PDA III Antipsychotics
1/63
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
64 Terms
Types of antipsychotics
-Typical: first gen
-Atypical: second gen
-Third gen
3 types of typical antipsychotics
-Phenothiazines: 3 subtypes
-Thioxanthenes
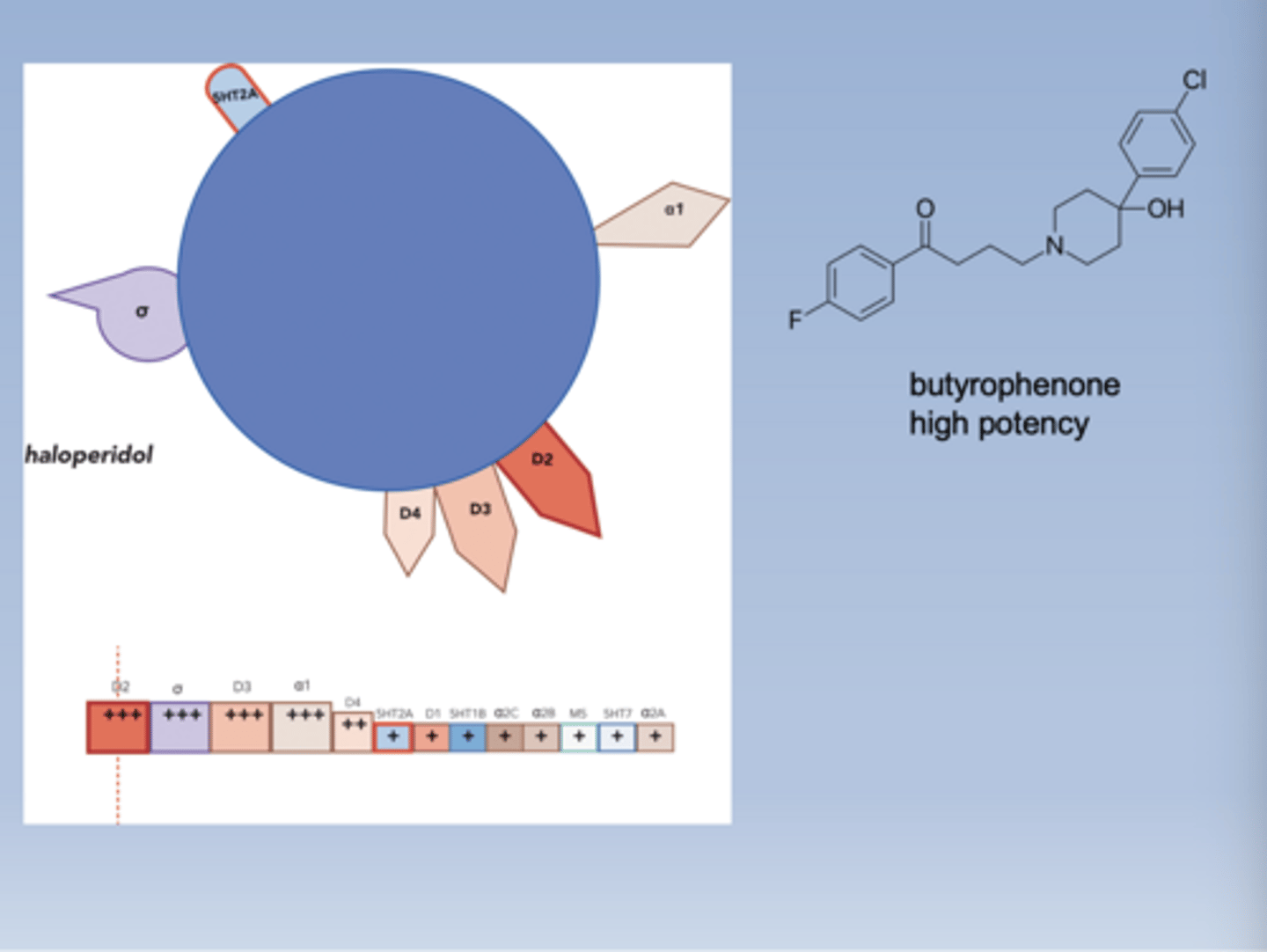
-Butyrophenones
3 types of phenothiazines
-Aliphatic: low potency
-Piperidine: low potency
-Piperazine: high potency
Atypical drugs
-Clozapine
-Risperidone
-Olanzapine
-Quetiapine
-Ziprasidone
Third gen drugs
-Aripiprazole
-Brexpiprazole
-Cariprazine
MOA of typical antipsychotics
-All are competitive D2 antagonists
-Vary in potency, but are all equally efficacious for treating schizophrenia when adjusted
-Main therapeutic effect is to relieve hallucinations, delusions, and disordered thought (positive symptoms)
-Not effective on negative symptoms (may make them worse)
D2 antagonists in the mesolimbic pathway
-Untreated symptoms on the top
-Treated symptoms on the bottom
-Decreases positive symptoms (good)
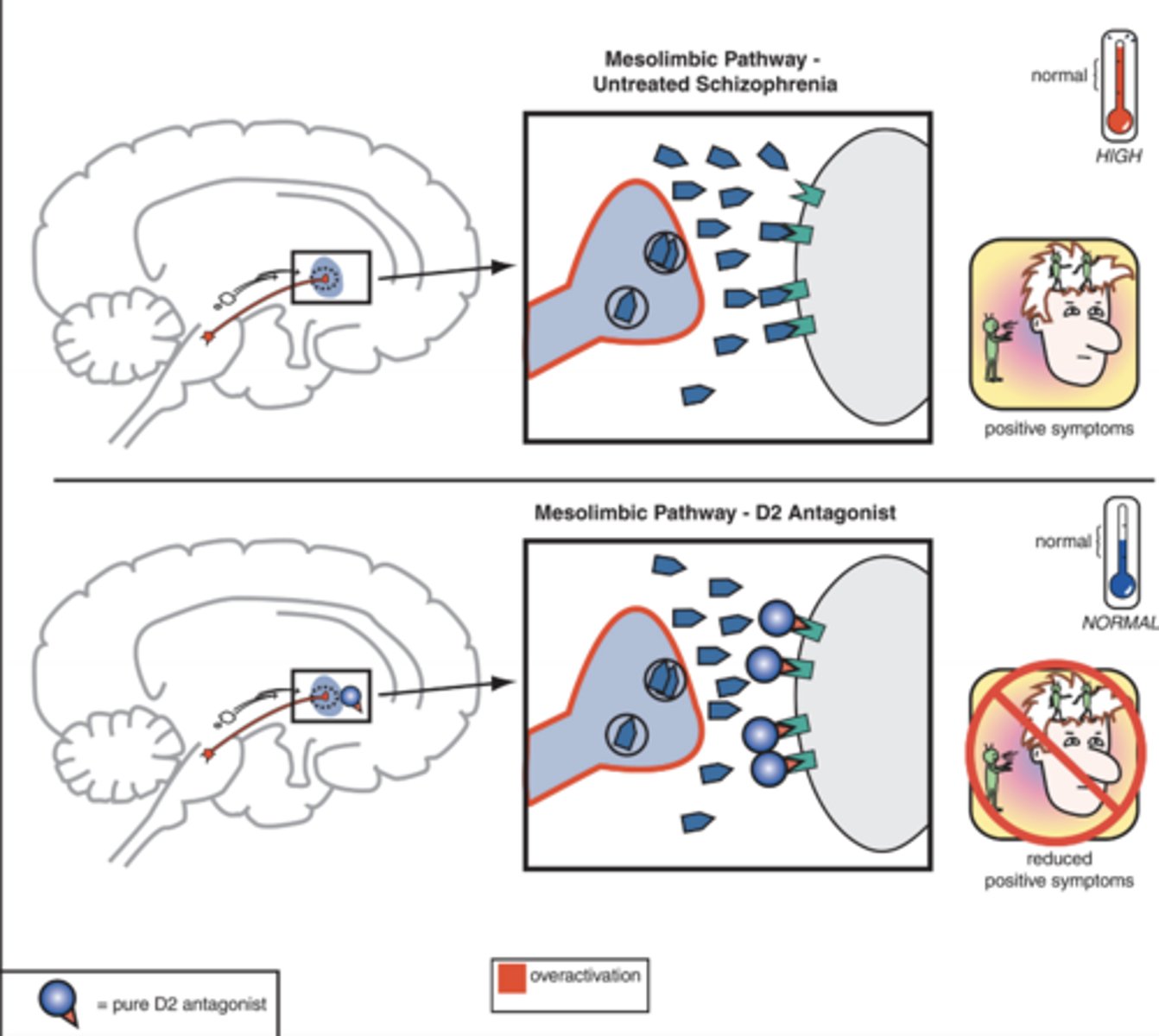
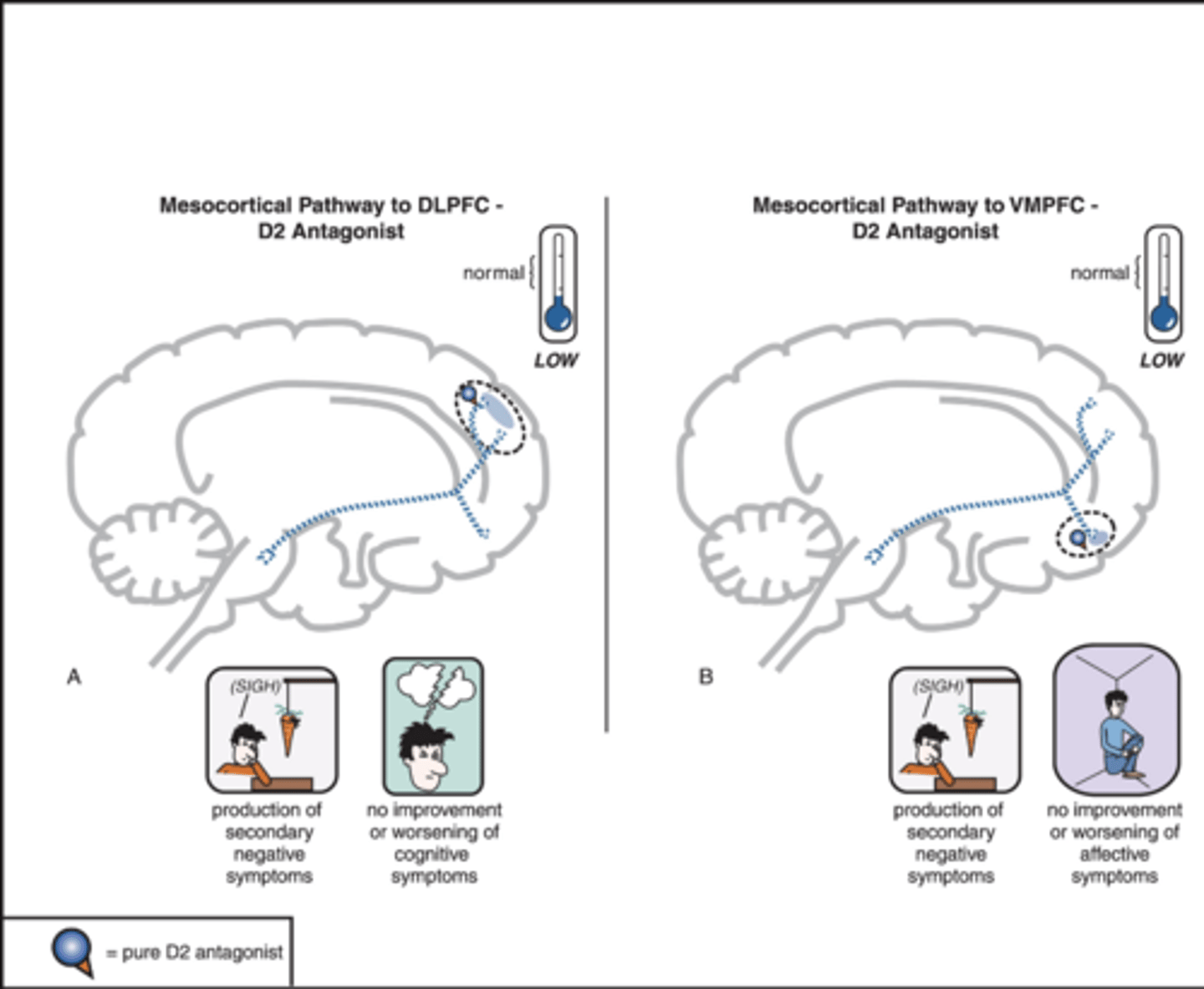
D2 antagonists in the mesocortical pathway
-Left: DLPFC (worsens motivation and cognitive function)
-Right: VMPFC (worsens motivation and increases social withdrawal)
-Worsens negative symptoms (bad)
Side effects of typical antipsychotics (D2 antagonism)
-Extrapyramidal motor symptoms
-Thermoregulatory effects
-Endocrine changes (prolactin)
