cardiovascular system
1/126
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
127 Terms
What is the open circulatory system
Cardiovascular system that delivers blood to and collects it from peripheral tissues and the lung using the heart and blood vessels (circulates blood through tissues and passes it through the lungs to reoxygenate it)
What systems is the circulatory system made out of
Open and closed system
What is the open circulatory system?
The lymphatic system collects lymph from peripheral tissue as and recycles it into the cardiovascular system. (It is the liquid that is filtered into the tissues through the capillaries and then back)
What does the open systems consist of?
Lymph nodes and lymph vessels
How is the cardiovascular closed system layed out?
Right Heart → lungs where it is oxygenated → Left Heart → peripheral tissues
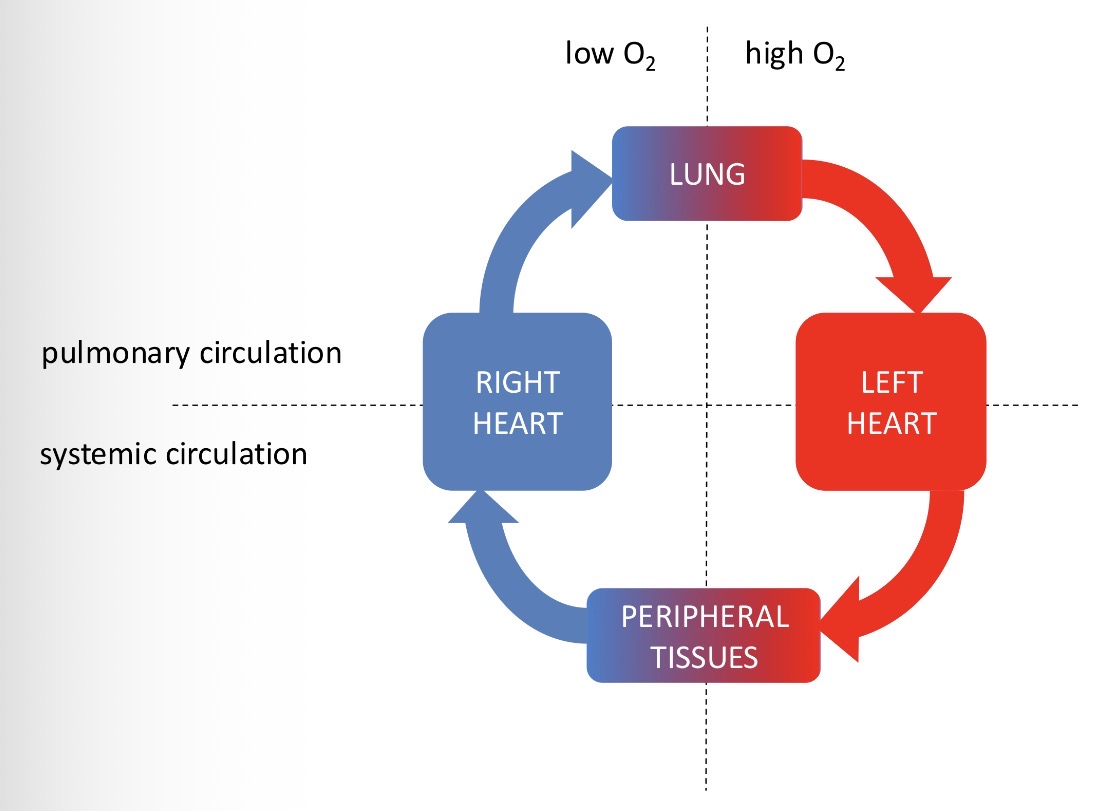
How to divide the closed circulation?
Low (peripheral tissues to right heart to lungs) and High (lungs to left heart to peripheral tissues) oxygen
Pulmonary circulation (right heart to lungs to left heart) Systemic circulation (left heart to peripheral tissues to right heart)
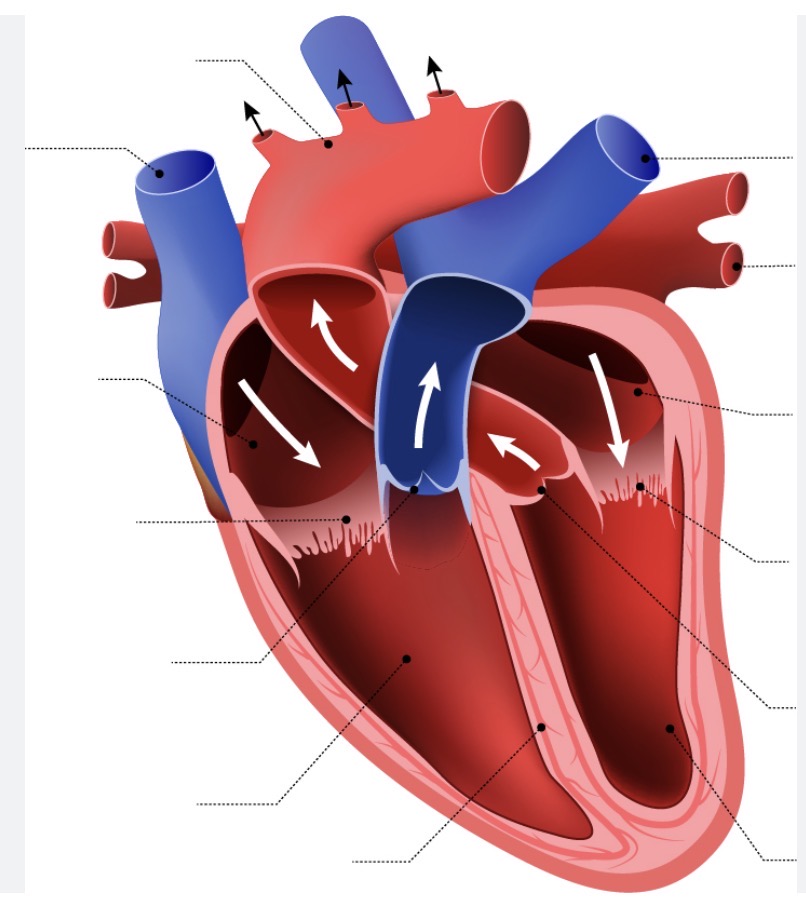
Name the sections of the heart
how many pumps does the heart consist of and what are they called?
One to the lungs from the: right ventricle → pulmonary artery → lungs → left ventricle → aorta → periphery
One to the metabolising tissues:
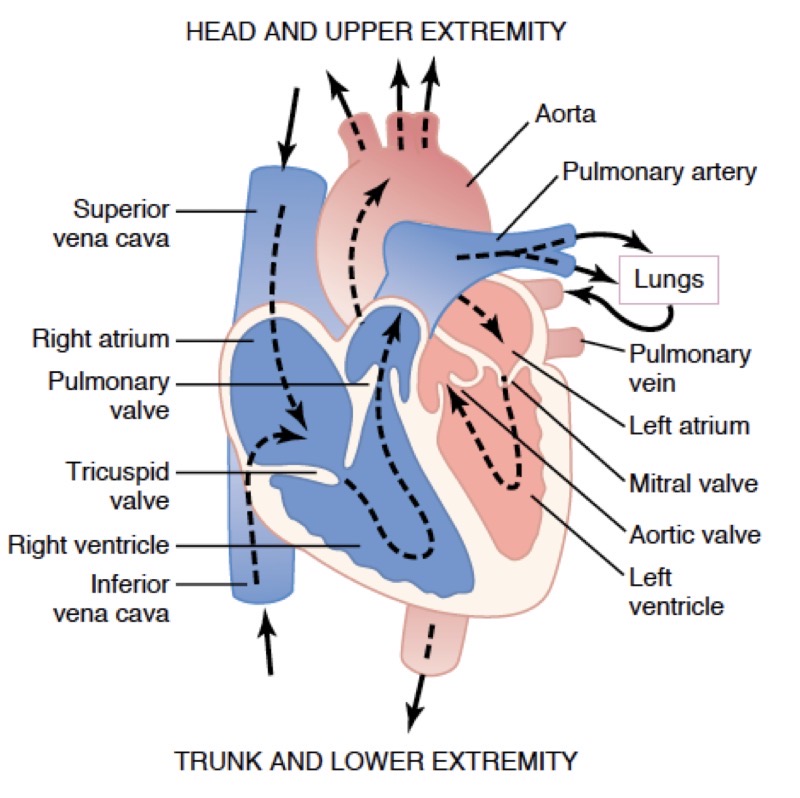
When do arteries carry oxygenated and deoxygenated blood?
Arteries carry deoxygenated blood to the lungs and oxygenated blood to the peripheries
Information of the layout of the whole cardiovascular system
What are arteries:
Transport blood under high pressure to tissues
What are arterioles:
The last arteries with muscular walls, regulate local tissue flow
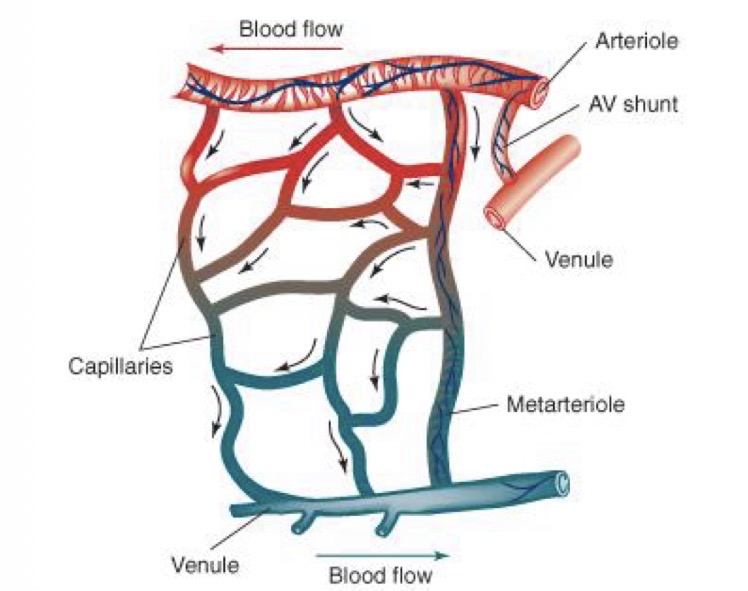
Microcirculation:
Exchange between blood and tissues through capillary walls
Venules and veins:
Collect blood and functions as a reservoir
Division of the circulation into more details (after the division into pulmonary system, systematic circulation and the heart):
Arteries → arterioles → capillaries → venules and veins
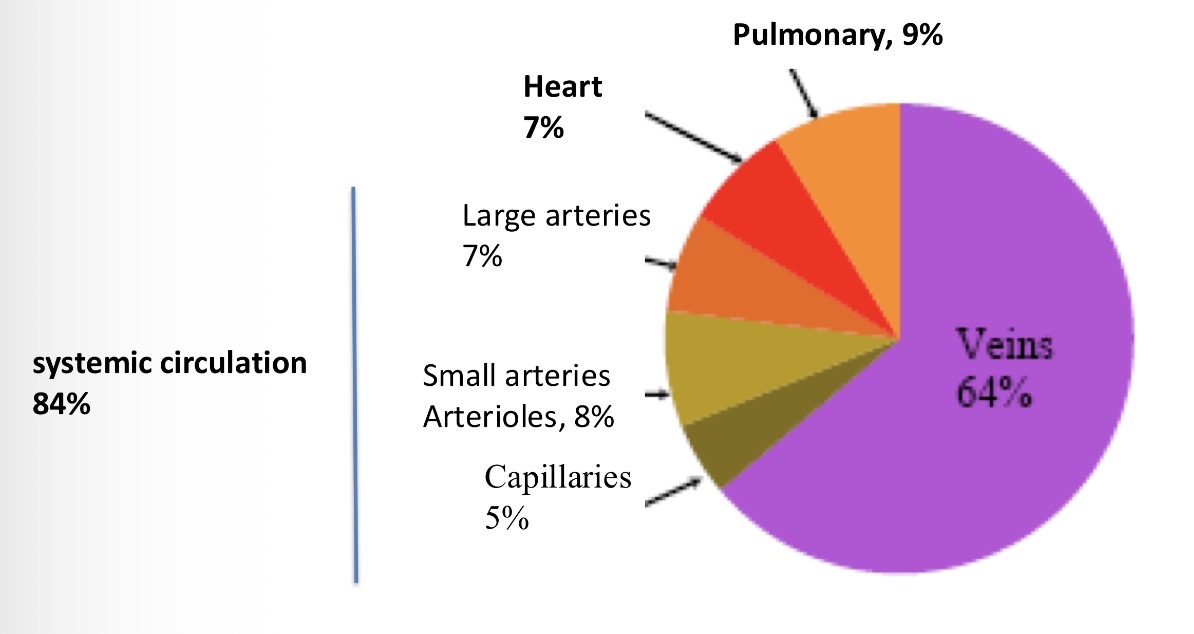
How is blood distributed in the system? the proportions in resting state
84% of blood in the systemic system, 7% in the heart and 9% in the pulmonary system
Size and structure of vessel walls: give the structures
Smooth muscle, fibrous tissue, elastic tissue, endothelium
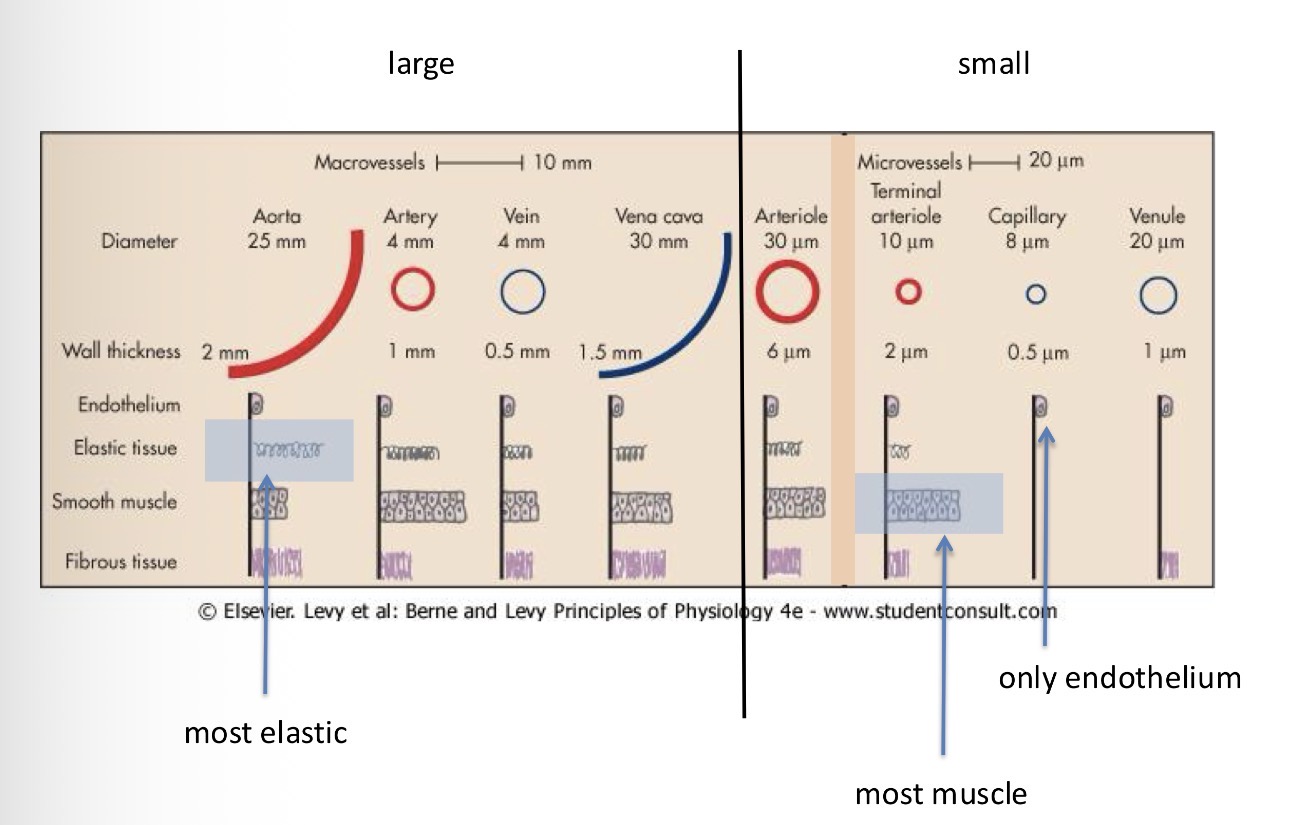
Which type of vessel is has the most elastic tissue?
The artery
Which type of vessel has the most muscle
Terminal arteriole
Which type of vessel is only made of endothelium?
Capillaries
Give me the thickness and diameter of macrovessels
Aorta - 25mm diameter, 2mm wall thickness
Artery - 4mm diameter, 1mm wall thickness
Vein - 4mm diameter, 0.5mm wall thickness
Vena cava - 30mm diameter, 1.5mm wall thickness
Arterioles 30 micro millimetre diameter and 6 micro millimetre wall thickness
Give me the diameter and wall thickness of microvessels:
Terminal Arteriole - 10 micro mil diameter and 2 micro millimetre wall wall thickness
Capillary - 8 micro mil diameter and 0.5 micro mil wall thickness
Venule - 20 micro mil diameter and 1 micro mil wall thickness
What are the blue and red colours in blood vessels?
red are oxygen rich (haemoglobin rich carrying oxygen) and blue are deoxygenated vessels
Where does the exchange of nutrients and gases happen?
In the micro circulatory/ capillary system
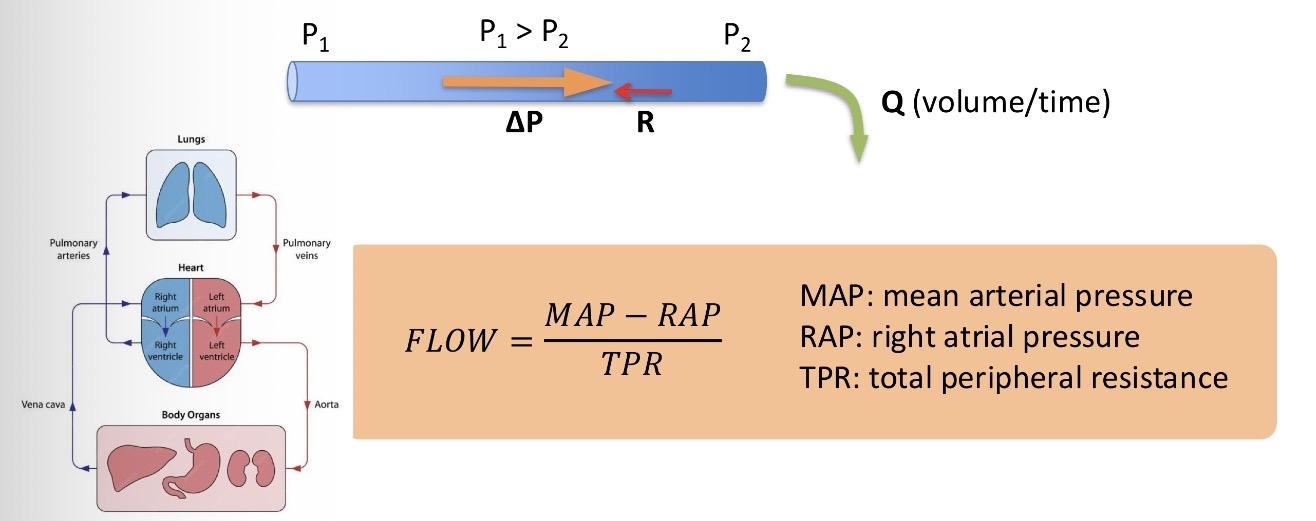
What are the physical determinants of the cardiovascular system?
Ohms law - flow Q, Pressure difference P and resistance R
Q=P/R
What is the name of the law talking about the flow of blood in the cardiovascular system?
Darcy’s law of flow
Is there a different way to calculate flow using arterial pressure etc.? And what is it?
Definition: a certain amount of blood getting through a certain spot in a certain amount of time
What is the ideal blood flow for the ideal human?
5L/min (usually viewed as a 72kg male)
What is the cardiac output?
The volume of blood the heart pumps out in a minute
How does the flow actually go through the vessels?
