Abdominal Diseases
1/57
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
58 Terms
“Abdominal Catastrophe”
Clinical signs
4 Mechanisms/causes (+ DDx)
Clinical Signs: Colic with distended abdomen and usually SHOCK
Mechanisms/Causes:
Torsions
RDA with torsion
Caecal dilation and torsion
Mesenteric torsion
Ileus
Blockages
Intussusception
Haemorrhagic bowel disease
Phytobezoar
Constricting bands (tears in ligaments at parturition/congenital which trap intestine)
Tears in omentum → Herniation
Toxic
Rumen acidosis
Septic mastitis → 2˚ ileus
Other
Bloat
Diffuse peritonitis
Perforating abomasal ulcer
Abdominal diseases NOT characterised by shock
Forestomach (5)
Abomasum (3)
Other (3)
Forestomach
Rumen acidosis
Traumatic reticuloperitonitis
Vagal atony
Actinobacillus of rumen/reticulum
Simple indigestion
Abomasum (esp. system grade 4 with high grain)
LDA or RDA without torsion
Impaction
Ulceration
Other
Caecal dilation
Chronic peritonitis
Non-gastrointestinal (eg. urinary tract)
5 Steps of abdominal disease diagnosis
History
Often associated with sudden drop in milk production due to visceral pain → Activation of sympathetic nervous system → Inhibit milk letdown
Distance examination
Physical examination
Rectal palpation
Additional tests
Good history and PE → Diagnosis made in up to 90% of cases (+ve: Save money for farmer)
9 Features to assess on distance examination for abdominal disease
Mentation (alert vs. depressed)
Interaction with environment
Behaviour (eating, chewing cud, urinating, defaecating)
Caution: Some sick animal still eat in new environments (eating = Stress response)
Chewing cud = GOOD sign
Posture (down, hunched)
Signs of colic (abdominal discomfort) = More subtle in cattle
Obvious colic with rolling and repeated recumbency is UNUSUAL
DDx:
Adult = Mesenteric torsion
Calf = Abomasal bloat
Gait (may appear slightly lame or subtly looking at flank)
BCS
Body symmetry and abdominal distension
Observe other cows in herd
Faeces present? Consistency, contents, contamination of hindlimbs
Large volumes of faeces = No obstruction → Immediate surgical intervention unlikely required
Some conditions resolve on transport
Mucus ONLY = Obstruction and no passage of digesta → Surgical management
Diarrhoea = LDA/RDA
Blood = Abomasal ulcer, haemorrhagic bowel disease (blackberry jam)
Large undigested fibre particles (>2cm length) = Hardware disease
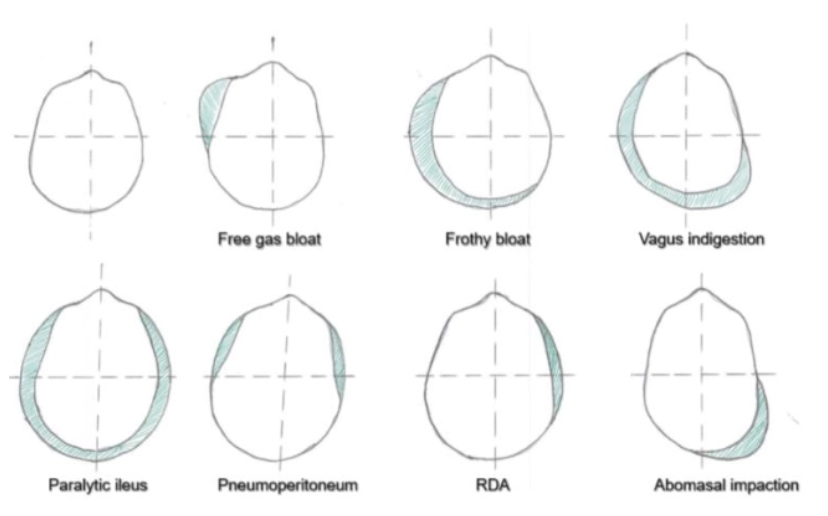
DDx: Body symmetry/abdominal distension
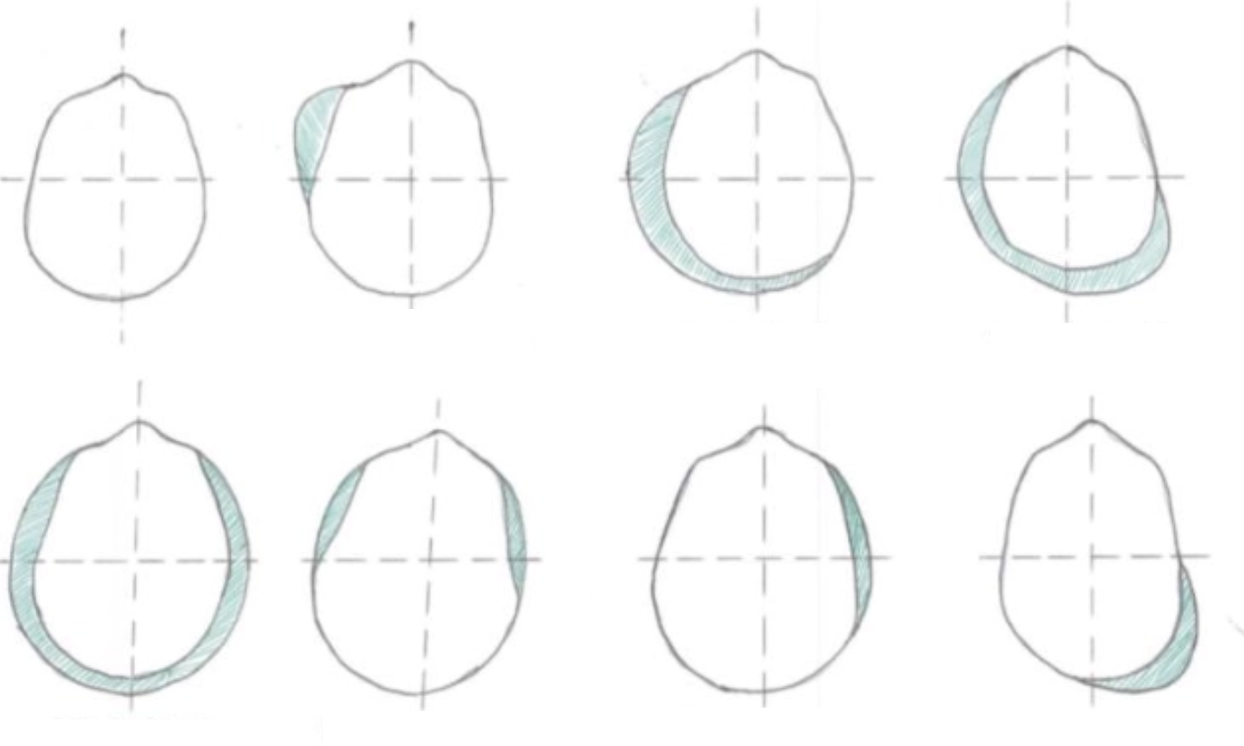
Normal
Free gas bloat (2˚ bloat)
Froth bloat (1˚ bloat)
Vagal indigestion aka. “papple”
Paralytic ileus, intestinal obstruction
Pneumoperitoneum
RDA
Abomasal impaction (sand, food particles etc.)
