T5 - IE3 - Pulmonology - Munjy - COPD
1/94
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
95 Terms
COPD
chronic obstructive pulmonary disease
COPD is a ________, _________, and _______ disease with persistent respiratory symptoms, airflow limitation due to airway and/or alveolar abnormalities due to exposure to noxious stimuli
- common
- preventable
- treatable (disease)
COPD is a common, preventable, treatable disease with ____________ respiratory symptoms, airflow limitation due to airway and/or _________ _________ due to exposure to ___________ stimuli
- persistent (respiratory symptoms)
- airflow limitation
- (exposure to) noxious (stimuli)
COPD symptoms
dyspnea
cough
sputum production
COPD risk factors
smoking
biomass fuel exposure
air pollution
genetic abnormalities
abnormal lung development
accelerated aging
COPD vs. Asthma Onset
COPD: onset AFTER age 40
Asthma: onset BEFORE age 20
COPD vs. Asthma Onset - Asthma: onset _________ ____ _____
- BEFORE age 20
COPD vs. Asthma Onset - COPD: onset __________ _____ _____
- AFTER age 40
COPD vs. Asthma - symptoms
COPD: persistence of symptoms with treatment
Asthma: vary over time
COPD vs. Asthma - lung function
COPD: abnormal lung function between symptoms
Asthma: lung function may be normal between symptoms
COPD vs. Asthma response to bronchodilators
COPD: limited relief from bronchodilators (FEV1 does NOT return to normal after bronchodilator use)
Asthma: FEV1 can return to normal post-bronchodilator use
COPD vs. Asthma response to bronchodilators: COPD has ________ relief from bronchodilators (FEV1 does _______ __________ to normal after bronchodilator use)
- limited (relief)
- NOT return (to normal after bronchodilator use)
COPD vs. Asthma response to bronchodilators: asthma __________ to bronchodilators (FEV1 can return to _________ post-bronchodilator use)
- responds (to bronchodilators)
- (return to) normal
COPD vs. Asthma Chest X-Ray
COPD: severe hyperinflation or other changes on X-ray
Asthma: normal chest x-ray
Prevention of COPD
smoking cessation
influenza vaccination
pneumococcal vaccinations: PCV13, PPSV23
reduce exposure to risk factors
Prevention of COPD - smoking cessation: ____________ capacity to influence _________ history of COPD
- greatest (capacity)
- natural (history of COPD)
Prevention of COPD vaccines
influenza
pneumococcal vaccines
- PCV13
- PPSV23
Prevention of COPD vaccines - pneumococcal: PCV13, PPSV23