Most cases: small vessels
Laminar flow - different layers of blood that flow in parallel but in different speed (the centre of the vessel are faster and the periphery is slower because of the contact with the wall = more resistance)
large vessels:
turbulent flow - less efficient flow, because the blood added into the veins is put in bits = this results in heart sounds and murmurs
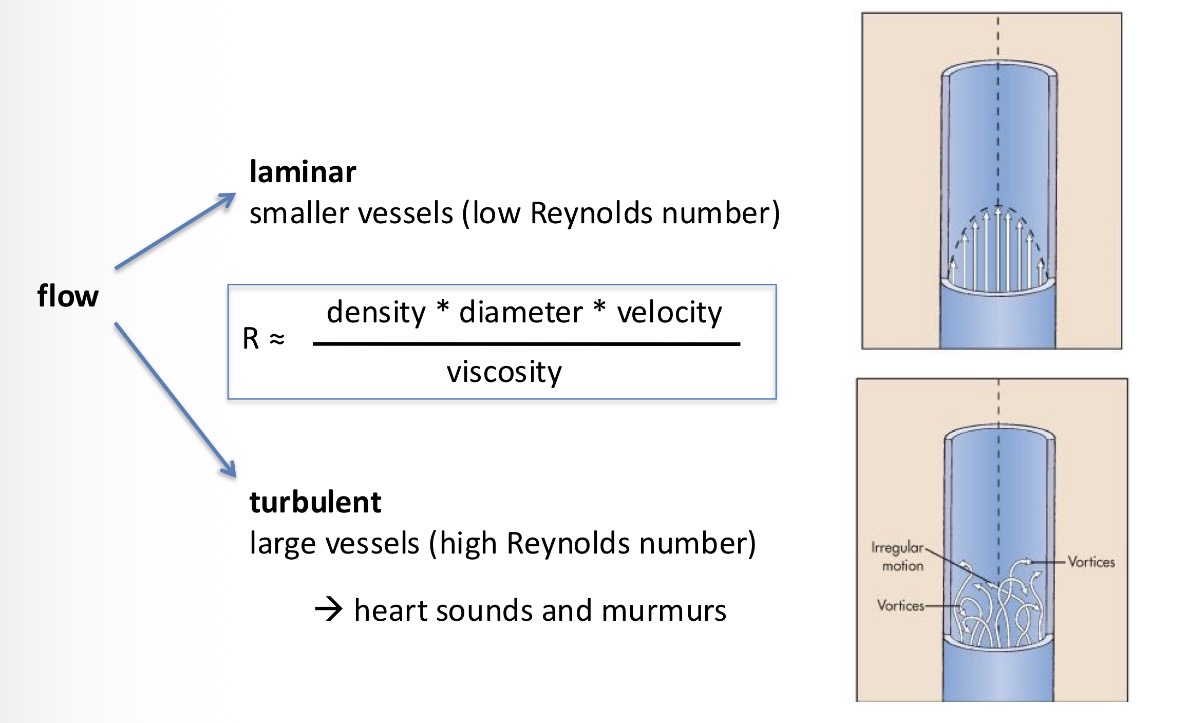
What flow is responsible for heart sounds?
Turbulent flow of large vessels
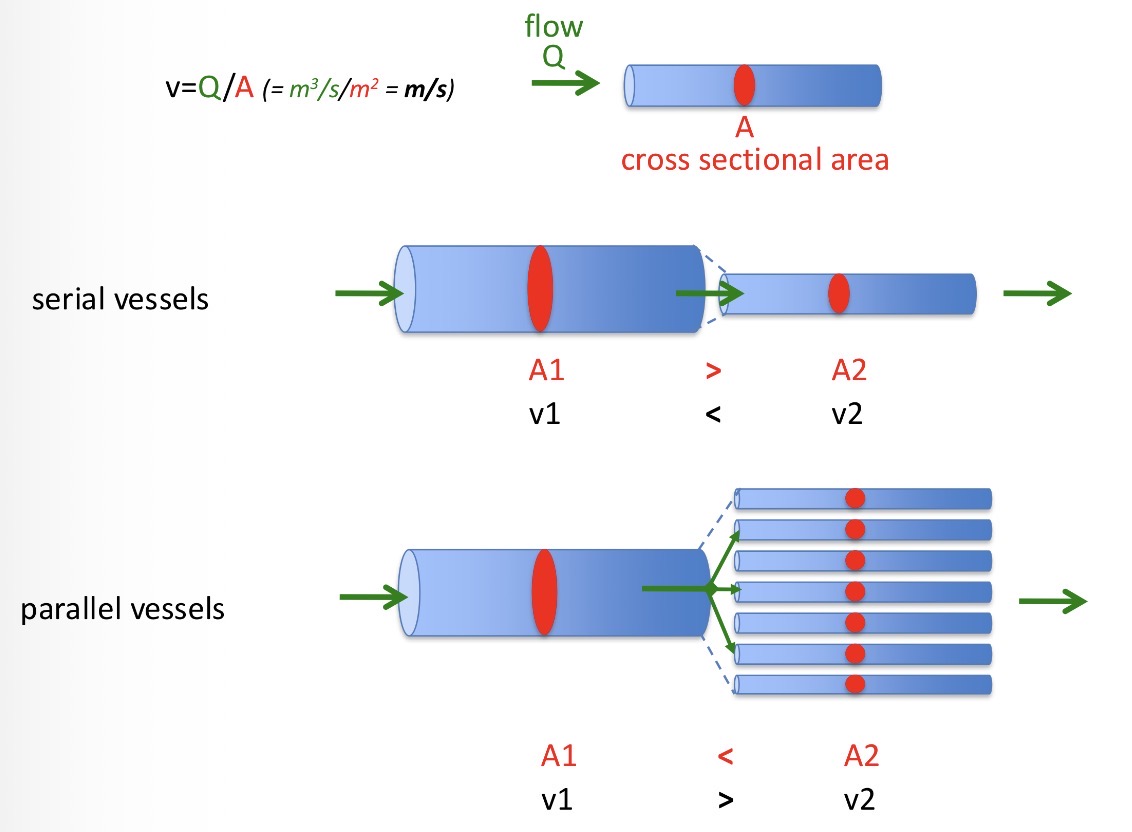
How do we measure the velocity of the blood and what is it made of?
Determined by the cross section of the vessel and the flow strength.
V=Q/A
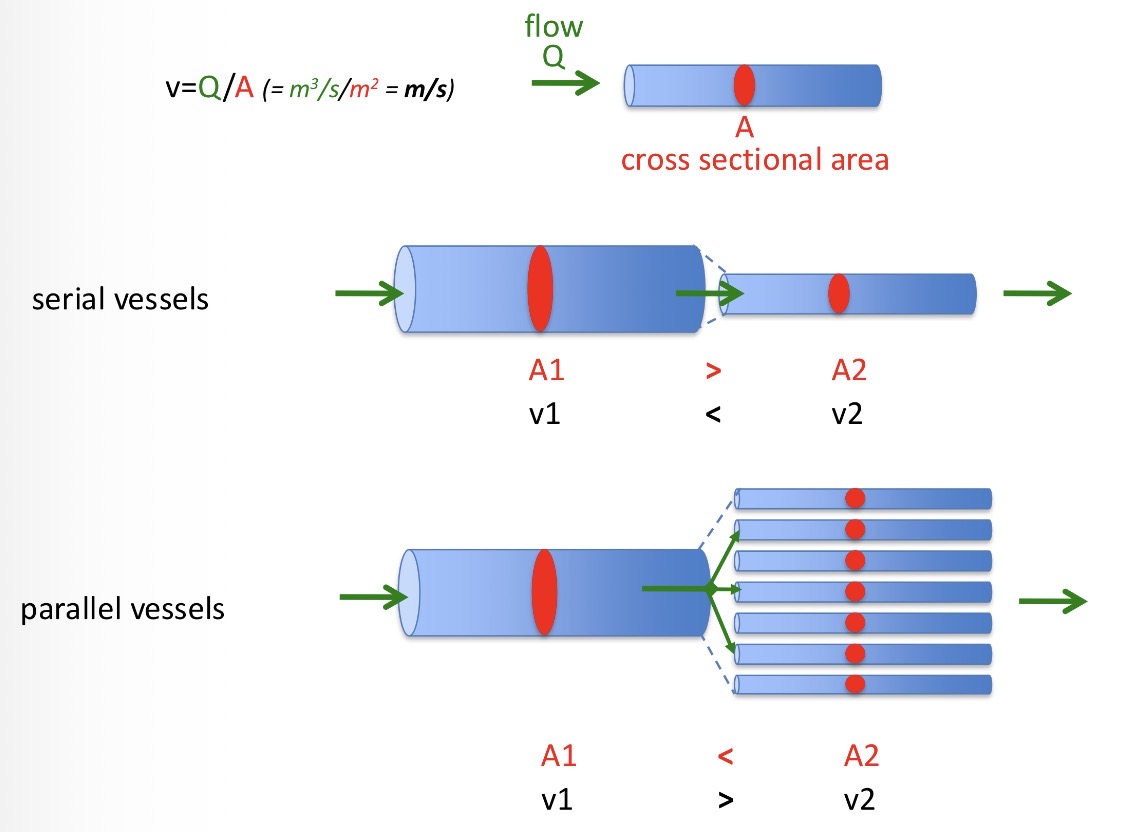
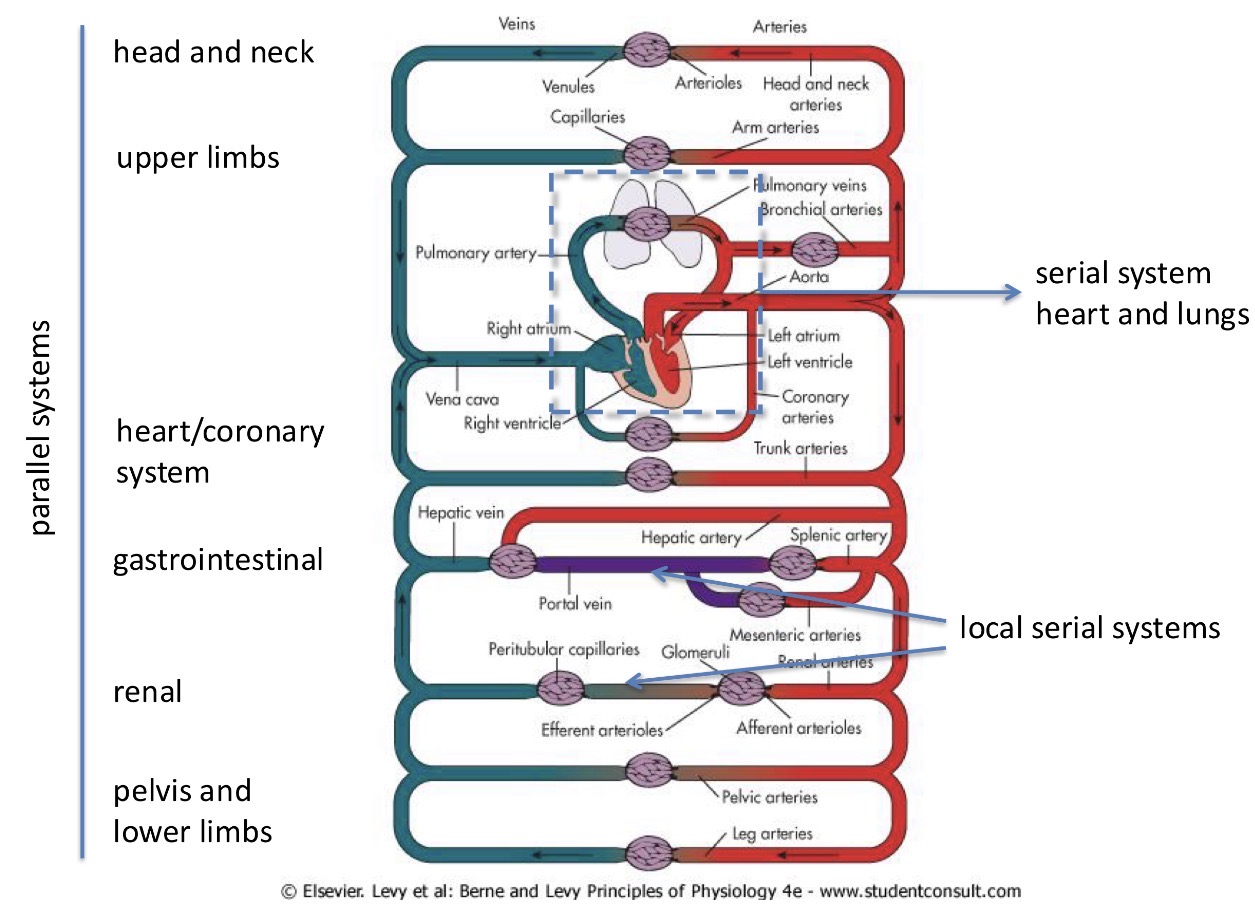
How can vessels be connected?
Serially - slower flow
Parallel vessels- during branching, blood flow usually slows down
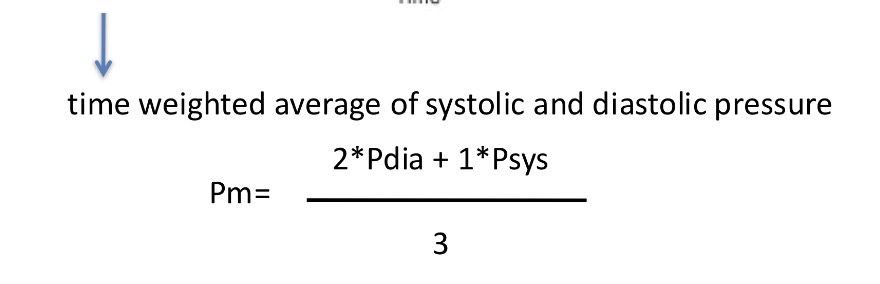
What is the distribution of velocity in the circulatory system?
fast - aorta, large arteries, small arteries, small veins, larger veins, vena cava
Slow - arterioles, capillaries, veins
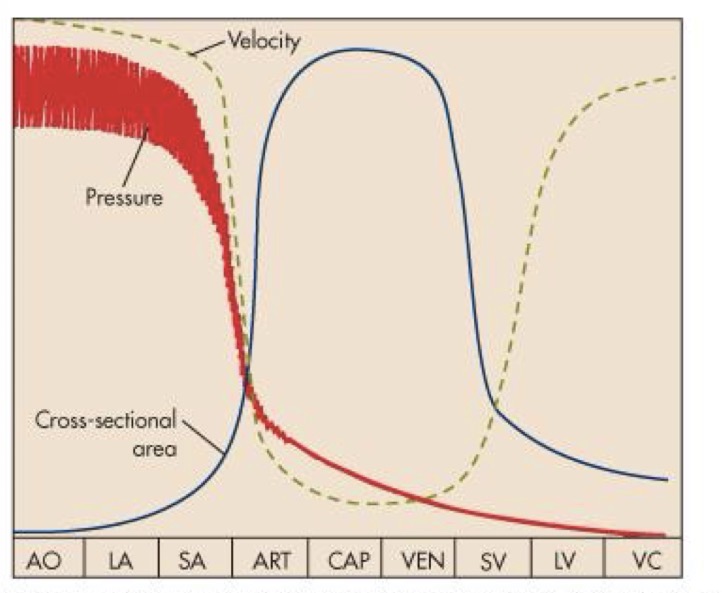
Why does the velocity slow down at the capillaries?
To promote the exchange of nutrients and gases in the blood
Determinants of flow:
Viscosity - physical property of fluids, depends on its density and particle size
Higher density means lower flow
What is viscosity determines by
The hematocrit ratio
Hematocrit = erythrocyte volume/ whole blood volume
When does the viscosity of blood decrease and increase? (What diseases)
Anemia - decrease in number of erythrocytes → decrease in viscosity which increases blood flow
Polycythemia - increase in erythrocyte level → increase in viscosity and decrease in blood flow
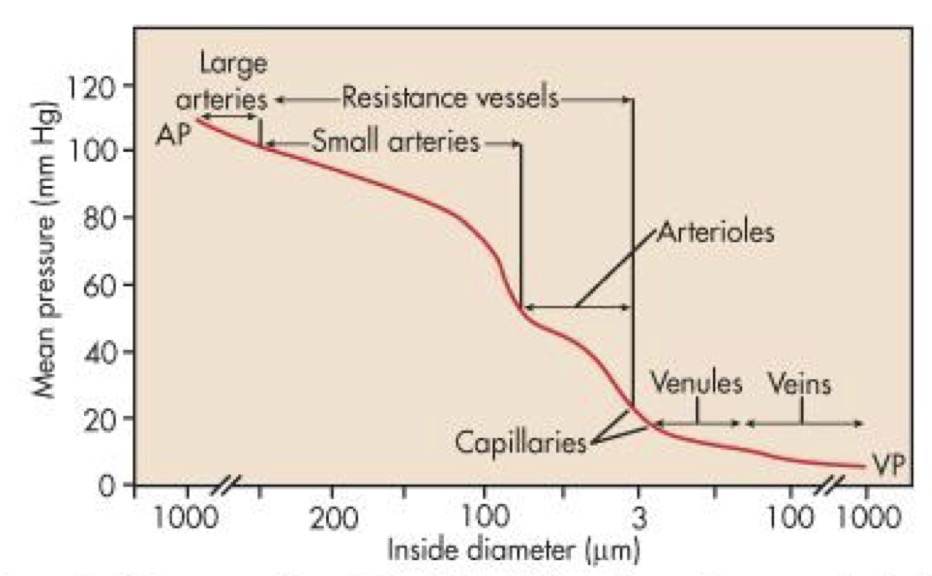
Blood pressure is the potential that makes blood move. Where is the most blood pressure and the least blood pressure?
Sharpest drop in arterioles and they determine the whole pressure of the system by having different diameters
What is the top of the pressure curve called and what happens to the heart?
Systolic pressure - the heart contracts
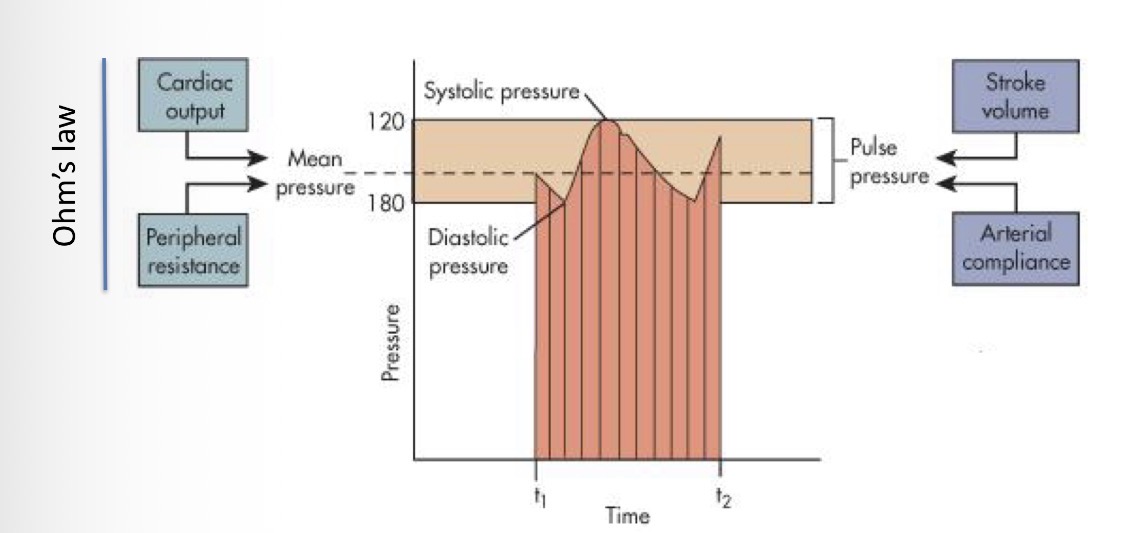
What is the bottom of the pressure curve called and what happens to the heart?
Diastolic pressure - relaxation of the heart
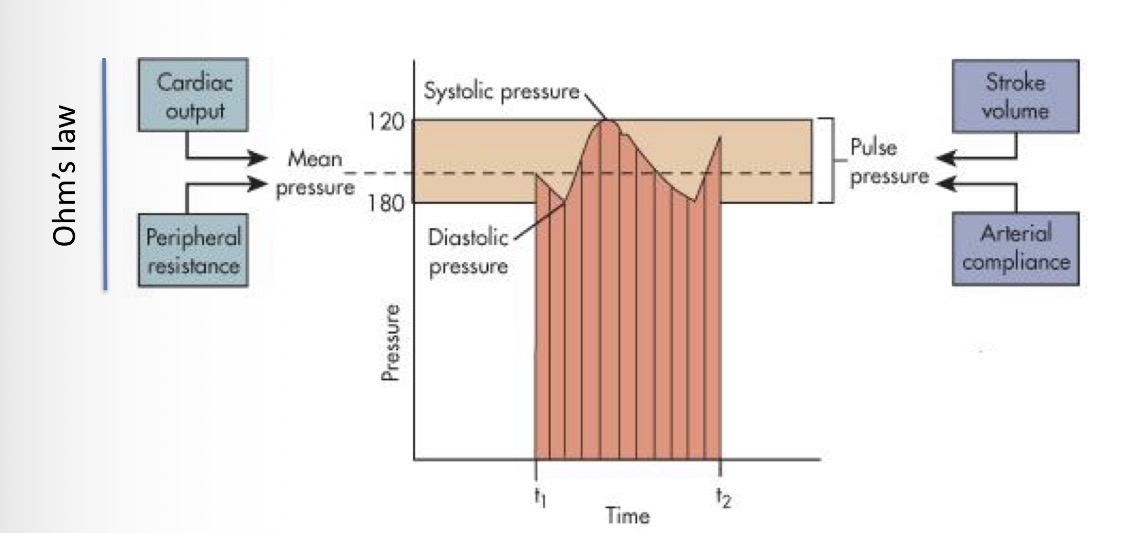
How do you get pulse pressure?
Difference between diastolic and systolic pressure
How do you calculate mean pressure?
