture, feet are supinated or pronated? Toes are? How do they return back to the floor?
Pulling to Stand
relies heavily on UEs to pull up on furniture or people from quadruped or kneel sit and stiffly extends knees
Standing at Furniture
feet pronation with toe curling
returns to floor by “falling”
9 months - sitting
In this month, sitting is? Transitions are?
In this month, the baby has good control of? What variety of LE posture will the baby use for sitting? Of all postures, which one should be discouraged when overused?
Continues practicing what motion?
May use what sort of pattern to get around? If they continue to use this pattern for a prolonged period of time, what does that mean?
CRAWLING for how many feet?
Independent and functional sitting; smooth transitions
Good trunk/pelvis control, now using a variety of LE postures:
Ring sit
Long sit
Side sit
W sit (normal, but if prolonged → risk of femur malalignment. Should be discouraged when overused)
Easily transitions in/out of sitting
Continues practicing trunk rotations
May use scooting pattern (comes in ~9 months; if remains, something is up)
Crawling (creeping on hands and knees) for 5 feet

Cross extension reflex
Occurs when?
Age of integration?
Stimulated when/with? What would be the response?
Occurs @ onset-birth
Age of Integration (AKA goes away, AKA AKA embeds in spinal cord, AKA AKA AKA maturing): 2 months
Stimulated when noxious stimulus is applied to ball of foot of LE fixed in extension; tested in supine position
The response to the stimulus: Opposite LE flexes, then adducts and extends

Startle reflex
Very similar to what other reflex?
Occurs when?
Age of integration?
Stimulated when/with? What would be the response?
Interferes with?
Very similar to the Moro Reflex
Occurs @ onset-birth
Age of Integration: DOES NOT INTEGRATE
Stimulated with sudden loud or harsh noise
The response to the stimulus: Sudden extension or abduction of UEs, crying
Interferes with:
- sitting balance
- protective responses in sitting
- hand-eye coordination
- visual tracking
- social interaction/attention
Rooting reflex
Occurs when?
Age of integration?
Stimulated when/with? What would be the response?
Interferes with?
Occurs @ onset-birth
Age of integration: 3 months
Stimulated with touch on cheek
The response to the stimulus: Turns head towards touch and opens mouth (think of mother’s nipple for breastfeeding).
Interferes with:
- oral-motor development
- midline head control
- optical righting
- visual tracking
- social interaction (speech)

Asymmetrical tonic neck reflex (ATNR)
Occurs when? Helps the infant do what and learn what?
Stimulated when/with? What would be the response?
Age of integration?
Interferes with?
Present at birth → develops around 18 weeks in utero
Helps the infant emerge through the birth canal and learn hand-eye control
Stimulated with head rotation to one side
The response to the stimulus:
Arm and leg on face side are extended, arm and leg on scalp side are flexed (Fencer positioning)
R head rotation = R arm + leg extended, L arm + leg flexed
The spine is curved with convexity toward face side
Age of integration: 4-6 months
If integration doesn’t occur → problems with hand-eye coordination, difficulty reading, immature handwriting + struggles with math

Moro reflex
Occurs when?
Age of integration?
Stimulated when/with? What would be the response?
Occurs @ onset-birth
Age of integration: 5-6 months
Stimulated with sudden changes in position of head in relation to trunk
by dropping patient backwards from sitting position the baby will reproduce this moro reflex/ startle reflex
extension when falling back
The response to the stimulus:
UEs will extend, abduct
Hands will open
Crying followed by flexion, adduction of arms across chest

Plantar + Palmar grasp reflex
Occurs when?
Age of integration for each?
Stimulated when/with? What would be the response?
Each Interferes with?
Occurs @ onset-birth
Age of integration:
Palmar reflex → 4-6 months
Plantar reflex → 9 months (b/c starting to stand/balance)
Stimulated with maintained pressure to palm of hand (palmar grasp) or to ball of foot under toes (plantar grasp)
The response to the stimulus: Maintained flexion of fingers/toes
Palmar reflex interferes with:
grasping and releasing objects voluntarily
weight bearing on open hands for propping
crawling
protective responses
Plantar reflex interferes with:
ability to stand with feet on surface
balance reactions
weight shifting in standing

