Biosystems II exam 5:
1/164
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
165 Terms
Steps of B cell activation/Antibody secretion:
Mature, Naive BCell in peripheral lymphoid organ recognizes Ag by BCR (IgM/D)
(TCell and other stimuli) - Clonal expansion of BCell
BCell proliferation and diffferentation
Turn into plasma cell and secrete IgM, IgG, memory BCells (Secretion, isotope switching, affinity maturation)
What is TCell dependent BCell activation? (TD)
Ag has a protein component (can cross-link Rs), activates in lymph node follicles and needs help Isotope switching, Affinity maturation, Plasma cells and inducing memory B cells
What is TCell independent BCell activation? (TI)
Ag with multiple identical/repeating epitopes (can cross-link Rs), activates in marginal zone of spleen and DOES NOT need help with functions (only need signal 1)
Example of a Thymus dependent agent (TD)
Protein Ag binds MHC class II molecule - Isotope switching, affinity maturation and memory BCell response occurs
Example of a Thymus independent agent (ID)
Polymeric antigens (polysaccharides, glycolipids and nucleic acids) CANNOT bind MHC but may bind multiple BCRs to activate but with little to no isotope switching, affinity maturation and memory cells
Plasma cells are…
Terminally differentiated, activated BCell; high rate of Ig production
2 types of plasma cells:
Short lived: TI Ag - white pulp of spleen/nonlymphoid tissue
Long-lived: TD Ag - migrate to bone marrow and constantly secreting Ig months to years following Ag exposure
What does cross-linking do to BCRs?
Initiates activation cascade when 2+ BCRs cross linked OR BCR + complementR/TLR
Signal 1 and 2 in TD activation:
Signal 1: Protein antigen bind BCR and associated with Iga/IgB heterodimer - Ag presented on MHC class II
Signal 2: Interaction between CD40 on BCell and CD40L on helper TCell
Signal 1 and 2 in TI activation:
Signal 1: Non-protein multivalent Ag binds BCR associated with Iga/IgB heterodimer
Signal 2: Complement R or TLRs = innate immunity = facilitates adaptive immunity (aka BCell activation)
BCells are professional…
APCs
Steps of BCell Ag presentation:
Ag binds BCR by PRR/TLR and MHC class I/II (usually class II)
Ag internalized, processed and presented to ACTIVATED T helper cells (Naive TCell previously activated by same Ag on DC)
In TD BCell activation, the BCell and TCell recognize…
the same Ags so the adaptive response is microbe-specific (recognize different antigenic epitopes from same microbe)
Helper TCell dependent response (TCell POV):
Ag presented by DC to naive TCell (peptide ; B7+CD28)
TCell now activated and secretes IL-2, CD40L and Th1/2 differentiation
Activated TCell migrates toward BCell follicle
Helper TCell dependent response (BCell POV):
BCR recognized protein Ag (captured and processed)
Migration of Ag-stimulated BCell towards T cell zone (for presentation)
Activation of BCell with help from activated TCell (Peptide ; CD40 (B) + CD40L)
Where does TD BCell activation occur?
The interface of the BCell follicle and TCell zone in secondary lymphoid organs
What are “germinal center reactions“?
Affinity maturation and Isotope class switching (done in a special part of lymph node/spleen)
What enzyme is involved in Affinity maturation/ Somatic Hypermutation?
Activation-induced deasminase (AID)
TD BCells REQUIRE what to induce AID expression (for affinity maturation and isotype switchingg)?
costimulation (signal 2; CD40 + CD40L)
What is the function of AID in affinity maturation/Somatic hypermutation?
Changes C to U and generates point mutations in variable regions (change affinity that increases with each exposure)
As exposure to Ag increases, Affinity of BCR to Ag..
Increases (increased ability to bind at lower concentration)
Isotope switching is…
Producing the same specificity for Ag as membrane-bound BCRs w/ switched BCR
Isotope switching occurs in response to which different cell/cytokines?
