gait deviations
1/158
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
159 Terms
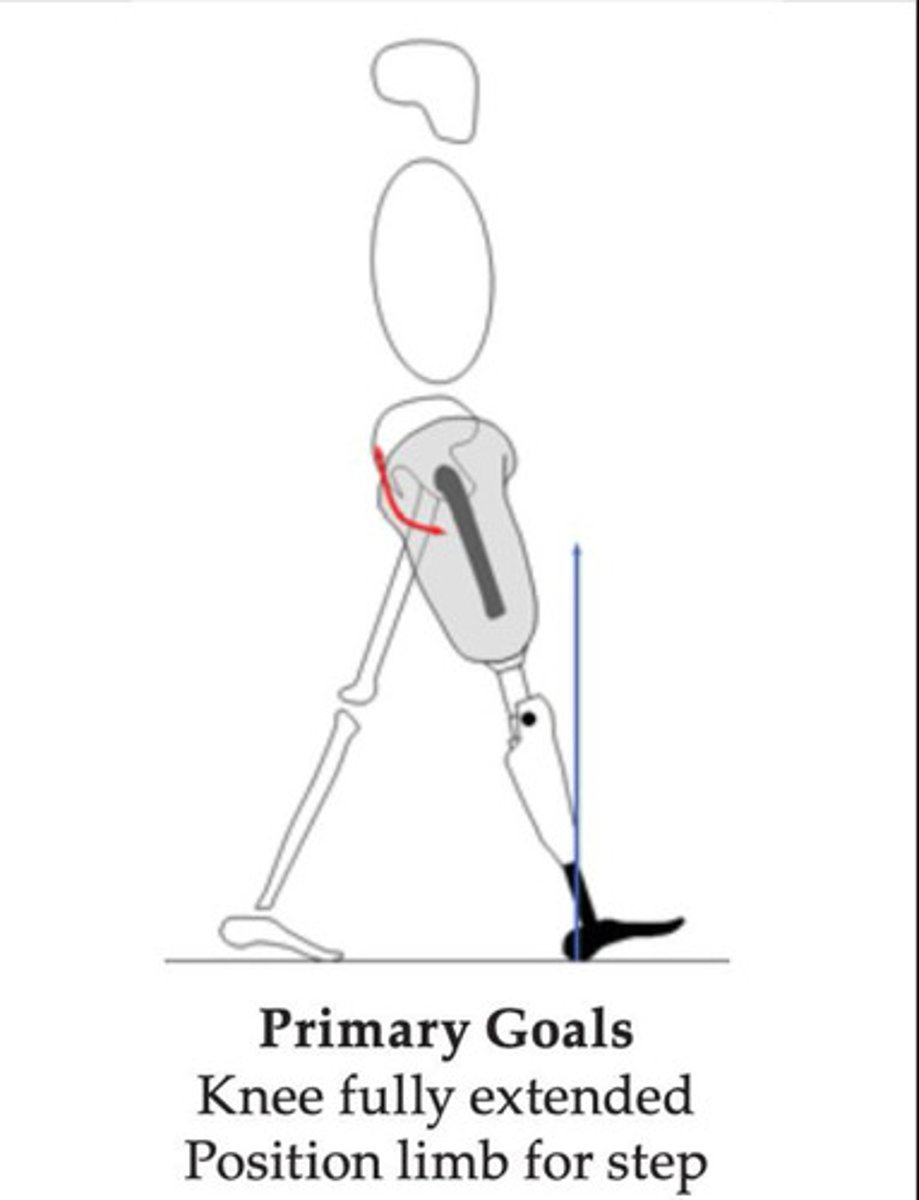
What are the two primary goals of IC in TF gait?
1. knee fully extended
2. limb positioned for step
Short sound side step deviation at IC is best viewed in the plane.
sagittal
What are three potential prosthetic causes of short sound side step at IC?
1. insufficient socket FL
2. excessive ankle PF
3. excessive knee EXT moment (knee too posterior)
How might insufficient socket FL cause a short sound side step at IC?
patient is unable to extend/pseudo-extend enough on the prosthetic side, shortening the sound step
How might excessive ankle PF cause a short sound side step at IC?
corresponds to "halted gait," keeping the patient from progressing the weight line forward, shortening the sound step
How might excessive knee EXT moment (knee too posterior) cause a short sound side step at IC?
corresponds to "halted gait," keeping the patient from progressing the weight line forward, shortening the sound step
What are three potential patient causes of short sound side step at IC?