-Tardive dyskinesia
Extrapyramidal motor symptoms
-Describes symptoms in the N. Striatal motor tract
-Acute dystonia
-Akinesia, parkinsonism, pseudo-parkinsonism
Acute dystonia
-Twisting contractions of trunk, limbs, and face
-Abnormal posture
-Pt thinks they're having a seizure
-Hypothesis: rapid decrease in D2 causes rapid increase in ACh
-First 1-5 days of treatment
-Seen when dose and/or potency is high
Akinesia, parkinsonism, pseudo-parkinsonism
-Akinesia: lack of movement
-(Pseudo) parkinsonism: pill rolling tremor, poor posture, shuffling gait
-Losing DA binding to receptors in the nigrostriatal tract
-Imbalance between DA and ACh
-"Dirty drugs" that also bind other receptors in the brain
-Occurs after around 5-30 days of treatment
Dirty drugs
-Nonspecific drugs
-These antipsychotics may also bind a few other receptors
-High potency group have higher affinity for DA receptors (more specific)
-Antipsychotics that bind muscarinic receptors are less likely to cause parkinsonism
Akathisia
-Uncontrolled restlessness, fidgeting
-Occurs after 5-60 days of treatment
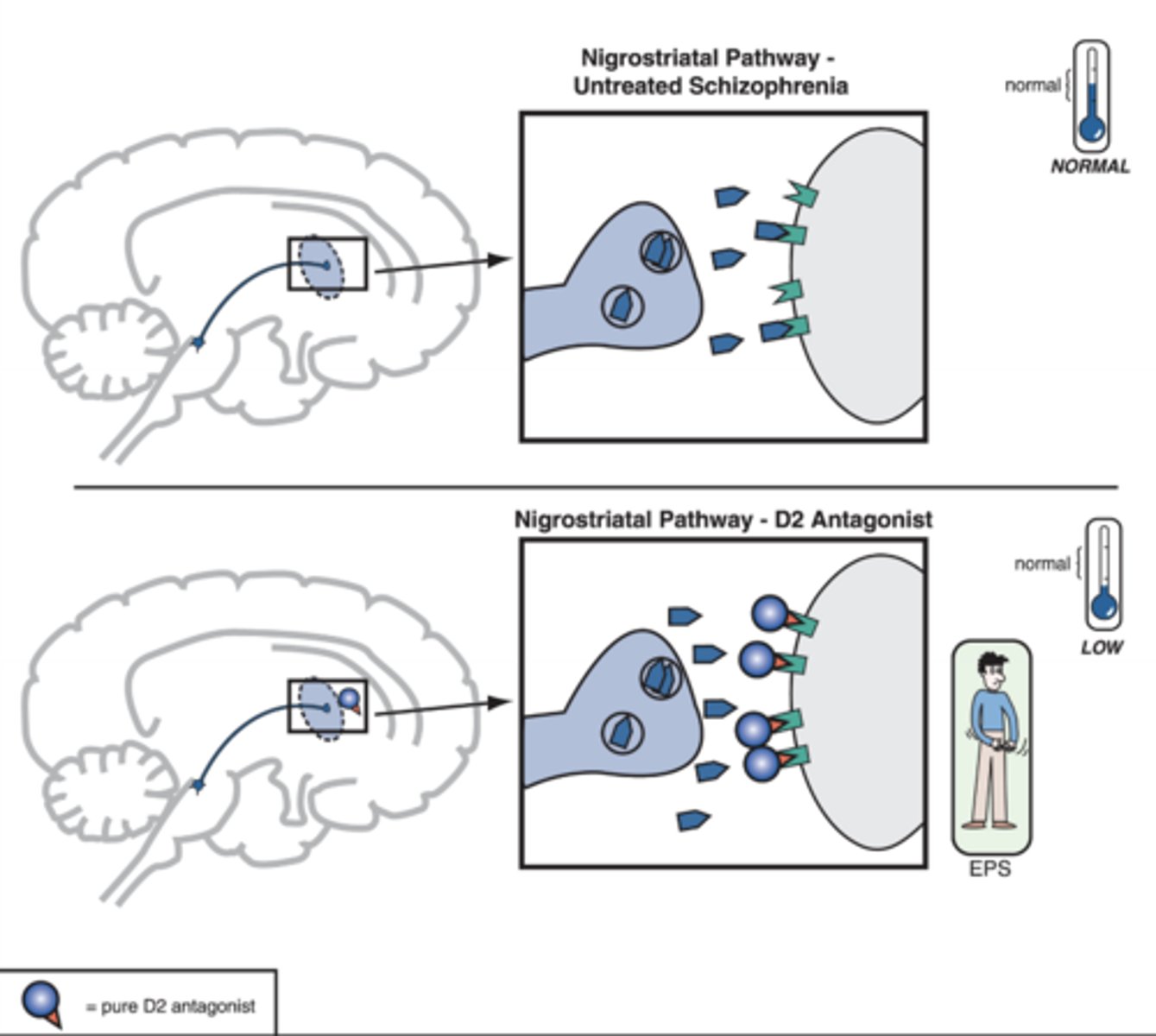
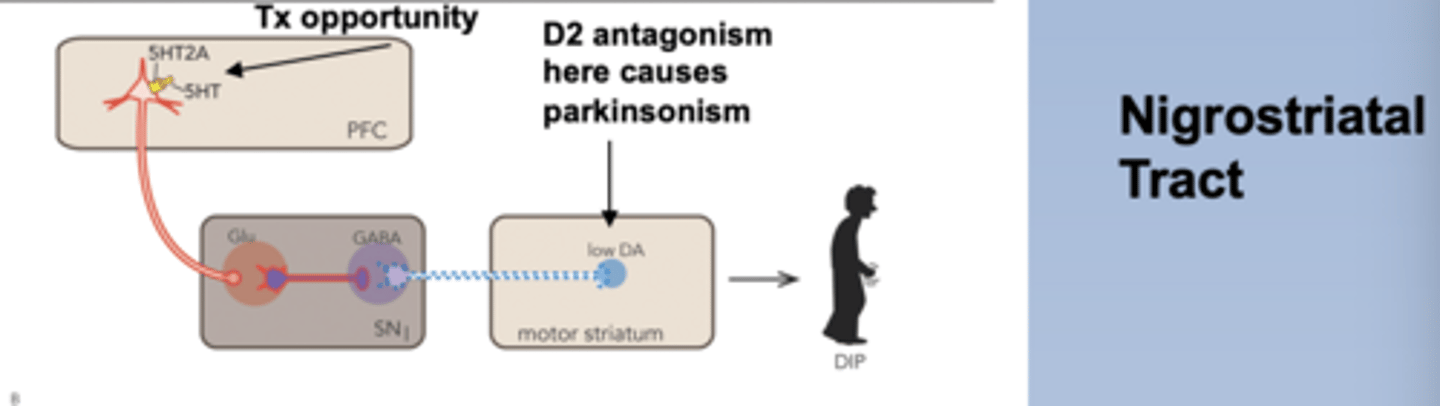
D2 antagonists in the nigrostriatal pathway
-Cause of parkinsonism
-Low DA, high ACh
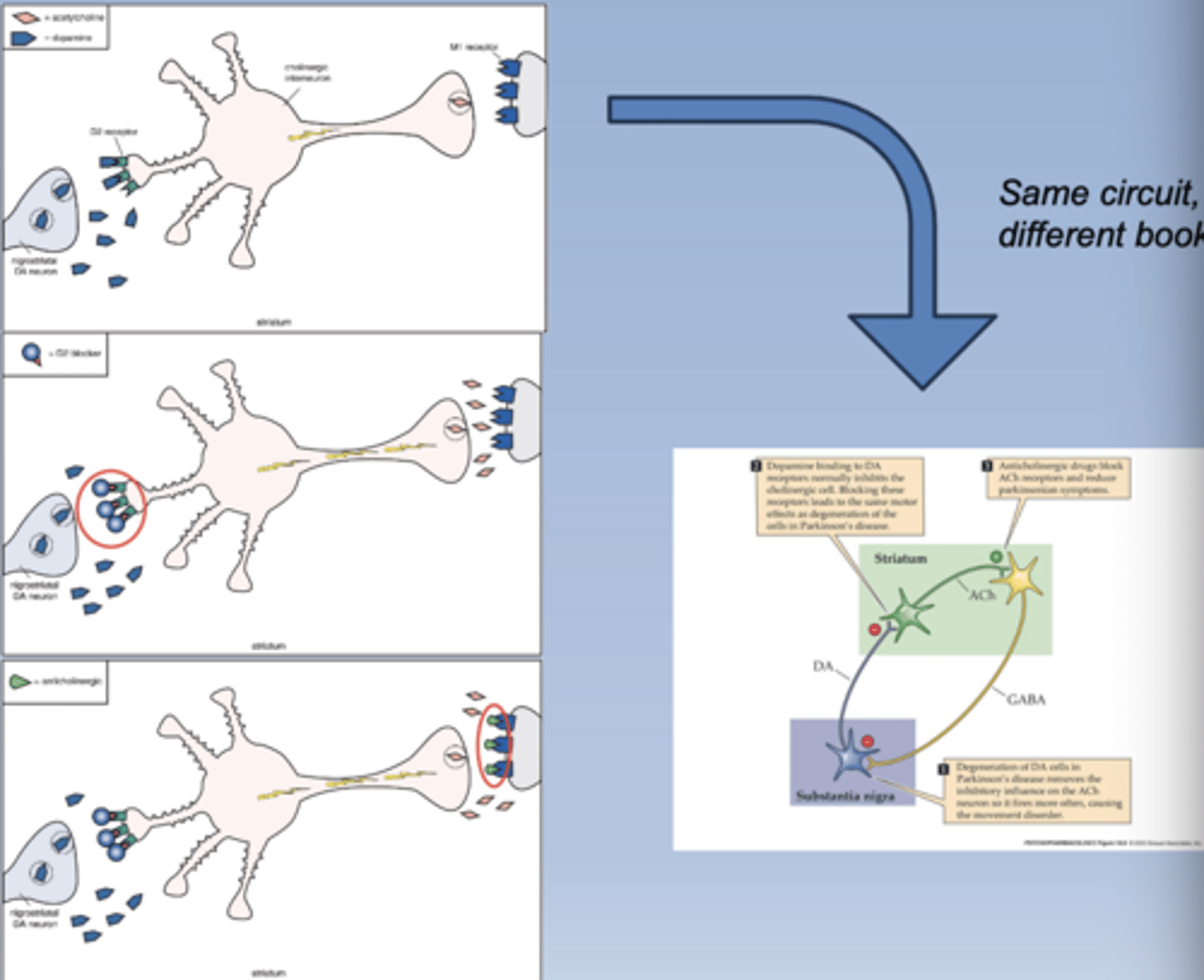
Cholinergic circuit review
-Muscarinic antagonists can combat the adverse effects from increased ACh
-Benztropine is a common muscarinic antagonist