3 years (39-46 months)
At this point, the child is able to do what two things? For each how are they tested?
Cognition, language, and social-emotional:
For cognition, what are some things we can do to test it?
For language, what would we expect to see?
For social-emotional, what would we expect to see?
Walking and Standing
Walking → walking a 4-foot line without stepping off
Standing → standing on tippy toes for 3 seconds (hands held overhead)
Cognition, Language, and Social-Emotional:
Cognition: tells a simple story
Counts up to 5; counts 5 objects
Puts together a puzzle
Follows a 3-step command
Language: speaks in complex sentences
More complex language; scribble writing
Social-Emotional: shows an interest in how things work, always asking “why”
Can learn aggressive behavior rapidly if taught
Has a hard time with conflicts
Participates in circle time, games, drawing and art time (learns a lot from home environment; emotional regulation)
4 years (47 - 54 months)
47-48 months: When it comes to hopping, how many times would be typical? What about on the non preffered foot?
51-52 months (just over 4 years old): When it comes to standing on tip toes, how long would we expect for them to hold that position for without too much sway? How much sway is allowed?
53-54 months (4.5 years old): When it comes to jumping, how far forward is expected? When jumping and turning, how many degrees is expected and how much deviation is allowed?
47-48 months
Hopping on one foot 5 times
o 3-5 hops on non-preferred foot
51-52 months (just over 4 years)
Standing on tip toes for 8 seconds without swaying >20 degrees (hands held overhead)
53-54 months (4.5 years old)
Jumping 36 inches forward
Jumping + turning 180 degrees (not deviating more than 20 degrees)

Clubfoot (Congenital Talipes Equinovarus)
What foot position can be seen with this condition? (At the forefoot, at the hindfoot, and at the ankle)
Deformities of the _____ bones and the joint ______ changes happen due to the distorted position
Ligament are _____ and muscles are ______ and ______.
What is the goal for treatment? What type of casting can be used to help address this deformity?
How often a week should this cast be used?
How does it correct the issue?
After 4-6 casting, may require what surgery?
Most can change to a brace for how many months? When can they begin using the brace? Once they wear the brace for the allotted time, a sleep brace can be used for how long after?
Forefoot adductus, hindfoot varus + ankle equinus
Deformities of the tarsal bones and joint capsule changes happen due to the distorted position
Ligaments are thickened and muscles are weakened and atrophied
Goal for Tx: Correction of deformity and retain mobility and strength
Ponseti method serial casting → semi-weekly or weekly
Correcting the cavus by rotating the foot from under the talus and correct the equinus
After 4-6 castings = may require Achilles tenotomy to lengthen the tendon
Most can change to a brace for 3 months after the 4-6 weeks, followed by a sleep brace for 2-4 years


Developmental dysplasia of the hip
What is it? How can it be clinically examined/screened for?
What is the treatment? How does it work? Enhances? How does kicking in it help? If this treatment is not successful then what can be done?
Instability at the hips due to dislocation of the femoral head
Clinical Examination: clinical screen using =
Barlow Maneuver
Ortolani Test
Diagnostic scans
Tx: Pavlik Harness (from birth to 6 months)
Creates abduction and flexion of the hips
Enhances acetabular development
Kicking in this position stretches the contracted hip adductors and promotes spontaneous reduction of the dislocated hip
If not successful, then surgery is needed