1. short RL
2. hip FL contracture
3. insecurity/fear
Why might a short RL cause a short sound side step at IC?
short lever arm makes limb usage difficult and energy consuming, so the patient does not extend as far, shortening the sound side step
Why might a hip FL contracture cause a short sound side step at IC?
lack of available hip extension/pseudo-extension to allow for longer advancement of the contralateral limb, shortening the sound side step
Why might insecurity/fear cause a short sound side step at IC?
patient may not trust putting weight in the device, so they get off of it as soon as possible and shorten the time spend on the prosthetic side, shortening the sound side step
Short prosthetic step deviation at IC is best viewed in the plane.
sagittal
What are five potential causes of short prosthetic step at IC?
1. excessive socket FL
2. insufficient EXT assist
3. excessive ankle DF
4. excessive FL moment (knee too anterior)
5. poor suspension
Why might excessive socket FL cause a short prosthetic step at IC?
the prosthesis is so flexed that they have no remaining ROM to flex the limb forward enough to take a bigger step
Why might insufficient extension assist cause a short prosthetic step at IC?
the knee does not extend enough in swing, so the patient makes contact with the floor as soon as possible before gravity bends the knee too much as they swing through, shortening the prosthetic step
Why might excessive DF cause a short prosthetic step at IC?
excessive DF increases the FL moment and the patient keeps the prosthetic leg closer to them for a more stable landing; the patient feels like they are falling forward, throwing the sound limb out in front of them, making the sound step longer than the prosthetic step
Why might an excessive FL moment (knee too anterior) cause a short prosthetic step at IC?
excessive FL moment makes for an unstable IC landing, so the patient keeps the prosthetic leg closer to their weight line (short step) for a more stable landing at IC
Why might poor suspension cause a short prosthetic step at IC?
the longer the prosthesis is off the ground, the more it begins sliding off, so the patient puts the prosthetic leg down as fast as they can to avoid that, shortening the prosthetic step
What are three potential patient causes of a short prosthetic step at IC?
1. poor balance
2. discomfort
3. weak hip musculature
Why might poor balance cause a short prosthetic step at IC?
poor balance can cause inconsistency in the placement of the foot (it is often an inconsistent deviation in itself), and the patient takes a longer step off the prosthesis on the sound side to protect against falling backwards
Why might discomfort cause a short prosthetic step at IC?
swing phase discomfort of the prosthetic leg may cause them to put it back on the ground in stance as soon as possible, shortening the prosthetic step
stance phase discomfort of the contralateral limb may lead them to spend more time on the prosthetic side, lengthening the sound side swing time/step length
Why might weak hip musculature cause a short prosthetic step at IC?
flexors: the patient's hip flexors are too weak to bring the prosthetic leg out further, leading to a shortened prosthetic step
extensors: the patient spends more time taking a long step with the sound side because is allows them to relax their extensors on the prosthetic side, since stability here is maintained by the GRF position
Insufficient knee extension deviation at IC is best viewed in the plane.
sagittal
What is one potential prosthetic cause of insufficient knee extension at IC?
1. excessive knee extension resistance
Why might excessive knee extension resistance cause insufficient knee extension at IC?
the knee extension resistance is too high and prevents the knee from reaching full extension by IC
What are two potential patient causes of insufficient knee extension at IC?
1. weak hip flexors
2. weak hip extensors
Why might weak hip flexors cause insufficient knee extension at IC?
patient is not strong enough to progress the limb through swing phase to extend the knee
Why might weak hip extensors cause insufficient knee extension at IC?