TH1 = IFN-y
TH2 = IL-4, IL-5 and IL-13
Where does isotype switching occur?
Peripheral lymphoid organs (activated BCells only, in follicles/germinal center)
DC activates TCell then TH1 TCell activates BCell with what cytokine/switch/function?
IFN-y causes switch to IgG which has FcR-d phagocytic response, complement activation and neonatal immunity effects
If TCell does NOT activate BCell, what signaling/functions occur?
IgM+ BCell sends no signal for switching and activates complement (innate)
DC activates TCell then TH2 TCell activates BCell with IL-4, what switch/function?
Causes switch to IgE which helps in helminth immunity and mast cell degranulation (hypersensitivity)
DC activates TCell then TH2 TCell activates BCell with IL-5, what switch/function?
Causes switch to IgA which plays a role in mucosal immunity
Bacteria with a polysaccharide rich capsule will cause what reaction?
TI - induce IgM = complement activation
A virus/bacteria enters what reaction is caused?
TD - IFN-y induced by TH1 = IgG
A helminth/parasite enters, what reaction occurs?
TD - IL-4 induced by TH2 = IgE
An infection in mucousal area occurs, what reaction follows?
TD - IL-5 induced by TH2 = IgA
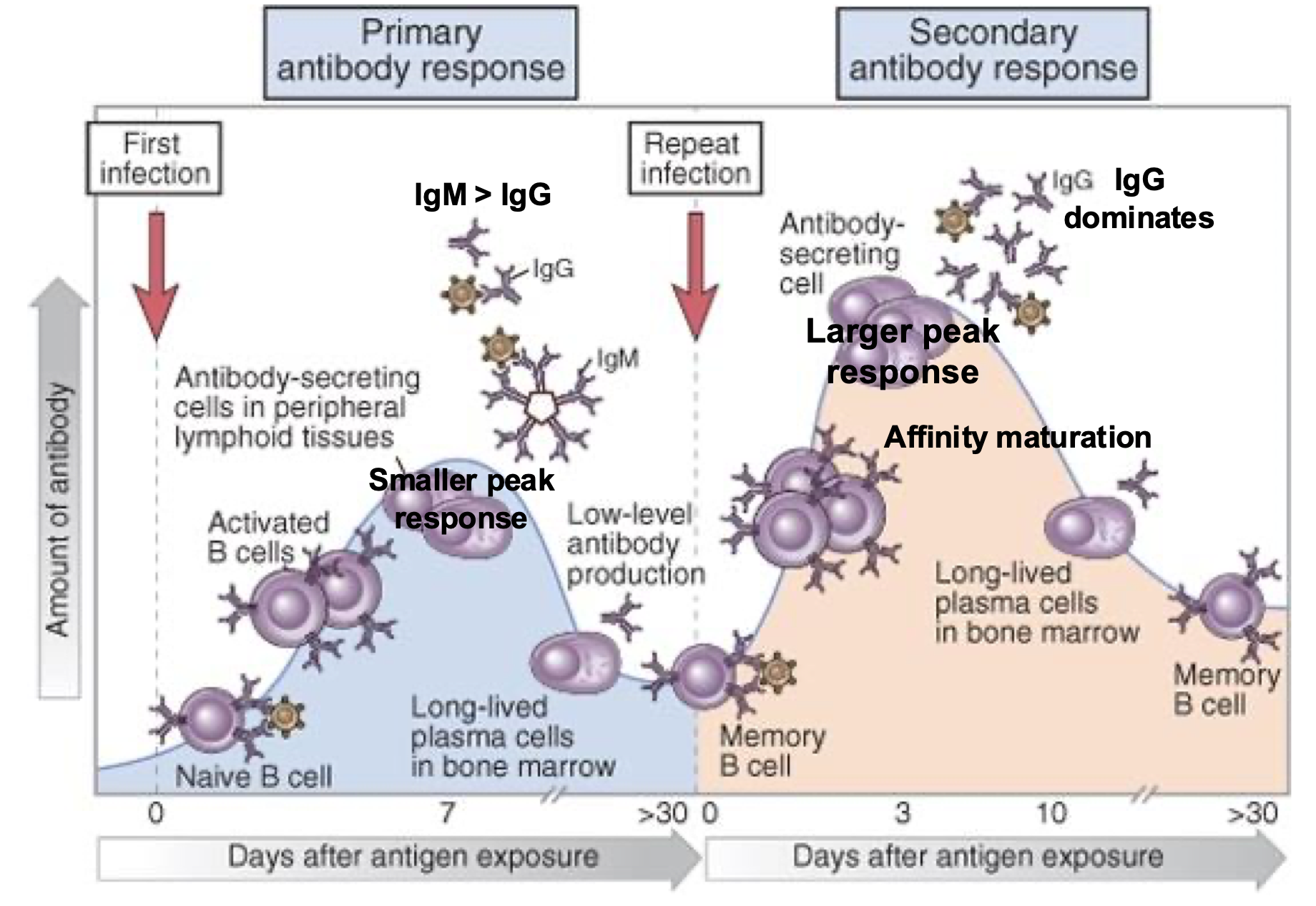
Primary Humoral response, Lag, Peak, Isotype and affinity:
7-10 days
Low peak
IgM (no TCell)
Low
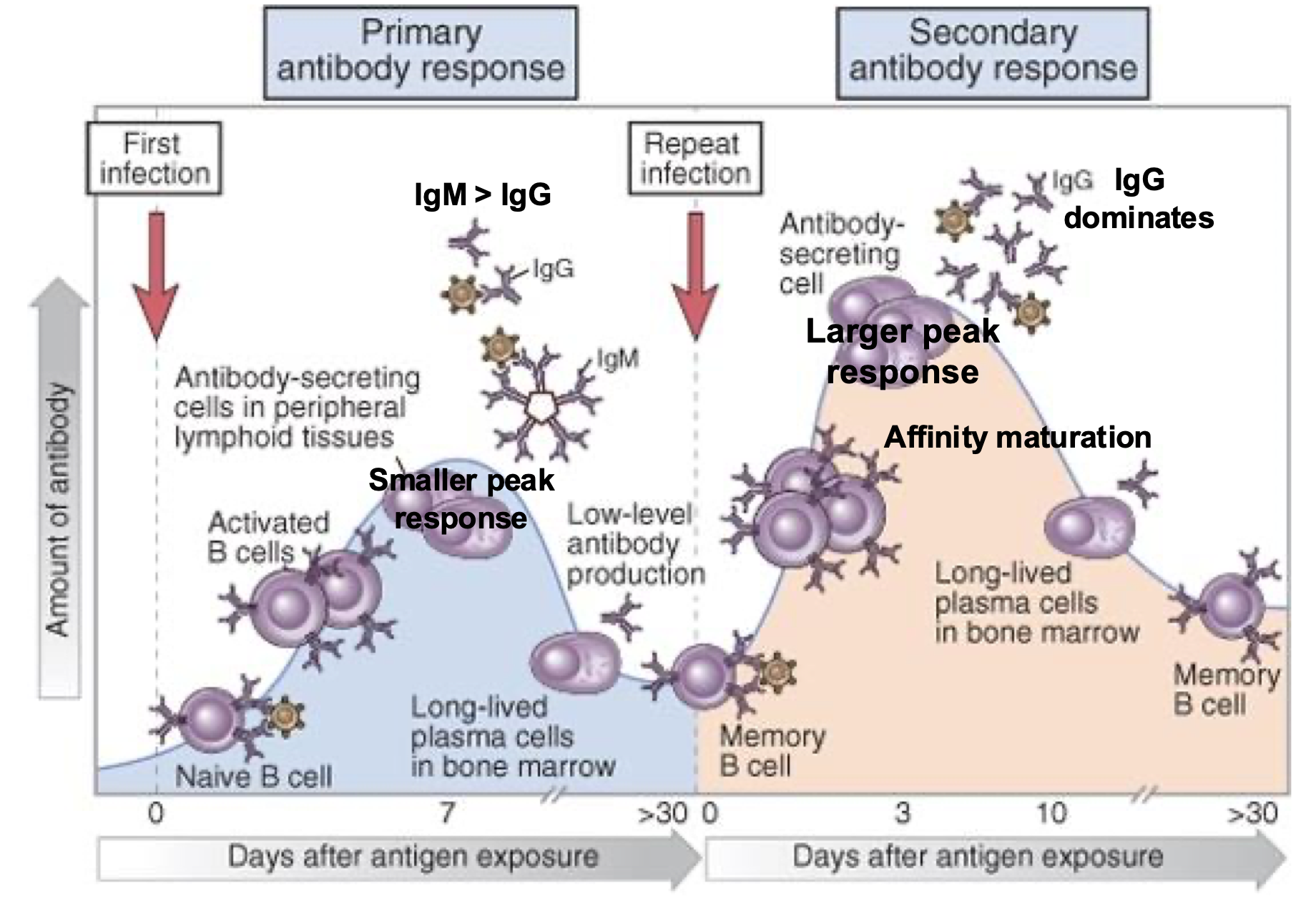