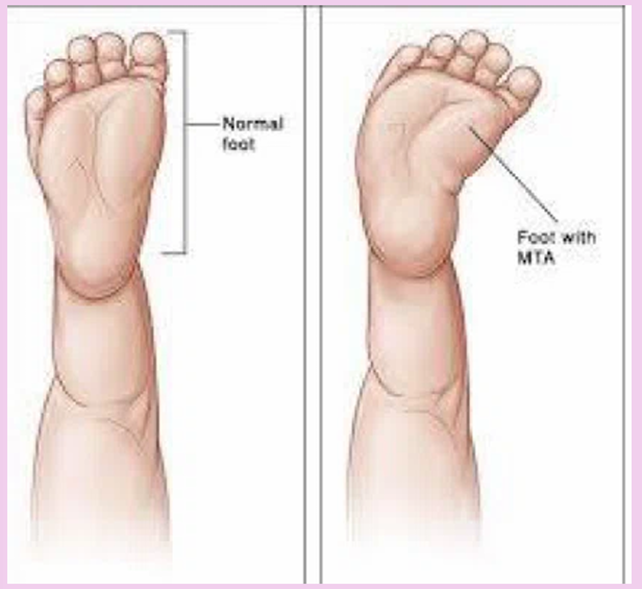
Torsional conditions: Metatarsus adductus/metatarsus varus
What is it? Causes what?
How is the forefoot in relation to the hindfoot?
Patients under 3 have a flexible?
Patients over 4 tend to develop a?
When is best to intervene?
A forefoot deformity at the tarsometatarsal joints, causing contracture of the soft tissues around this joint
Forefoot is ADDucted in relation to the hindfoot
Patients under 3 have a flexible metatarsus adductus
Patients over 4 years old tend to develop a more rigid deformity
Best is to intervene when they are young because you’ll have pliable tissue that you can mold
Torsional conditions: In-toeing
What three things can play a role in causing in-toeing?
What 4 interventions can be done to help? What age can they be done? What if its severe?
Femoral antetorsion AND anteversion: can play a role in causing in-toeing (version = angular difference between the transcondylar axis of the knee and the axis of femoral neck)
Internal Tibial Torsion
Different interventions orthopedic doctors utilize to help correct internal tibial torsion after 18 months of age are:
Friedman counter splint
Flexible leather strap/Denis Browne bar
Wheaton brace
Tibia counter rotator with toe-out gait plate
Surgical correction if severe

Torsional conditions: Flat foot
For flexible flat feet, what can be seen happen to the arch of the foot?
For rigid flat feet, what is the percentage of it being present of the flat foot pediatric population?
Typical causes?
Flexible Flat foot: Normal arch during non-weight bearing and a flattening of the arch on stance that may be symptomatic or asymptomatic
Rigid Flat Feet: Present in only 1% of flat feet in pediatrics
Typical causes:
Tarsal coalition → involves 2 or more tarsal bones; reduces movement; foot pain; difficulty with gait
Congenital vertical talus → presents in infancy as a rigid rocker bottom
Talus is PF’d and the navicular is dislocated dorsally on the talus
Contractures of the Achilles tendon and the extensor digitorum longus muscle are seen
Usually needs corrective surgery and casting

Antetorsion
How does this occur? How does it impact the femoral shaft?
How is this different to retroversion?
At birth, the normal developing femur has a max antetorsion of how many degrees?
Rapid angular decreasing during what year(s)?
Slow angular decrease during what year(s)?
Rapid angular decrease again during what year(s)?
How can the femur return to normal?
Occurs when the head and neck of the femur are rotated forward in the transverse plane compared to the femoral condyles, A FORWARD twist of the femoral shaft.
If rotated posterior (backward); its called retrotorsion
At birth, the normal developing femur has a max antetorsion of 30-40 degrees
RAPID angular DECREASE during the infants first year
SLOW angular DECREASE during 1-8 years old
RAPID angular DECREASE AGAIN during adolescence to 14-16 years
The femur will untwist through the process of growth, muscle action, reduction of coxa valga angle and hip flexion contracture