Thermoregulatory effects
-Problems for elderly pts in the summer
-Body can't regulate its temperature
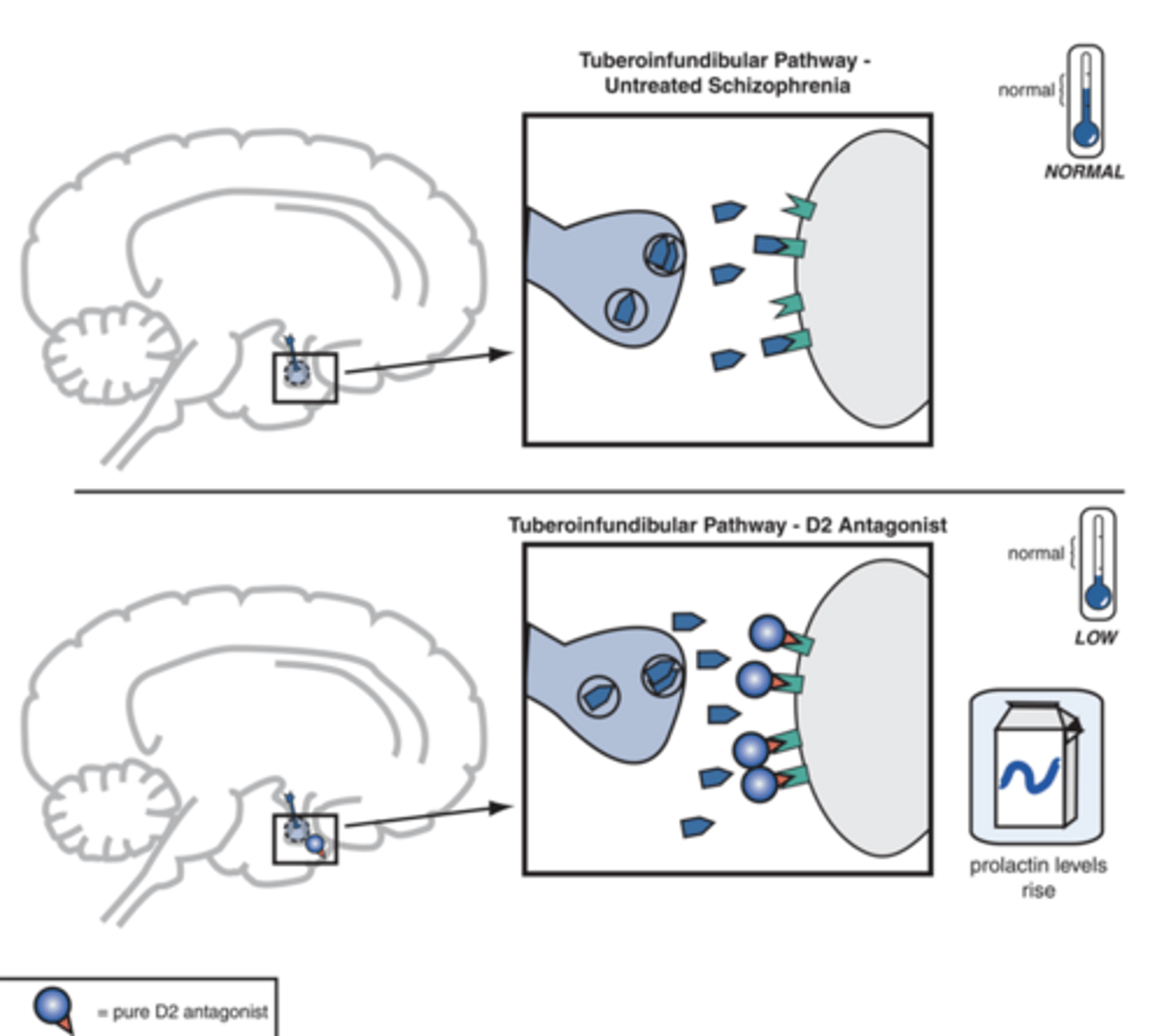
Endocrine changes
-DA in the hypothalamus inhibits the release of prolactin
-Removal of inhibition allows for excessive release of PRL
-Result is gynecomastia and milk production (galactorrhea): both men and women
-Decreased libido
-Causes adherence issues
D2 antagonism in the tuberoinfundibular pathway
-Leads to hyperprolactinemia
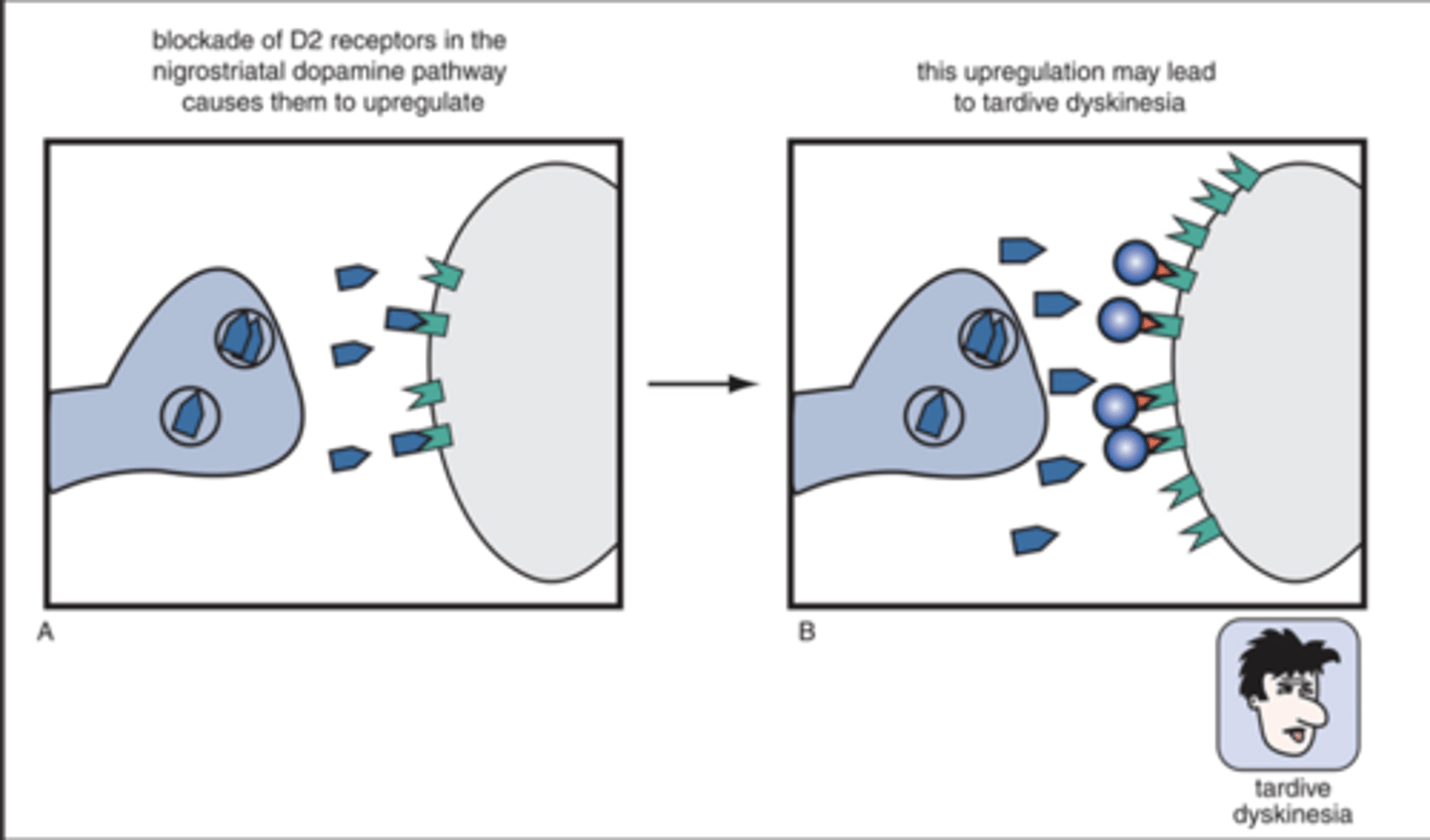
Tardive dyskinesia
-Involuntary, repetitive movements of face, tongue, lips
-Thought to be caused by DA receptor supersensitivity due to long term use
-Most cases preceded by drug-induced parkinsonism
-Occurs in the nigrostriatal tract
-Abrupt removal of antipsychotic makes it worse
-Increased dose only temporarily delays TD
-Anticholinergics worsen TD
-Pretty bad side effect
Tardive dyskinesia treatment
-VMAT2 inhibitors: valbenazine (ingrezza)
VMAT 1 vs VMAT2
-1: in the periphery and brain
-2: only in the brain
Reserpine
-Irreversibly blocks VMAT1 in the periphery
-Prevents the storage of DA, and therefore the storage of NE
-Causes depression, not used anymore
VMAT2 MOA
-Normally transports DA from the cytoplasm into synaptic vesicles for storage and release
-VMAT2 inhibitors prevent this storage: decreased DA stimulation overall
VMAT2 inhibitors drugs
-Tetrabenazine