Pdia - diastolic pressure , Psys - systolic pressure
Look at the distribution in the cardiovascular system and explain it
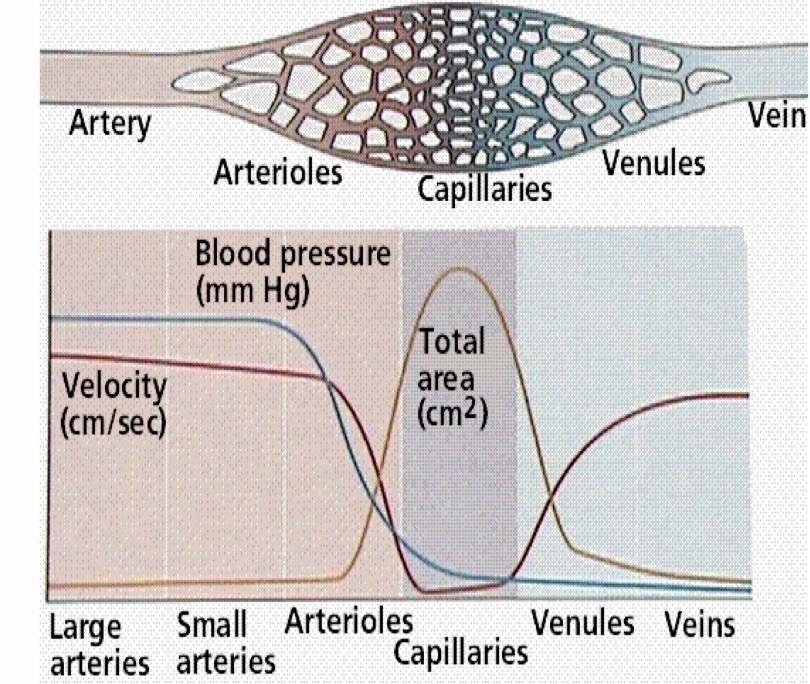
How do we measure arterial pressure
1 - probe into the vessel but that is a procedure you cannot do routinely
2 - method with the cuff - pump up the cuff with pressure that is higher than systolic pressure (more than 120) → no flow from the artery because it is blocked → gradual decrease of pressure in the cuff and during the tip of the pause when the pressure is at its highest, the flow returns to the arm and since the Diameter is slow and the pressure in those veins is high, SOUND IS GENERATED - Korotkoff sounds → as we further reduce the pressure that ensures continuous flow through the vessel = reached diastolic pressure
Tip of the pause → pressure is higher than max systolic pressure
When the flow turns smooth → the pressure reaches under diastolic pressure for a second
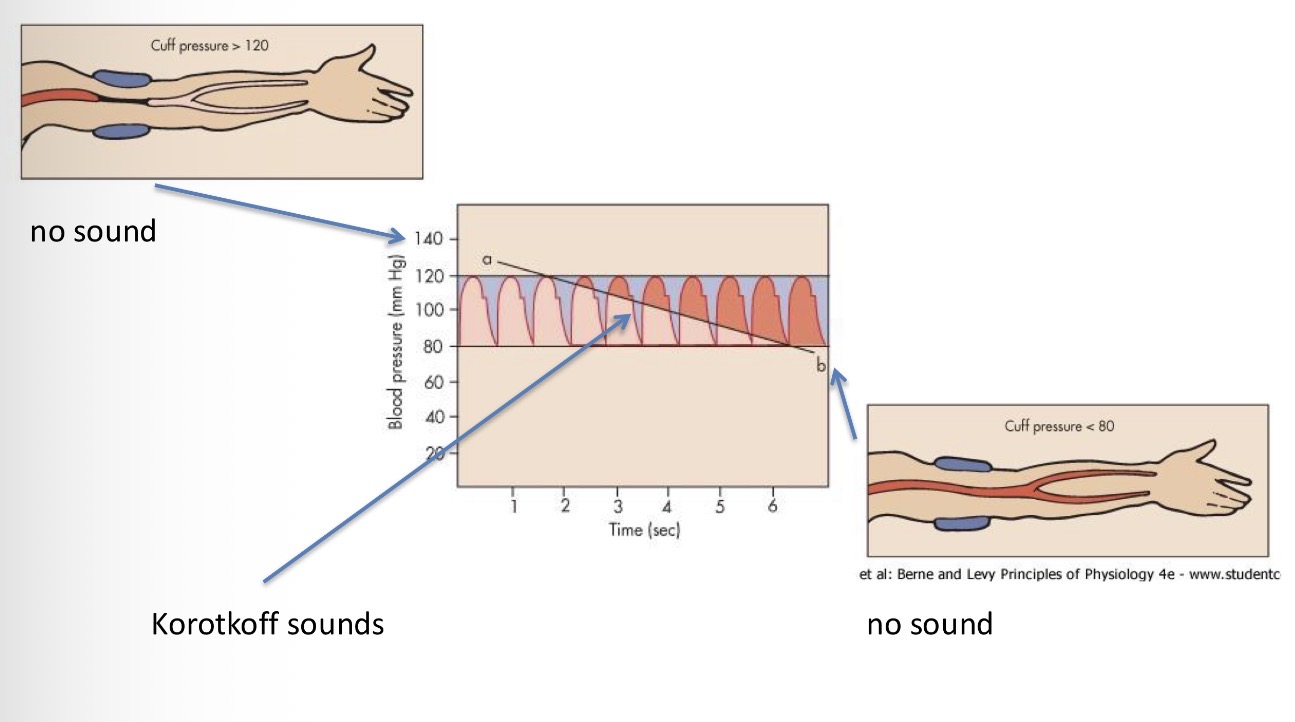
Explain this image
method with the cuff - pump up the cuff with pressure that is higher than systolic pressure (more than 120) → no flow from the artery because it is blocked → gradual decrease of pressure in the cuff and during the tip of the pause when the pressure is at its highest, the flow returns to the arm and since the Diameter is slow and the pressure in those veins is high, SOUND IS GENERATED - Korotkoff sounds → as we further reduce the pressure that ensures continuous flow through the vessel = reached diastolic pressure
Tip of the pause → pressure is higher than max systolic pressure
When the flow turns smooth → the pressure reaches under diastolic pressure for a second
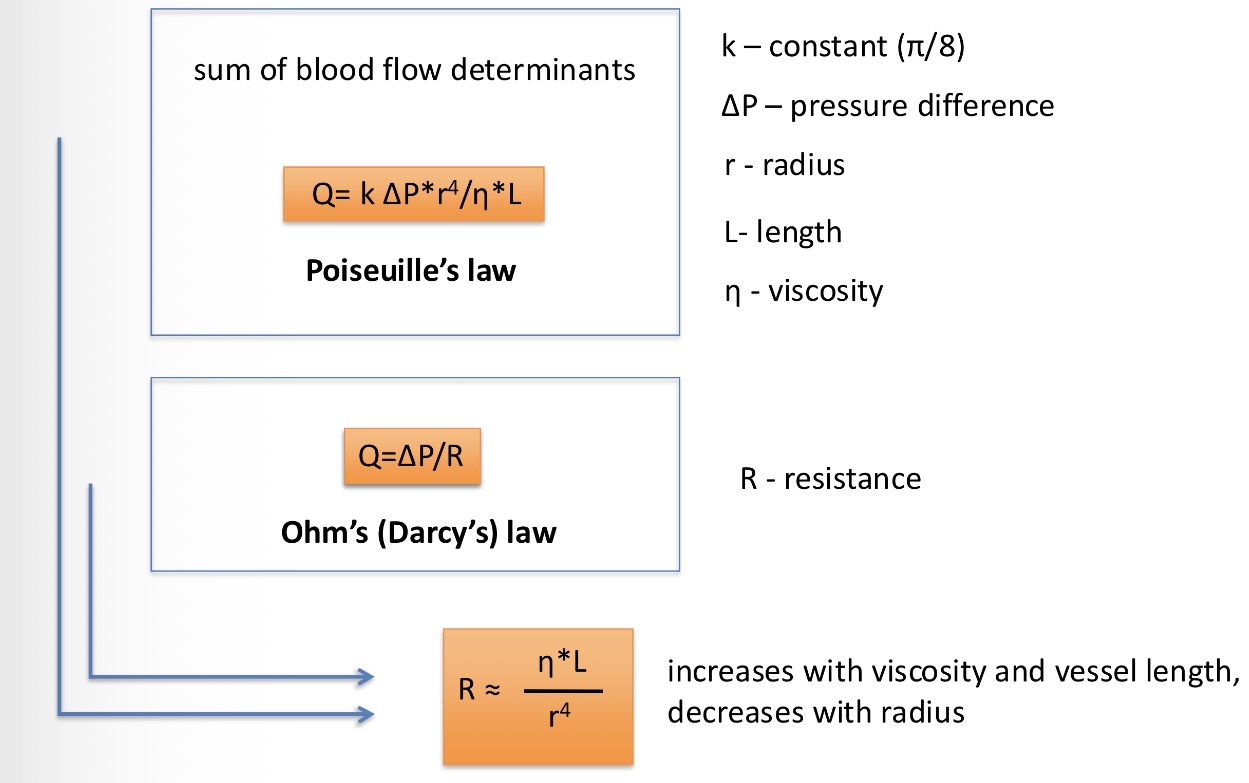
poiseulles law - determinants of blood flow = definition of resistance. Give me all three necessary equations
What is the total peripheral resistance?
Mean arterial pressure = cardiac output * total peripheral resistance (serial and parallel vessels sum)
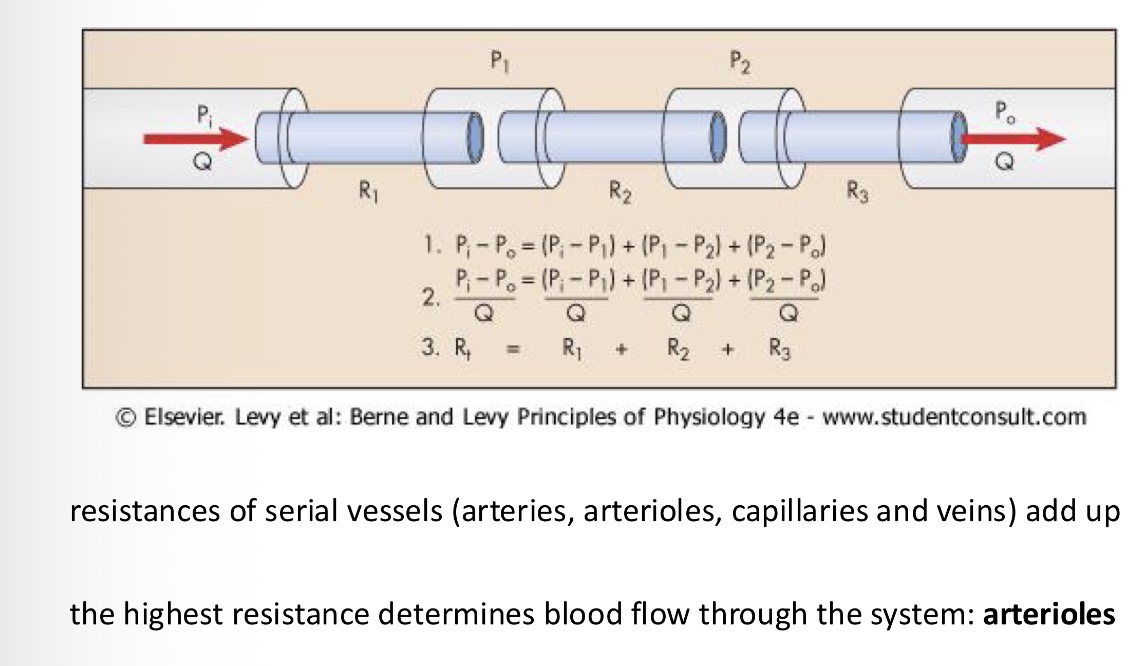
Which type of vessels has the highest resistance?
Arterioles
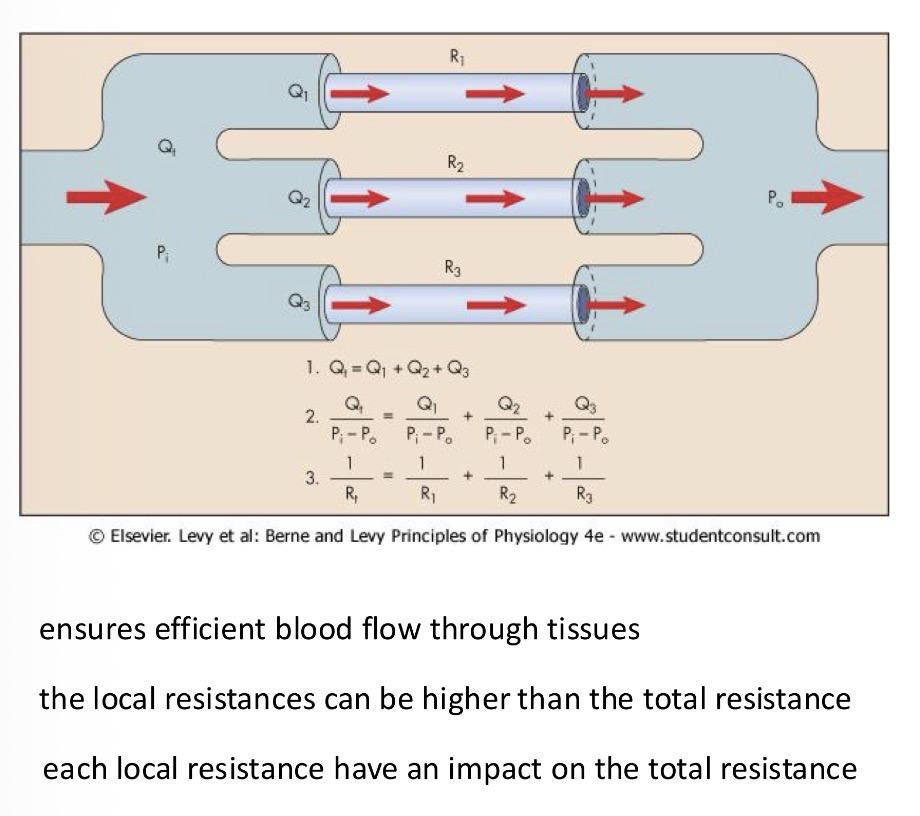
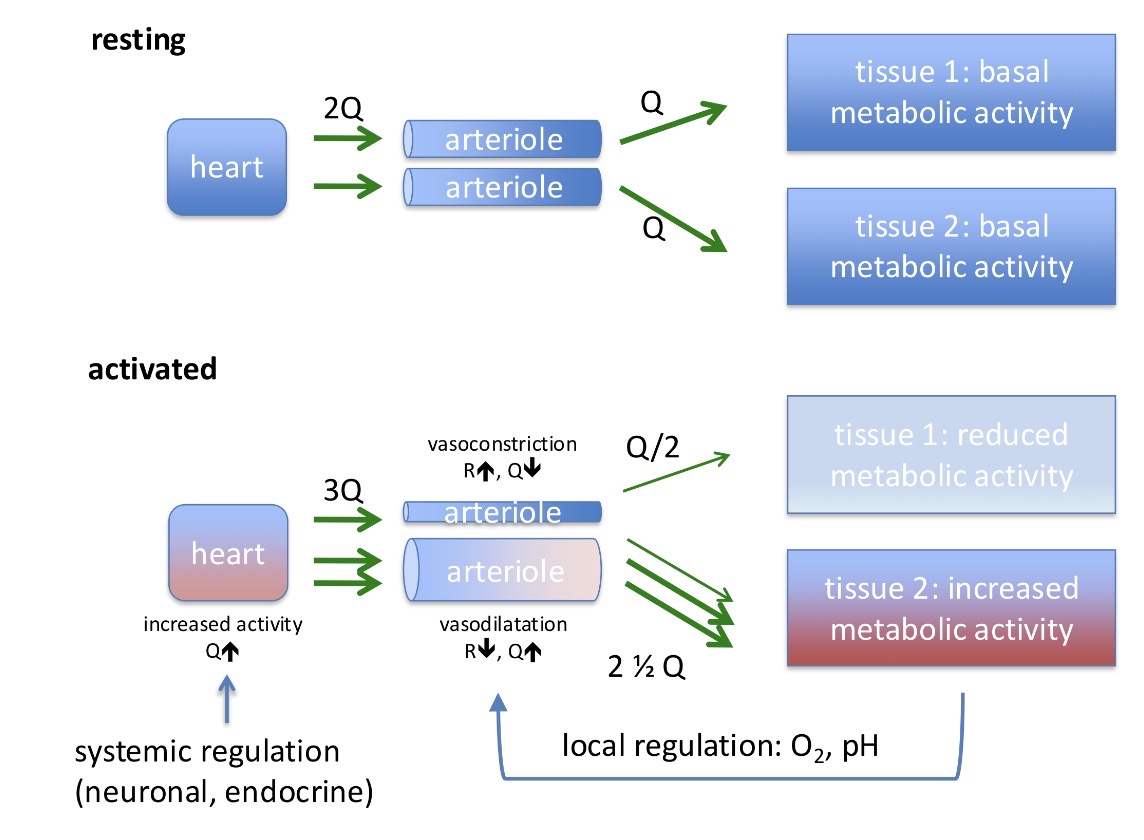
Can local resistances be regulated separately?
Yes, each organ can have its own system regulating the blood flow there
Relationship between resistance and radius:
Inversely proportional
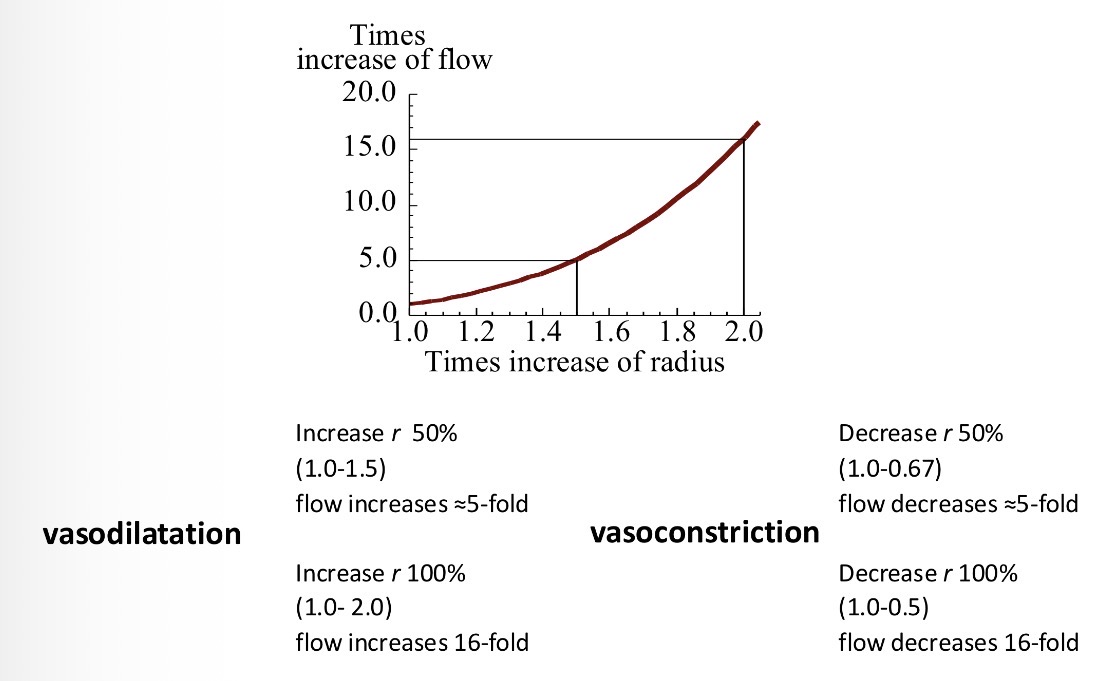
What is vasodilation and vasocontstriciton
Vasodilation - increase in diameter of a vessel
Vasoconstriction - decrease in diameter of a vessel
What are the physical determinants of micro circulation?