11 Features to assess on left/right abdominal examination (+ signs indicating abdominal disease)
Rumen: Contraction, eructation, rumen fill, layers
Left paralumbar fossa
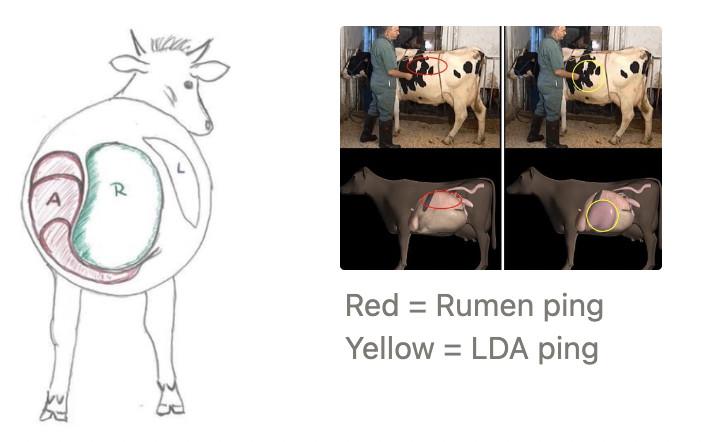
Percussion (“ping”) along line between olecranon and tuber coxae
Left AND right side
Ballottement: Splashing sounds
HR: ≥120/min → BAD
RR: Tachypnoea
Wither’s pinch test → Cranial abdominal pain
Hydration status → Severe dehydration is a concerning sign
Do not lose fluid, but usually sequestered in large organs
Percussion of liver: Absent → RDA (abomasum between liver and abdominal wall)
Spontaneous gut sounds: Hyper-/hypomotility
Percussion of ventral abdominal wall with hammer and spoon: Hollow sound → Fibrin adhesions/abomasal ulcers
List 5 requirements of a “ping” on percussion
Gas distended organ
Gas/fluid interface (will NOT ping if fibre present in rumen)
Gas under pressure
Gas distended organ against body wall
Precussor AND stethoscope over gas distended organ → Determine extent of gas distension
Changing pitch in same spot indicates residual contractility of intestine
DDx for “pings”
Left-sided ping (4)
Right-sided ping (5)
Left-Sided Ping
LDA (metallic)
Rumen gas cap (ABNORMAL as no fibre in rumen → Gas-fluid interface)
Physometra = Gas in uterus
Pneumoperitoneum
Right-Sided Ping
RDA ± torsion
Caecal dilation/volvulus
Spiral colon/small intestinal gas (ileus, intussusception, haemorrhagic bowel syndrome)
Physometra
Pneumoperitoneum

List 6 further diagnostic tests to perform for suspected abdominal disease
Rumen fluid analysis via rumenocentesis or stomach tube→ pH, protozoa, rumen Cl-
Ultrasound (rectal probe)
Radiography
Haematology
Serum biochemistry: Na, K, Cl, Ca, P, Mg, HCO3, TP
Abdominocentesis
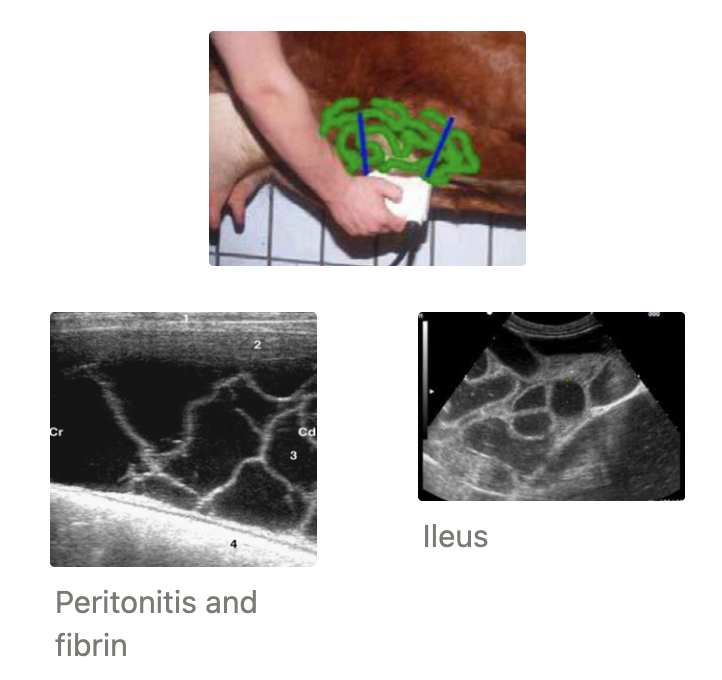
3 Abdominal diseases which can be diagnosed on U/S
Peritonitis = Fibrin looks like moving seaweed
Free abdominal fluid (uroperitoneum or ascites): Place probe along right caudoventral abdomen
Intestinal ileus/obstruction
Hypoechoic lumen (fluid-filled)
Lack of gut motility
Diameter of intestinal loops >4.cm → Surgery (normal < 3.5cm)
Abomaso-ruminal reflux
2 Causes
Electrolyte features
Pathogenesis
Causes:
Abomasal outflow obstruction (eg. LDA or RDA)
Proximal intestinal obstruction
Electrolytes:
Hypokalaemia
Hypochloraemia (>30mEq/L = Abomasal reflux)
Metabolic alkalosis
Opposite results (acidosis and hyperkalaemia) = Decompensation and poor prognosis
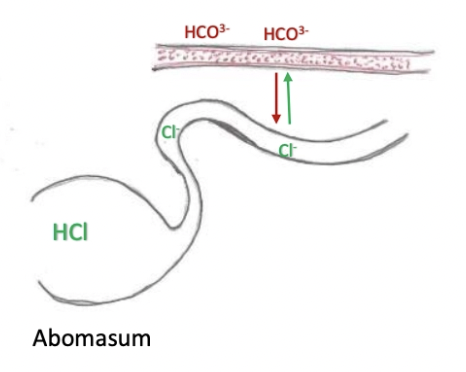
Pathogenesis:
Normal: Cl- from abomasal lumen exchanged for HCO3- in blood → Cl- enters circulation and HCO3- enters abomasum to buffer H+
Obstructed abomasal outflow: Cl- cannot be absorbed into blood (hypochloraemia) and HCO3- remains in blood (alkalosis)
3 Aetiologies of left OR right displaced abomasum
Multifactorial
Anatomy = Deep-bodied and lack of fixation of the abomasum in the abdominal cavity
Signalment: Holstein-Friesians (genetics and deep-bodied)
Mechanical = Reduced feed intake peripartum AND reduced forage:concentrate ratio (lactation rotation) → Lower rumen fill
Normal: Rumen prevents abomasal flipping/displacement
Metabolic → Abomasal atony
Signalment: FAT cows
Produce VFAs and ketones → Reduced abomasal motility
Concurrent Diseases: Cause reduced smooth muscle contraction
Hypocalcaemia
Metritis, mastitis, RFMs → Septicaemia and toxaemia
Are displaced abomasums caused by space left after calving?