-Deutetrabenazine
-Valbenazine
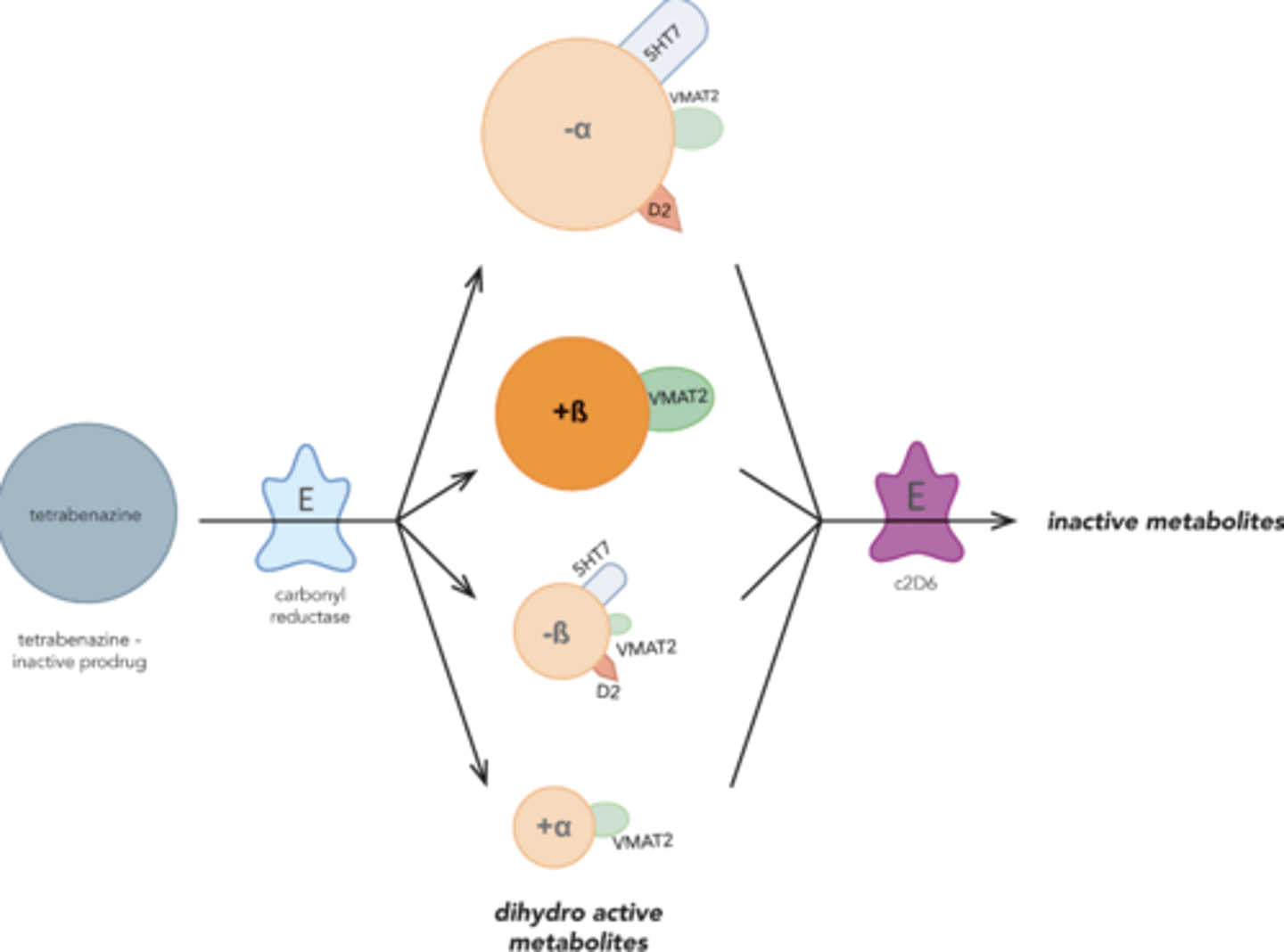
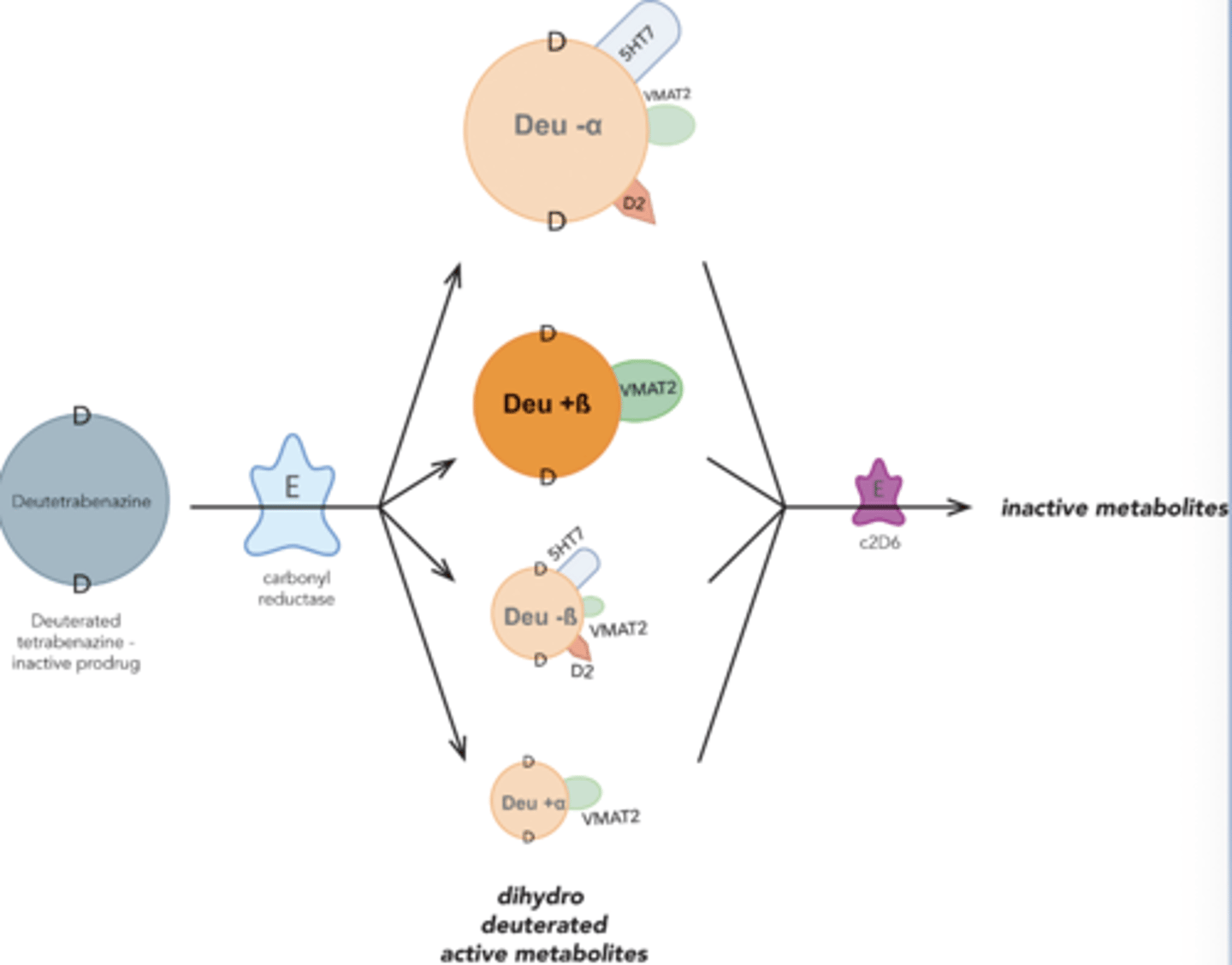
Tetrabenazine
-All four of these are reversible inhibitors of VMAT2
-Tetrabenazine converted to 4 enantiomers via carbonyl reductase
-4 enantiomers are metabolized by 2D6
-Approved for Huntington's disease, not TD
Deutetrabenazine
-Longer half life
-Less drug interactions w/ 2D6
-Approved for HD and TD
Valbenazine
-Prodrug
-End with an agent that inhibits VMAT2
-Drug goes inside DA neurons, inhibiting VMAt2 preventing VMAT from breaking down DA vesicles,

Typical antipsychotic side effects
-Sedation
-Anti-sludge
-Decreased BP and orthostatic hypotension
Sedation
-Low potency group is more sedating than high potency group
-Can be an advantage in aggressive or violent pts
-Sedative effects subside in 1-2 weeks
Anti-sludge
-Anticholinergic effects (tachycardia, dry mouth, constipation)
-Due to muscarinic antagonism
-Most common in low potency group
Decreased BP and orthostatic hypotension
-Due to alpha blockade
-Most common in low potency group
Elements of low potency group
-Sedation
-Anticholinergic effects (muscarinic antagonism)
-Decreased BP and orthostatic hypotension (alpha blockade)
Elements of high potency group
-More dopaminergic effects
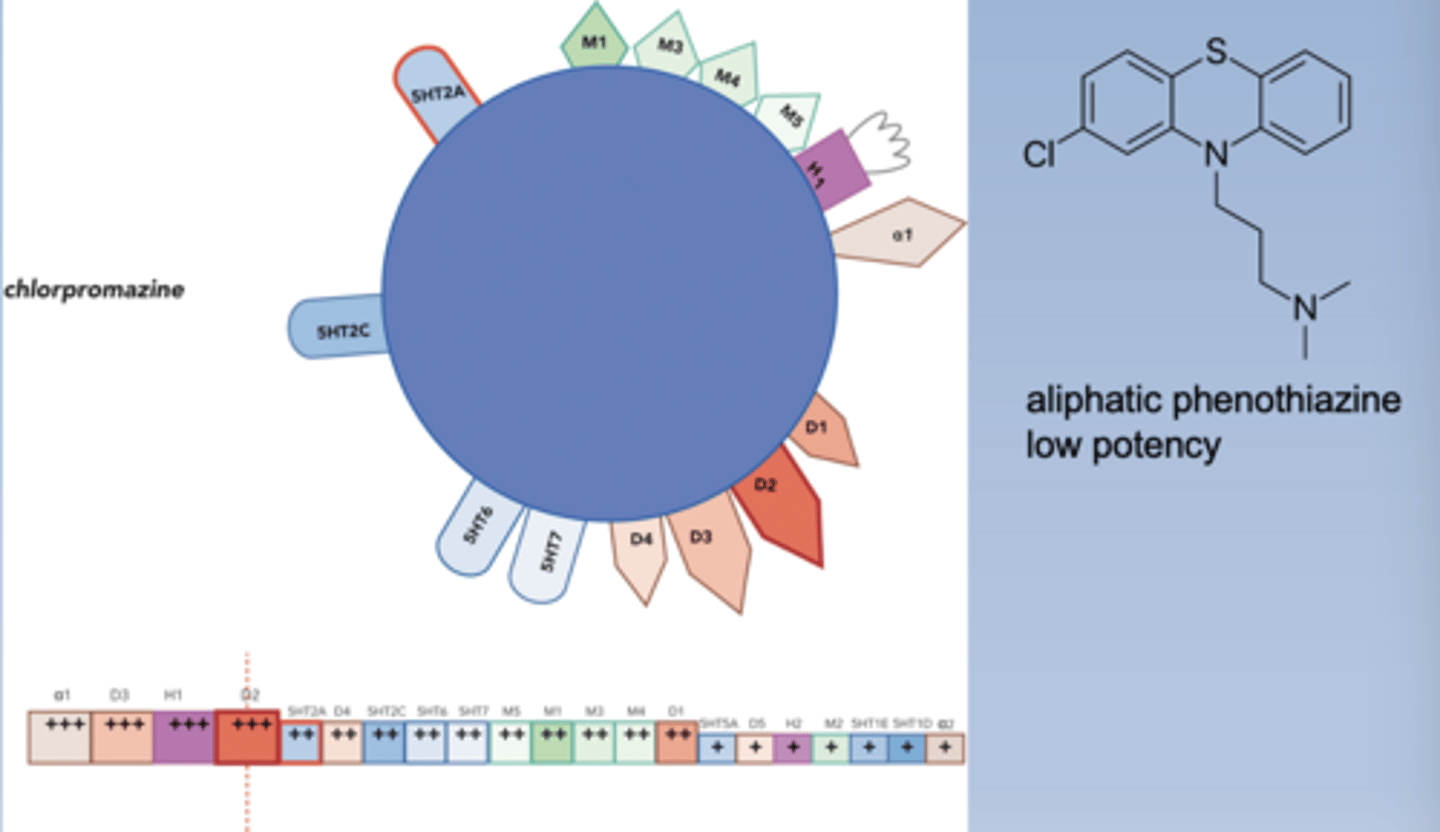
Chlorpromazine
-Low potency
-Dirty drug: binds a lot of receptors