Hydrostatic pressure
Net filtration = hydrostatic pressure - oncotic pressure
Filtrated fluid = reabsorbed fluid + lymph
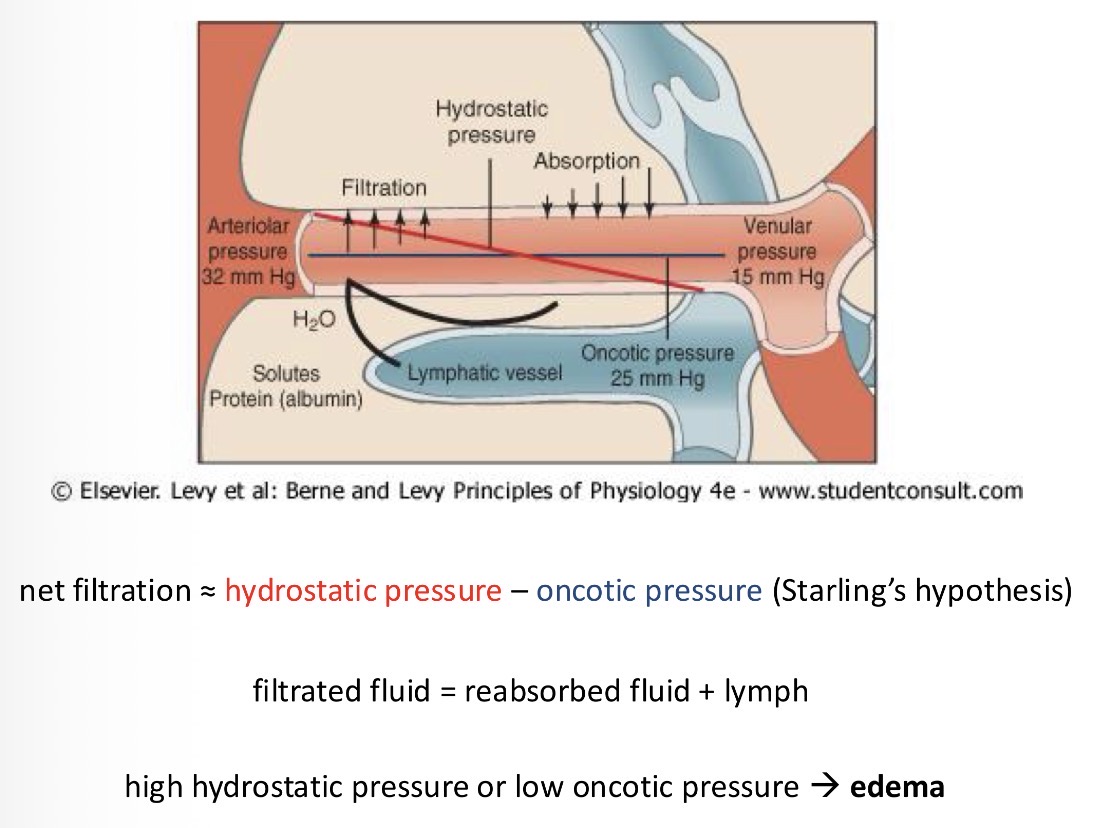
Where does all the liquid that is not reabsorbed into the capillaries go?
The lymphatic system takes it away
Why do we need to regulate circulation?
Adapt to the physical activity of the whole organism
Controlled parameters:
tissue blood flow
Cardiac output
Arterial blood pressure
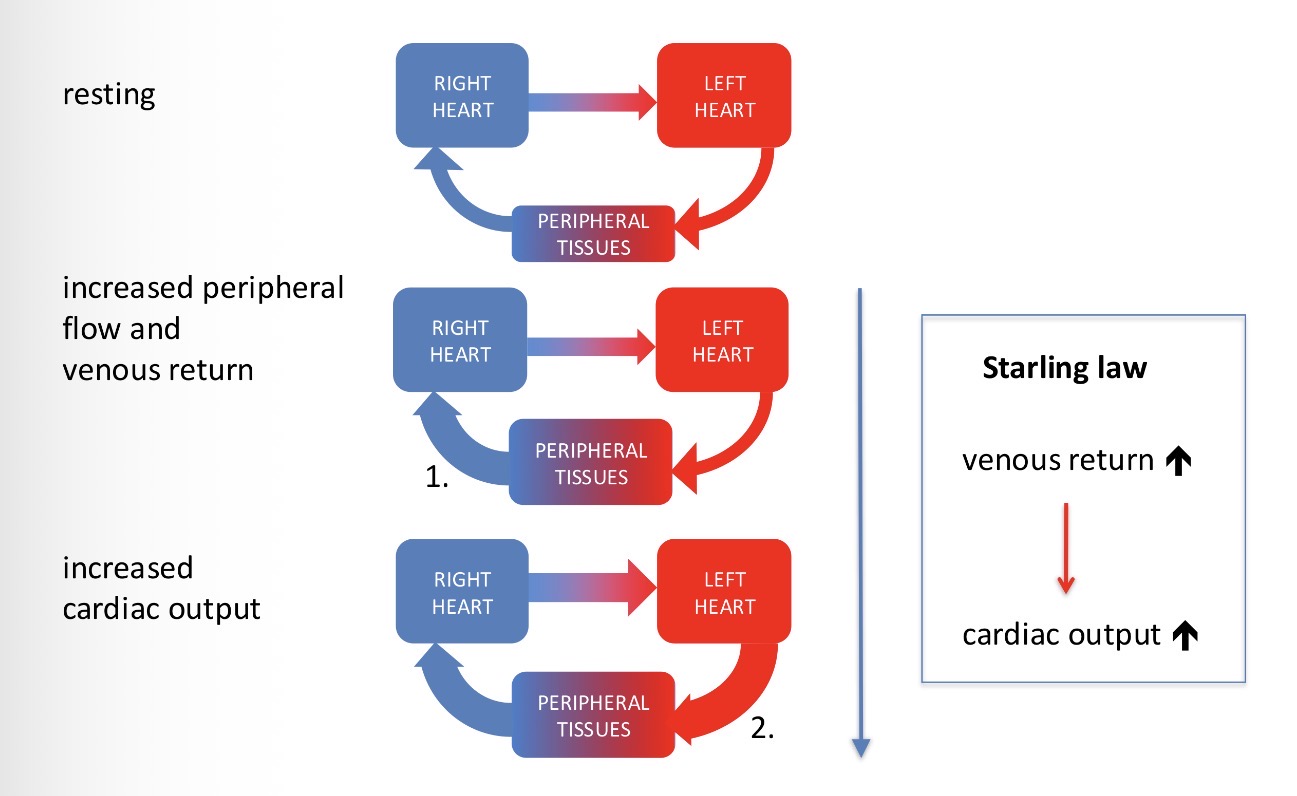
How is the cardiac output controlled? And what is the law called?
Controlled by the sum of local tissue flows. Starling Law
Explain what’s going on in this image
how does the electrical signal travel through the heart?
Sinoatrial node → Atrioventricular node → crosses the border of the atria and the ventricles using via the Bundle of His into the septum between the ventricles → terminally branches into small fibres called purkinje fibres
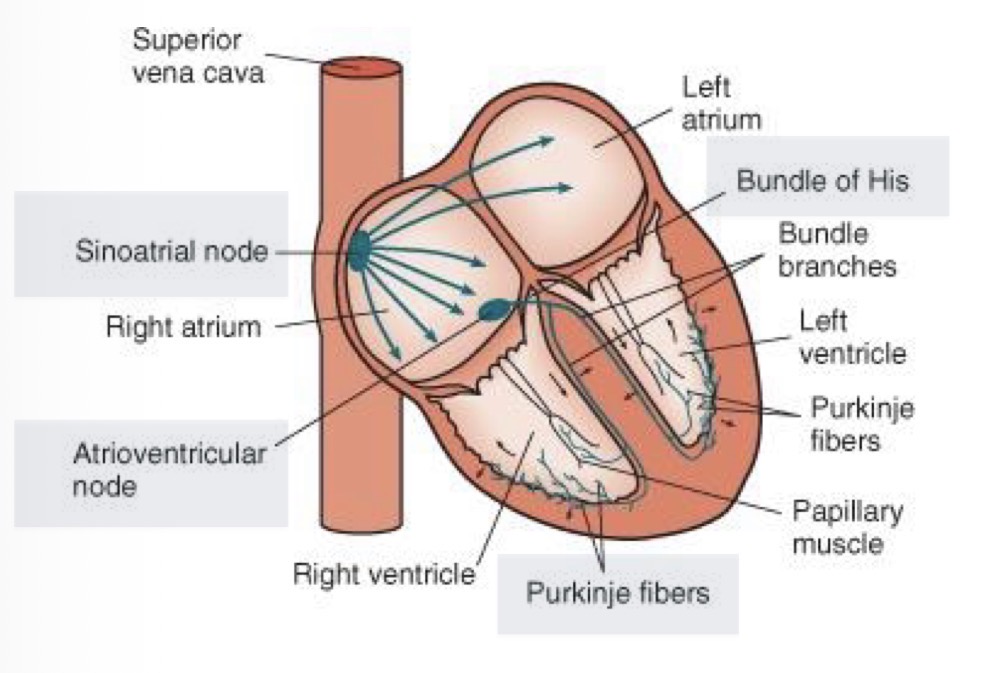
How does an electrical signal start?
The sinoatrial node (SA node) spontaneously depolarizes
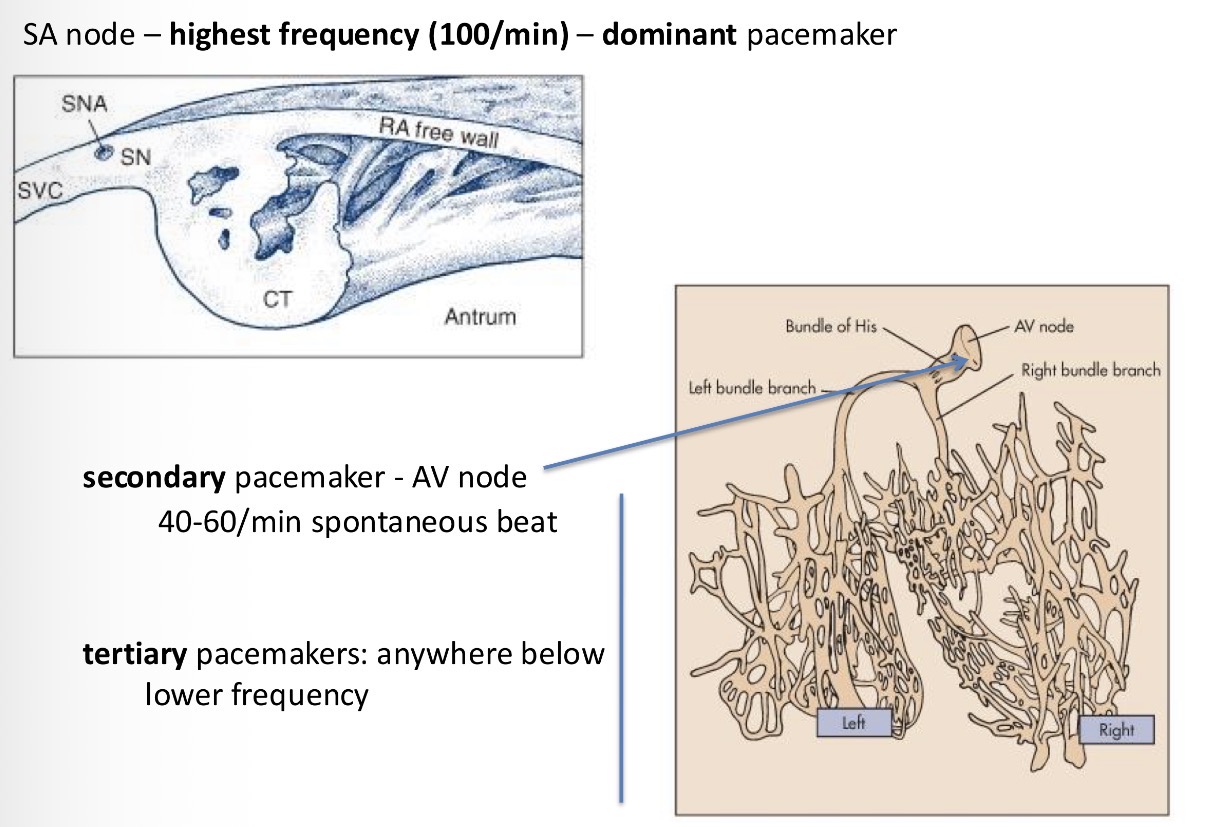
What is the dominant pacemaker and what is its frequency?
SA node. Frequency of 100/min.
It always starts at the SA node because it is able to generate a signal at the highest frequency
What are other pacemakers and their frequency?
Secondary pacemakers - AV node 40-60/min
Tertiary pacemakers - anywhere at lower frequency
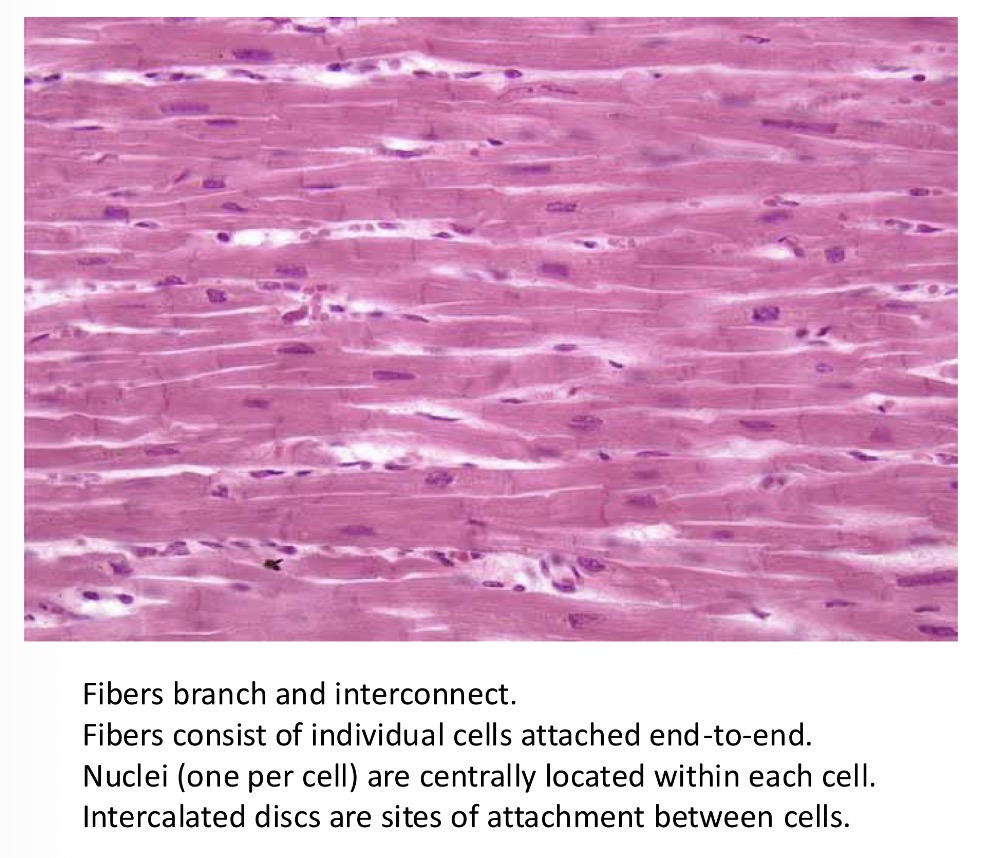
What is syntitium? And what is it made out of?
A unit structure of muscle that can propagate electric activity
Do isolated cardiac myocytes keep on beating when cut off?
Yes (using Ca2+)
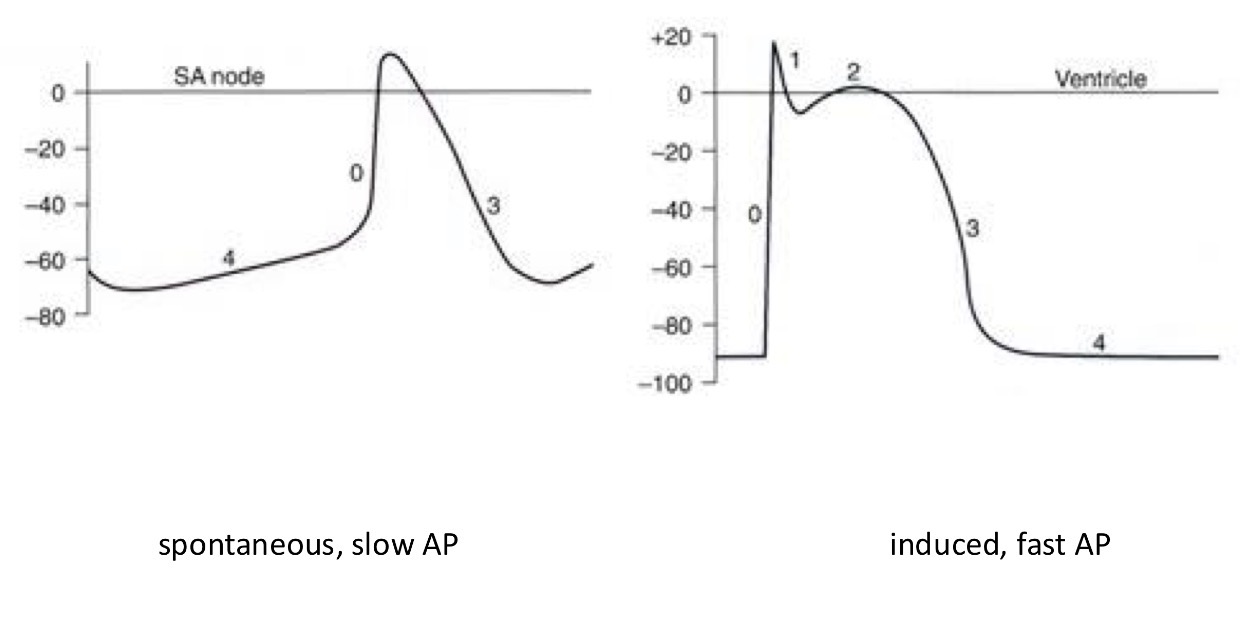
Try drawing action potentials of different sections of the heart: Which ones start the earliest? Which ones look similar? Where are they similar?
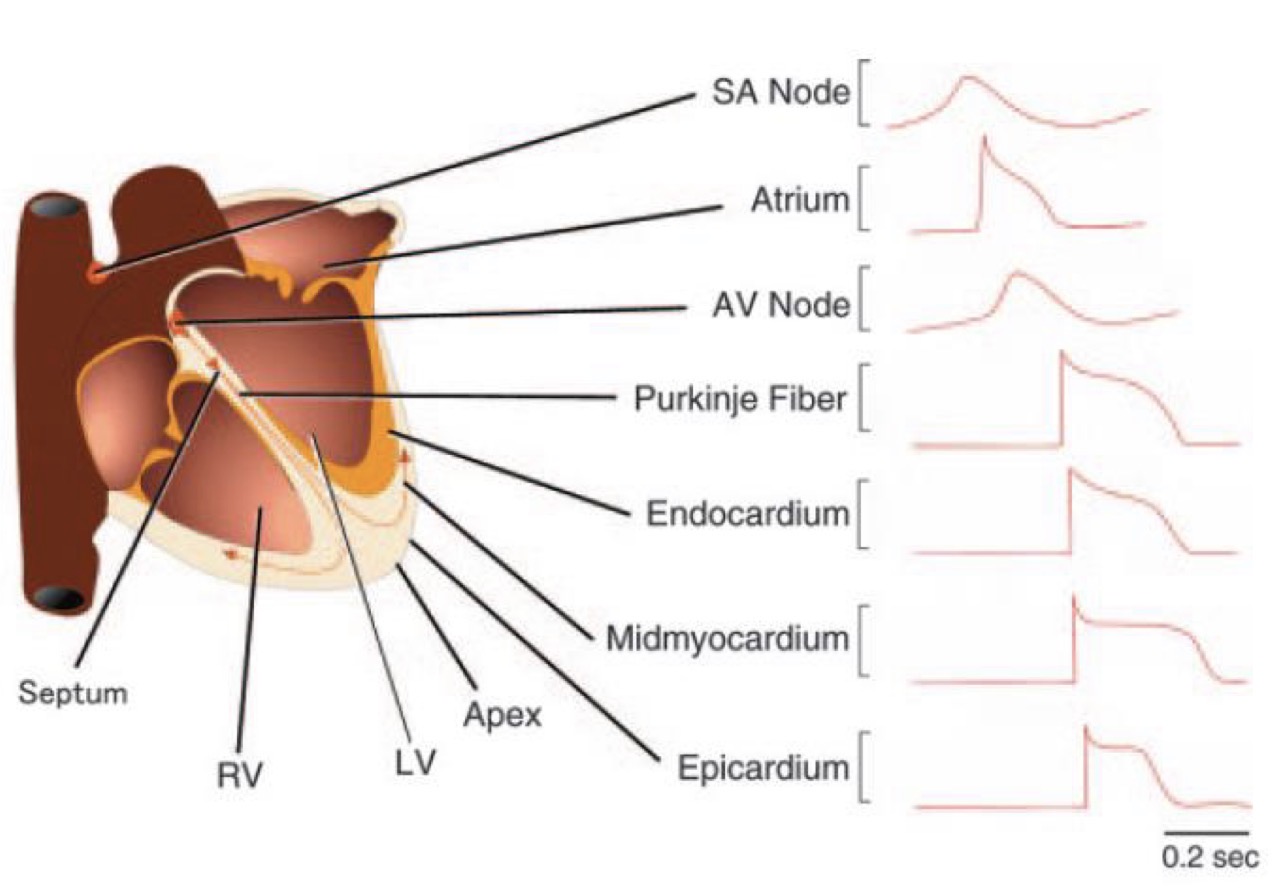
Which two types of AP exist in the heart and which sections of the heart/ which pacemakers go into each category?