NO!
LDA are NOT seen immediately post-calving
Timing: First 4 - 5 weeks post-calving
Calves positioned on RIGHT side of abdomen → Would expect more RDA as consequence (no calf as blocker)
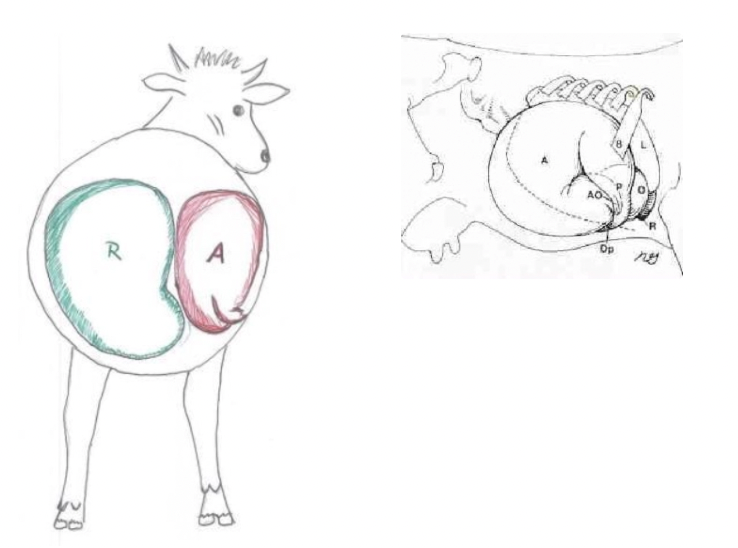
Left Displaced Abomasum
Mechanism
6 Clinical signs
2 Methods of diagnosis
Mechanism:
Anatomy, mechanical and metabolic factors cause abomasum to shift to the LEFT of midline
Abomasum distends with gas to occupy space between left body wall and rumen
Partial obstruction of pyloric outflow
Clinical Signs:
Sudden drop in milk production
Anorexia
Bright(ish) and no fever
Mild constipation OR diarrhoea
Concurrent illness
Distended left paralumbar fossa (no dorsal triangle)
Diagnosis: History and PE →
Metallic ping between the 9 - 12th ribs on the LEFT
Differentiate abomasal ping from rumen ping caused by anorexia) with DOUBLE auscultation:
Blow air into rumen via orogastric tube → Listen for bubbling sounds over the left paralumbar fossa from the rumen
No bubbles = Abomasal ping
Listen for rumen contraction over site of pig
No rumen contractions = Abomasal ping (abomasum between abdominal wall and rumen)
Biochemistry = Hypochloraemia, hypokalaemia, hypocalcaemia
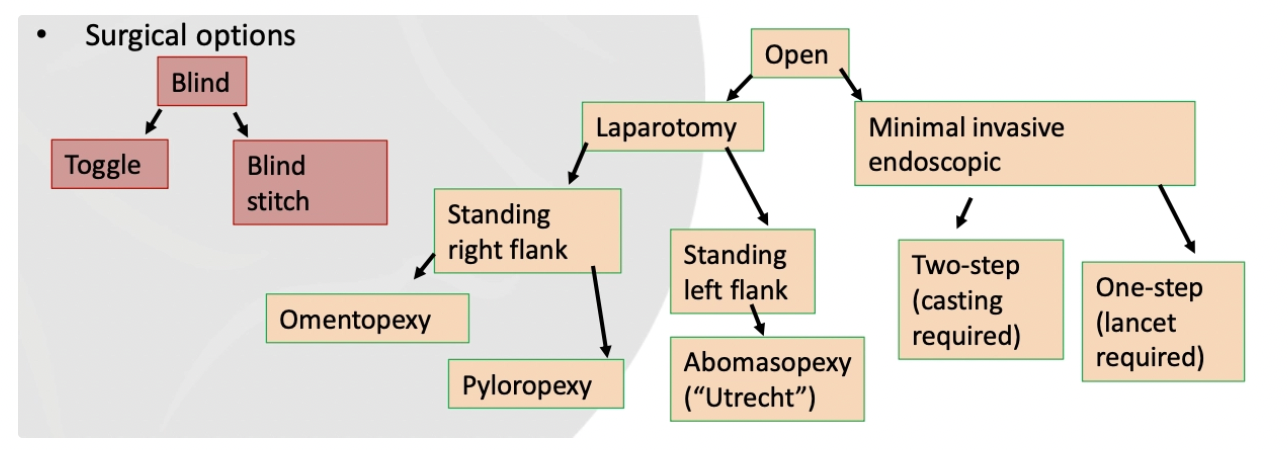
List 3 methods of LDA treatment (+ success rates)
Conservative (non-surgical): Rolling OR bumpy ride
20% success rate
Open Surgery: Standing right flank omentopexy
90% success rate
Blind Surgery: Cast and percutaneous toggling (Grymer/Sterner toggle suture)
80 - 90% success rate
Describe the method of rolling to treat an LDA
Gently cast cow into RIGHT lateral
Auscultate and ping the LDA to determine location
Rock into dorsal then LEFT lateral to help evacuate gas
OR prolonged LEFT lateral recumbency (eg. tilt table for claw trimming) BUT care with radial nerve
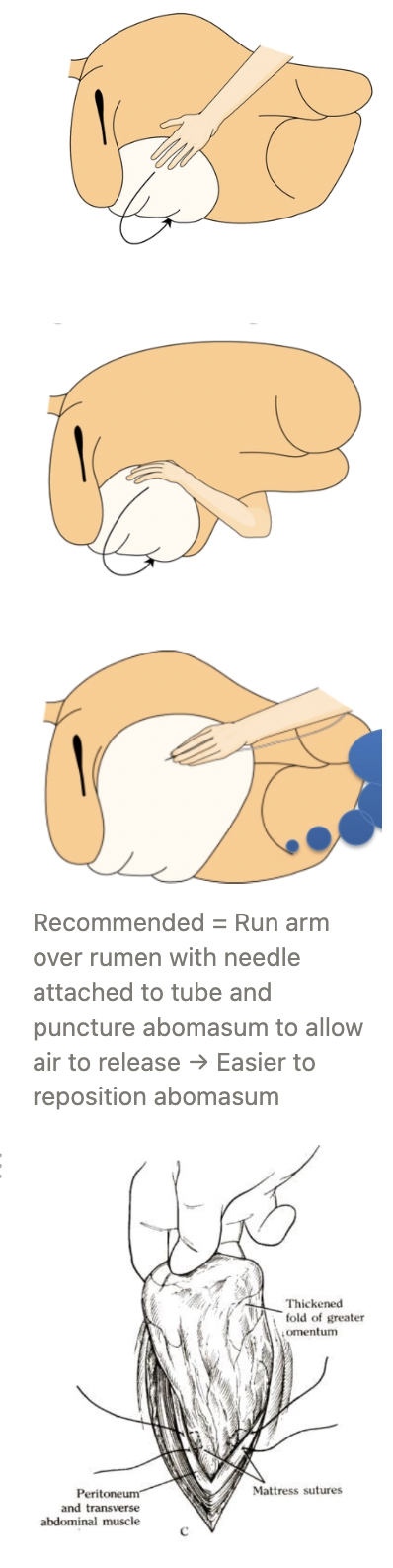
Describe the method of right flank omentopexy for LDA treatment
Right flank laparotomy
Systematic exploration of abdominal cavity
Reached over rumen and deflate abomasum with needle with flutter valve attached to a long tube
Reposition abomasum
Omentopexy = Tack omentum to ventral abdominal wall to prevent future abomasal displacement
Pull omentum through incision until pylorus can just be seen
Place mattress sutures through peritoneum, omentum and muscle
Place continuous sutures on inner layers of muscle incorporating the omentum
Grymer/Sterner toggle suture
Advantage
Kit
+ve: Introduced as improvement on the blind stitch method → Uses litmus paper to test pH of fluid to be certain abomasum is being sutured
Kit:
Trocar/canula
Nylon handle
Suture push rod
Suture
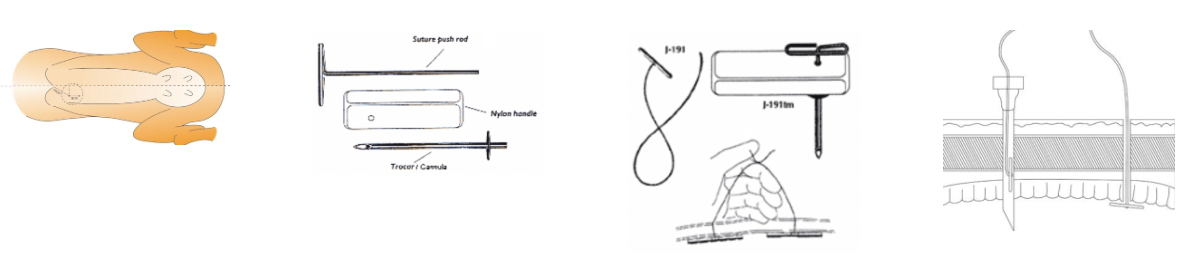
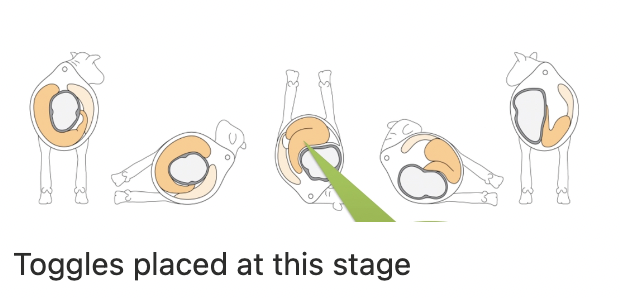
Describe the method of grymer/Sterner percutaneous toggle suture for LDA treatment
Cast cow onto right side using Reuff’s method → Roll onto back (0.1mg/kg xylazine IV)
Tie front and rear legs if required
Insert 10 - 15cm behind xyphoid and 5 - 8cm to the right of midline
Use pressure to push abomasum into right position
Push trocar through wall avoiding milk vein and other vital structures
Draw off fluid and check pH is 2 - 4
Remove nylon handle and introduce toggle
Push toggle clear of trocar/cannula with the push rod
Pull to ensure toggle is clear of trocar (not too tightly)
Remove trocar/cannula and clamp nylon with needle holder