once IC is made, weak hip extensors cannot maintain knee extension
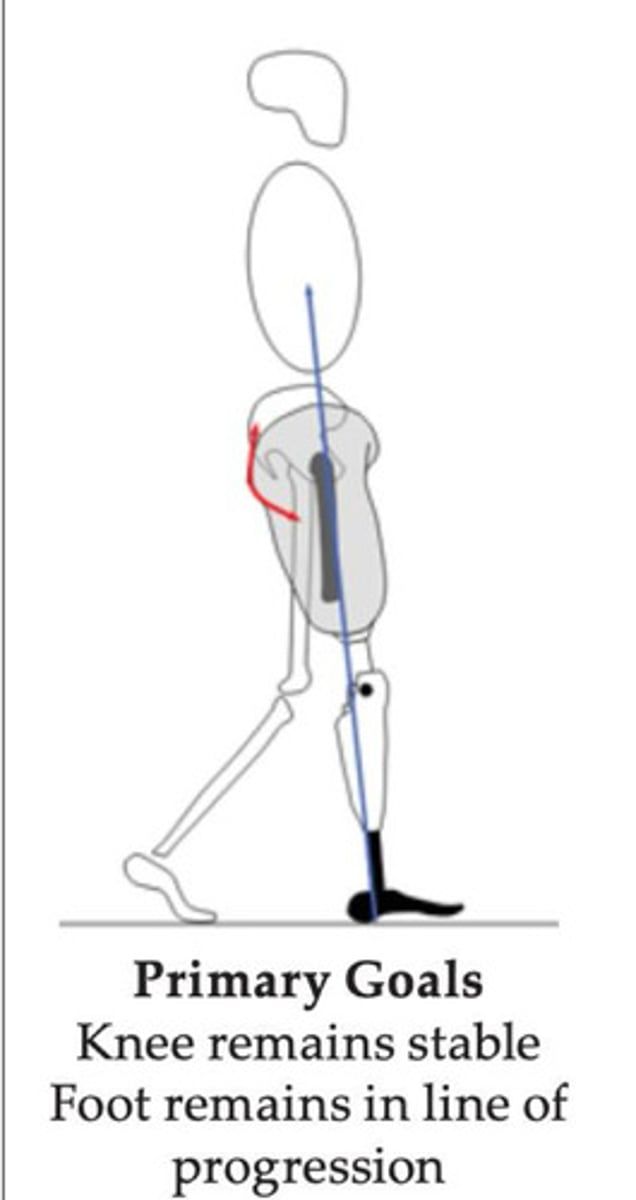
What are the two primary goals of LR in TF gait?
1. knee remains stable
2. foot remains in line of progression
Rapid toe descent (foot slap) deviation at LR is best viewed in the plane.
sagittal
What is one potential cause of rapid toe descent (foot slap) at LR?
1. PF bumper (heel) too soft
Why might a soft PF bumper cause rapid toe descent (foot slap) at LR?
heel compresses too quickly, bringing the foot quickly to the ground (often seen in single axis feet)
What is one potential patient cause of rapid toe descent (foot slap) at LR?
1. insecurity/fear
Why might insecurity/fear cause rapid toe descent (foot slap) at LR?
patient wants to ensure stability at LR so they kick their heel into the ground and cause rapid toe descent to reach stability quicker
External foot rotation deviation at LR is best viewed in the plane.
coronal
What are four potential prosthetic causes of external foot rotation at LR?
1. excessive toe-out
2. PF bumper (heel) too stiff
3. socket too loose
4. socket too tight
Why might excessive toe-out cause external foot rotation at LR?
alignment causes external rotation of the foot through all phases of gait
Why might a stiff PF bumper (heel) cause external foot rotation at LR?
heel cannot compress and the forces cause the foot to externally rotate
Why might an excessively loose socket cause external rotation of the foot at LR?
socket may rotate on the limb and cause them to land with it externally rotated and/or internally rotated (inconsistent deviation)
Why might an excessively tight socket cause external rotation of the foot at LR?
if the socket is too tight around the posteromedial wall, the hamstrings will press against the wallet hollow modification and cause external rotation of the socket
What is one potential patient cause of external rotation of the foot at LR?
1. poor hip muscular control
Why might poor hip muscular control cause external rotation of the foot at LR?
the patient is too weak to overcome the forces on the prosthesis during LR and becomes unable to maintain the LOP
Knee instability deviation at LR is best viewed in the plane.
sagittal
What are four potential prosthetic causes of knee instability at LR?
1. knee too anterior
2. PF bumper (heel) too stiff
3. insufficient socket FL
4. stance flexion damping too low
Why might an excessively anterior knee cause knee instability at LR?
knee position in relation to GRF causes a FL moment, causing instability at the knee
Why might an excessively stiff PF bumper (heel) cause knee instability at LR?
heel cannot compress and the forces cause the knee to FL
Why might insufficient socket FL cause knee instability at LR?
hip extensors/glutes are not placed on stretch when the socket is not flexed enough, so they are not effective at controlling the stability of the knee at LR
Why might insufficient stance flexion damping cause knee instability at LR?
knee allows for too much stance FL for the patient to handle, causing instability
What are two potential patient cause of knee instability at LR?