Secondary Humoral response, Lag, Peak, Isotype and affinity:
3-5 days
>100x higher
IgG (IgE/IgA)
High
The humoral immune response is mediated by…
secreted antibodies
The humoral immune response (Ig secretion) gives immunity against..
extracellular microbes and toxins
Humoral immunity includes components of both…
Active and Passive immunity
Humoral protectiveness can come from…
vaccines
Harmful humoral immunity is caused by..
Auto-antibodies
What is the primary Ig in the blood?
IgG
What is the primary Ig in mucosal organs?
IgA
What is antibody neutralization?
Ig bonds virus/toxin before it can bind to cells = prevents infection/attachment
Examples of antibody neutralization:
HIV-go120 binds CD4
Influenza-HA binds sialic acids
Tetanus binds neurotoxin
Cholera activates AC
2 things that function as opsonins? (promote phagocytosis via Fc-R)
Antibodies
Complement proteins
Fc-R specificity…
Fcy-R = IgG
Fca-R = IgA
FcE-R = IgE
How does opsinization/Fc-R work?
Fc-R associates with signaling molecules (ITAMs and ITIMs)
ITAMs recruit…
kinases
ITIMs recruit…
Phosphotases
Steps of Fc-R mediated phagocytosis:
Opsonization of microbe by IgG
Opsonized microbe binds by IgG and Fcy-R
Fc-R signals to activate phagocytosis
Phagocytosis and killing of microbe by ROS and NO (IFN-y from TH cell = kill signal)
What is Antibody-Dependent Cellular Cytotoxicity (ADCC)