Place 2nd toggle 5 - 7cm anterior of 1st toggle
Before removing 2nd trocar, remove as much free gas as possible from abomasum
Place surgeon’s knot tied with hands (clamps still remain on)
Leave a hand width’s distance between knot and body wall
Consider placing a toggle button to distribute pressure (MANY knots to secure in place)

Right Displaced Abomasum
Mechanism
4 Clinical signs
Mechanism:
Rumen acts as barrier to prevent LDA, but anatomical, mechanical and metabolic factors cause gas distension and atony of the abomasum
Allows abomasum to float up on the right side
Torsion = Dorsal displacement of the greater curvature
→ Counterclockwise (180 - 360˚) torsion as the pylorus moves cranially via the abdominal wall side (2nd flip)
→ Complete inflow AND outflow obstruction
Vagus nerve compromised within twist
Clinical Signs: More acute and serious than LDA
Severe dehydration
± Diarrhoea
more fluid sounds than LDA
Severe illness when torsion develops (shock)
→ Emergency surgery required ASAP
Describe treatment and prognosis for RDA
Treatment: EMERGENCY → Euthanasia OR right flank omentopexy
Right flank paracostal approach
Correct displacement by pushing greater curvature cranioventrally → Push pylorus caudally
→ Bubbling (toilet-flushing) sound when gas evacuates from pylorus (good sign)
Decompress (may need to remove fluids too with stomach tube purse-string suture)
Check viability of abomasum
Anchor with omentopexy
Prognosis: Good(ish) success rate if caught early BUT vagal indigestion may occur after severe RDA despite a successful surgery
Caecal Dilation ± Torsion
Seasonality
Clinical signs
Risk factor
Seasonality: More variable than LDA/RDA
Clinical Signs: As for RDA
Fluid sounds more caudodorsal than RDA (ventral to short ribs on RIGHT side)
French load palpated on rectal exam projecting into pelvis = Distal end of caecum OR curve of flipped caecum
Risk: High VFAs in circulation
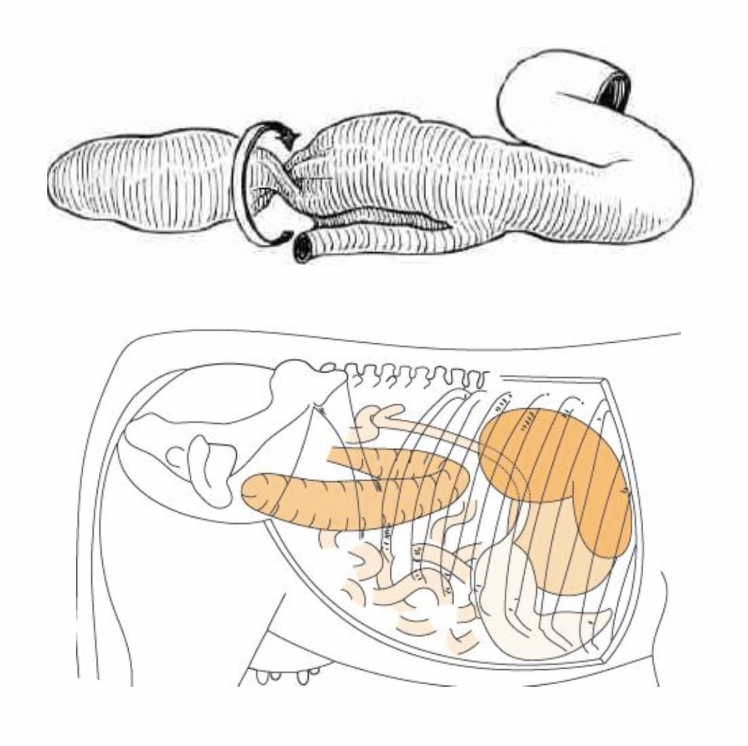
Describe treatment of caecal dilation ± torsion
Right flank approach but more caudal than RDA
Exteriorise caecum (care as necrotic)
Stab end of caecum and drain, using left hand inside to massage contents out
Invert and oversew caecum (± amputation of distal caecum if necrotic)
Return caecum to abdomen and hope it sorts itself out
Rumen acidosis:
Prevalence
Severity
Aetiology
Prevalence: Common and important disease (esp. South Island)
Severity: Mild inappetence/vague clinical signs → Severe/life-threatening
Aetiology: Excessive soluble/readily fermentable CHO in diet OR poor quality, sour feeds which animal has not had time to adapt to
Poor transition is KEY
Describe the normal mechanism of CHO metabolism in ruminants
Cow ingests non-structural CHO (eg. cellulose) which enters the rumen for microbial fermentation
Microbes produce volatile fatty acids (VFAs): Acetate, propionate and butyrate which are kept within a certain ratio
VFAs absorbed through rumen wall to enter the Kreb’s cycle for energy
Acetate (~60 - 70%) = Major energy source and used for fat synthesis (eg. milk fat in mammary gland)
Propionate (~15 - 25%) = Major precursor for glucose production in liver via gloconeogenesis
Butyrate (~10 - 15%) = Converted to ketones in rumen epithelium as source of energy
List 7 causes of rumen acidosis
Poor transition onto crops (eg. fodder/sugar beet) = Fodder beet farmer management disorder