1. shoe heel too high/stiff
2. weak hip extensors
Why might an excessively high/stiff shoe heel cause knee instability at LR?
causes increased FL moment on the knee (usually caused by change of shoe into one that it was not dynamically aligned for)
Why might weak hip extensors cause knee instability at LR?
patient has little control over knee extension with their extensors, causing instability
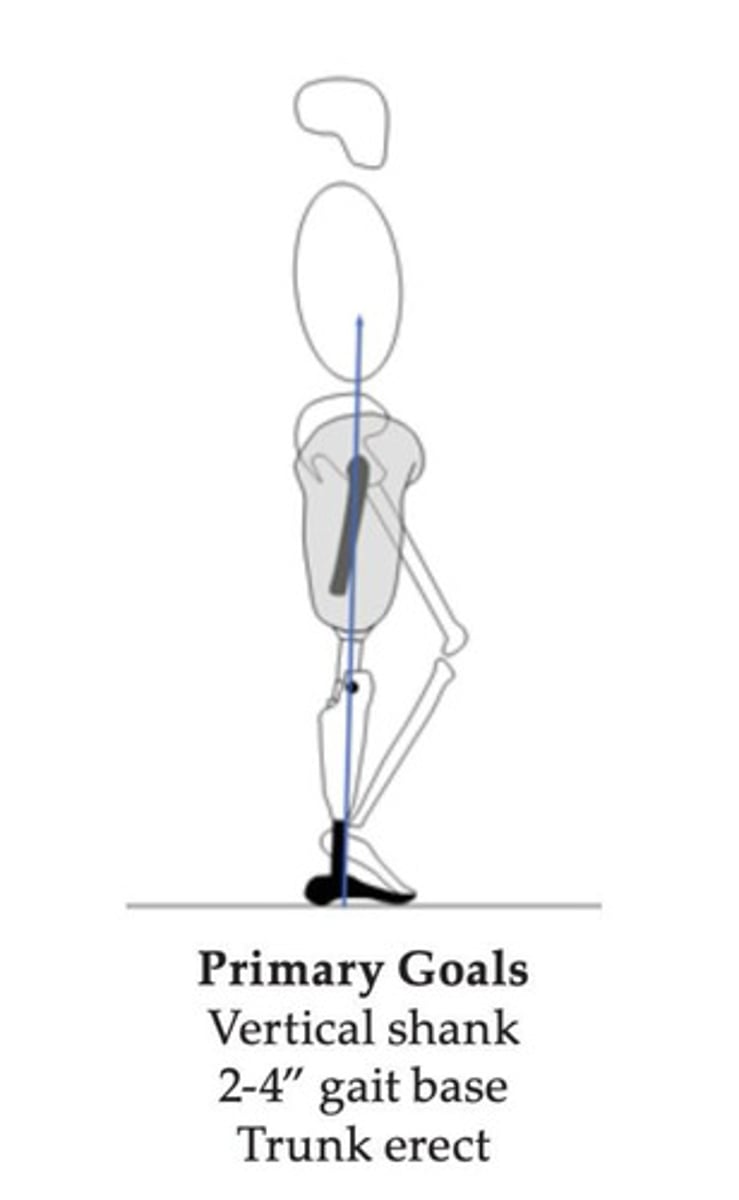
What are the three primary goals of MSt in TF gait?
1. vertical shank/pylon
2. 2"-4" gait base
3. trunk erect
Laterally leaning trunk deviation at MSt is best viewed in the plane.
coronal
What are four potential prosthetic causes of laterally leaning trunk at MSt?
1. prosthesis height too short
2. medial wall tooo high
3. socket too ABD/insufficient socket ADD
4. insufficient lateral wall support
Why might a short prostheses cause a laterally leaning trunk at MSt?
patient must lean over in order to reach the ground with the short prosthesis, causing a lateral lean
Why might an excessively high medial wall cause a laterally leaning trunk at MSt?
the medial wall may be impinging on the perineum and causes a lateral lean as an antalgic deviation
Why might an excessively ABD socket/insufficiently ADD socket cause a laterally leaning trunk at MSt?
patient may not be ABD inside the socket and has to lean over to accommodate the angle, causing a lateral lean
Why might insufficient support from the lateral wall cause a laterally leaning trunk at MSt?
lack of support from the lateral wall will fail to ADD the femur inside the socket, so it is ABD, causing pain at the distal lateral femur, causing a lateral lean as an antalgic deviation
What are four potential patient causes of a laterally leaning trunk at MSt?