Antibody-coated cell destruction by release of granules by IgG binding and NK cell recognition = granzyme and perforin
What is the role of complement in host defense:
Circulating cell membrane proteins are activated during innate immunity in absence of Ig (alternative pathway) AND/OR in presence of Ig during adaptive immunity (classical pathway) to opsonize, form MAC and inflammation/recruitment
Complement proteins are involved in antibody-mediated tissue injury AKA
Hypersensitivity reactions
Functions of complement: (3)
Opsonize microbes to promote phagocytosis
Form polymeric protein complex (MAC)
Promote inflammation at the site of complement activation
Functions of IgA:
Mucosal immunity (GI and upper respiratory)
Transport across epithelium (to get to lumen/breastmilk)
Acts as poly-Ig R
Neutralization in the lumen
Functions of IgG:
Neonatal immunity (transport across placenta by FcRn)
Neutralization (most secreted)
Opsonization
ADCC
Complement (classical)
IgE functions:
Eosinophil, mast cell activation and helminth defense
IgM functions:
Complement activation (classical)
BCR
IgD functions:
BCR only
ABO phenotypes:
Type A (Ag-A and Ig-B)
Type B (Ag-B and Ig-A)
Type AB (Ag-A and B so NO Ig) (universal recipient)
Type O (Ig- A and B so NO Ag) (universal donar)
Type A has self Ag and Ig-B so who CAN and CANNOT donate?