All patients ≥ 65 years old
Patients 19-64 years old with smoking history
Prevention of COPD: reduce exposure to risk factors
noxious stimuli
environmental toxins
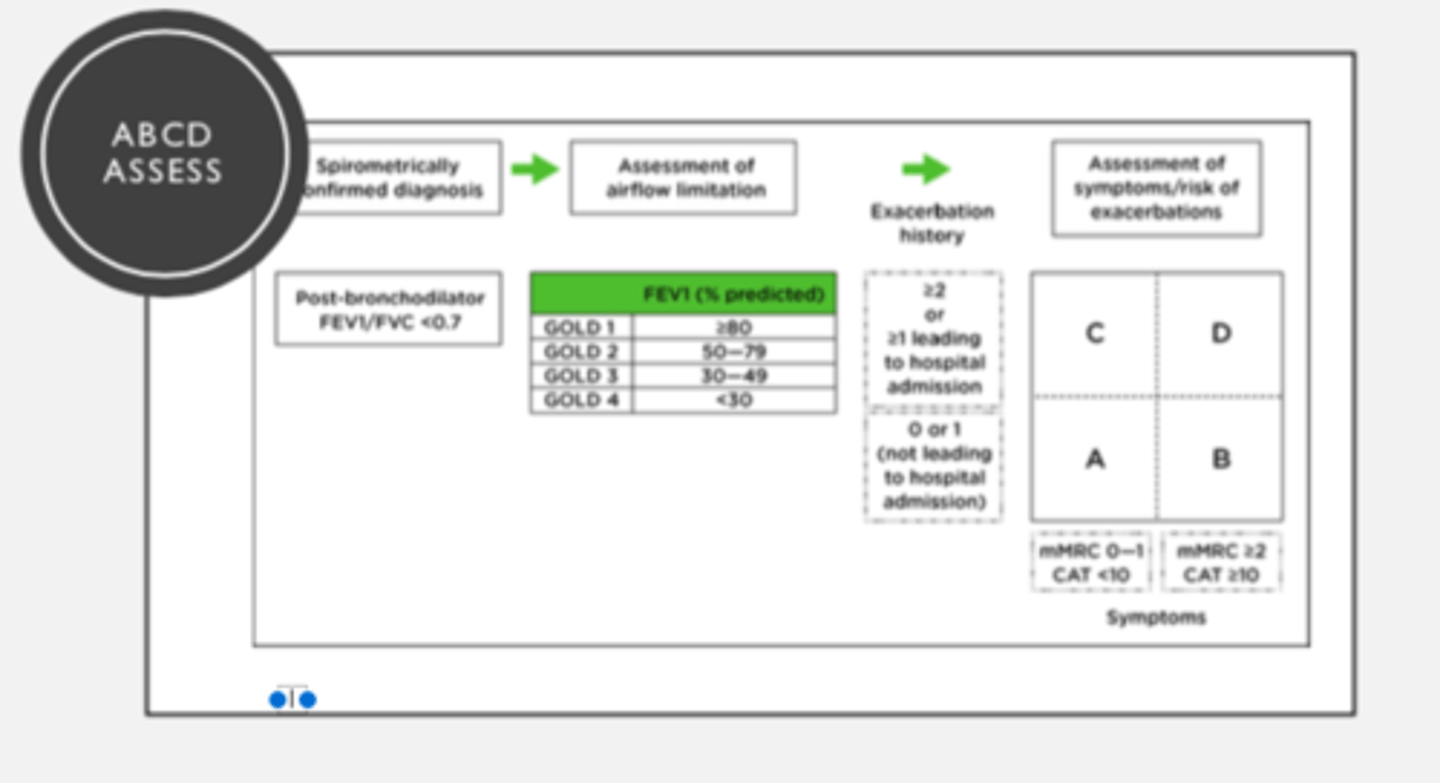
Similar to asthma, COPD is assessed by looking at the patient's ____________ and history of ___________
- (patient's) symptoms
- (history of) exacerbations
COPD assessment: ________ __________ also assist in objective data for assessment
- GOLD categories (also assist in objective data)
AIRFLOW limitation: ___________ is used to assess airflow limitation
- Spirometry (is used to assess)
Spirometry is conducted after the administration of an adequate dose of at least one short-acting bronchodilator
COPD vs. Asthma Monotherapy Don'ts
COPD: DO NOT USE ICS monotherapy
Asthma: DO NOT USE LABA monotherapy
AIRFLOW limitation: Spirometry is conducted _______ the administration of an adequate dose of at least one ______-______ ______
- after (the administration)
- (at least one) short-acting bronchodilator
GOLD categories: in patients with FEV1/FVC <0.70 - GOLD I
MILD
FEV1 ≥ 80% predicted
GOLD categories: in patients with FEV1/FVC <0.70 - GOLD II
MODERATE
50 - 79% predicted FEV1
GOLD categories: in patients with FEV1/FVC <0.70 - GOLD III
SEVERE
30 - 49% predicted FEV1
GOLD categories: in patients with FEV1/FVC <0.70 - GOLD IV
VERY SEVERE
FEV1 < 30% predicted
COPD Symptoms Assessment
COPD Assessment Test (CAT)
Modified Medical Research Council dyspnea questionnaire (MMRC)
CAT
COPD Assessment Test
MMRC
Modified Medical Research Council (MMRC) dyspnea scale
Exacerbation risk for COPD
acute worsening of respiratory symptoms that result in additional therapy
Mild exacerbation risk for COPD - treatment
short-acting bronchodilators (SABAs)
Moderate exacerbation risk for COPD treatment
treat with short-acting bronchodilators (SABAs)
Antibiotics (if infection)
and/or
oral corticosteroids
Severe exacerbation risk for COPD treatment
Hospitalization occurs AFTER visit to ED
Comorbidities associated with COPD
Cardiovascular disease
Skeletal muscle dysfunction
Metabolic syndrome
Osteoporosis
Depression
Anxiety
Lung Cancer
ABCD Assessment Tool Figure
ABCD Practice Case #1:
KL 65-year old female with COPD. She has had one exacerbation in the last year that she went to the ED for but did not result in hospital admission. Her CAT score is 9 and her mMRC score is 1.