1. weak hip ABD
2. ABD contracture
3. very short RL
4. insufficient weight shift over the prosthesis
Why might weak hip ABD cause a laterally leaning trunk at MSt?
Trendelenburg gait
Why might an ABD contracture cause a laterally leaning trunk at MSt?
the patient must lean over to get their prosthesis under them
Why might a very short RL cause a laterally leaning trunk at MSt?
shorter lever arm to control M/L stability of the trunk, so patient reduces the need to control stability by moving their weight line over their heel with a lateral lean
Why might insufficient weight shifting over the prosthesis cause a laterally leaning trunk at MSt?
patient is trying to shift their weight using their trunk instead of their pelvis, typical of inexperienced walkers
Abducted gait deviation at MSt is best viewed from the plane.
coronal
What are five potential prosthetic causes of abducted gait at MSt?
1. prosthesis too tall
2. socket too ABD
3. medial wall too high
4. insufficient contouring of the lateral wall
5. pelvic band and hip joint positioned too far from the patient
Why might an excessively tall prosthesis cause abducted gait at MSt?
the patient cannot get their prosthesis directly under them with even hips, so they bring their leg out to the side in abducted gait
Why might an excessively ABD socket cause abducted gait at MSt?
patient's limb is consistently abducted through the gait cycle, causing an abducted gait pattern
Why might a high medial wall cause abducted gait at MSt?
the medial wall may be impinging on the perineum and the patient will walk with abducted gait as an antalgic deviation to relieve the perineum
Why might insufficient contouring of the lateral wall cause abducted gait at MSt?
lack of support from the lateral wall will fail to ADD the femur inside the socket, so it is ABD, causing pain at the distal lateral femur, causing abducted gait as an antalgic deviation
Why might a misaligned pelvic band and hip joint (too far from patient) cause abducted gait at MSt?
patient must abduct the legs to bring the pelvic band closer to their hip to restore a better alignment
What are four potential patient causes of abducted gait at MSt?
1. ABD contracture
2. weak hip ABD
3. poor balance/proprioception
4. insufficient weight shift over prosthesis
Why might an ABD contracture cause abducted gait at MSt?
patient physically cannot get their prosthesis directly under them, so they walk with consistently abducted gait
Why might weak hip ABD cause abducted gait at MSt?
the patient will also have weak ADD due to the TF amputation, but will maintain the hip in ABD to maintain a wider base of support while walking
Why might poor balance/proprioception cause abducted gait at MSt?
patient is seeking a wider base of support for stability/balance or cannot directly control where in space the foot lands
Why might insufficient weight shifting over the prosthesis cause abducted gait at MSt?
patient does not shift weight over the prosthesis, so it posts out to the side in abducted gait, typical of inexperienced walkers
Medially leaning pylon deviation at MSt is best viewed from the plane.
coronal
What is the prosthetic cause of a medially leaning pylon at MSt?
1. excessive socket ADD
Why might an excessively ADD socket cause a medially leaning pylon at MSt?
distal socket moves medially while foot remains lateral
Laterally leaning pylon deviation at MSt is best viewed from the plane.
coronal
What is the prosthetic cause of a latearlly leaning pylon at MSt?
1. insufficient socket ADD
Why might insufficient socket ADD cause a laterally leaning pylon at MSt?
distal socket drifts too far laterally, while the foot remains more medial
Excessive stance flexion deviation at MSt is best viewed from the plane.
sagittal
What are the four potential prosthetic causes of excessive stance flexion at MSt?
1. knee too anterior
2. excessive ankle DF
3. insufficient stance flexion damping
4. change in heel height
Why might an excessively anterior knee cause excessive stance flexion at MSt?
there is too much of a FL moment at the knee, causing excessive stance FL
Why might excessive ankle DF cause excessive stance flexion at MSt?