CAN receive: A and O
CANNOT receive: AB or B
Type B has self Ag and Ig-A so who CAN and CANNOT donate?
CAN receive: B and O
CANNOT receive: A or AB
Type AB has self Ag and NO Ig so who CAN and CANNOT donate?
CAN receive: A, B, AB and O (universal recipient)
Type O has NO Ag BUT Ig-A and B so who CAN and CANNOT donate?
CAN receive: O only
CANNOT receive: A, B, AB (universal donor)
Rh in pregnancy:
Rh+ father
Rh- mother carrying first Rh+ fetus
Rh+ fetus makes self Ag - cross to mother
Mother produces anti-Rh+ Ig (non-self)
Mothers 2nd pregnancy with Rh+ fetus = fetal damage by anti-Rh+ Ig
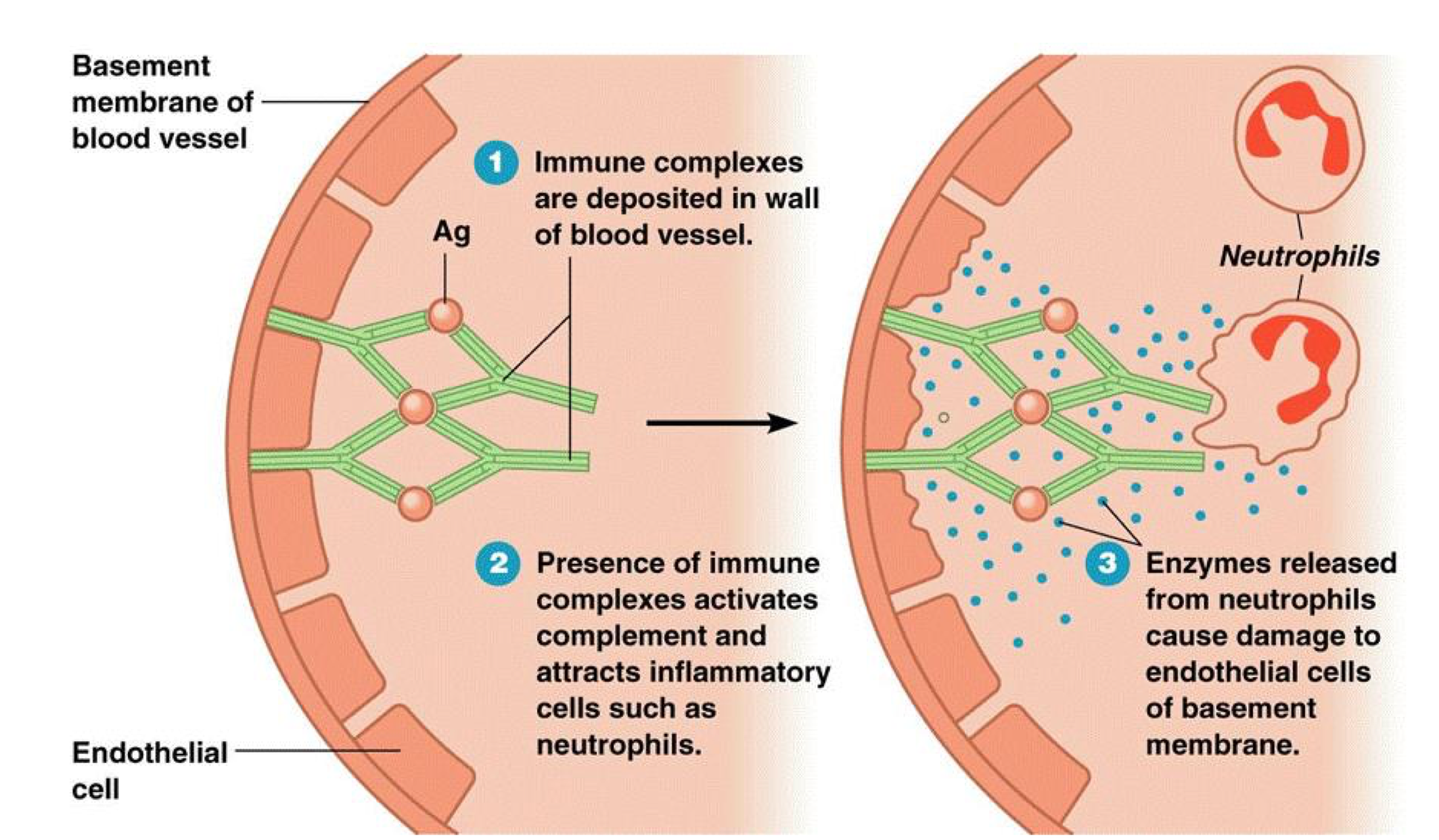
SLE/Lupus
Immune complexes are deposited in wall of blood vessel
Presence of immune complexes activates complement and attracts inflammatory cells such as neutrophils
Enzymes released from neutrophils cause damage to endothelial cells of basement membrane
What is a hypersensitivity reaction defined as…
An excessive, exaggerated and/or abnormal immune response that causes tissue injury
Symptoms of a hypersensitivity reaction can manifest as…
Immediate
Delayed
Chronic
Autoimmune
2 ways that hypersensitivity occurs:
Response to foreign Ag may be dysregulated or uncontrolled leading to tissue injury
Immune responses may be directed against self Ag (due to failure of self-tolerance)
What is autoimmunity?
Responses against self Ag leading to autoimmune diseases
4 types of hypersensitivity reactions:
Type I: immediate by TH2
Type II: Ig-mediated from auto-reactive Ig
Type III: Immune complex mediated by Ag-Ig complexes
Type IV: TCell mediated by TH1 Cells
Type I hypersensitivity is….
Immediate
TH2 mediated (IgE)
Mast cells cause histamine, LT and Cytokine release
Eosinophil and Neutrophil inflammation
What is Atopy:
Tendency to produce an exaggerated IgE response to harmless substances (can have increased genetic risk aka “atopic individual“)