How would you grade her COPD based the ABCD assessment tool?
a. A
b. B
c. C
d. D
A
Since KL's CAT score is 9 and her mMRC score is 1; she went to the ED but did NOT have hospital admission
ABCD Practice Case #2
DD is a 71-year old male with COPD. He has had 1 exacerbation in the last year that led to a hospital admission. His CAT score is 18 and his mMRC score is 2.
How would you grade his COPD based the ABCD assessment tool?
a. A
b. B
c. C
d. D
D
DD has a CAT score of 18 and mMRC of 2. He has had only 1 exacerbation but it LEAD to hospital admission
Drug therapy used in COPD - bronchodilators
LABAs and LAMAs are preferred over short-acting agents EXCEPT in patients with OCCASIONAL dyspnea
Inhaled bronchodilators are preferred over oral bronchodilators
Theophylline is NOT recommended unless other long-term treatment bronchodilators are UNAVAILABLE
Drug therapy used in COPD - bronchodilators: LABAs and LAMAs are preferred over short-acting agents EXCEPT in...
patients with OCCASIONAL dyspnea
Drug therapy used in COPD - bronchodilators: ________ and _________ are preferred over _____-acting agents EXCEPT in patients with OCCASIONAL dyspnea
- LABAs
- LAMAs
- (preferred over) short(-acting)
Drug therapy used in COPD - bronchodilators: _________ bronchodilators are preferred over ______ bronchodilators
- inhaled (bronchodilators)
- (preferred over) oral
Drug therapy used in COPD - bronchodilators: theophylline is _______ _________ unless other long-term treatment bronchodilators are unavailable
- NOT recommended (unless other-long term treatment)
Drug therapy used in COPD - anti-inflammatory agents
long-term monotherapy with ICS is not recommended
Consider ICS in conjunction with LABA for patients with history of exacerbations despite appropriate treatment with long acting bronchodilators
In patients with exacerbations despite LABA/ICS or LABA/LAMA/ICS, chronic bronchitis and severe to very severe airflow obstruction, a PDE4 inhibitor (roflumilast) can be considered
Consider macrolides in patients with smoking history who have exacerbations despite appropriate therapy
Drug therapy used in COPD - anti-inflammatory agents: long-term monotherapy with _______ is not recommended
- ICS (is not recommended)
Drug therapy used in COPD - anti-inflammatory agents: _____-_____ ___________ with ICS is not recommended
- long-term monotherapy (with ICS)
Drug therapy used in COPD - anti-inflammatory agents: long-term monotherapy with ICS is ______ ____________
- NOT recommended
Drug therapy used in COPD - anti-inflammatory agents: Consider ICS in _____________ with LABA for patients with history of __________ despite appropriate treatment with long acting bronchodilators
- conjunction (with LABA)
- (history of) exacerbations
Drug therapy used in COPD - anti-inflammatory agents: Consider ICS in conjunction with _______ for patients with history of exacerbations despite appropriate treatment with _______ ___________ ____________
- (conjunction with) LABA
- long acting bronchodilators
Drug therapy used in COPD - anti-inflammatory agents: In patients with exacerbations despite LABA/ICS or LABA/LAMA/ICS, chronic bronchitis and severe to very severe airflow obstruction, a _____ ___________ (___________) can be considered
- PDE4 inhibitor (roflumilast)
Drug therapy used in COPD - anti-inflammatory agents: In patients with exacerbations despite _______/_____ or ______/________/_______, chronic bronchitis and severe to very severe airflow obstruction, a PDE4 inhibitor (roflumilast) can be considered
- LABA/ICS
- LABA/LAMA/ICS
i.e., patients need to be on LABA / ICS or LABA / LAMA / ICS prior to PDE4 inhibitor usage
Drug therapy used in COPD - anti-inflammatory agents: Consider ___________ in patients with smoking history who have exacerbations despite appropriate therapy
- macrolides (in patients with smoking history)
i.e., azithromycin, clarithromycin etc.