DF causes an increased FL moment at the knee with foot flat, increasing stance FL
Why might insufficient stance flexion damping cause excessive stance flexion at MSt?
patient's knee allows for too much stance flexion for the patient to control
Why might a change in heel height cause excessive stance flexion at MSt?
if the patient changed from a lower to a taller heel height, the FL moment at the knee would be increased, increasing stance FL
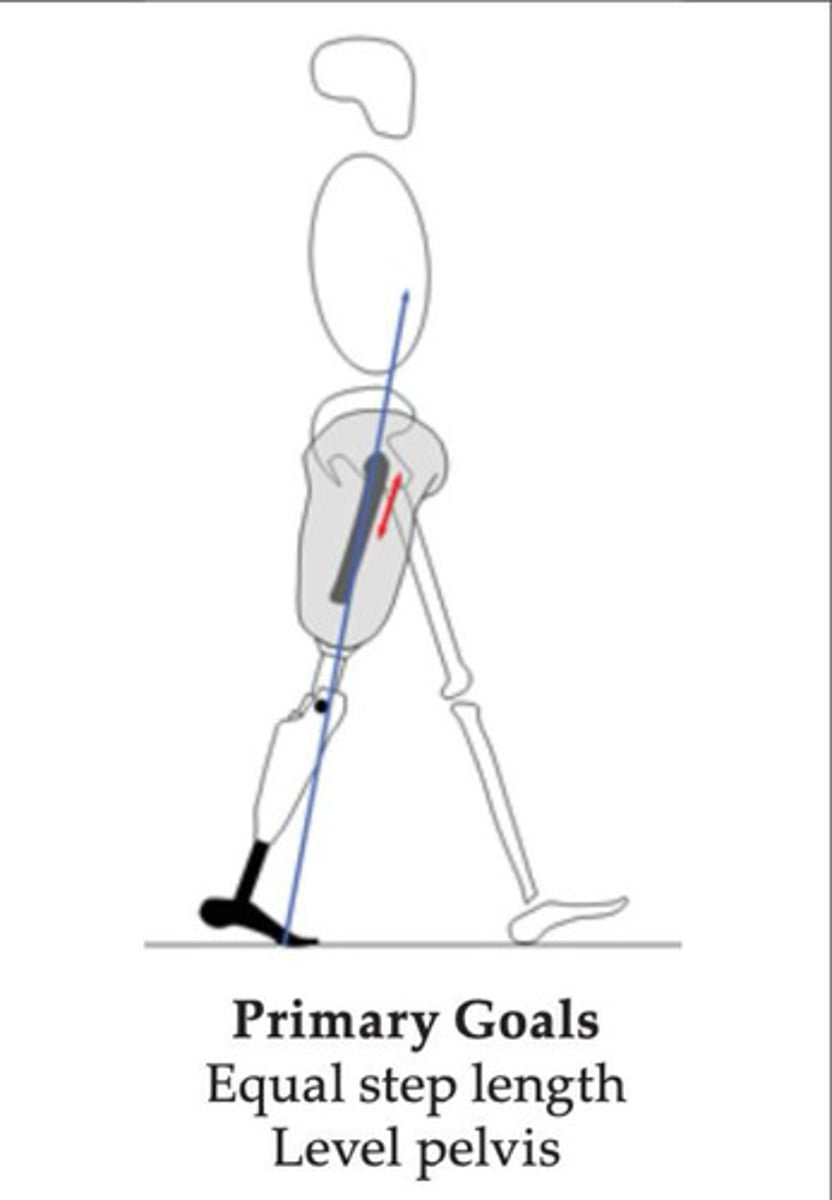
What are the two primary goals of MSt through TSt in TF gait?
1. equal step length
2. level pelvis
Excessive lordosis deviation at MSt/TSt is best viewed from the plane.
sagittal
What are two potential prosthetic causes of excessive lordosis at MSt/TSt?
1. insufficient socket FL
2. insufficient support from anterior wall
Why might insufficient socket FL cause excessive lordosis at MSt/TSt?
patient may have limited extension/pseudo-extension ROM and uses lordosis to compensate to extend their leg
Why might insufficient support from the anterior wall cause excessive lordosis at MSt/TSt?
if the Scarpa's triangle modification is insufficient, it will not act as a counterforce to the glutes/ischium so the patient may lose the flexion of the socket, losing the ability to extend and compensating with excessive lordosis
What are three potential patient causes of excessive lordosis in MSt/TSt?