General issue with feedlots (TMRs with highly soluble CHO to maximise growth)
Malfunction of automatic feeders
Mischievous/greedy cows which escape and get into grain
Improper mixing of TMR → Allows cattle to preferentially eat highly soluble CHO
Very lush pasture
Other cheap food sources: Grain, fruit, potatoes, turnips, brewer’s grain, fodder/sugar beet, cookie waste
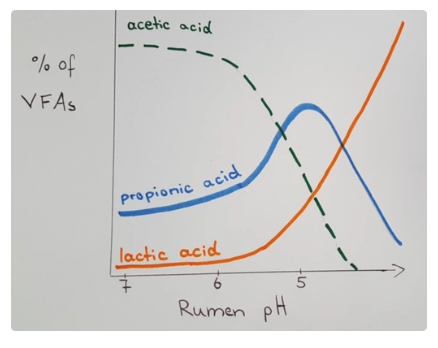
Describe the pathogenesis of rumen acidosis (ACRA)
Downward spiral
Excessive readily fermentable CHO intake (eg. fodder beet)
Readily fermentable CHO broken down by bacteria within 2 - 6hr → D/L-lactate
D-lactic acidosis decreases rumen pH allowing lactic acid-producing bacteria to increase (Strep. bovis and Lactobacillus)
Rumen pH ≤ 4.5 as more lactic acid is produced (wrong type of VFA eg. more butyrate and less acetate)
Rumen microbes die (pH < 5) → Rumen stasis and increased intraruminal osmolarity
Only Strep. bovis survives and produces more lactic acid → Local and systemic metabolic acidosis
Acid and increased osmolarity (unabsorbed nutrients) draws water into rumen via osmosis → Dehydration (fluid sequestration)
Irritation of rumen mucosa and reduced rumen epithelial blood flow → Rumenitis and no absorption of nutrients from the rumen wall
Plasma transudation into rumen
Endotoxin and bacteria escape into portal circulation
7 Clinical signs of rumen acidosis (ACRA)
Distended rumen and abdomen (slushy contents)
Reduced/absent rumen motility
Recumbent/staggering/drunk (hypocalcaemia and D-lactic acidosis)
Non-specific signs of pain: Depression, inactivity, dehydration, weak, anorexia, teeth grinding
Soft to foetid diarrhoea ± undigested grains
Hypovolaemic shock (low temperature and increased HR)
± Acute death (within 2 - 3d after rumenitis event)
4 Methods of acidosis (ACRA) diagnosis
History #1 →
Rumen fluid pH < 5 and no motile protozoa with lots of G+ bacteria
Biochemistry = Increased PCV, metabolic acidosis and hyperlactaemia
Acidic urine
PM exam = Severe inflammation with rumen mucosal sloughing

List 3 goals or rumen acidosis (ACRA) treatment
Correct ruminal and systemic acidosis → Prevent further production of lactic acid
Restore fluid and electrolyte losses → Maintain circulating blood volume
Restore forestomach and intestinal motility
5 Treatments for rumen acidosis (ACRA)
Prevent further access to CHO → Offer good hay (encourage salivation) and exercise animal where possible
Keep unaffected cattle on crop, but reduce allowance to 75% of previous day
Triage if outbreak in herd
Cull if unlikely to survive
80 - 90% of cows during acidosis outbreak recover WITHOUT treatment as they stop eating in time (disease causes anorexia)
Rumen lavage (liquid content eg. grain) OR rumenotomy (solid content eg. fodder beet) when severe
Ideally with transfaunation to replace rumen microflora
ONLY treatment that addresses issues (other treatments are symptomatic management)
IV sodium bicarbonate (5L of 5% Na2HCO3 for 450kg) (wobbly cow)
SC/IV calcium borogluconate (wobbly cow)
Additional therapy: NSAIDs, penicillin (severe rumenitis), antihistamine (prevent laminitis), thiamine (prevent PEM), fluid therapy
Care with fluid therapy as it may be sequestered into the highly osmotic rumen
Indication of intraruminal alkalinising agents (eg. MgO)
Do NOT give!