Drug therapy used in COPD - anti-inflammatory agents: Consider macrolides in patients with __________ history who have ____________ despite appropriate therapy
- smoking (history)
- (who have) exacerbations (despite appropriate therapy)
ICS use in COPD: _______ __________ as monotherapy or _____ _______ for patients with grade A or B disease
- not indicated (as monotherapy)
- [not indicated for] first line
ICS use in COPD: blood eosinophil count of ___ ______ cells / uL seen in trials to be indicator for use of ICS therapy earlier on to prevent exacerbations
- > 300 (cells / uL)
ICS use in COPD: _______ _________ count of > 300 cells / uL seen in trials to be indicator for use of _____ therapy earlier on to prevent exacerbation
- blood eosinophil (count)
- ICS (therapy earlier on to prevent exacerbation)
Suggests inflammatory pathway is prominent in pathophysiology of disease
ICS use in COPD: >300 cell/uL blood eosinophils suggests _________ pathway is prominent in ____________ of disease
- inflammatory (pathway)
- pathophysiology (of disease)
ABCD Assessment tool and initial therapy: Group A
bronchodilator usage
(GROUP A)
ABCD Assessment tool and initial therapy: Group B
Long acting bronchodilator (LABA or LAMA)
(GROUP B)
ABCD Assessment tool and initial therapy: Group C
LAMA
ABCD Assessment tool and initial therapy: Group D
LAMA
LAMA + LABA (if highly symptomatic)
ICS + LABA when blood eosinophil ≥ 300
ABCD Assessment tool and initial therapy: Group D when blood eosinophil ≥ 300
use ICS + LABA
ABCD Assessment tool and initial therapy: Group D if highly symptomatic
LAMA + LABA
Goals for management of COPD
reduce symptoms
- relieve symptoms
- improve exercise tolerance
- improve health status
reduce risk
- prevent disease progression
- prevent and treat exacerbations
- reduce mortality
Patient Case:
KL is a 68-year old female who is currently on a LABA + LAMA combination therapy for COPD. She has been complaining of worsening dyspnea and
increased limitation of her daily activities. It is noted that in the last year she has had 2 exacerbations in which she received treatment in the ED before being discharged. She is a former smoker with a 15-pack year history. Her blood eosinophil count is 150 cells/uL.
Patient KL seems to be experiencing exacerbations in her condition and has had dyspnea.
Since she has both follow the exacerbations guideline.