Spontaneous slow AP - SA node, AV node = dominant and secondary pacemakers
Induced fast AP - everything else = all the other pacemakers
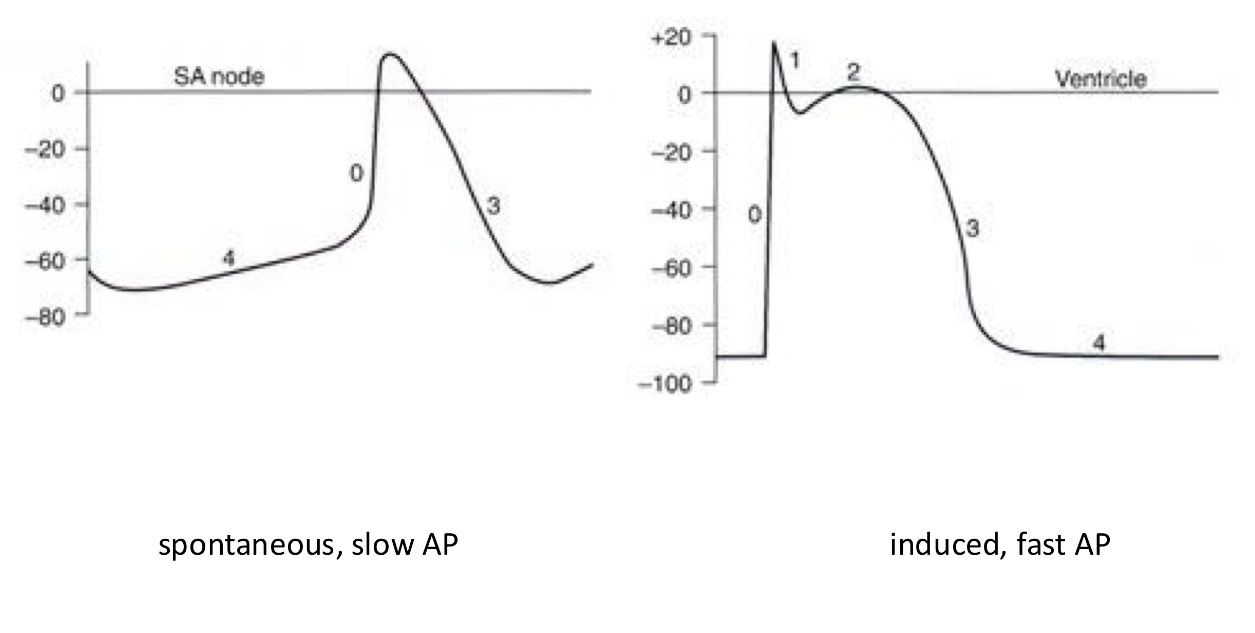
What are the shared phases of APs in the heart?
0 - fast depolarisation → in both APs
1 - small repolarisation → induced AP only
2 - plateau → in induced AP only
3 - repolarization → in both APs
4 - resting membrane potential (not stable in the SA node) → in both APs
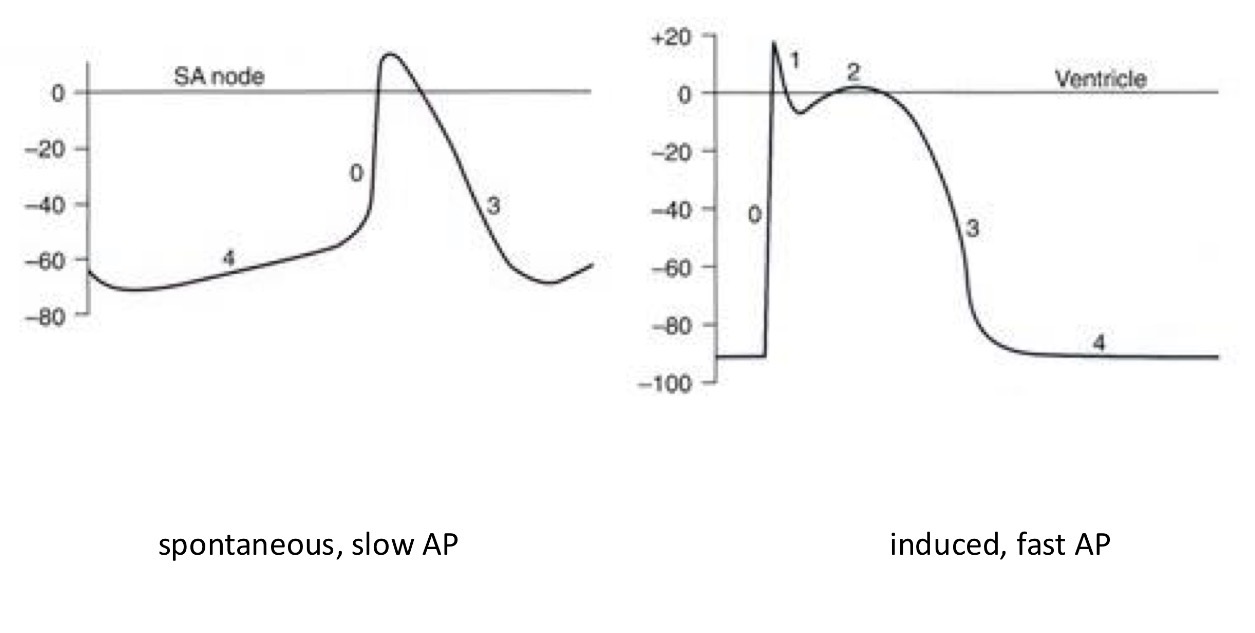
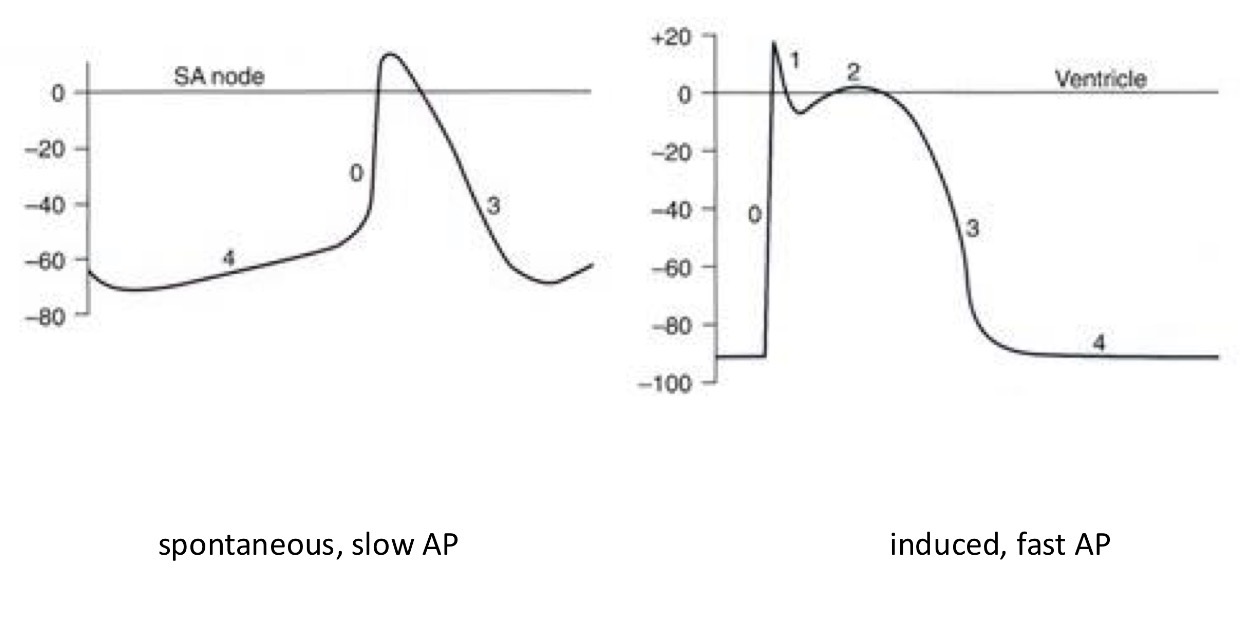
Explain what’s happening in both pictures
0 - fast depolarisation → in both APs
1 - small repolarisation → induced AP only
2 - plateau → in induced AP only
3 - repolarization → in both APs
4 - resting membrane potential (not stable in the SA node) → in both APs
What is thee biggest difference between the APs?
The resting membrane potential is much more negative and flat in the ventricle but in the SA the moment it reaches the lowest point it slowly gets back into a slope going up hill = spontaneously depolarizing
Which ions have and influx in depolarization and repolarization?
Depolarization - sodium or calcium
Repolarization - potassium
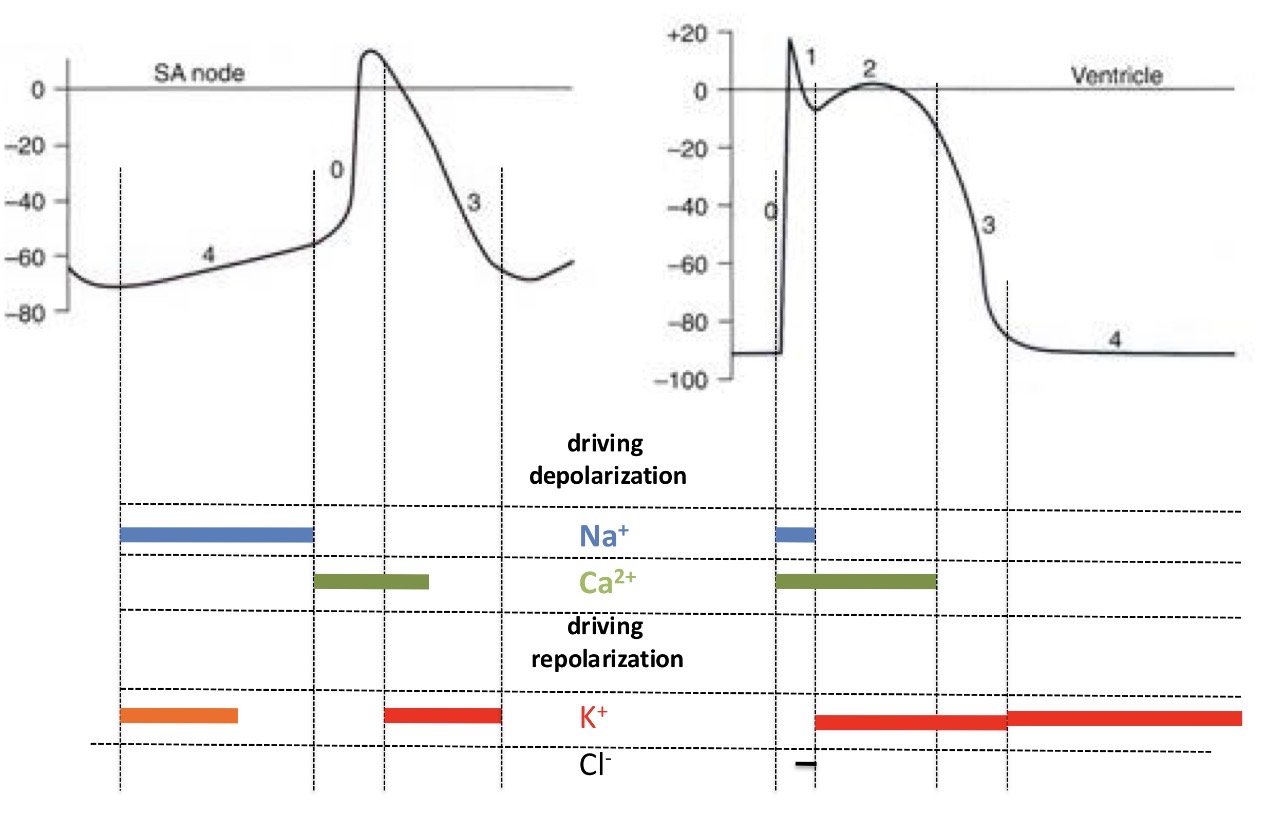
Which channels are behind the fluxes of ions during electrical signals of the heart?
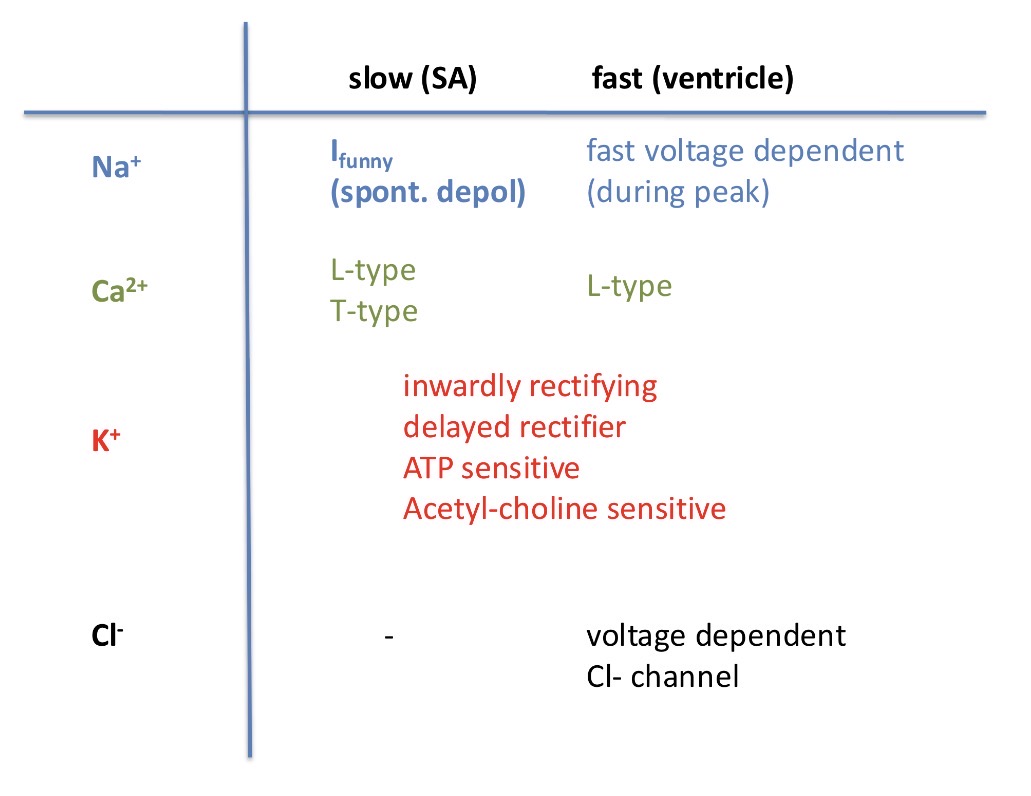
Where are fast voltage channels present?
Only in ventricles
What is the significance of a spontaneous depolarization?
It triggers the excitatory wave of the heart
The SA node is the main pacemaker so it controls the frequency. What is the change in frequency called in the sympathetic and parasympathetic system?
Tachycardia (symp) = higher frequency
Bradycardia (para) = lower frequency
What’s another way to achieve the same effect where the AP in the SA node changes?
Change of threshold potential (higher frequency if changed up)
OR
Hyperpolarize the cell so that the resting potential is more negative and it takes longer for a cell to reach the resting potentitial (lower frequency)
What is the significance of ventricular action potentials?
The goal for spontaneous APs is to travel down and trigger ventricular cells = trigger contractions and push the blood out into the system
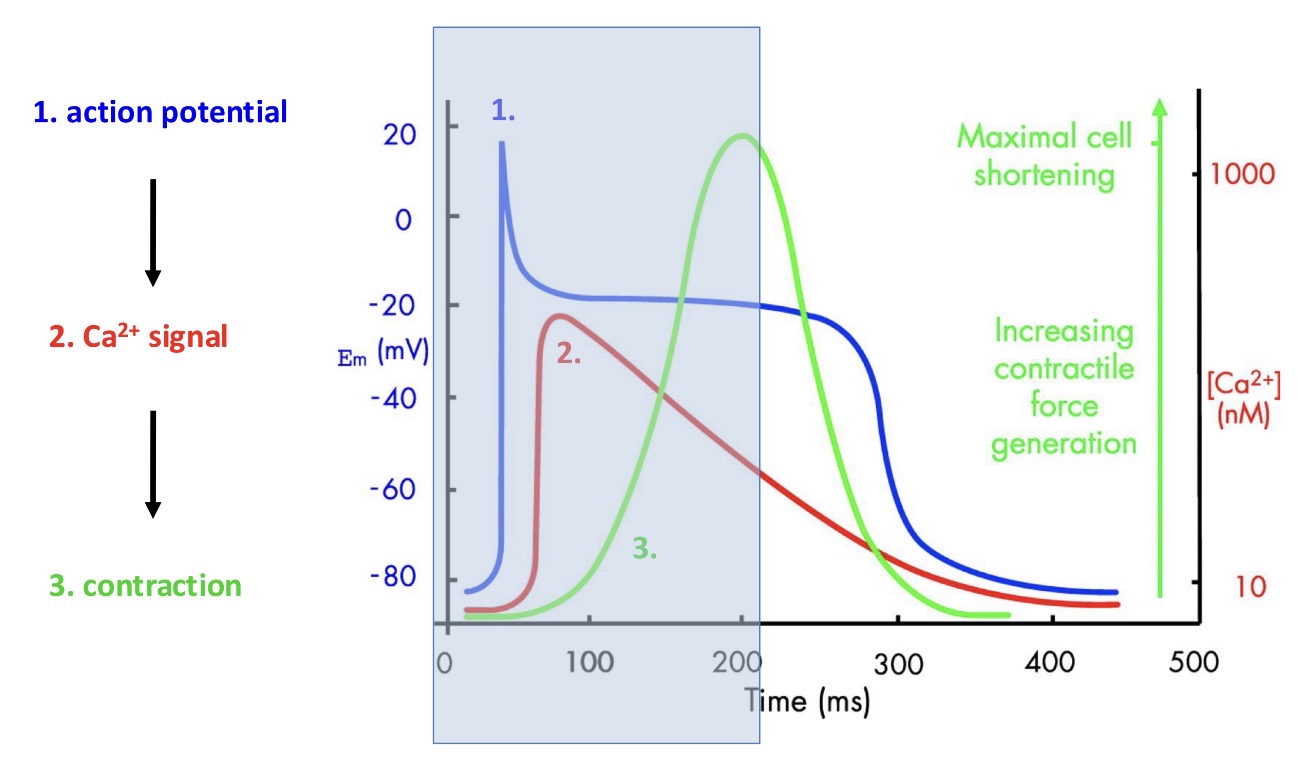
Explain what happens here:
1 - electrical activity of the myocyde
And in response to the AP there is a calcium signal generated
2 - calcium signal generated
And in response to the calcium signal contraction is generated
3 - contraction
then the resting phase starts (the part outside the blue box) = equally as important
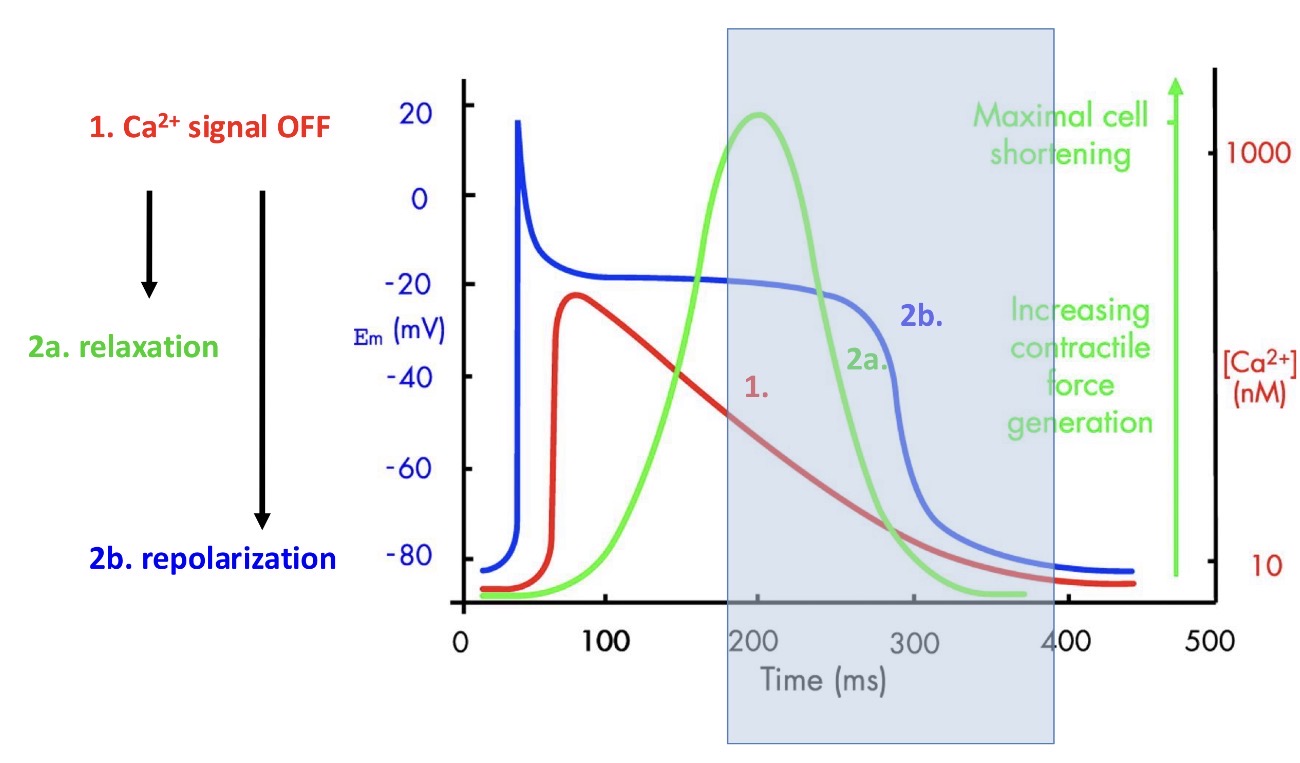
What happens here:
1 - calcium signal turns off (trigger)
2 - this triggers muscle relaxation and repolarizes the cell
Contraction finishes before the action potential finishes
The heart has to work rhythmically and thus it has to relax. To ensure that there is no titanic activity what does the heart do?