-Boxes on the bottom: furthest to the left has highest affinity, bigger box has higher affinity
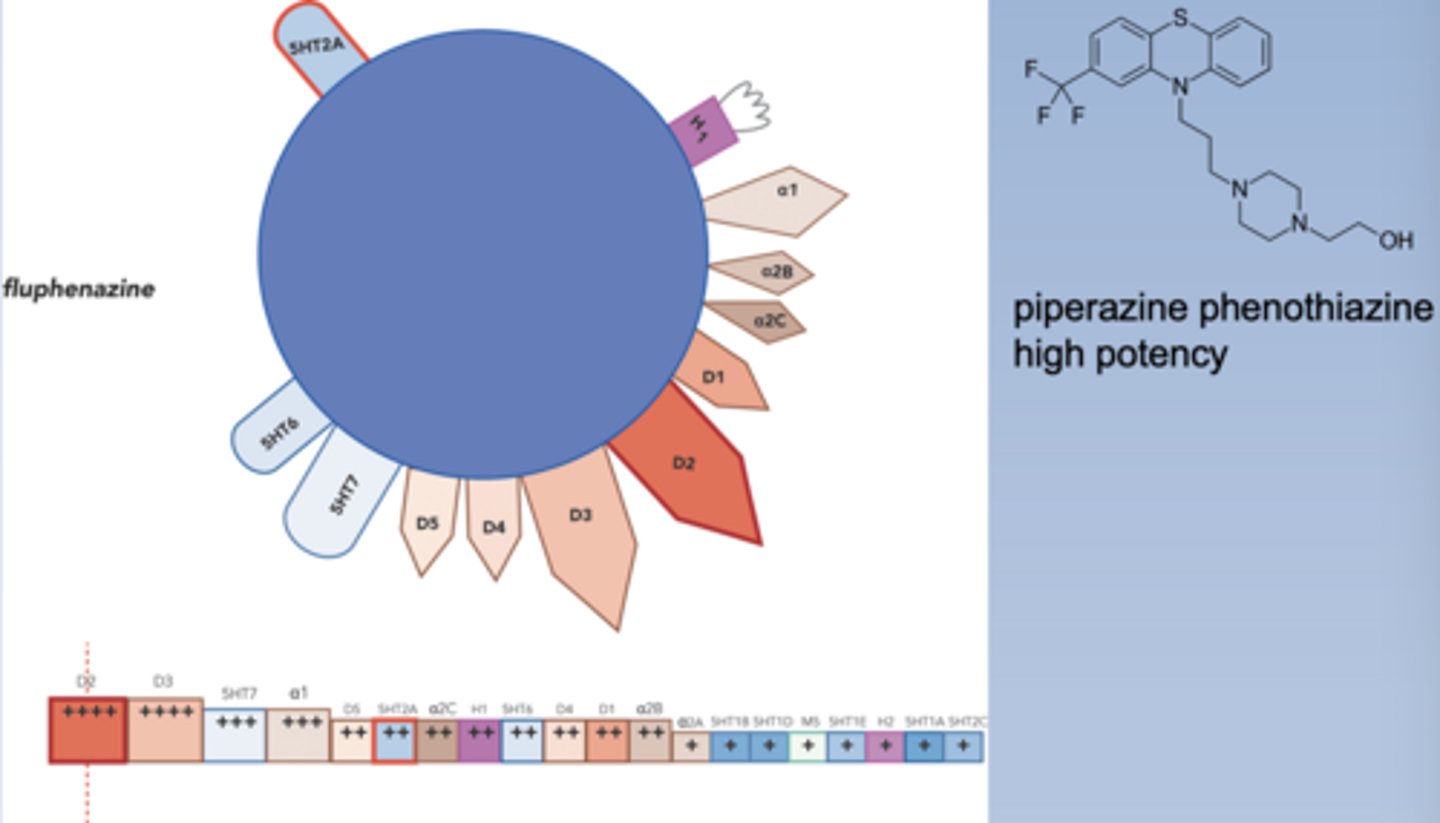
Fluphenazine
-High potency
Haloperidol
-High potency
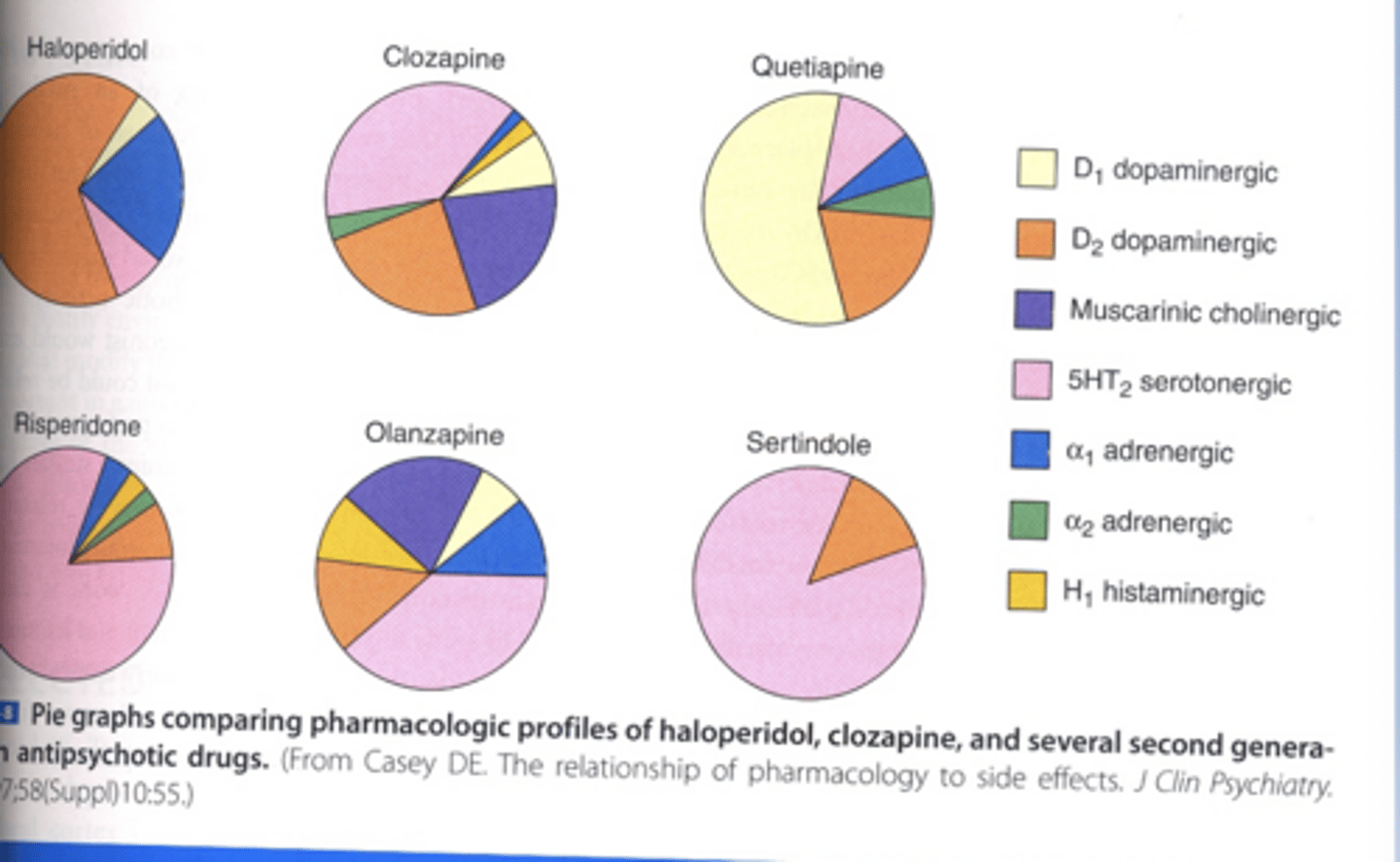
Characteristics of atypical antipsychotics
-Distinguished by side effect and efficacy profile
-Lower incidence of motor side effects and TD
-Effective at treating negative symptoms
Atypical antipsychotic MOA
-5HT2A antagonists
-Block 5HT2A receptors in addition to D2
-Benefits of 5HT2A appear to include decreased EPS, TD, and treating negative symptoms
-Work on 3 pathways in the brain
EPS
-Extrapyramidal symptoms: motor symptoms
3 pathways effected by 5HT2A antagonists
-Mesolimbic
-Nigrostriatal
-Mesocortical
Mesolimbic pathway and its therapy in atypical antipsychotics
-Glutical neurons in cortex release glutamate at the VTA
-VTA: where cell body is in mesolimbic pathway
-Emotional striatum: where axons release DA in mesolimbic pathway
-When there is too much DA in emotional striatum, causes positive symptoms
-So excitement of glutical neurons in cortex cause positive symptoms
-Glutical neurons are regulated by 5HT2A (excites glutical neurons)
-5HT2A antagonist inhibit glutical neurons, causing less DA release in emotional striatum, decreasing positive symptoms

Nigrostriatal tract and its therapy in atypical antipsychotics
-5HT2A excites glutamate's effect on GABA
-GABA causes less DA to be released in the motor striatum