1. hip FL contracture
2. weak hip EXTs
3. weak core
Why might a hip FL contracture cause excessive lordosis at MSt/TSt?
patient may compensate to keep their posture upright to avoid a forward lean by using lordosis
Why might weak hip EXTs cause excessive lordosis at MSt/TSt?
the patient may have weakness when extending the hip to stand upright, so they compensate to avoid a forward lean by using lordosis
Why might a weak core cause excessive lordosis at MSt/TSt?
a patient's core may be weak and fatigued while attempting to maintain an upright posture, so they use lordosis instead to relieve their abdominals
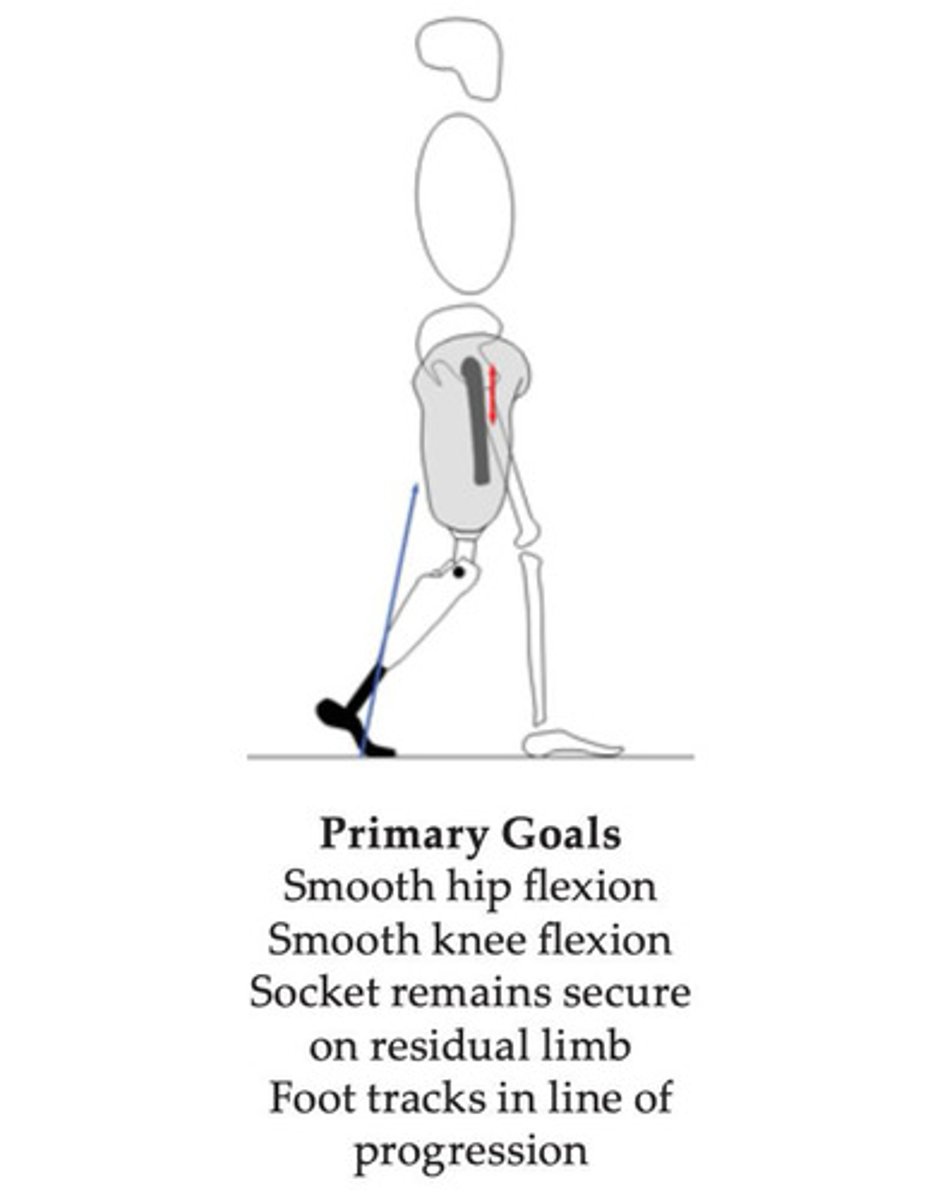
What are the four primary goals of PSw in TF gait?
1. smooth hip FL
2. smooth knee FL
3. maintain suspension
4. foot track through LOP
Medial whip deviation at PSw is best viewed from the plane.
coronal
What are two potential prosthetic causes of medial whip at PSw?
1. EXT ROT of knee
2. socket too tight/inappropriately contoured
Why might EXT ROT of the knee cause a medial whip at PSw?
even though the patient's limb moves through the LOP, the knee flexes externally and the ankle comes in medially
Why might an excessively tight/inappropriately contoured socket cause a medial whip at PSw?
as the muscles contract, the socket rotates to the area of least resistance in an externally rotated position, causing a medial whip