Ensured by refractory period!!! - no further AP cannot be generated because the channels are inactive
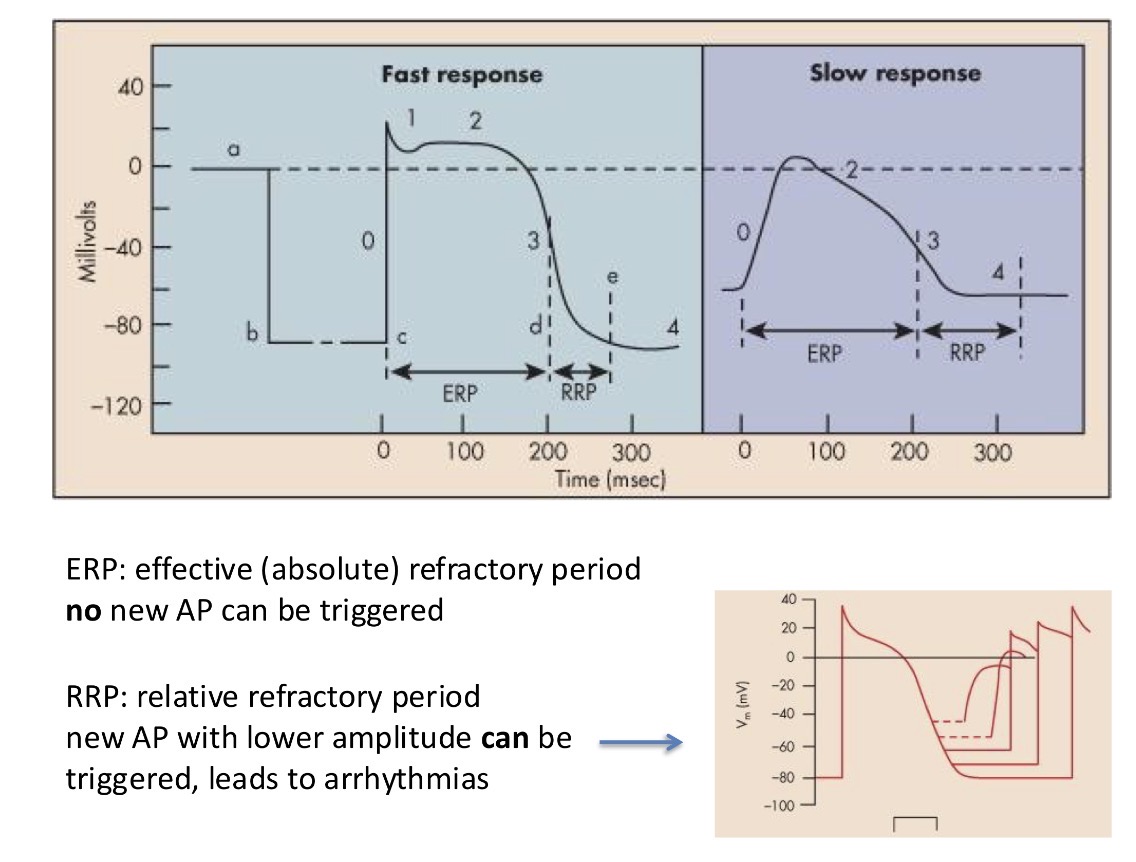
What is the relative refractory period?
New AP with lower amplitude can be triggered and it leads to arrhythmias (= an event where the heart beats too fast, too slow or irregularly)
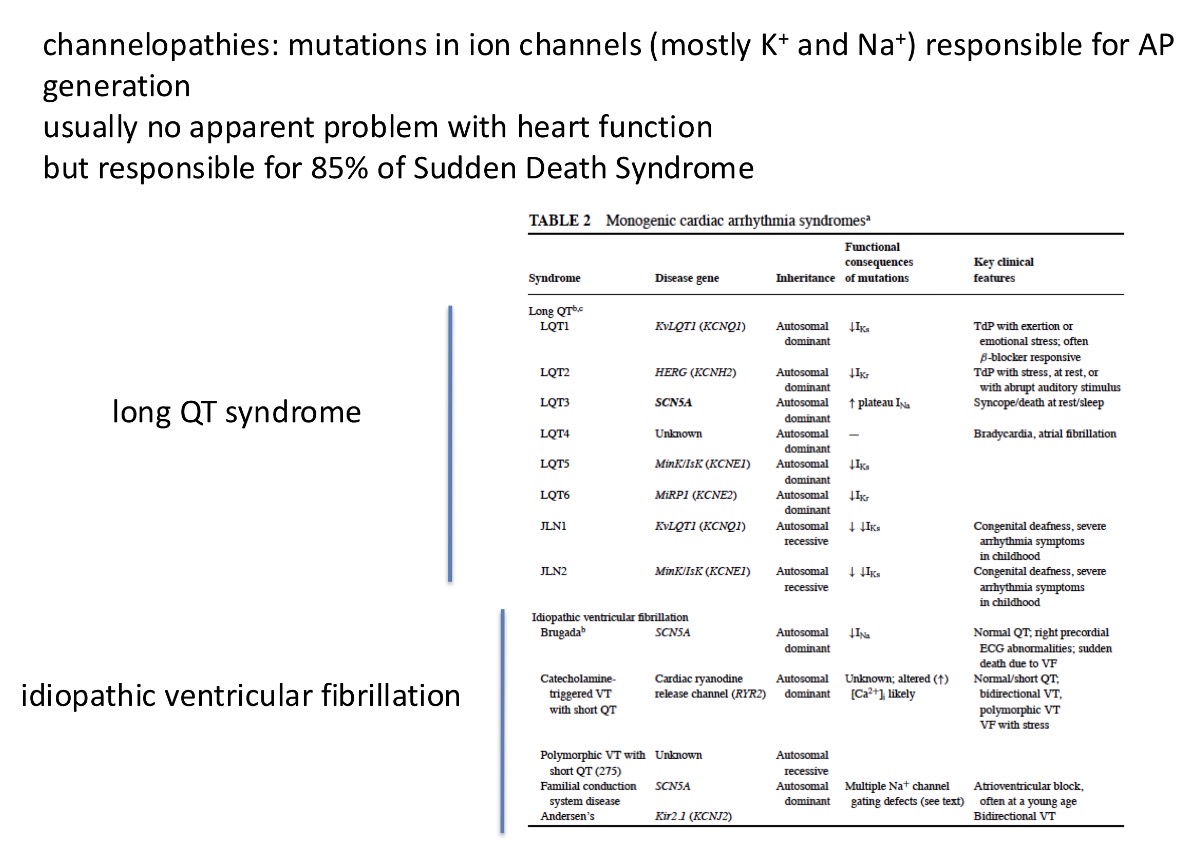
Why is it important to know the ion channels? Give 2 reasons
Mutations in ion channels can occur and they are responsible for 85% of sudden death syndrome (a young sports person doing hard exercise and then spontaneously dying)
The channels are usually targets for medicine to fight cardiovascular diseases - eg/ arrhythmias and hypertension targets (eg ion channel inhibitors)
Mutations in the ion channels can be detected by?
ECG - electrocardiogram
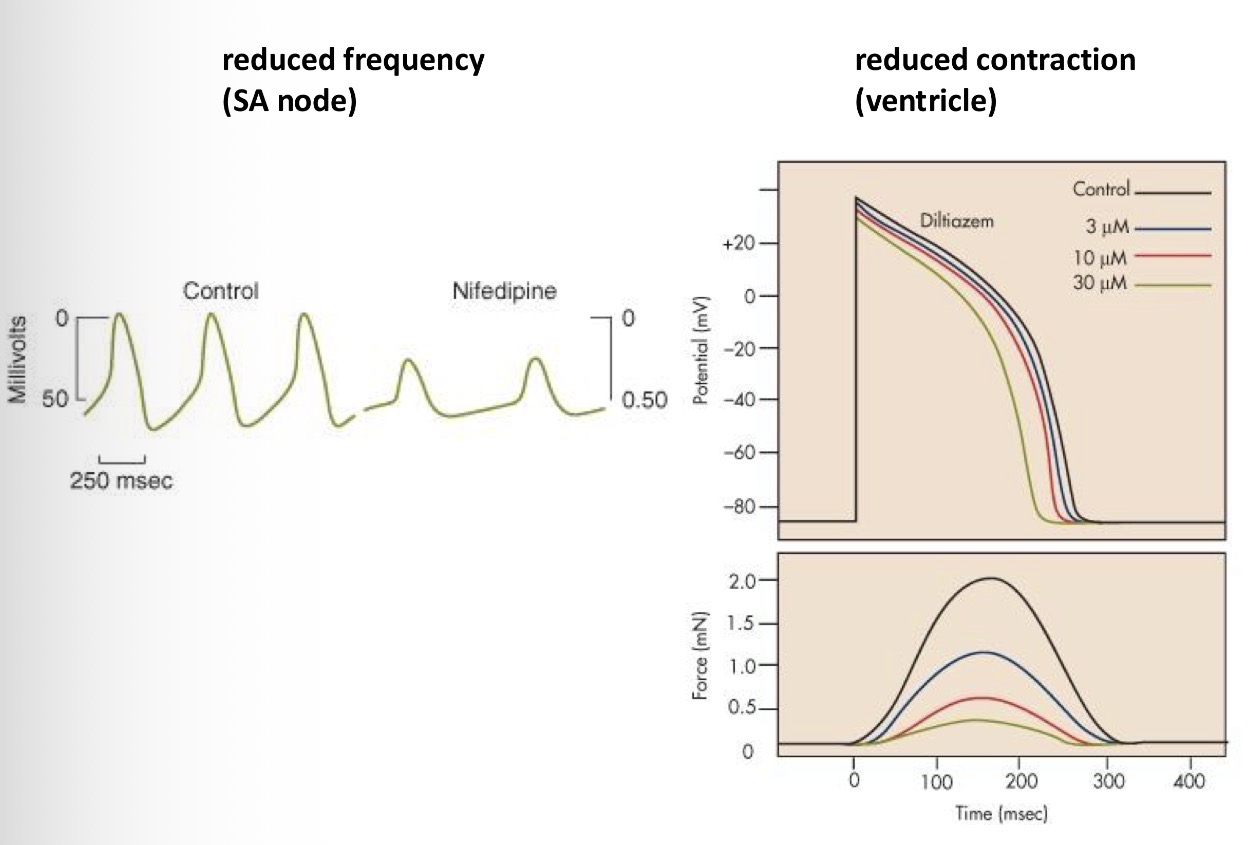
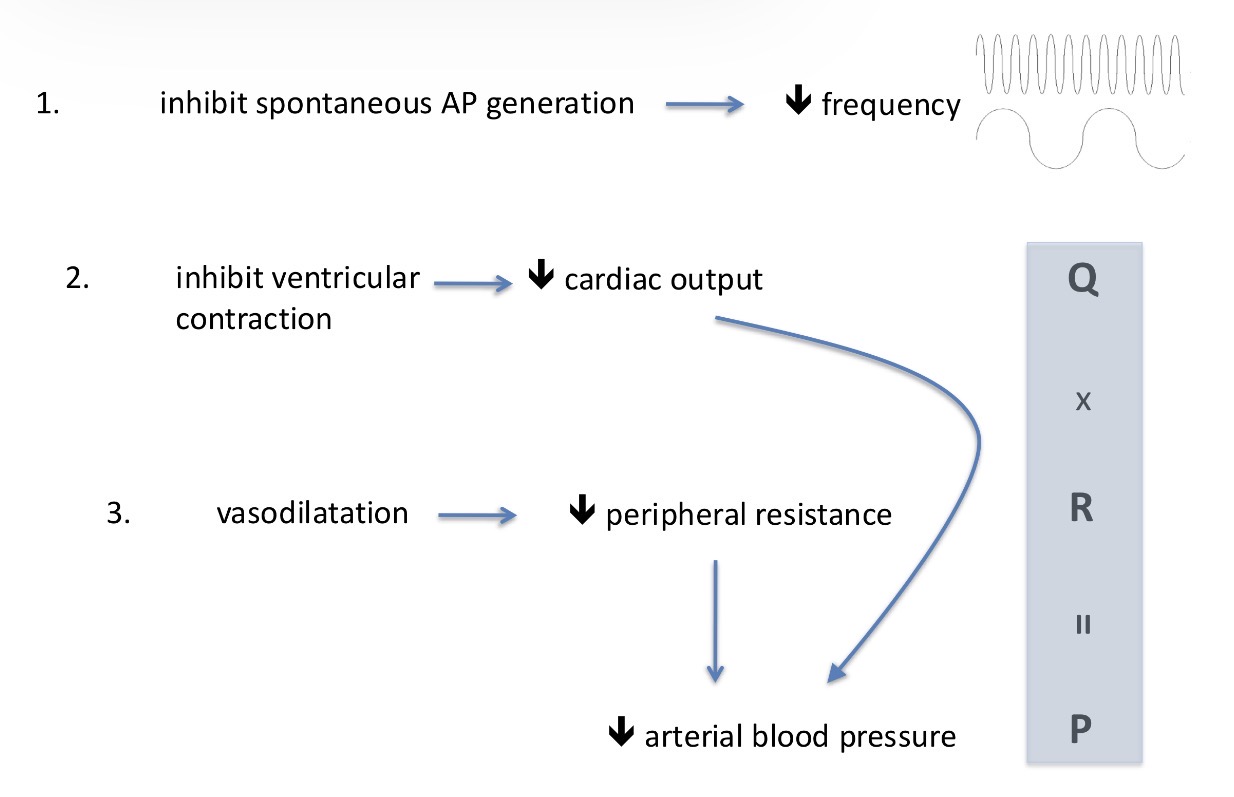
Give me an example of a calcium channel inhibitor and what does it do?
Nifedipine - can inhibit the AP, the frequency, the plateau level, the calcium influx = can inhibit contractions - reduces force created by the heart = reduces the blood pressure
Explain what’s happening here
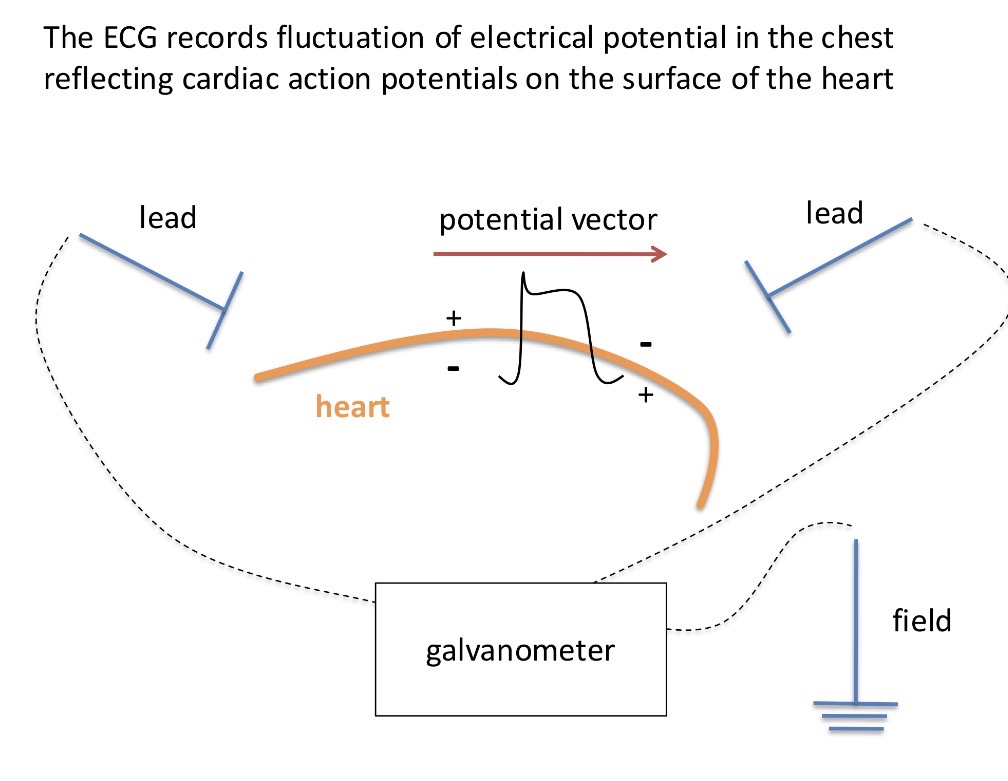
Explain what happens in an ECG:
When an AP happens in the heart, it changes the potential which can be measured by the ECG that can record the change in the potential of the cardiac cycle (the change happens inside the heart, which changes the potential on the surface of the heart and it is sent throughout the whole body which can be picked up by sensitive electrodes)
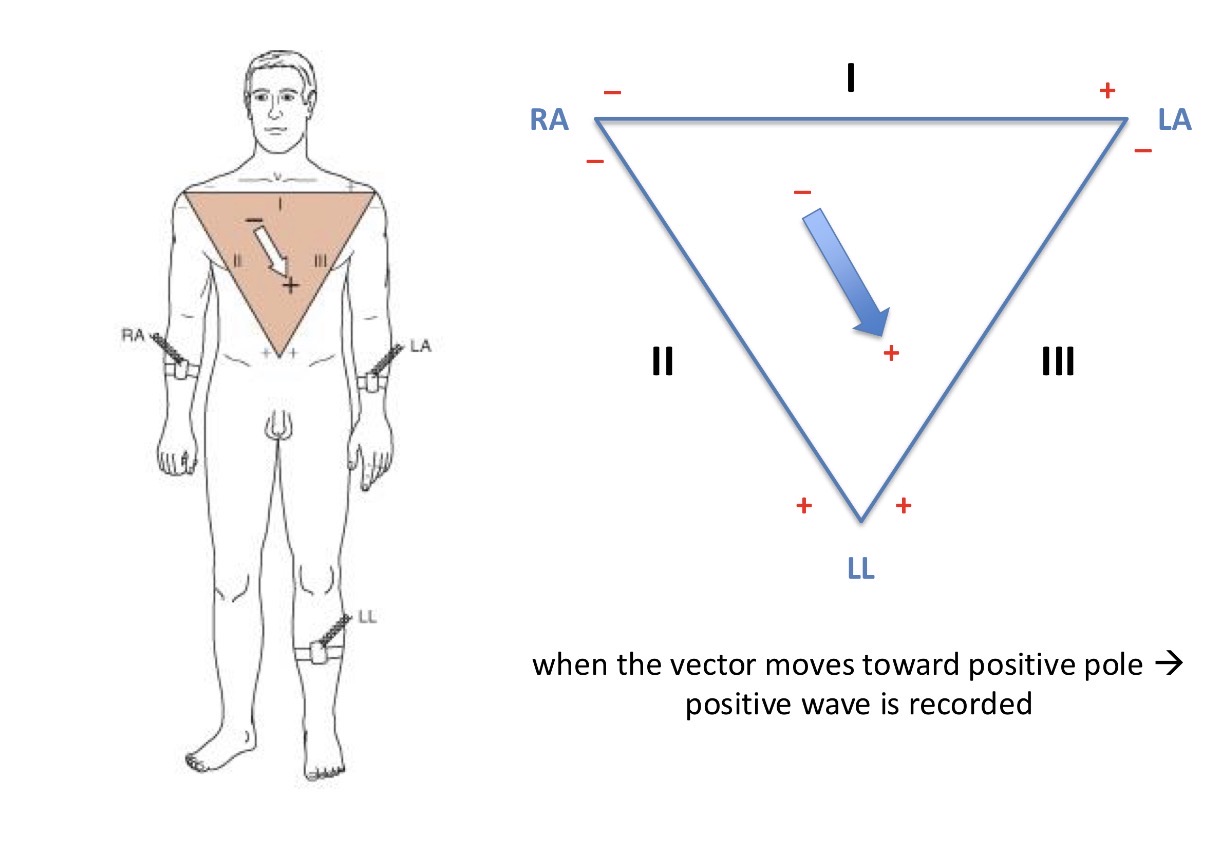
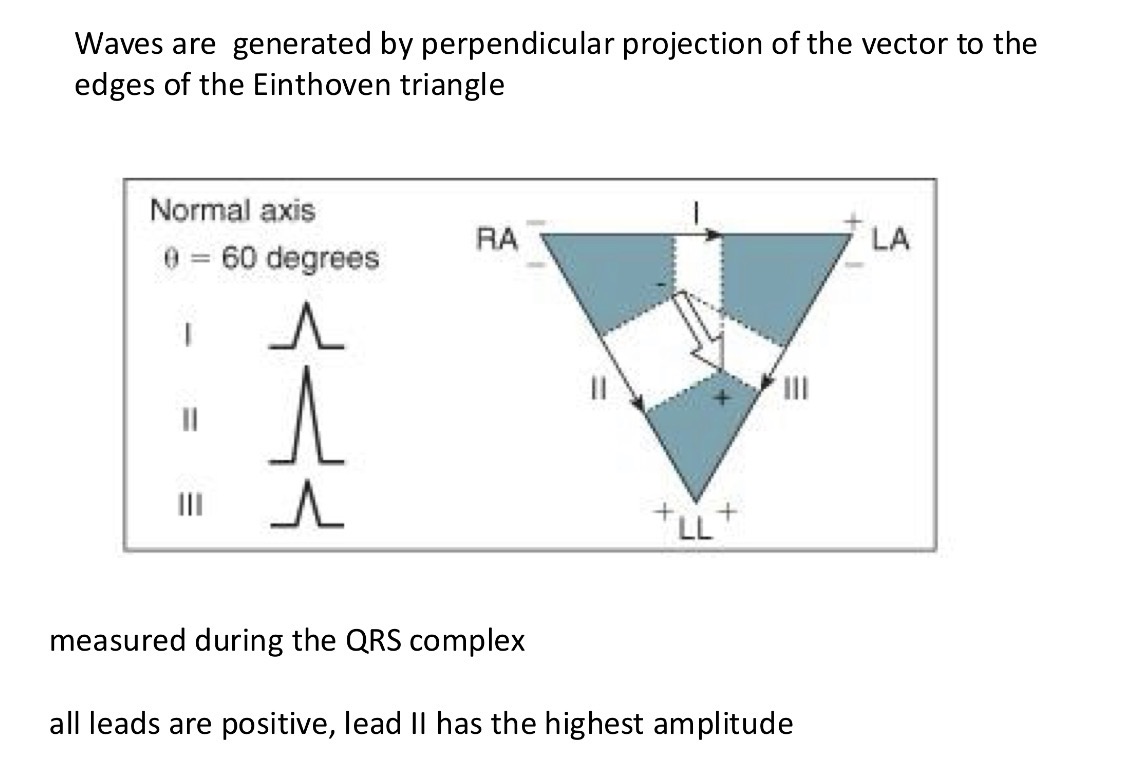
What is the basis to measure ECG
The Einthoven triangle - right arm, left arm, lower limb
You measure the potential differences on each part of the triangle and this measures the change parallel with that side. So when the vector moves towards a positive pole, a positive wave is recorded
This is the highest wave on the ECG - the R wave
What are the waves you see in the cardiogram and which is the biggest?