Rumen has no absorptive capacity for alkaliniser AND will exert increased osmotic effect
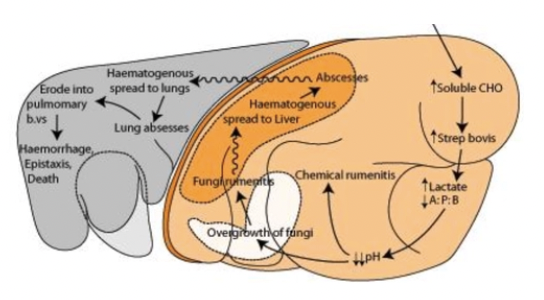
4 Sequelae of rumen acidosis (ACRA)
Abortion 10 - 14d later
Laminitis
Fungal rumenitis
Caudal vena cava syndrome
Liver abscess → Lung abscess
Pulmonary embolic aneurysm
Fatal epistaxis

Subacute rumen acidosis (SARA)
Definition
Cause
4 Clinical signs
Diagnosis
2 Treatments
Definition: Prolonged periods of depressed rumen pH between 5.1 - 5.5
Caused by VFAs (NOT lactic acidosis as for ACRA)
Cause: HERD problem due to incorrect feeding (eg. fibre:CHO imbalance from lush pasture)
Clinical Signs:
Inappetence
Poor rumen function (empty and reduced motility)
Soft faeces
Low milk fat syndrome due to altered ratio of VFAs
Reduced acetate required for milk fat production
Diagnosis: Rumenocentesis on random sample of 15 cows (mean pH 5.1 - 5.5)
Treatment:
Increase forage in diet (neutral detergent fibre = NDF)
Add sodium bicarbonate to ration if fed in shed
Mesenteric torsion
Clinical signs
Treatment
Prognosis
Clinical Signs: Classic signs of colic with rapid deterioration
Treatment: Right flank laparotomy → ID twist in mesentery and reposition intestines
Prognosis: Poor, but can get lucky
Intussusception
4 Clinical signs
Pathogenesis
Signalment
Method of diagnosis
Clinical Signs:
Colic may disappear after 12hr
± Saw-horse stance
± High HR → Drop
± Groaning and collapse
Shock, dehydration and metabolic acidosis
Distended bowel on rectal examination (± fist-shaped mobile mass to right if lucky)
± Ping over right paralumbar fossa
Pathogenesis: Orad segment of intestine slides into adjacent aborad intestine → Partial to complete obstruction
Signalment: Young animals (motility disorders = enteritis)
Older animals → Intra- or extramural masses
Diagnosis: ± Exploratory laparotomy
Treatment and prognosis of intussusception
Treatment:
Standing right flank approach
ID intussusception
Inject local into mesentery
Exteriorise intussusception and use clamps to resect devitalised bowel
Side-to-side anastomosis (superior than end-to-end)
Close defect in mesentery
Wash bowel with sterile saline
Close abdomen
Prognosis: Success if faeces passed in 24 - 48hr (BUT guarded prognosis)
Haemorrhagic Bowel Syndrome
Aetiology
Pathogenesis
8 Clinical signs
Diagnosis
2 Treatments
Prognosis
Aetiology: Acute and highly fatal enterotoxaemic disorder caused by
Clostridium perfringens type A
Aspergillus fumigatus mycotoxin
Pathogenesis: Haemorrhaging bowel → Large blood clot obstructs intestinal lumen
Clinical Signs:
Depressed, inappetence, dehydration
Decreased rumen motility
Sudden/severe drop in milk production
Succussible fluid with ballottement of right abdomen AND right-sided abdominal ping
Reduced to scant faecal production
Colic
Melaena and clotted blood in faeces (blackberry jam) → SCANT
Tachycardia
Diagnosis: U/S or exploratory laparotomy
Treatment:
Surgery = Laparotomy to find obstruction and break down clot
Do NOT open bowel → Generalised fibrinous peritonitis
Lignocaine CRI = Pro-kinetic and analgesia for 1 - 3d until faeces passed
Loading dose 1.3mg/kg → CRI @ 0.05mg/kg/min
Prognosis: 60% survival with surgery (100% mortality without treatment)

Aetiology of traumatic reticuloperitonitis (TRP)
aka. Hardware disease
Cattle are prey species with no defence mechanisms → Rapid grazing with tongue to gulp down feed without chewing (non-selective eaters)
→ Cattle will pick up metal without knowing
Hide in bushes later to ruminate away from predators
Metal only causes issues when in reticulum due to strong biphasic contractions which normally sort ingesta and presents for rumination (reticulum impales itself onto nail)
No effect when in rumen as organ is massive and will simply contract around it
7 Clinical signs of traumatic reticuloperitonitis (TRP)
Acute, subacute and chronic syndromes
Usually INDIVIDUAL cows (may be outbreaks with lots of metal eg. construction at the farm)
Sudden drop in milk yield
Anorexia and off-colour
Elevated TPR
Pain
Teeth-grinding, grunting on eructation
Hunched posture, abducted elbows or sawhorse stance
Positive Wither’s pinch test (x2), William’s test or bar test
± Large particles in faeces (sorting function of reticulum is impaired)
Severe = Generalised peritonitis → No negative pressure in abdomen
No paralumbar fossa
Tense abdominal wall
Rough peritoneum on rectal exam
Free fluid in abdomen
± Clinical signs of pericarditis or pleuritis (20%)
List 5 DDx for traumatic reticulopericarditis (positive wither’s pinch)
DDx for cranial abdominal/caudal thoracic pain
Liver abscesses
Abomasal ulcers
Acute intestinal obstruction
Diaphragmatic hernia
Omasal impaction
5 Caudal thoracic structures and 7 cranial abdominal structures that may cause positive Wither’s pinch test
Caudal Thoracic Structures:
Heart
Pleura
Pericardium
Oesophagus
Caudal lung lobes
Cranial Abdominal Structures:
Reticulum
Diaphragm
Liver
Abomasum
Omasum
Kidney
Small intestine
3 Methods of diagnosis of traumatic reticuloperitonitis
History, PE and signs of cranial abdominal pain →