Causes of limping in children:
Legg calve Perthes disease
Affects what of the immature femur?
Blood supply to where is lost, causing it to start to die/necrosis?
What can be done intervention wise?
What age does this occur in?
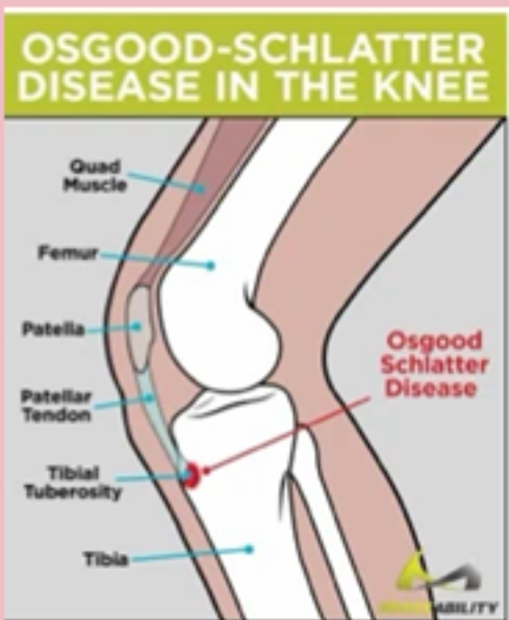
Osgood-Schlatter Syndrome
What is it?
Very common in what age of children?
Treatment focuses on what 2 things?
Osteomyelitis
What is it? How can it occur? What part of the bones and what extremity is this usually occurring in?
Legg-Calve- Perthes Disease: affects the capital epiphysis of the immature femur
Blood supply to the head of the femur loses blood supply and it starts to die (necrosis)
Surgical intervention to help relocate the femoral head in the acetabulum
Bracing is also an option
Occurs in children 4-10 years of age
Osgood-Schlatter Syndrome: activity related pain at the anterior knee due to repetitive traction of the patellar tendon on the tibial tubercle causing ossification
Very common in children 14-16 years of age
Treatment: focus on patellar tracking and stabilization exercises
Osteomyelitis: highest incidence in children under the age of 3 years
Autoinflammatory bone disease that presents with pain and signs of inflammation due to:
Infected wounds
Open fractures in which broken bones penetrate through the skin
Foreign object penetrating the skin
Infected joints or infections spreading from another source inside the body (ear infections)
Trauma
Usually found in the ends of long bones and usually the LEs
Models of service delivery
Direct model
Child is seen _____ __ _____. This type is the most?
Emphasis on?
How is it scheduled?
Consultative model
In this model, the therapist interacts with who and for what reason?
PT will work on?
Visits depends on?
Who will mostly intervene?
Monitoring model
Provides information for?
May be seen every ____ months to access what?
Integrative model
Therapist interacts with who and for what reason?
Student will practice what skills?
How it it scheduled?
Collaborative model
Interactive team process that focusses on what to improve what?
Who makes the goals for the student/child?
Direct Model:
Child is seen one-on-one, most common type of service provided
Emphasis is on acquisition of motor skills
Regularly scheduled
Consultative Model
Therapist interacts with the team members, including parents, who implement the recommended activities
PT will work on positioning and adapting environment
Visits will depend on staff member
Teacher will mostly intervene
Monitoring Model
Provides information to team members, monitor a student’s progress, equipment needs, etc.
Maybe seen every 6 months to assess the need for therapy or more adaptations
Integrative Model
The therapist interacts with the child, team members within the learning environment, and several people are involved in implementation oof the therapy program
Student will practice skills already acquired during the direct care portion
Routinely scheduled visits
Collaborative Model
Interactive team process that focuses on student, family, education, and related service providers to improve academic and functional performance of all students in school
The team makes the goals for the child/student
IEP: Individual education program
The IEP or plan is a written statement that includes what 5 things?
Statement of measurable annual goals: academic and functional
Goals are developed dependent on? What about PT support?
Not _____ specific
Not written in what language, but rather in?
PT develops plan of treatment based on?
If a skill cant be measured or observed during a school day, then it?
Date to begin what? Frequency, location, and duration of?
Description of how progress will be?
Statement of the ______ ______ and ______ ______ and ______ ______ and _____, based on peer-reviewed research to the extent practicable, to be provided to the?
16 years of what must be developed? What else must be provided?
Consider whether the child needs what?
The IEP or plan is a written statement that includes:
Child’s present levels of academic and functional performance
The child’s priority educational needs (PEN) are determined by the team
Explanation of how the disability affects the child’s involvement and progress the general education curriculum
Goals developed to enhance the child’s performance in school
Accommodations for assessments
Statement of measurable annual goals: academic and functional
Goals are developed dependent on student’s priority educational needs (PEN) and PT support, if needed, is added to specific goals cobsidered
Not discipline specific
Not written in clinical language, but rather functional and educational language
PT develops a plan of treatment based on the goal being supported