Mast cells express elevated levels of FcE-R (IgE R) which causes…
hyperreactive airway manifestation
Steps of allergen exposure (general)
Allergen exposure (Pollen)
Allergens registers as a foreign “threat“
Immune system produces IgE and mast cells
Allergy symptoms: runny nose, itchy eyes and sneezing
Examples of allergens/triggers:
Food, pollen, venom, dander, drugs, pollutants, exercise, temperature
Immediate hypersensitivity chain of events: (11)
Primary allergen exposure
Allergen presentation to allergen-specific naive CD4 TCell
Differentiation TH2 (IL-2 and IL-4)
Activation of allergen-specific BCell (IL-5 and IL-13)
IgE class switch
Sensitization of mast cells
Secondary allergen exposure (binds IgE made by previous exposure)
Mast cell activation/Fc-crosslinking (by FcE-R)
Release mediators (degranulation of mast cells = vasoactive amines/Histamines and lipid mediators/PG+LT)
Late phase cytokine release (2-8 hours after repeat exposure to allergens)
Response occurs in minutes AKA immediate
______ exposure is required for activation of ‘sensitized‘ mast cells
repeat
Mast Cell Mediators:
Histamines: vascular permeability, smooth muscle contraction, vascular dilation (edema)
LT: vascular permeability, smooth muscle contraction and mucus secretion
PG: vascular dilation (blood flow)
Protases (tryptase): local tissue damage
Histamine and lipid mediators are _____ while cytokines are NOT
premade
Cytokines involved in mast cell functions (late phase):
IL-4: TH2
IL-5: eosinophil activation
IL-13: mucus secretion
TNFa: increased leukocyte recruitment
Histamines cause
Vascular permeability, smooth muscle contraction, vascular dilation (edema)
Leukotrienes cause:
Vascular permeability, smooth muscle contraction and mucus secretion (Bronchoconstriction and GI hypermobility)
Inflammation mediators of hypersensitivity:
TNFa
IL-4/5/13
LT
PG
Which mediators cause tissue damage?