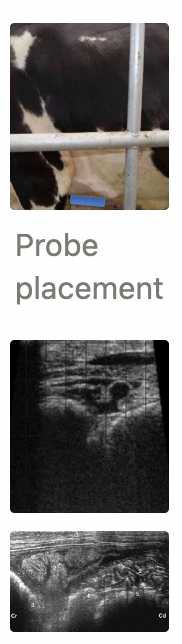
U/S over left cranioventral abdomen (near olecranon) to assess reticulum for normal biphasic contraction
Lack of reticular contractions does NOT confirm hardware disease, but presence CAN rule OUT
Radiography (high power) to ID metallic foreign bodies
Biochemistry = Increased WBC, TP and fibrinogen
Fibrinogen sequestered within minutes to save the cow’s life (wall off disease to localised peritonitis → survivable)
-ve: Location of fibrin may reduce function of other organs (eg. vagal indigestion)
2 Treatment options for traumatic reticuloperitonitis
Conservative management 1st
Oral magnet within plastic cage → Prevents further penetration of metallic foreign body
Can check success of magnet with radiographs
NSAIDs
± Fluid therapy
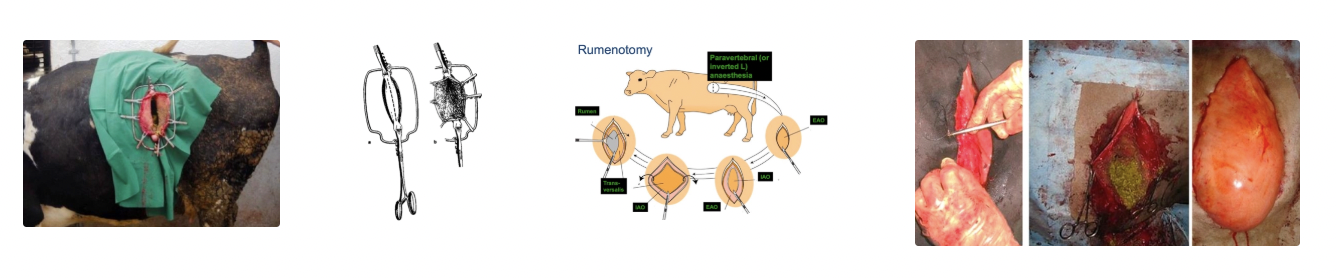
→ Left flank rumenotomy to remove foreign body
Left flank approach: Small incision as close to the last rib as possible (± rib resection if arm too short to reach reticulum)
Use anchoring sutures (continuous sutures around serosa/muscularis of rumen → Submucosa/mucosa) OR device to anchor rumen wall to abdominal wall to prevent rumen fluid leaking into abdominal cavity → Contamination
Use fingers to explore reticulum (honey combed)
Check oesophageal groove and reticulo-omasal opening → Should contract)
Remove foreign body ± fibre if necessary
Close rumen in TWO layers with continuous Cushing/Lembert
6 Sequelae of traumatic reticuloperitonitis
Depends on direction of foreign body migration
Cranial → Lung abscessation and pleurisy
Outbreak of caudal lobe pneumonia/pleurisy/thoracic abscess in ADULT cows → TRP should be considered a major DDx
Cranial/lateral → Localised peritonitis
Cranial → Traumatic pericarditis and cardiac puncture
Generalised peritonitis = Poor prognosis
Medial → Liver abscess
Medial → Vagal indigestion
Traumatic reticuloperitonitis → Pericarditis
Pathogenesis
3 Additional clinical signs
PM findings
Prognosis
Treatment
Prevention
Pathogenesis:
~20% of TRP cases have foreign bodies puncture through the reticulum into the pericardium
Infection with Trueperella pyogenes
Effusion and fibrinous inflammation
RCHF
Clinical Signs:
Jugular cording/distension and elevated pulse
Brisket oedema
Abnormal sounds (eg. muffled heart sounds, murmur, splashing)
Prognosis: Grave
Treatment: Euthanasia
Prevention:
Rumen magnet
Environmental management
Aetiology and 6 example causes of vagal indigestion
Aetiology: Vagal nerve dysfunction → Disruption of ingesta transportation from rumen to omasum
Causes: ANYTHING affecting the vagus nerve
Local abscess
Post-pneumonia → Swelling of the mediastinal lymph nodes
Common in weaner calves
Bovine leukosis
Prolonged RDA (vagal nerve runs through abomasal twist)
Reticulo-omasal (oesophageal) adhesions
Infection/neoplasia of the reticulo-omasal (oesophageal) groove
Sequelae of TRP
10 Clinical signs of vagal indigestion
CHRONIC DISEASE
Chronic and non-specific signs: Anorexia, reduced production, loss of BCS, lethargy, rough coat
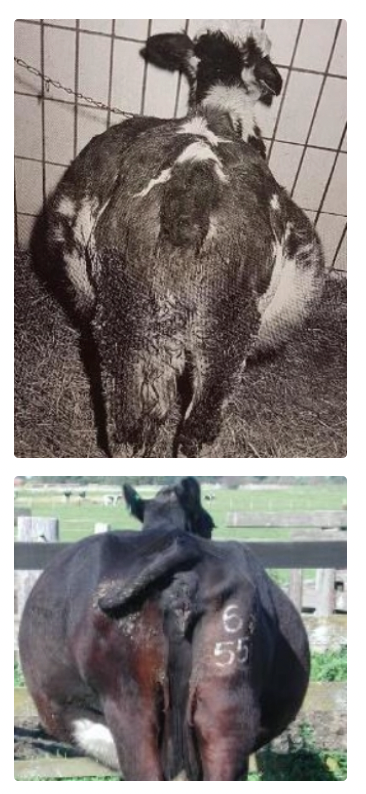
Papple (10-to-4) shape of abdomen due to rumen overload
Apple on left and pear on right due to distension of the right ventral rumen sac too
Free gas bloat with NO oesophageal obstruction (check by passing tube)
Increased frequency but decreased intensity of rumen contractions (inefficient contractions)
Bradycardia (<60bpm) due to hypokalaemia caused by anorexia
± Absent rumen layers and rare rumen ping
Iceberg effect = Fibre content form ball creating areas of gas-fluid interface
Palpable ventral rumen sack on rectal exam
Flaccid reticulo-omasal opening on laparotomy
NOT painful
Normal temperature and RR
Scant, sticky faeces with long fibres (not chewing cud)
Prognosis and 2 treatments of vagal indigestion
Prognosis: Guarded to poor (nerve damage)
Treatment:
Treat 1˚ cause if known (eg. bronchopneumonia in calves)
Rumenotomy to empty rumen, permanent rumen fistula or red devil trocar (similar to bloat treatment) = Symptomatic treatment
Aim: Address stretching of rumen to allow normal contractions to occur

6 Advantages and 3 disadvantages of standing surgery with paralumbar approach in cattle
Advantages: Cattle are stoic
Similar regardless of indication (eg. C-section and LDA)
Most practitioners are familiar with this approach
Do not need to cast cow → Fewer staff required
Easier closure of abdominal wall (vs. recumbent approaches)
Less risk for cow AND staff (vs. casting and recumbency)
Risks of Recumbency:
Muscle/nerve damage
Bloat/regurgitation
Risk of sedation
Risk of casting cow/getting kicked
No need to starve cow → Better for emergency interventions
Disadvantages:
Require minimum facilities (head bail, race with good flank access)
Cow can move around more
Risk of cow going down during surgery → Contamination
5 Steps of decision-making in abdominal surgery
Pick cases carefully to maximise chances of success (full PE essential to assess risk and concurrent disorders)
Give accurate prognosis
Get help
Location (head bail or other facilities)
Honest opinion of success rate to farmer