If a skill can’t be measured or observed during a school day, then it might not be relevant to the child’s educational needs
Date to begin services and the frequency, location, and duration of services
Description of how a child’s progress will be measured
Statement of the special education and related services and supplemental aids and services, based on peer-reviewed research to the extent practicable, to be provided to the child
16 years of appropriate measurable postsecondary goals must be developed, and transitional services provided
Consider whether child needs assistive technological devices and services
IDEA 2004 PT EVALUATIONs
PT and OT evaluation to include what in most states?
Evaluation do need to provide what?
Under IDEA, a student must be in what to be considered for related services
Time frame for initial special education evaluations is how many student attendance days?
PT and OT evaluations to include standardized assessments in most states
Evaluations do need to provide a clear picture of the child’s ability to function within the school setting
Under IDEA a student must be in special educations to be considered for related services
Time frame for initial special education evaluations is 60 student attendance days
Team based goals
Developed by?
Example for long term objective? The goal must be what two things?
Example for short term objective? The goal must be what two things? Give an example of a short term goal that is measurable but NOT objective.
Developed by APTA section on Pediatrics IDEA Conference Faculty
Ex)
Annual goal (long term objective): Jonathan will walk up and down the school stairs independently without using the railing → this goal is MEASURABLE AND EDUCATIONALLY RELEVANT
Short term Objectives: Jonathan will climb up 8 stairs to enter the school with standby supervision using a railing → MEASURABLE AND EDUCATIONALLY RELEVANT
Short term Objectives: Jonathan will progress from 30 degrees to 50 degrees of active flexion of his right knee → MEASURABLE BUT NOT DIRECTLY EDUCATIONALLY RELEVANT
Difference between IEP and 504 plan?
Basic description
What it does
What law applies
Who’s eligible
What’s in it
IEP | 504 Plan | |
|---|---|---|
Basic Description | A blueprint or plan for a child’s special education experience at school. | A blueprint or plan for how the school will provide support and remove barriers for a student with a disability. |
What it does | Provides individualized special education and related services to meet a child’s unique needs. These services are provided at no cost to families. | Provides services and changes to the learning environment to enable students to learn alongside their peers. As with an IEP, a 504 plan is provided at no cost to families. |
What law applies | The Individuals with Disabilities Education Act (IDEA) | Section 504 of the Rehabilitation Act of 1973 |
Who’s Eligible | A child has one or more of the 13 disabilities listed in IDEA. The law lists specific challenges, like learning disabilities, ADHD, autism, and others. The disability must affect the child’s educational performance and/or ability to learn and benefit from the general education curriculum. The child must need specialized instruction to make progress in school. | A child has any disability. Section 504 covers a wide range of different struggles in school. The disability must interfere with the child’s ability to learn in a general education classroom. |
What’s in it | The child’s present levels of academic and functional performance—how the child is currently doing in school Annual educational goals for the child and how the school will track progress The services the child will get—this may include special education, related, supplementary, and extended school year services The timing of services—when they start, how often they occur, and how long they last Any accommodations—changes to the child’s learning environment Any modifications—changes to what the child is expected to learn or know How the child will participate in standardized tests How the child will be included in general education classes and school activities | Specific accommodations, supports, or services for the child Names of who will provide each service Name of the person responsible for ensuring the plan is implemented |
Timing of transition
Recommended timeline? (Begin, active planning, transfer)
Key responsibilities? (4)
Recommended timeline
Begin: ~12-14 years
Active Planning: adolescence
Transfer: 18-21 years
Key responsibilities
Promote self-management skills
Address mobility for adult environments
Facilitate participation (school, work, community)
Collaborate with TEAM (OT, SLP, MD, Social Worker)