Tryptase and mast-cell proteases
Inhaled (type I) hypersensitivity syndromes:
Allergic rhinitis and Sinusitis (hay fever): Increased mucus and inflammation of upper airways/sinuses
Bronchial asthma: bronchial hyper-responsiveness caused by SM contraction, inflammation and tissue injury from late phase cytokines
Ingested (type I) hypersensitivity syndrome:
Food allergies (increased peristalsis due to contraction of intestinal muscles)
Systemic (type I) hypersensitivity syndrome:
Anaphylaxis (drugs/bee/food, Fall in BP (shock) caused by vascular dilation and airway obstruction due to laryngeal edema
Treatment for Type I hypersensitivity: Various allergic diseases
“Desensitization” (repeated admin of low doses of allergens) - Unknown, may inhibit IgE production and induce TCell tolerance
Anti-IgE antibody - Neutralize and eliminate IgE
Antihistamines - Blocks actions of histamine on vessels and SM
Cromolyn - inhibits mast cell degranulation
Treatment for Type I hypersensitivity: Anaphylaxis
Epinephrine (SM contraction, increase CO, inhibit mast cell degranulation)
Treatment for Type I hypersensitivity: Bronchial asthma
Corticosteroids and PI’s (Reduce inflammation and relax bronchial SM)
Singulair is a ______ that inhibits _____
LTa ; Bronchoconstriction
-mabs for type I hypersensitivity MOA:
Binds Fc portion of IgE to prevent binding to FcE-R
Corticosteroids and cromolyn MOA:
Prevent cytokine production and mast cell degranulation = no inflammatory cytokines or PG/LT
What are type II hypersensitivity reactions?
Antibodies are reactive to self tissue where normal Ig-mediated effector functions lead to cellular injury or dysfunction (complement activation, Fc-R activation, inflammation)
Type II Antibody-mediated diseases:
Autoimmune hemolytic anemia
Goodpasture syndrome
Myasthenia gravis
Graves disease
Autoimmune hemolytic anemia (Type II):
Target: Erythrocyte membrane proteins (Rh blood group Ag)
Mechanism: Opsonization and phagocytosis of erythrocytes
Manifests: Hemolysis and anemia
Goodpasture syndrome (Type II):
Target: Noncollagenous protein in basement membranes of kidney glomeruli and lung alveoli
Mechanism: Complement and Fc-R mediated inflammation
Manifests: Nephritis and Lung hemorrhages
Myasthenia gravis (type II):
Target: ACh R
Mechanism: Ig inhibits ACh binding; down-modulates R’s
Manifests: Muscle weakness/paralysis
Graves disease (type II):
Target: TSH R
Mechanism: Ig-mediated stimulation of TSH R’s
Manifests: Hyperthyroidism
What is Type III hypersensitivity?
Occurs when circulating immune complexes deposit in blood vessels and cause complement- and Fc receptor–mediated recruitment and activation of leukocytes, especially neutrophils, leading to inflammation and vasculitis