Honest opinion of likely cost to farmer
Clinical signs of surgical abdominal diseases
Acute < 3hr
Subacute 3 - 6hr
Chronic (>6hr)
Acute (<3hr): Colic
Kicking at abdomen and stretching out legs
Paddling in recumbency
Frequent lying down and getting up
Subacute (3 - 6hr):
Restless
Lethargy
Anorexia
Chronic (>6hr):
Recumbent
Depressed
Abdominal distension
7 Indications for surgery
Very high HR (>100 in cow and >120 in calf) that does not drop with removal of stressors
Severe colic (kicking abdomen and severe discomfort)
Full abdomen and very dehydrated
Not enough faeces and mucus in rectum
Palpable loops of distended intestines on rectal exam
Severely distended intestinal loops on U/S
No diagnosis after full clinical exam ± additional tests → Exploratory laparotomy
Indication of right vs. left flank approach for abdominal surgery
Right = Better access to most of the abdominal viscera (liver, abomasum, caecum, small intestine)
More dorsal incision to prevent spontaneous prolapse of viscera through incision
Indicated with exploratory laparotomy, LDA/RDA, caecal dilation, mesenteric torsion, intussusception
Left = Access to rumen, spleen, uterus and ovaries
4 Types of anaesthesia for abdominal surgery
Method
Advantages
Disadvantages
OR indications
Line Infiltration
Method: Local anaesthetic under skin (into muscles) directly over area of incision
+ve: Easy
-ve: NOT accurate
May not be deep enough to block the peritoneum OR risk of perforation through abdominal wall
Inverted L-Block
Method: Block nerves CRANIAL to incision
+ve:
No oedematous tissue to incise
Less risk of slow wound healing (local away from incision)
-ve: NOT accurate
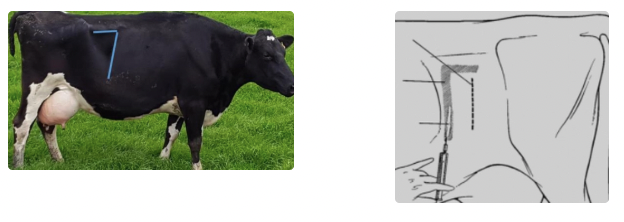
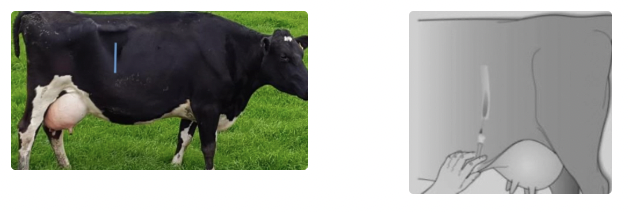
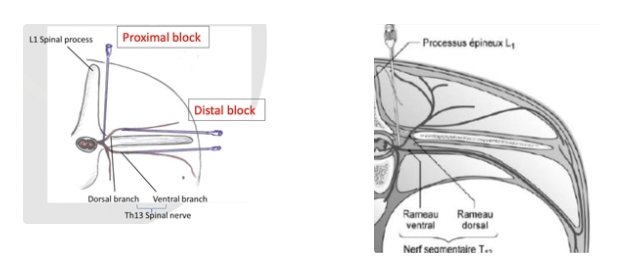
Proximal/Distal Paravertebral Anaesthesia = T13 - L2
Method:
Proximal = Block more proximal to where spinal nerves exit spinal canal
Distal = Block dorsal and ventral to transverse processes where spinal nerve exits spinal canal
+ve: Lower risk for peritonitis/adhesions and contamination → Superior post-op survival
-ve: More skill and anatomical knowledge required
General Anaesthesia = CALVES (avoid in cows)
Indications:
Regional anaesthesia cannot be used
Maximum relaxation required
Long surgery duration anticipated
Maximum asepsis needed (eg. umbilical surgery in calves or fracture repairs)
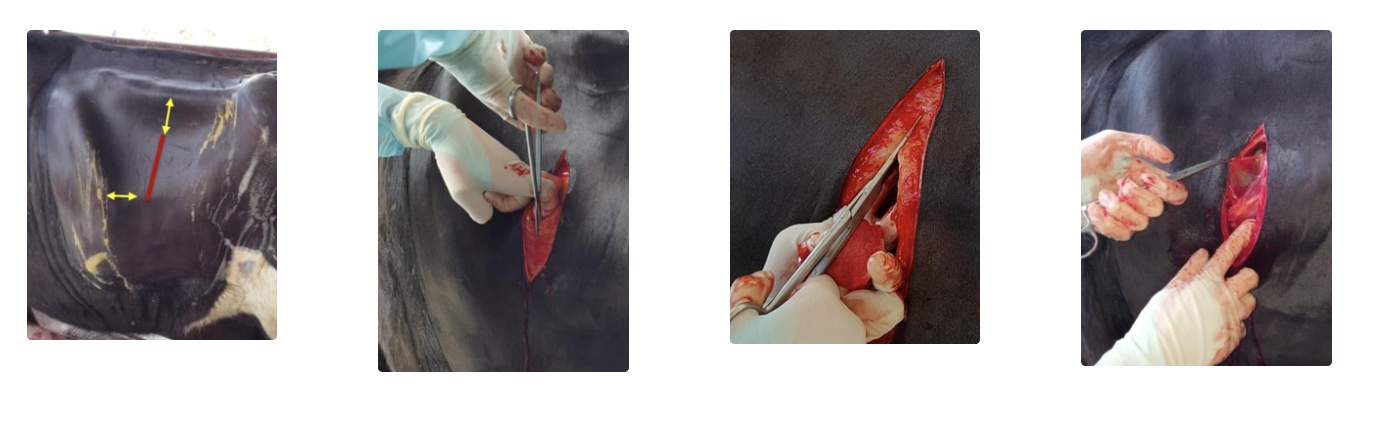
Describe the process of opening the abdominal wall (skin → muscle → peritoneum)
SKIN
Location: 4 - 5 fingers below transverse processes and 4 - 5 fingers caudal to last rib
Too high → Retroperitoneal
Too low → Viscera prolapses through incision
Size: Depends on indications (must be able to pass at least arm)
Skin cut = LONGEST
Method: Hold scalpel FLAT with index finger OR thumb over tip to protect cow from scalpel
MUSCLE
Layers:
External abdominal oblique muscle = Thickest
Internal abdominal oblique muscle
Transverse abdominal muscle = Thinnest
Methods:
Sharp approach = Cut straight through muscle layers
+ve: Easy and straight line to suture
-ve: More bleeding, trauma and higher risk of injury to internal structures
Grid approach = Stretch muscle fibres in direction they run with fingers/blunt dissection
+ve: Little bleeding, good healing, minimal trauma and protection of internal organs
-ve: Harder to suture and NOT suitable for C-section/larger manipulations
PERITONEUM
Form tent with clamps/forceps
Make small incision with scissors OR scalpel
Listen to air rush into abdomen (rule out pneumoperitoneum)
Standing animal: Wait a few seconds to allow internal organs to fall away from abdominal wall
Extend cut under finger protection
Describe the process of closing the abdominal wall
Layers
Pattern
Suture material
Needle type
3 - 4 layers
FIRST LAYER = Apposition of peritoneum and transverse fascia/muscle (peritoneum too fragile alone)
Pattern: Simple continuous AND tight → Most important layer to prevent wound emphysema
Begin suture line at ventral commissure and tie dorsally →
Less pressure on knot
Easier to make final knot
No spillage of guts ventrally during suturing
Suture: Monofilament absorbable
Needle: Round bodied
SECOND LAYER = Apposition of external and internal abdominal oblique muscles (separately OR together)
Pattern: Simple continuous OR cruciate
Suture: Braided absorbable → More tensile strength and less concern for abrasion
Needle: Round bodied
THIRD LAYER = Apposition of skin
Pattern: Ford interlocking, cruciate or interrupted horizontal mattress (ideal for midline surgery)
Pull sutures tight as less concern for skin necrosis
Suture: Monofilament nylon OR supramid
Needle: Cutting edge, semi-curved
3 After-care treatments for abdominal surgery
± Antibiotics
Routine intra-abdominal medication NOT necessary (no evidence of therapeutic/prophylactic antibiotic levels achieved)
IF required: penicillin 20,000 IU/kg for 3 - 5d #1 prophylactic choice (unless dirty/contaminated)
NSAIDs for 3 - 5d
Supportive environment (shelter, water, high quality forage)
20L oral fluids
Propylene glycol drench for 5d ± dextrose IV