P, Q, R, S, T
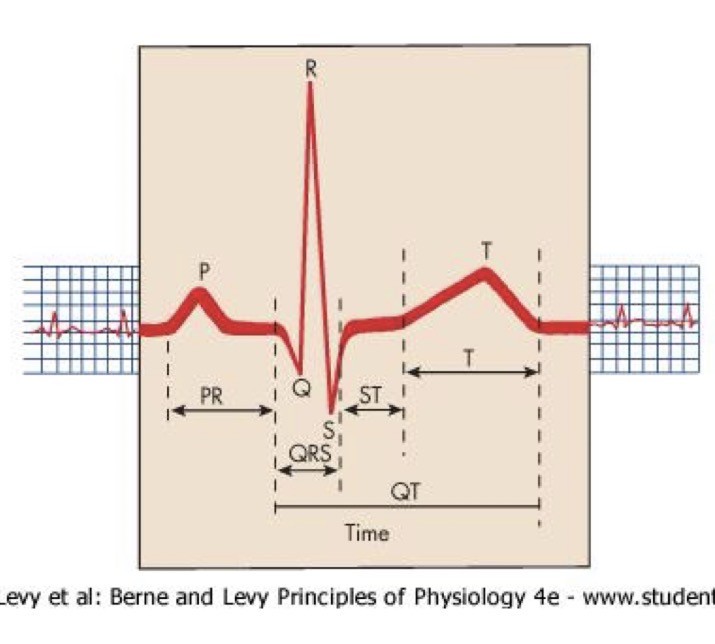
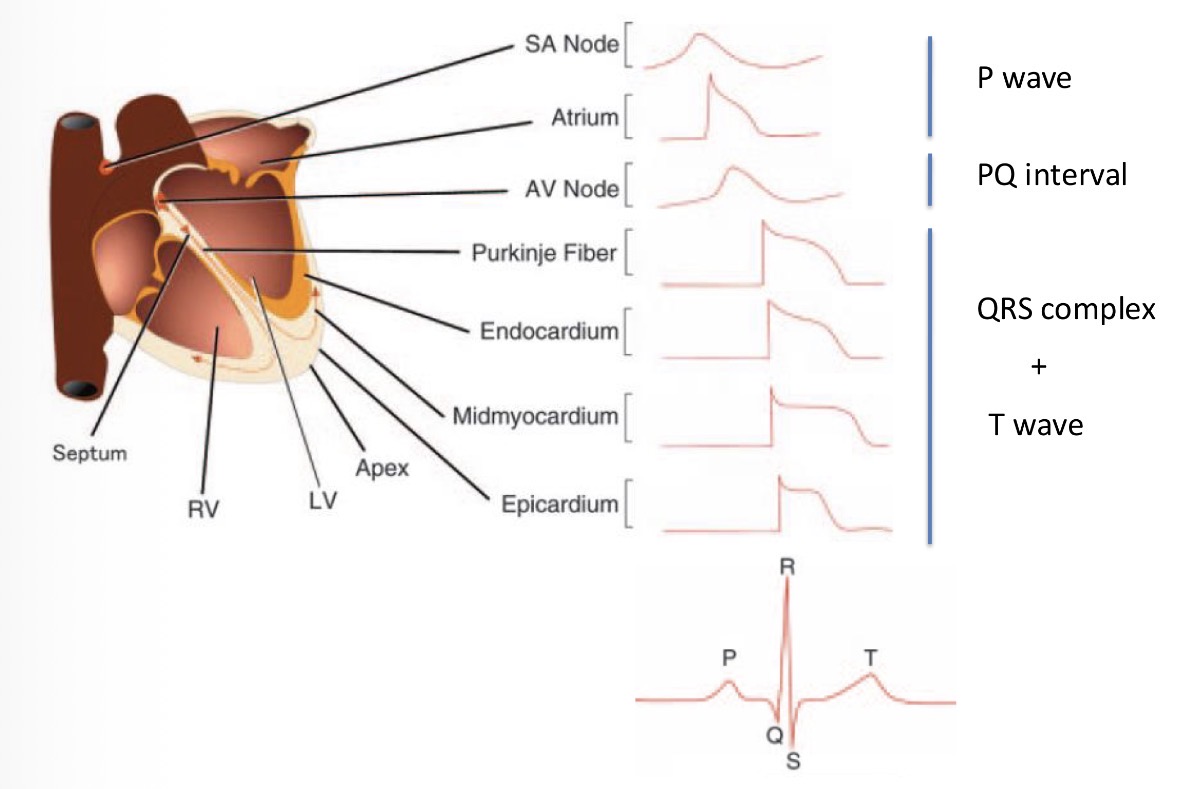
What does the P,Q,R,S,T wave reflect?
P - The APs in the atria
Q, R, S - shift of the AP peaks in the ventriclesn (highest amplitude because it has the highest muscle mass)
T - reflects the repolarization of the heart
How do we get a negative and positive peak in the ECG?
If the vector goes from negative to positive, the ECG will show a positive peak and vice versa
Repolarization to a negative pole = positive reflection
Repolarization to a positive pole = negative reflection
Depolarization to a negative pole = negative reflection
Depolarization to a positive pole = positive reflection
This is why the T wave is positive even if it reflects repolarization
What is ECG used for?
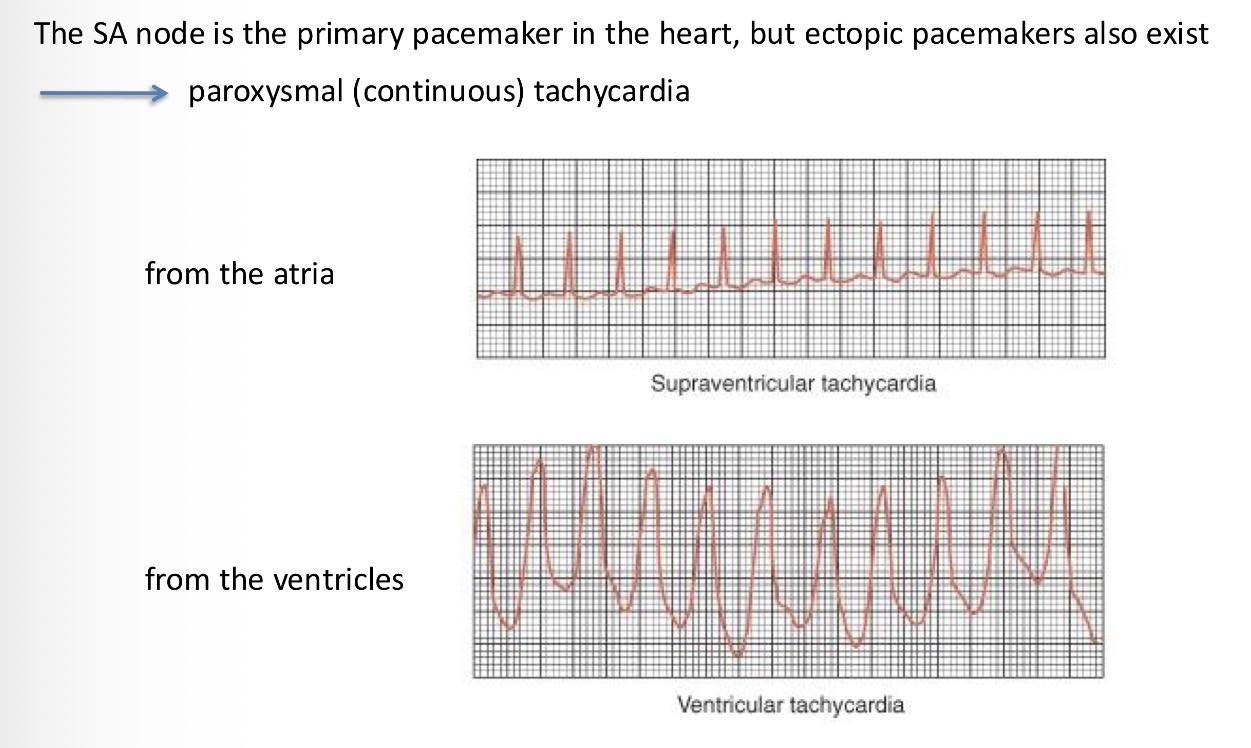
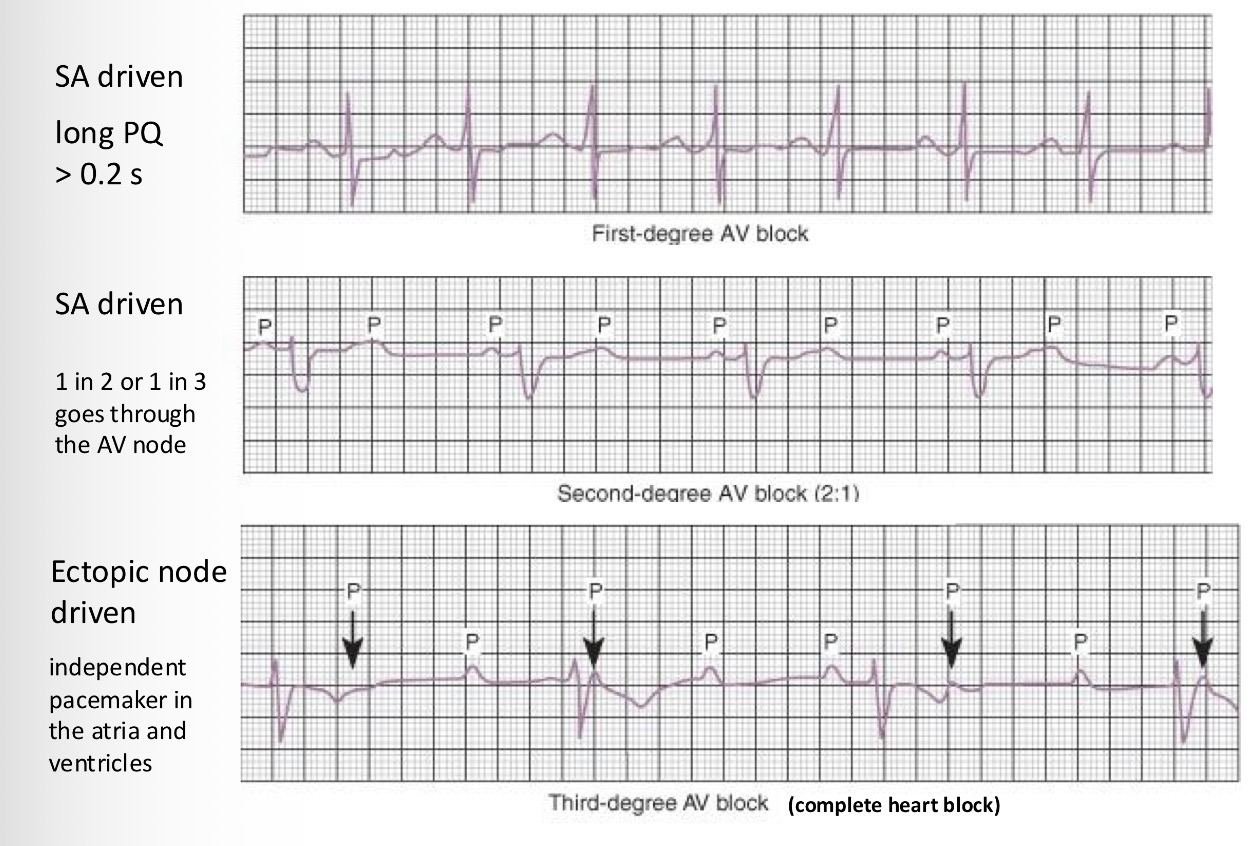
What are the types of arrhythmias? What blocks you can detect:
Explain what happens in these pictures too:
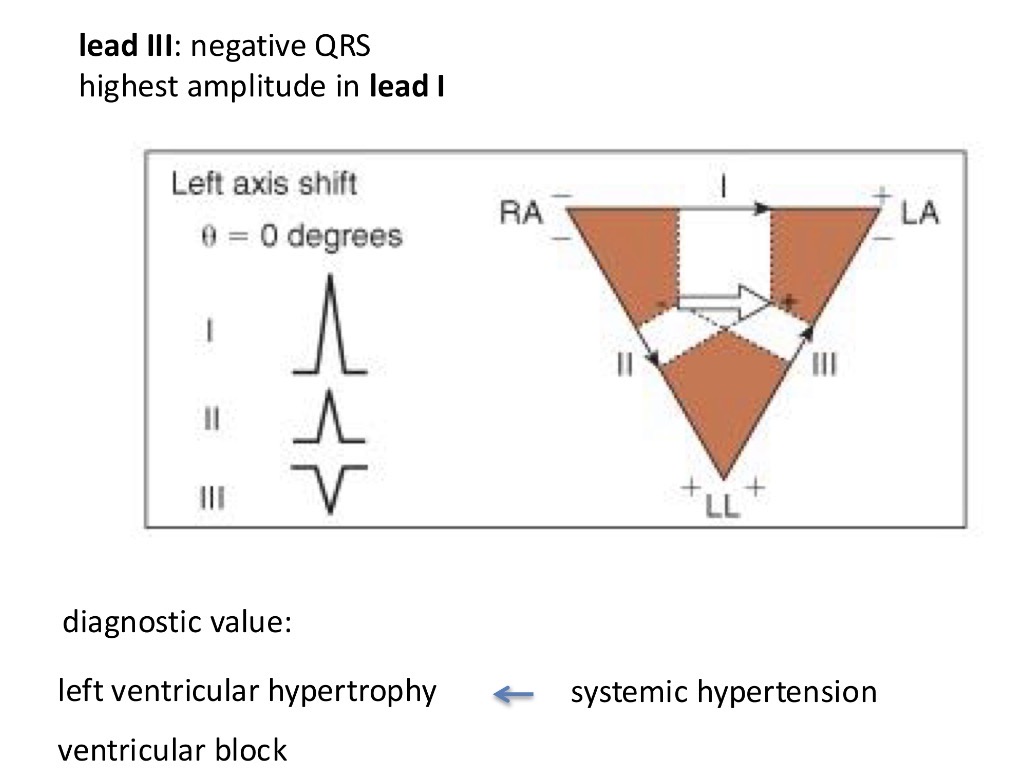
How do you reconstruct the direction of the activation of the heart?