-5HT2A antagonists will decrease excitement on GABA, less GABA gives more activity in the motor striatum, decreasing motor side effects (parkinsonism): drug recruits its own endogenous DA competitor
Mesocortical pathway and its therapy in atypical antipsychotics
-5HT2A excites glutamate's effect on GABA (low DA)
-GABA inhibits mesocortical pathway: causes negative symptoms
-5HT2A antagonist decrease excitement on GABA, less GABA gives more activity in mesocortical pathway, resulting in increased DA and a reduction in negative symptoms

Ratio of binding D2 to 5HT2A
-5HT2A : D2
-Higher in atypicals than typicals
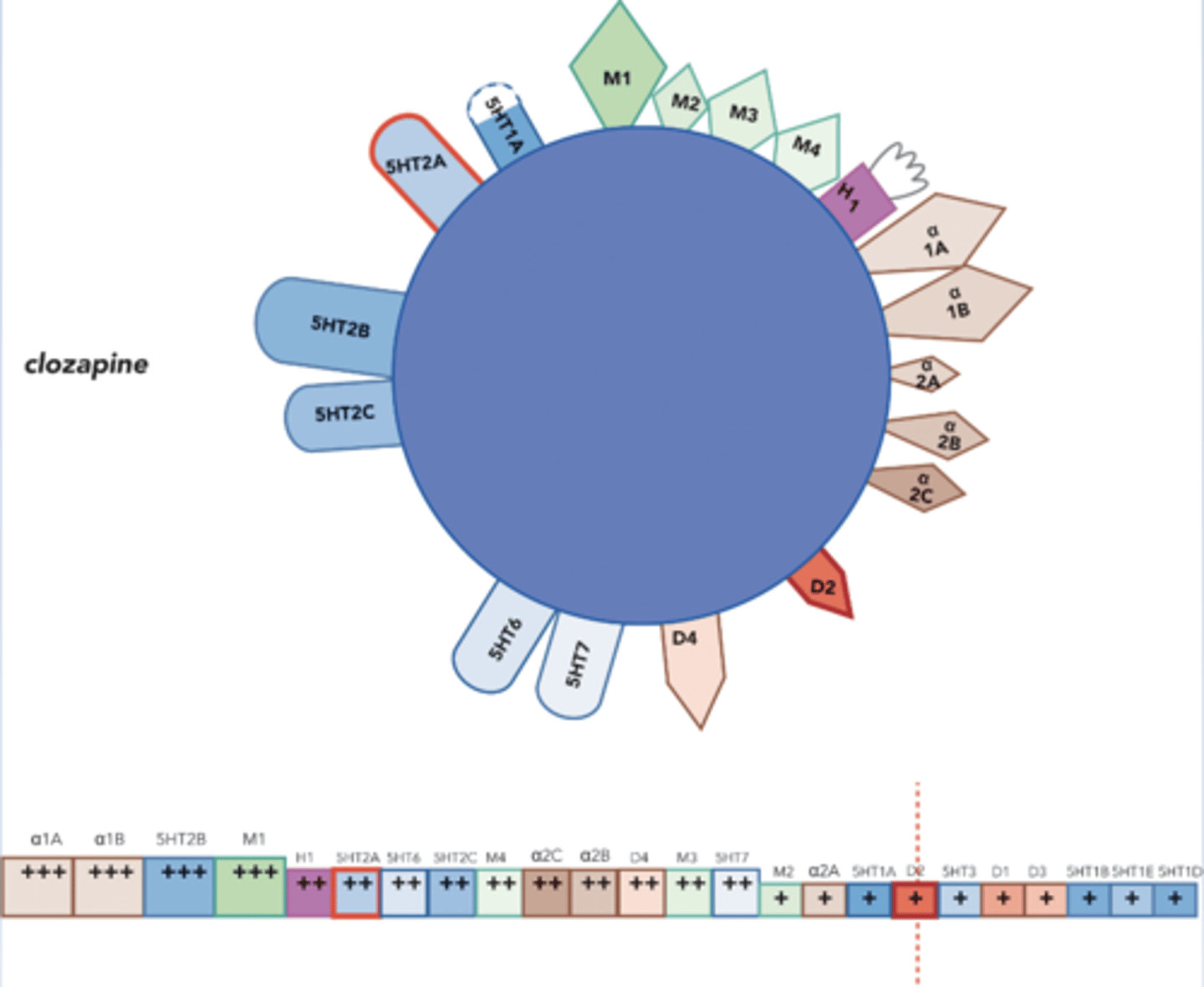
Clozapine
-Granddaddy
-5HT2A > D4 > D2
-Fewer EPS side effects (no parkinsonism), few cases of TD, no effect on PRL secretion
-Strong antimuscarinic action (but hypersalivation), rapid/dramatic weight gain, increased blood sugar, QTc prolongation, dose related seizure risk
-Agranulocytosis
Pines/dones on weight gain / blood sugar
-Both pines and dones cause rapid weight gain and increased blood sugar
-Effect is more dramatic in pines (based on high 5HT2A to D2 ratio receptor binding)
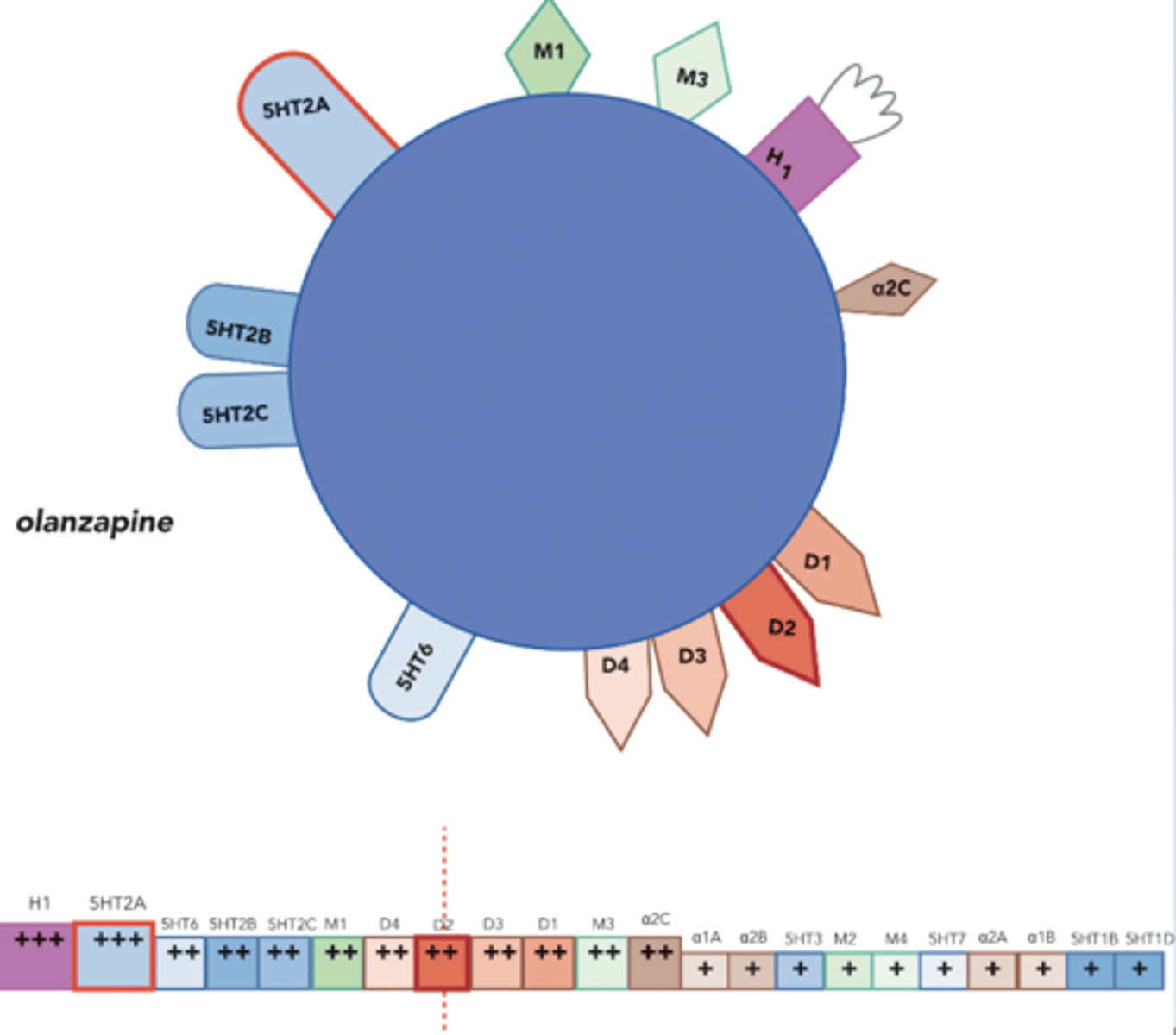
Olanzapine
-Very similar to clozapine, but without agranulocytosis
-Sedating: H1
-Increased body weight (H1), DM, increased cholesterol
-EPS effects at high end of dise range
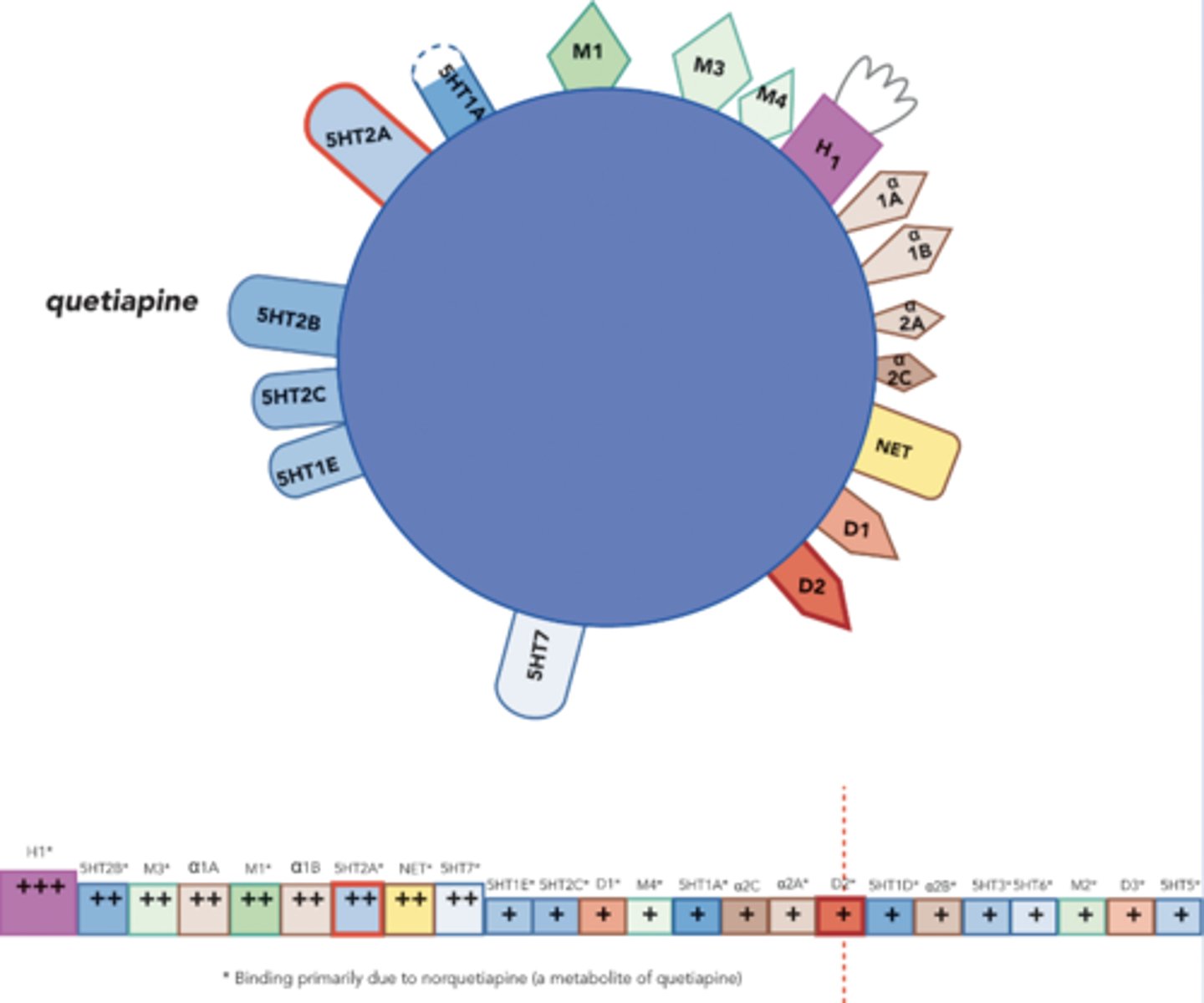
Quetiapine