Note she also has eosinophil count of 150 cells / uL and is on LABA + LAMA (GROUP D) and blood eosinophil count is 150 cells / uL follow LABA + LAMA + ICS
If patient is experiencing only dyspnea follow dyspnea flow chart or exacerbations follow exacerbations flow chart
However, if patients experience BOTH dyspnea and exacerbations follow the ___________ flow chart
- exacerbations (flow chart)
COPD Gold Guidelines 2019 Flow Chart
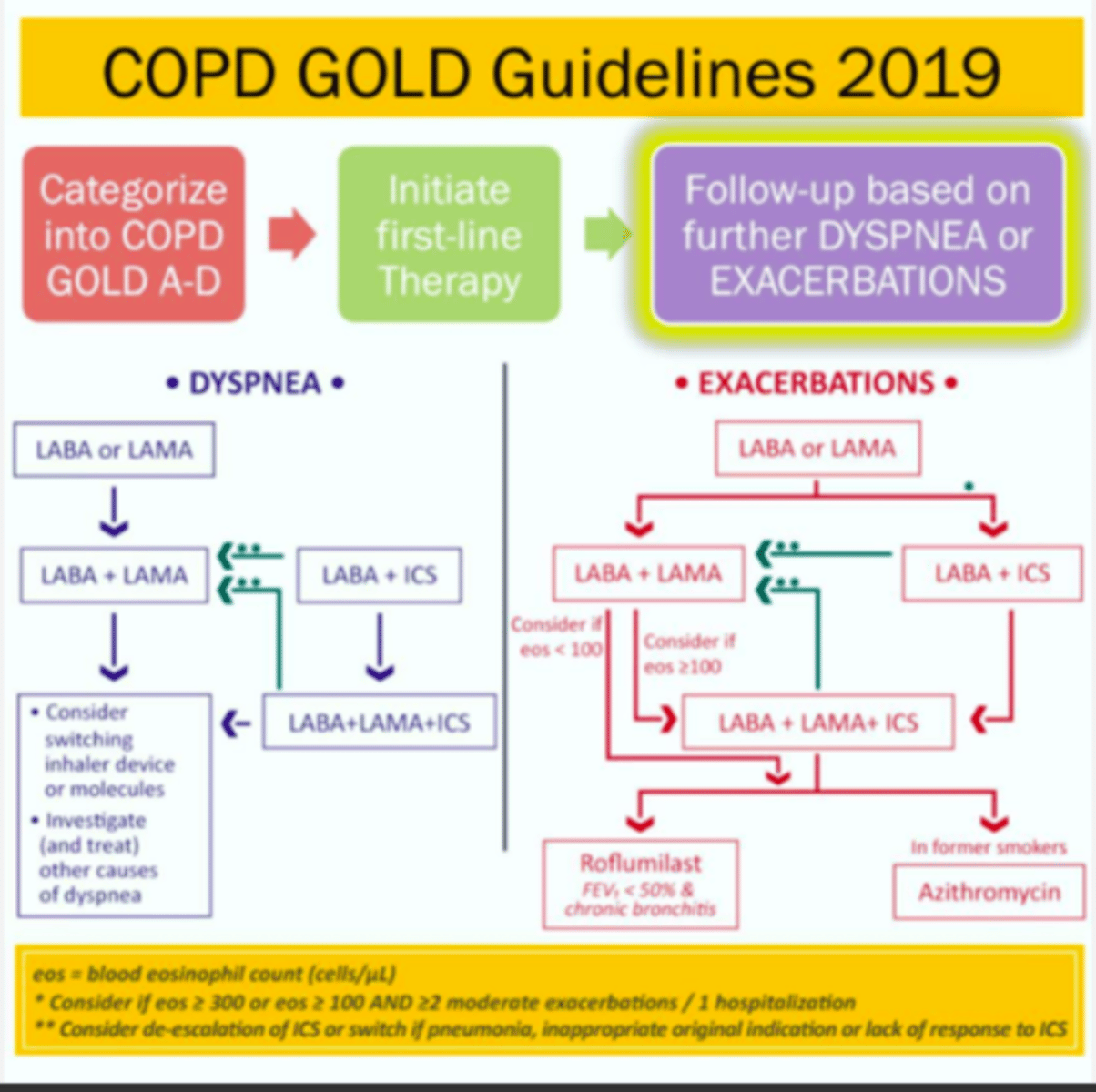
If a patient is already on LABA + LAMA + ICS and experience exacerbations they may try...