Activation goes from atria to the ventricles → arrow down
Measure the the amplitude of the different sides so you measure the angle of where the activation happens
If activation is somehow deviated - if one of the ventricles is hypertrophied
Eg the right side is hypertrophied - and so the growth of that ventricle goes in a different direction and the wave direction changes
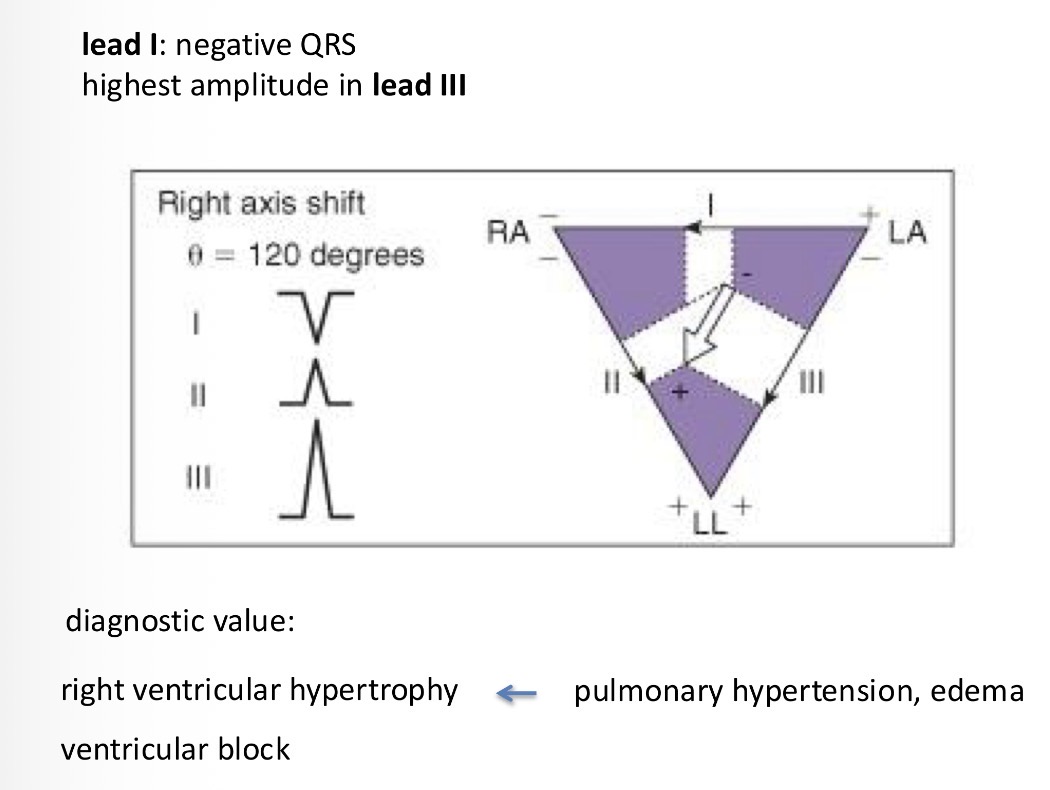
Lastly there is a left derivation of the heart
Systemic hypertension by the left ventricle and so the activation goes to that side and the largest R wave is in league 1
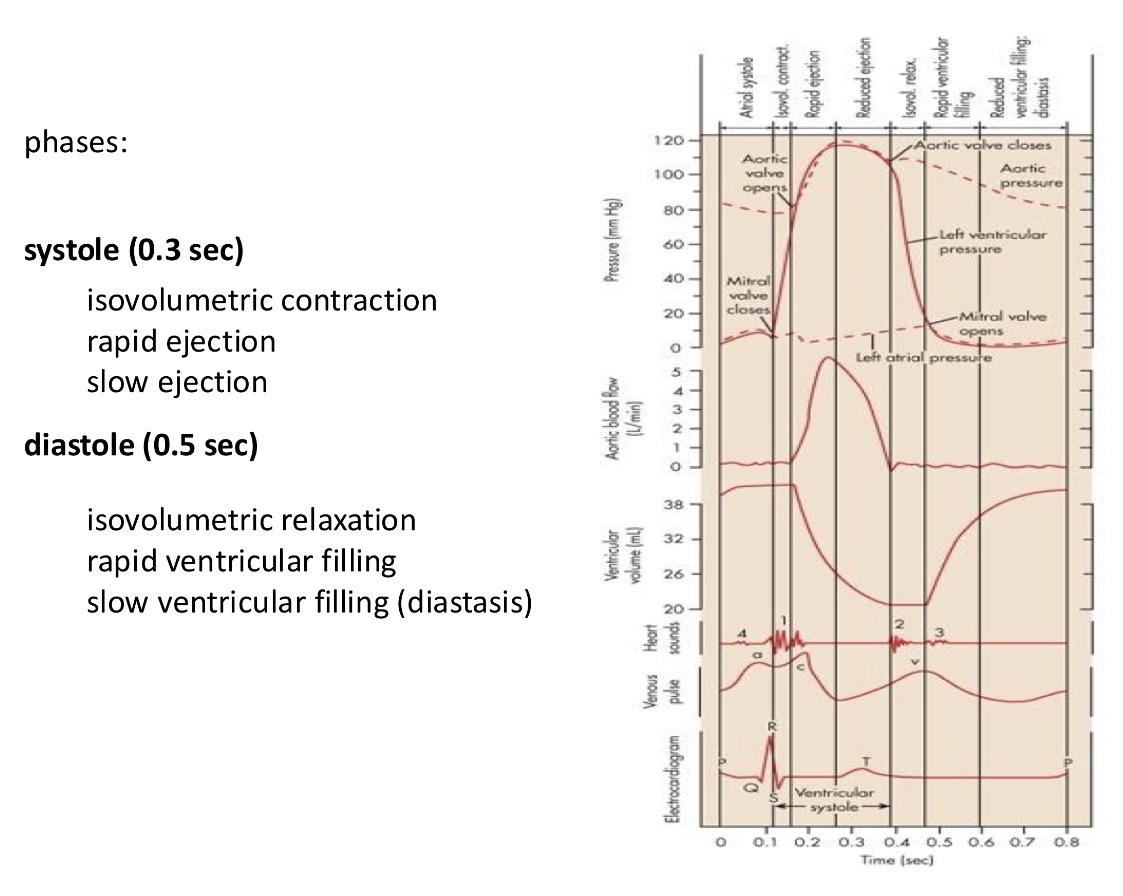
Explain the integration of electric signals into the cardiac cycle. Explain this image
The most informative is to measure the pressure in the different parts of the heart - pressure in the aorta, ventricles, atria = the pressure gradient will determine in which direction the blood is flowing
If you measure the blood flow in the aorta you can measure the ventricle volume depending on if it is relaxed or contracted
You can align this with heart sounds (lub and dub) and you can align it with ECG

try to remember:
Flow from higher pressure to lower pressure
Valves are opened and closed by the flow generated by the pressure difference (directing the flow)
In the picture you have all the different pressures:
when ventricular pressure is lower than atrial pressure = which will open the mitral valve and generate a flow form atria to ventricles
Heart starts to contract and generate pressure in the ventricles is higher than in the atrials and this will generate a backflow and this will close the mitral valve
This pressure is still lower than in the aorta = this means the ventricles are closed from both sides and this phase is called the isovolumetric contraction phase
This is followed by an increased pressure in the ventricles where the pressure increases and goes over the pressure in the aorta = and the blood rushes out from the ventricles and into the aorta through semi lunar valves
In this phase at the start there is a rapid ejection phase which will be reduced
Then the pressure starts to drop and when the pressure from the ventricles drops below that of the aorta, the aortic valve closes and that ensures a unidirectional flow of blood = isovlumetric relaxation (no change in volume)
This relaxation goes until the point until the pressure in the ventricles is below that of the atria and this opens the mitral valve
Then the cycle repeats
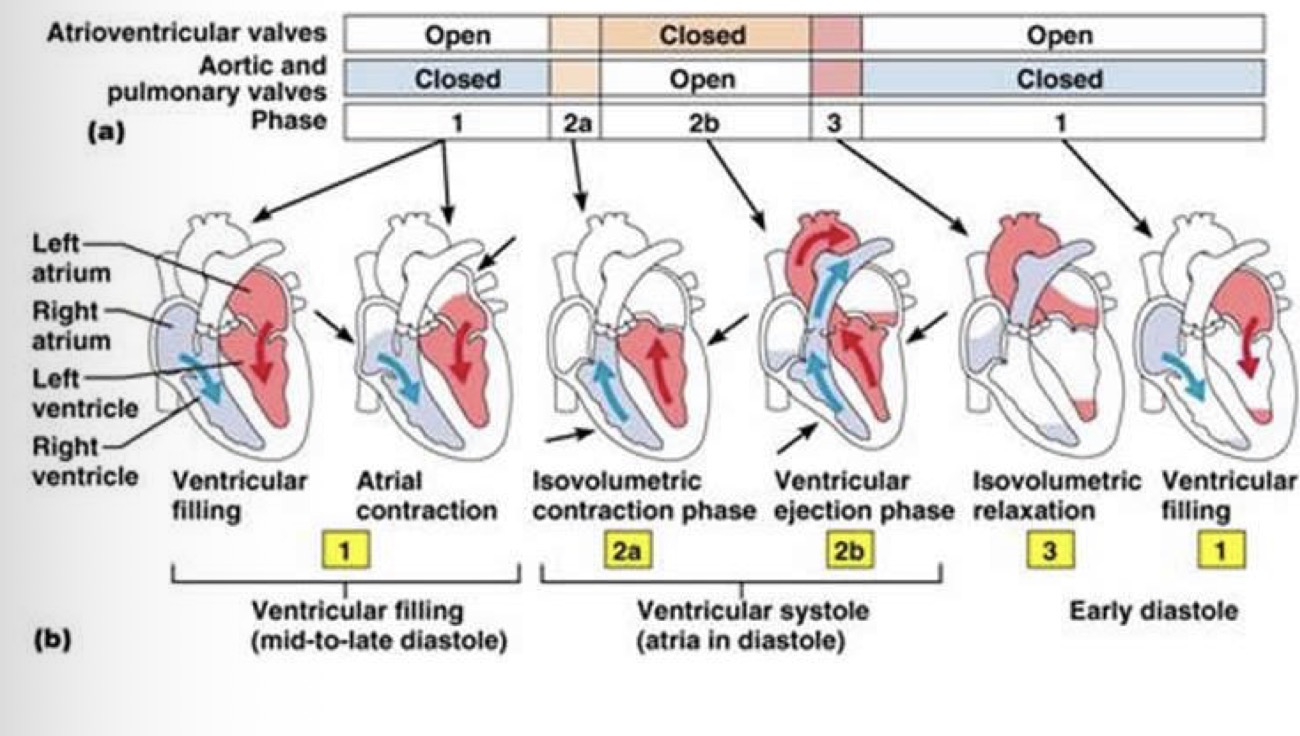
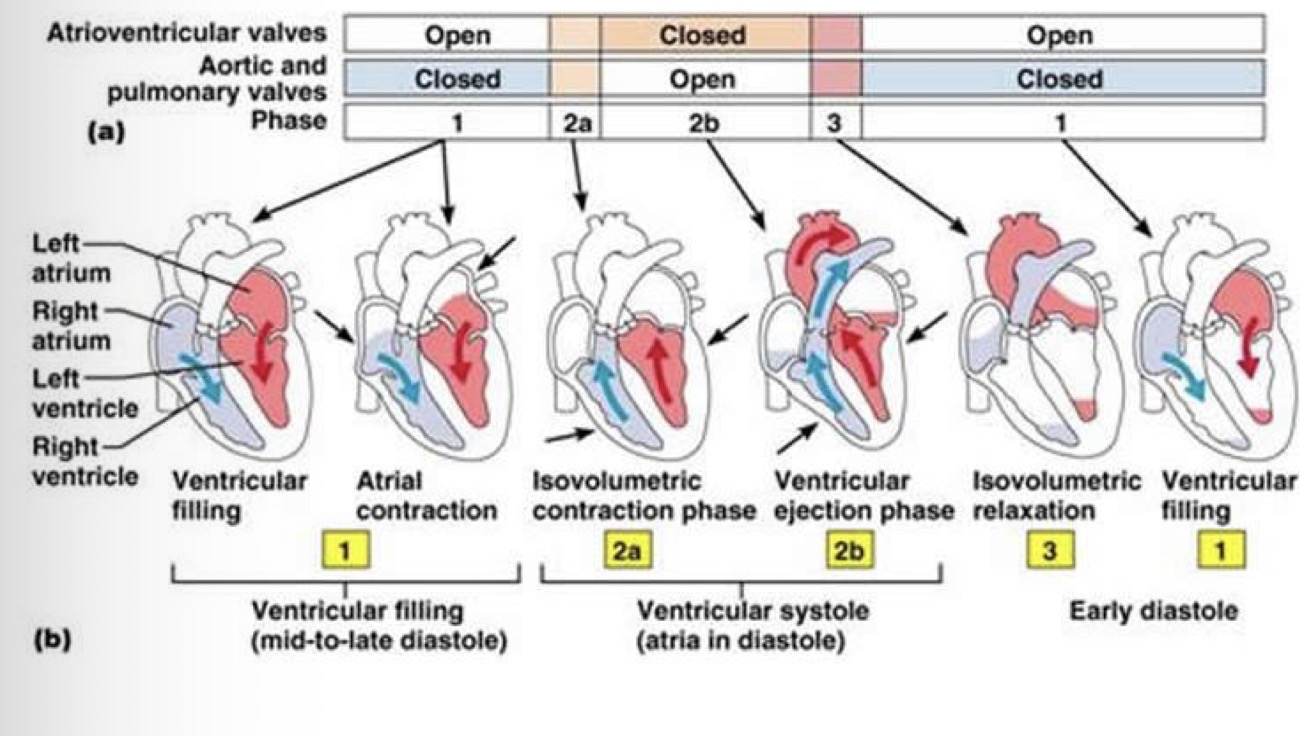
Explain what is on this picture:
Flow from higher pressure to lower pressure
Valves are opened and closed by the flow generated by the pressure difference (directing the flow)
In the picture you have all the different pressures:
when ventricular pressure is lower than atrial pressure = which will open the mitral valve and generate a flow form atria to ventricles
Heart starts to contract and generate pressure in the ventricles is higher than in the atrials and this will generate a backflow and this will close the mitral valve
This pressure is still lower than in the aorta = this means the ventricles are closed from both sides and this phase is called the isovolumetric contraction phase
This is followed by an increased pressure in the ventricles where the pressure increases and goes over the pressure in the aorta = and the blood rushes out from the ventricles and into the aorta through semi lunar valves
In this phase at the start there is a rapid ejection phase which will be reduced
Then the pressure starts to drop and when the pressure from the ventricles drops below that of the aorta, the aortic valve closes and that ensures a unidirectional flow of blood = isovlumetric relaxation (no change in volume)
This relaxation goes until the point until the pressure in the ventricles is below that of the atria and this opens the mitral valve
Then the cycle repeats
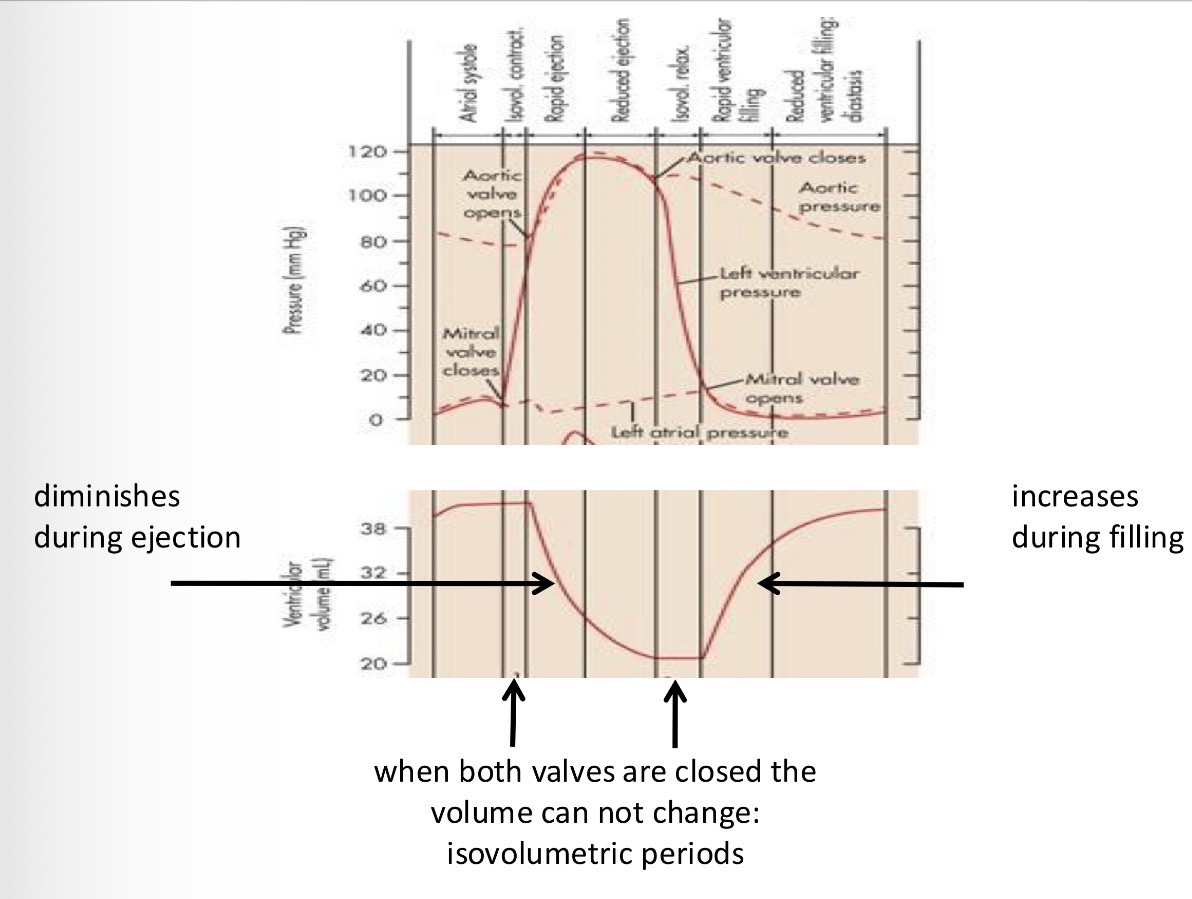
What happens to the volume of the ventricles during the cardiac cycle?
1 - beginning of the systole no change in volume
2 - when the aortic valve opens the blood is ejected so the volume goes down
3 - when the ventricular pressure drops below the aortic pressure, the volume stays the same
4 - the filling of the ventricles starts when the pressure of the ventricles is lower than that of the atria so the volume grows
The difference between the top and bottom of the blood volume is the amount of blood that was ejected in one stroke = stroke volume
When does the heart generate sound?
Flow generates sound when the flow is turbulent. This happens when the valves are closing because when the valves close, the blood hits the valve and the flow become turbulent. Sound is generated by the turbulent flow hitting the valve
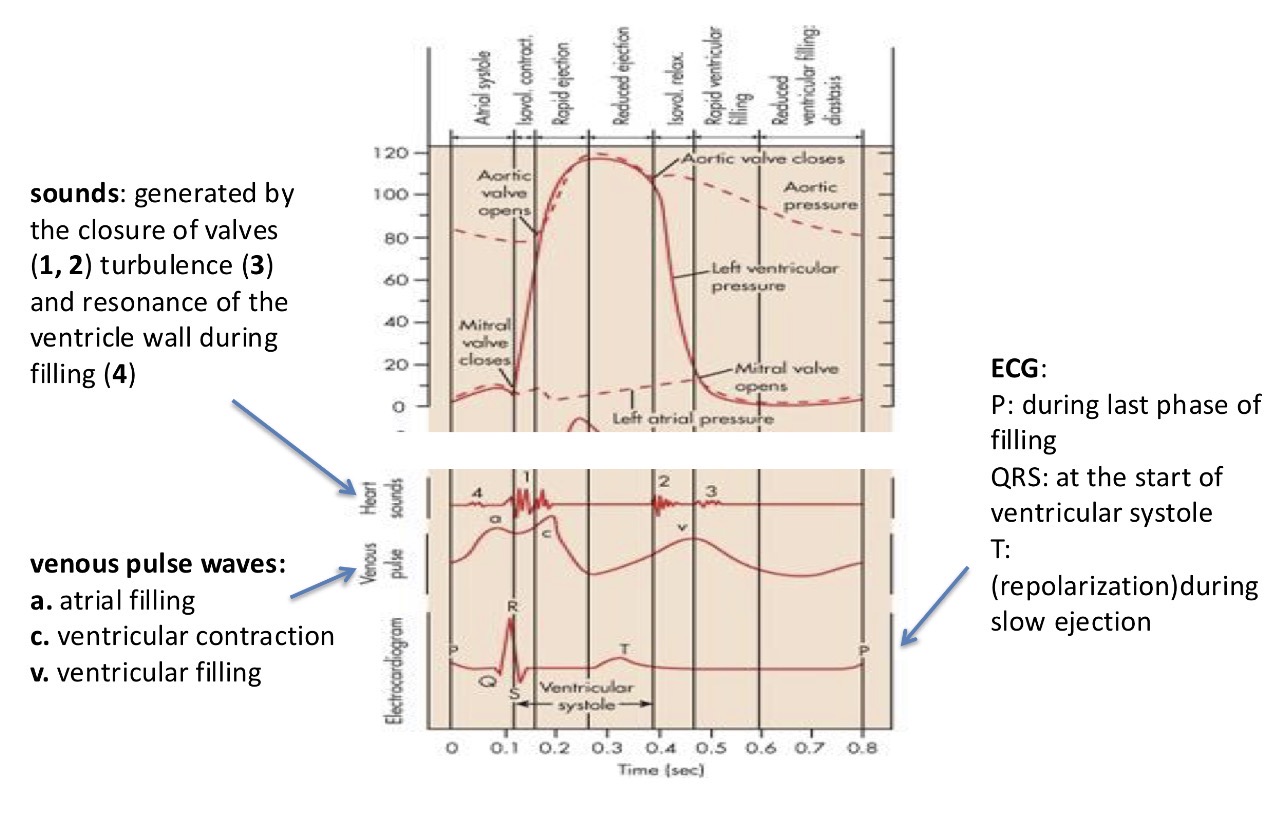
What valves is the sound generated by in the heart?
The first sound is generated by the mitral valves closing
The second sound is generated by the semilunar valves closing
The third sound is generated by the mitral valve opening
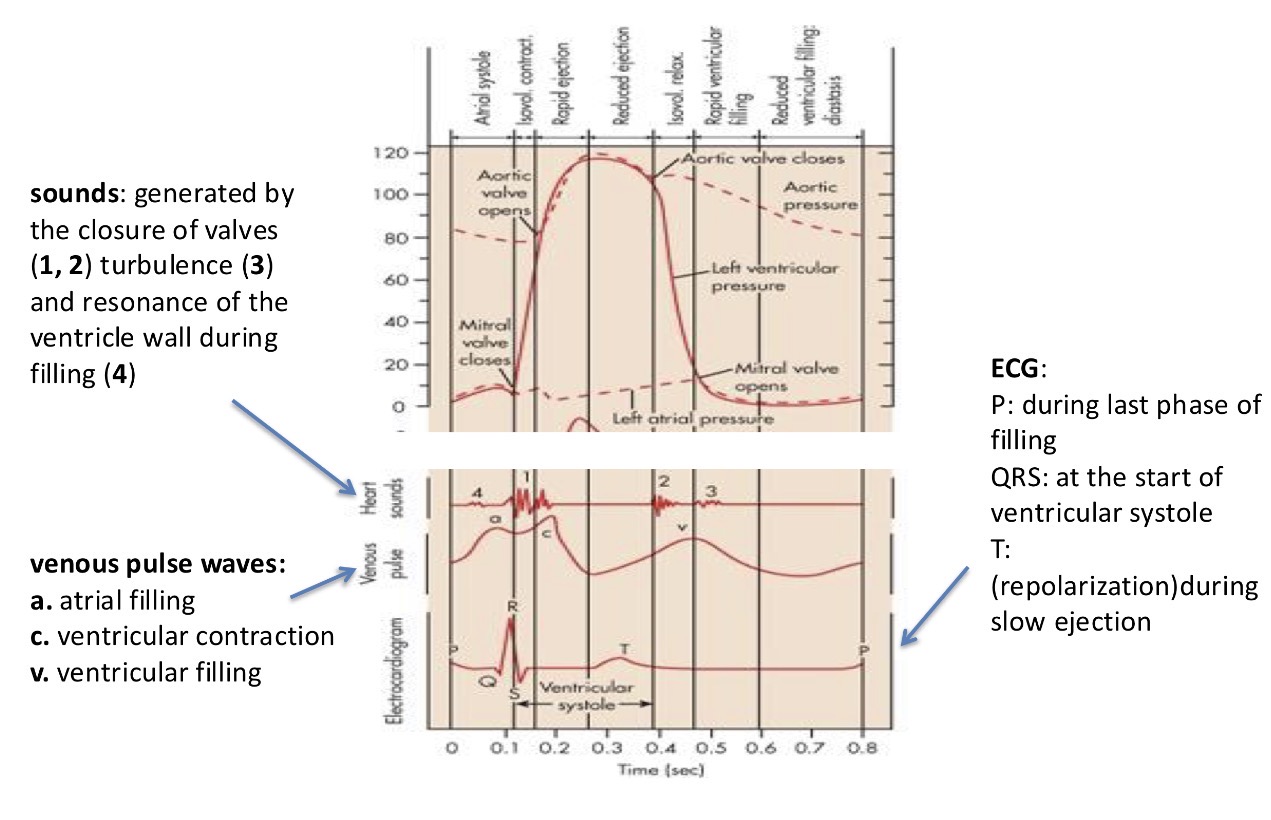
How long does the systole and diastole last? (Using the peaks on the ECG)
systole lasts form the R to the end of the T on the ECG
And the diastole lasts form the end of the T to the next QRS that happens