-Just as effective on positive symptoms, but not as effective on negative symptoms as other atypicals
-Increased body weight, cataracts (eye exam before tx and q6months thereafter)
-Stars indicate norquetiapine metabolite
-H1: good for sleep in depression related insomnia
-NET binding is good for depression
-5HT2C and H1 may contribute to weight gain
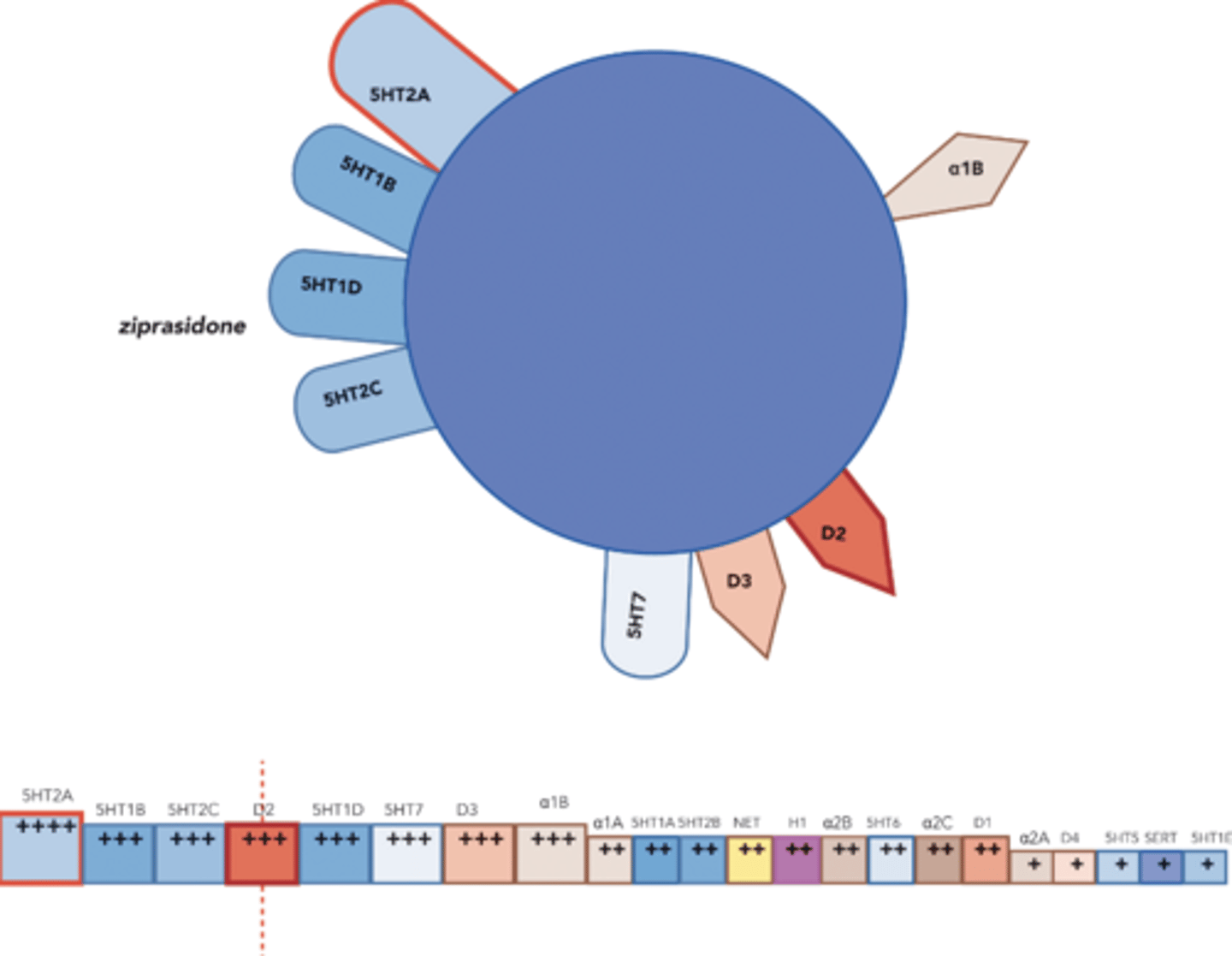
Ziprasidone
-Contraindicated in pts w/ hx of prolonged QT, MI, or arrhythmias
-Causes QT prolongation, ventricular arrhythmias and sudden death
-No effect on body weight and blood glucose
-Doesn't act at sedating receptors
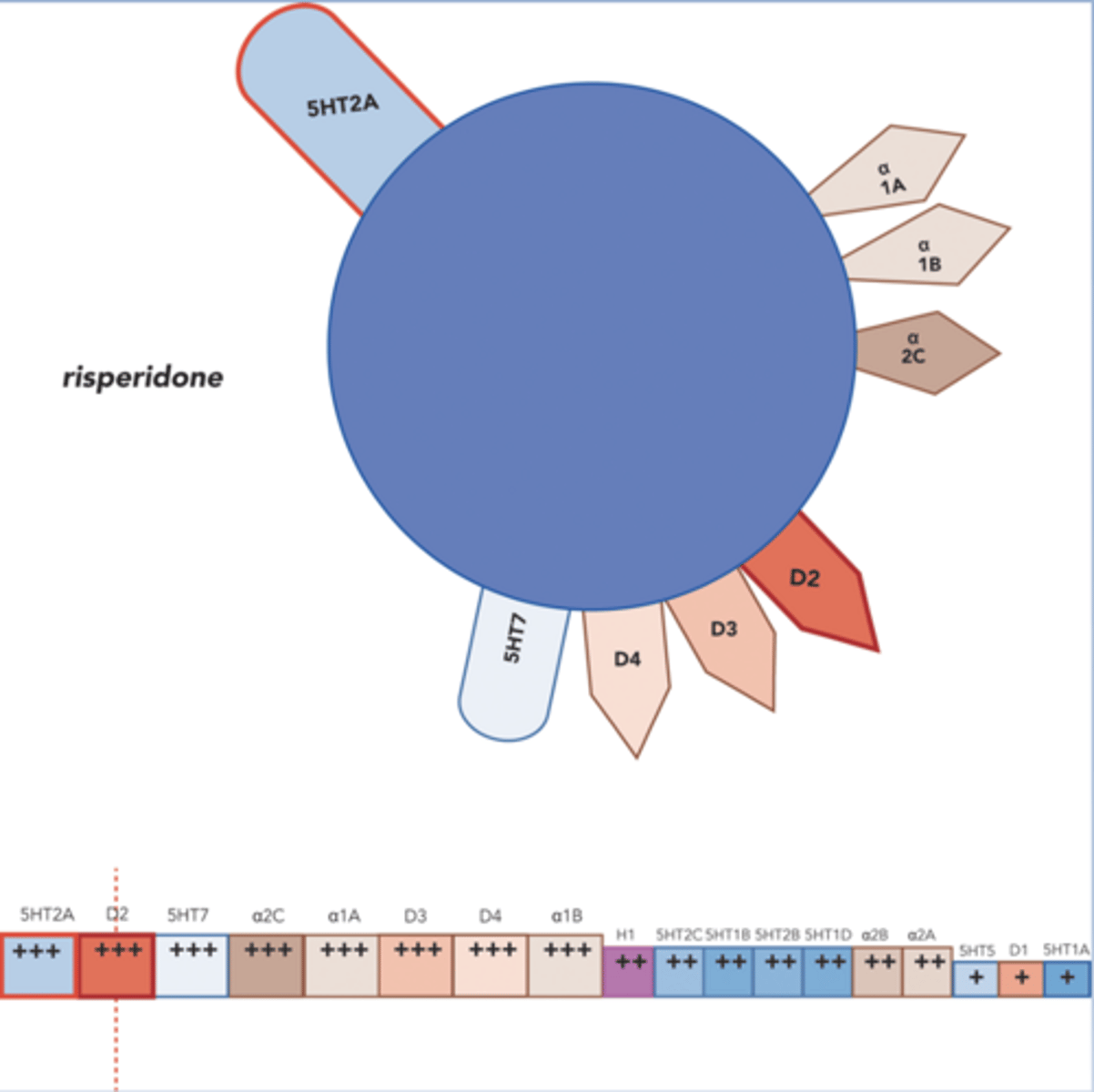
Risperidone
-Most typical of the atypicals
-Low to moderate doses, no EPS side effects
-Moderate to high doses can produce EPS side effects
-Minimal anticholinergic effects and orthostatic hypotension on the first dose
-Insomnia, agitation, anxiety
-Less weight gain than clozapine
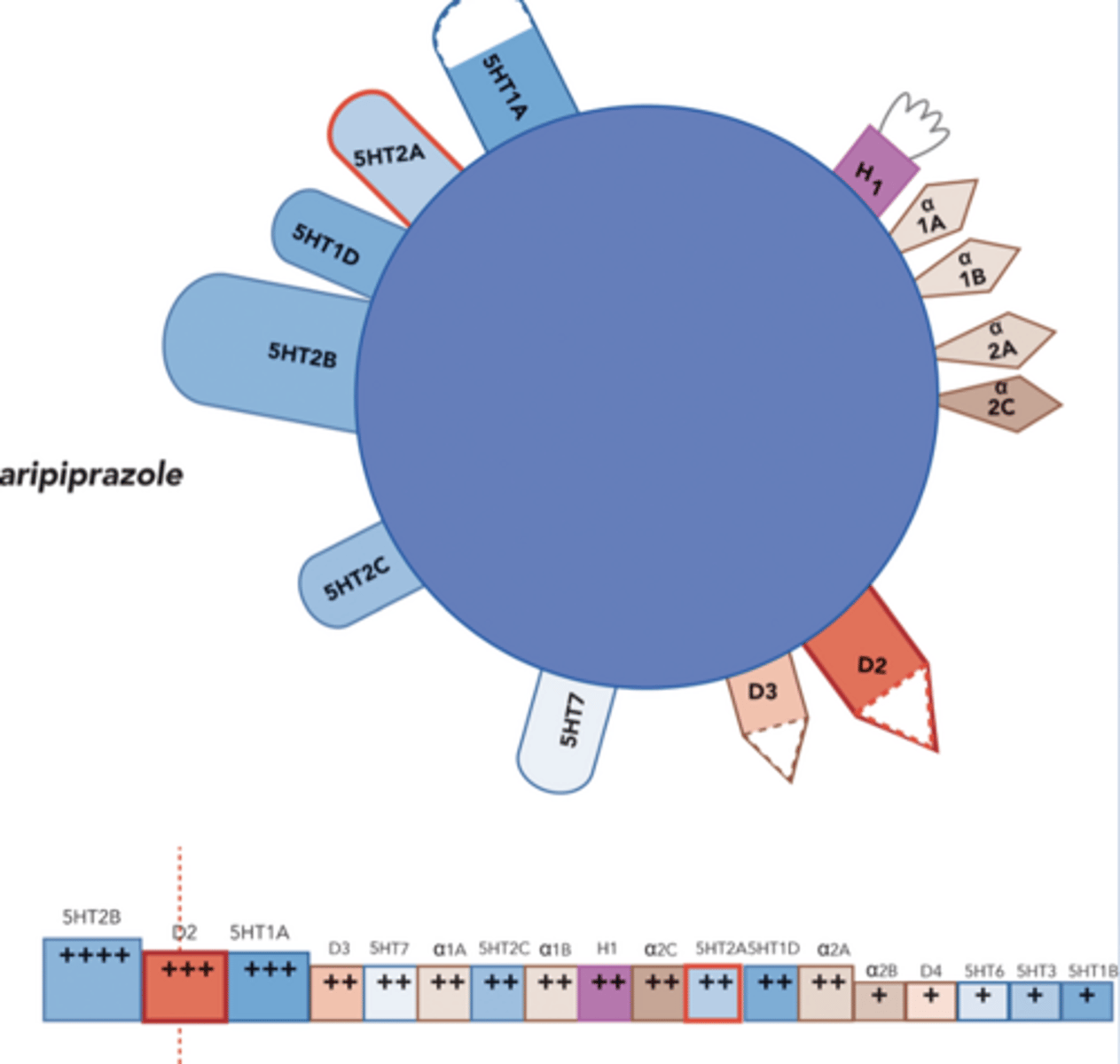
Aripiprazole
-Partial DA agonist for D2 and D3 receptors (decrease DA where its too high, increase DA where its too low)
-5HT2A antagonist
-May decrease DA activity where it is too high and increase where it is too low
-Minor side effects: headache, agitation, insomnia, anxiety
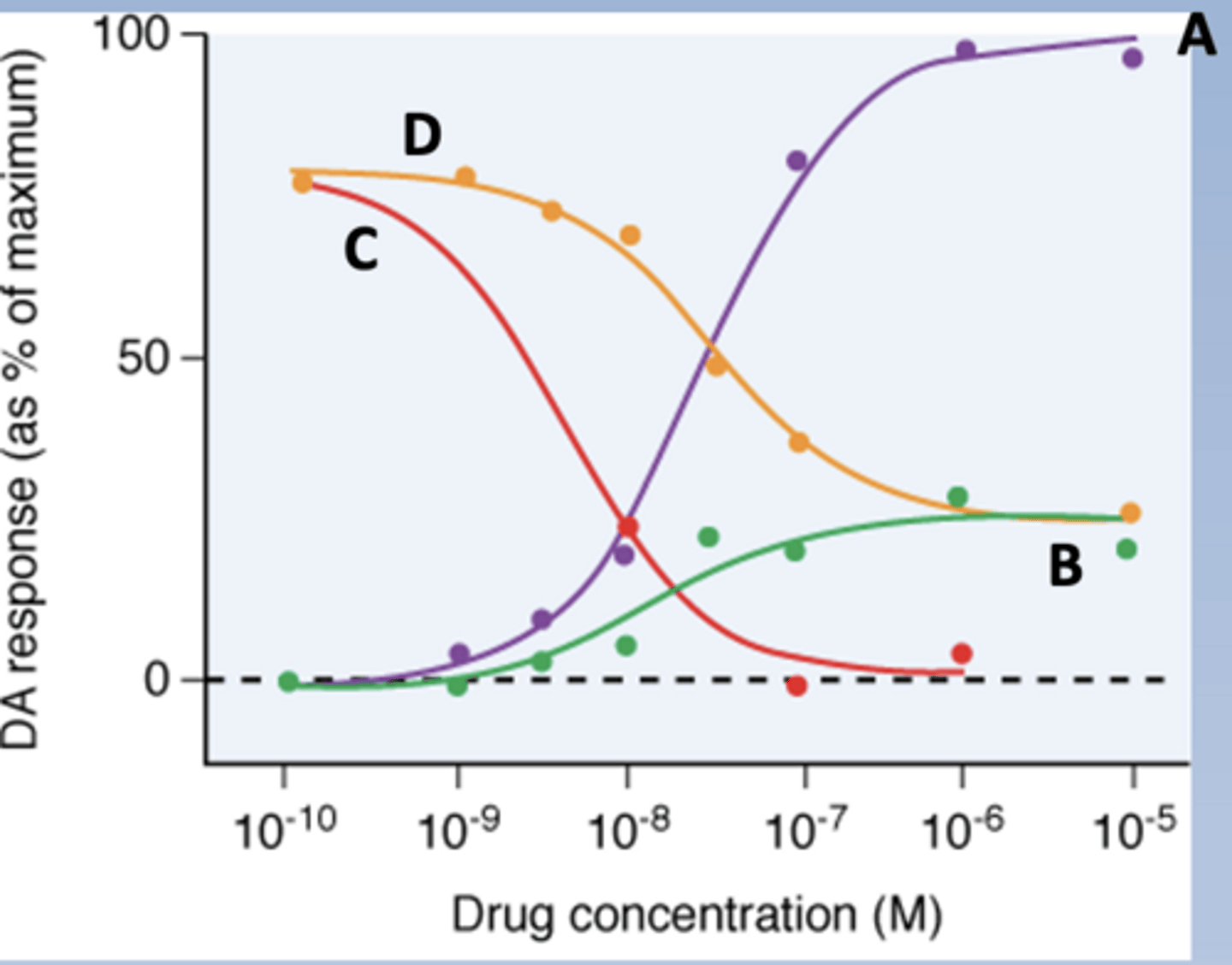
Label each curve: DA, abilify, DA+abilify, DA+haloperidol
-A: DA
-B: abilify
-C: DA + haloperidol
-D: DA + abilify