Roflumilast (FEV1 < 50% & chronic bronchitis)
Azithromycin (in former smokers)
Education and self-management of COPD
Educate patient regarding how to reduce risk of exacerbations , create an action plan, use other health-care professionals (social workers)
Rehabilitation is recommended in
ALL patients with relevant symptoms and/or high risk for exacerbations
Physical activity is a strong predictor of mortality and therefore patients should be encouraged to increase level based on individual ability
Education and self-management of COPD: educate patient regarding how to reduce risk of ____________ , create an ______ _____, use other _____-_____ professionals (social workers)
- (reduce risk of) exacerbations
- action plan
- health-care (professionals)
Education and self-management of COPD: ______________ is recommended in ALL patients with _________ symptoms and/or _____ risk for exacerbations
- Rehabilitation (s recommended in ALL patients)
- relevant (symptoms)
- high (risk)
Education and self-management of COPD: __________ activity is a strong predictor of mortality and therefore patients should be encouraged to increase level based on individual ability
- Physical (activity)
End-of-life & Palliative care: all clinicians managing COPD patients should determine if palliative care is ___________ for their patient
- appropriate (for their patient)
End-of-life & Palliative care: end-of-life disccusions should be considered with patients and family members
advance directives
place of death preference
Treatment of hypoxemia & hypercapnia: patients with __________ are indicated for long-term oxygen therapy considerations
- hypoxemia (are indicated for long-term oxygen)
Treatment of hypoxemia & hypercapnia: patients with hypoxemia are indicated for ______-_________ ________ therapy considerations
- long-term oxygen (therapy considerations)
Treatment of hypoxemia & hypercapnia: Patients with _______ COPD and _________ or ______-_______ moderate desaturation are NOT routinely indicated for long-term oxygen therapy
- stable (COPD)
- resting
- exercise-induced (moderate desaturation)
Treatment of hypoxemia & hypercapnia: patients with __________ _______ ______ and history of ________ for acute respiratory failure should be considered for long-term non-invasive ventilation
- severe chronic hypercapnia
- (history of) hospitalization (for acute respiratory failure)
Treatment of hypoxemia & hypercapnia: Patients with severe chronic hypercapnia and history of hospitalization for _____ _________ failure should be considered for long-term ____-______ ____________
- acute respiratory (failure)
- (long-term) non-invasive ventilation
Intervention bronchoscopy and surgery: _____ _______ ________ surgery is considered in patients with upper-lobe emphysema
- lung volume reduction (surgery)
Intervention bronchoscopy and surgery: lung volume reduction surgery is considered in patients with ______-_______ ________
- (patines with) upper-lobe emphysema
Intervention bronchoscopy and surgery: bronchoscopic lung volume reduction should be consider in selected patients with __________ ___________
- advanced emphysema
Intervention bronchoscopy and surgery: patients with very severe COPD may be considered for ________ ______________ if 1 of the following exists
- history of hospitalization exacerbation with acute hypercapnia ensures
- pulmonary hypertension despite oxygen therapy
- FEV1 < 20% and either DICO <20% of homogenous distribution of emphysema
- lung transplantation
Lung transplant patients for COPD
history of hospitalization exacerbation with acute hypercapnia ensues
pulmonary hypertension despite oxygen therapy
FEV1 < 20% and either DICO <20% of homogenous distribution of emphysema
Lung transplant patients for COPD: history of hospitalization exacerbation with ______ ____________ ensues
- acute hypercapnia (ensues)
Lung transplant patients for COPD: ___________ ___________ despite oxygen therapy
- pulmonary hypertension (despite oxygen therapy)
Lung transplant patients for COPD: FEV1 __ _____% and either DICO __ ____% of homogenous distribution of emphysema
- (FEV1) < 20(%)
- (DICO) < 20(% of homogenous distribution)
ACOS
asthma-COPD overlap syndrome
ACOS: syndrome of __________ diseases of the ________
- multiple (diseases)
- airways
ACOS: not clearly defined - ___________ airflow limitation with several features usually associated with ______ and several features associated with _______
- persistent (airflow limitation)
- asthma
- COPD
Never use _______ monotherapy in asthma OR ______ monotherapy in COPD
- (never use) LABA (monotherapy in asthma)
- [never use] ICS (monotherapy in COPD)
Treatment of ACOS: combination of ______ and ______ is acceptable EVEN if less than grade C or D on ABCD assessment tool
- ICS
- (and) LABA (is acceptable)
Treatment of ACOS: combination of ICS and LABA is acceptable EVEN if ______ than grade __ or __ on ABCD assessment tool
- less (than grade)
- C
- D
Treatment of ACOS: remember warning regarding increased risk of death for ________ monotherapy in asthma patients
- LABA (monotherapy in asthma patients)