Aripiprazole receptor profile
Brexipiprazole
-Rexulti
-D2 and D3 partial agonist
-5HT2A antagonist
-Weight gain, akathisia
Cariprazine
-Vraylar
-D2 and D3 partial agonist, selective for D3
-Weight gain, akathisia, insomnia
Other antipsychotics
-Pimavanserin
-Lumateperone
-Cobenfy
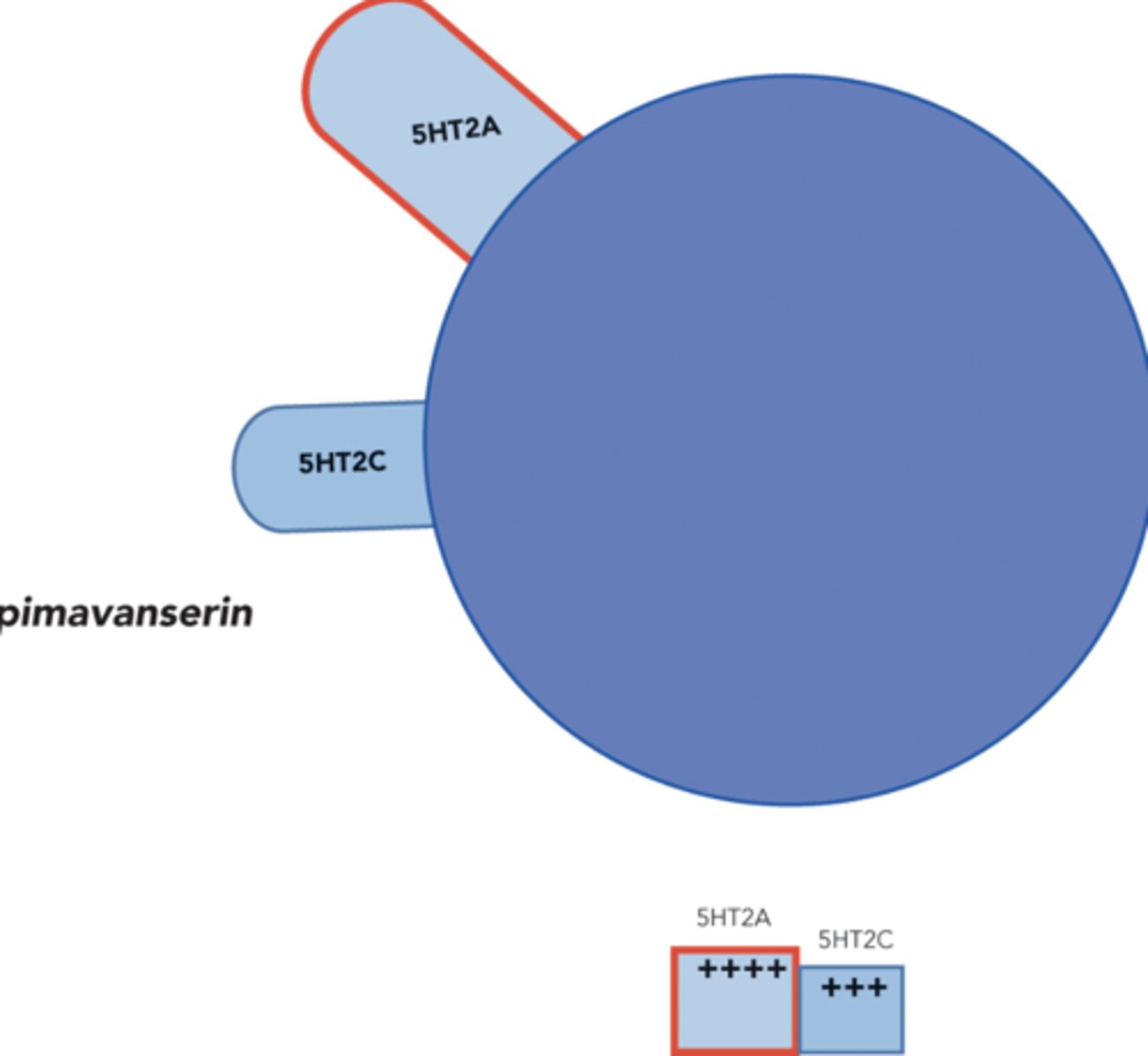
Pimavanserin
-Treat psychosis and PD
-5HT2A and C inverse agonist (decreases 5HT activity)
-Not a D2 antagonist
Inverse agonist
-The opposite effect of whatever the agonist does
-Decreases basal activity in receptors with basal activity
-Decrease signaling
Basal activity
-Level of the biological response in the
absence of added drug
-Receptor has an effect even when ligand isn't attached
Pimavanserin receptor profile
Lumateperone
-Caplyta
-Schizophrenia, Bipolar, depression adjunct
-D2 antagonist, 5HT2A antagonist, SERT inhibitor
-2nd gen MOA, 1st gen structure
Cobenfy
-Xanomeline and trospium
-Xanomeline: M1 and M4 agonist (decreases mesolimbic DA)
-Trospium: peripheral muscarinic antagonist (prevents peripheral cholinergic side effects)
Choosing an antipsychotic
-Determined mainly by risk of adverse effects
-1st and 2nd gen have about equal efficacy for positive symptoms
-2nd gen are more efficacious for negative and cognitive symptoms
-Typicals are limited by EPS and endocrine SEs
-Atypicals are limited by metabolic effects (weight gain, DM)
-First line: atypicals other than clozapine