Transport in animals
1/31
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
32 Terms
Need for Transport Systems in Multicellular Animals
As size increases, SA:V ratio decreases.
A lower SA:V ratio means diffusion across the body surface becomes too slow.
Multicellular animals have a high metabolic rate, so cells need a constant supply of oxygen and nutrients and rapid removal of wastes.
Many cells are far from the body surface, increasing diffusion distance
Open and closed circulatory system
Open:
Blood (haemolymph) is not always contained within vessels.
Haemolymph is pumped into body cavities (haemoceol) and directly bathes tissues.
Low pressure, slower transport.
Insects do not use haemolymph to transport oxygen (tracheal system does this).
Closed:
Blood remains within vessels at all times.
Higher pressure and faster transport.
More efficient delivery of substances.
More complex
Single and double closed circulation
Single (fish):
Blood passes through the heart once per complete circuit.
Heart → Gills → Body → Heart
Blood pressure falls at the gills.
Slower circulation to the body.
Double (mammals):
Blood passes through the heart twice per complete circuit.
Heart → Lungs → Heart → Body → Heart
Pulmonary circulation (heart ↔ lungs)
Systemic circulation (heart ↔ body)
Blood is re-pressurised after the lungs.
Faster blood flow and more efficient oxygen delivery.
Arteries
Function: Carry blood away from the heart at high pressure.
Structure & adaptations:
Thick wall, small lumen.
Elastic tissue stretches and recoils to maintain pressure.
Smooth muscle allows vasoconstriction/dilation.
Collagen prevents bursting.
Relative wall composition:
Collagen ~30%
Smooth muscle ~35%
Elastic tissue/ elastin ~35%
Arterioles
Function: Control blood flow into capillaries so they do not burst.
Structure & adaptations:
Small lumen, relatively thick wall.
Lots of smooth muscle for vasoconstriction/dilation (more than arteries), vasoconstriction is contracting of smooth muscles to decrease lumen size, and vasodiliation is relaxation
Little elastic tissue.
Relative wall composition:
Collagen ~20%
Smooth muscle ~70%
Elastic tissue/ elastin ~10%
Capillaries
Function: Exchange of substances.
Structure & adaptations:
Wall one cell thick squamous endothelium.
Very narrow lumen (slows blood for more time for diffusion and makes only one RBC at a time and more contact surface).
Short diffusion distance.
Relative wall composition:
Collagen 0%
Smooth muscle 0%
Elastic tissue/ elastin 0%
Veins
Function: Return blood to the heart at low pressure.
Structure & adaptations:
Thin wall, large lumen reduces resistance, less likelihood of backflow.
Valves prevent backflow for a one way flow to heart.
More collagen than muscle or elastic tissue to prevent collapse.
Relative wall composition:
Collagen ~60%
Smooth muscle ~20%
Elastic tissue/ elastin ~20%
Venules
Function: Carry blood from capillaries to veins.
Structure & adaptations:
Thin wall, large lumen reduce resistance.
Very little muscle or elastic tissue.
Relative wall composition:
Collagen ~70%
Smooth muscle ~15%
Elastic tissue/ elastin ~15%
Formation tissue fluid
Arteriole End
Hydrostatic pressure > oncotic pressure.
Water and small dissolved substances (e.g. glucose, O₂, ions) are forced out through gaps in the capillary endothelium by ultrafiltration.
Red blood cells and plasma proteins remain in the blood as they are too large to pass through.
Venule End
Hydrostatic pressure decreases due to fluid loss.
Plasma proteins remain in the capillary, lowering the blood's water potential creating oncotic pressure
Oncotic pressure > hydrostatic pressure.
Water with dissolved ions (tissue fluid) re-enters the capillary by osmosis.
Composition blood, tissue fluid, lymph
Blood
Plasma, red blood cells, white blood cells, platelets, plasma proteins, dissolved solutes.
Tissue Fluid
Similar to plasma but lacks red blood cells and contains very little protein.
Contains O₂, glucose, ions and other small molecules.
Lymph
Similar to tissue fluid but contains fewer nutrients and oxygen (having supplied tissues).
May contain lymphocytes.
Very low protein concentration.
Lymphatic system
Lymph is excess tissue fluid that has not re-entered the capillaries at the venule end.
It enters lymphatic vessels because the excess fluid would otherwise accumulate in tissues, causing swelling (oedema).
As lymph passes through lymph nodes, it is filtered and more lymphocytes can be added to help detect and destroy pathogens.
The lymphatic system returns this fluid (and any leaked proteins) back to the bloodstream, helping maintain blood volume and pressure.
External Structure heart
Four chambers: right atrium, right ventricle, left atrium, left ventricle (directions changed as if you are looking at the heart so left is on right side)
Coronary arteries supply the heart muscle (myocardium) with oxygenated blood.
Aorta carries oxygenated blood from the left ventricle to the body.
Pulmonary artery carries deoxygenated blood from the right ventricle to the lungs.
Pulmonary veins return oxygenated blood from the lungs to the left atrium.
Vena cava returns deoxygenated blood from the body to the right atrium.
Internal Structure
Atria: thin-walled upper chambers that receive blood.
Ventricles: thicker-walled lower chambers that pump blood out.
Left ventricle has the thickest wall as it pumps blood around the entire body.
Septum separates the left and right sides of the heart, preventing mixing of oxygenated and deoxygenated blood.
Atrioventricular (AV) valves prevent backflow from ventricles to atria create lub sound when shut.
Right AV valve = tricuspid valve.
Left AV valve = bicuspid (mitral) valve.
Semilunar valves prevent backflow from arteries into ventricles create dub sound when shut.
Aortic valve.
Pulmonary valve.
Chordae tendineae ("heart strings") attach AV valves to papillary muscles, preventing valve inversion during ventricular contraction.
Cardiac cycle
Atrial Systole (depolarisation)
Atria contract.
Atrial pressure > ventricular pressure.
AV valves open, semilunar valves closed.
Blood is forced into the ventricles.
Ventricular Systole (depolarisation)
Ventricles contract about 0.1 second delay so they can fill up from atria.
Ventricular pressure > atrial pressure → AV valves close.
Ventricular pressure > arterial pressure (aorta/pulmonary artery) → semilunar valves open.
Blood is pumped into the arteries.
Diastole (repolarisation)
Atria and ventricles relax.
Arterial pressure > ventricular pressure → semilunar valves close.
Ventricular pressure < atrial pressure → AV valves open.
Blood flows passively into the ventricles.
Role of Valves
AV valves prevent backflow into the atria during ventricular systole.
Semilunar valves prevent backflow into the ventricles during diastole.
Valves open and close due to pressure differences.
Direction blood flow in heart
Vena cava → Right atrium → Tricuspid valve → Right ventricle → Pulmonary valve → Pulmonary artery → Lungs → Pulmonary veins → Left atrium → Mitral valve → Left ventricle → Aortic valve → Aorta → Body.
Cardiac output
Cardiac Output = Heart Rate × Stroke Volume
Cardiac output: volume of blood pumped per minute.
Heart rate: beats per minute (bpm).
Stroke volume: volume of blood pumped per beat.
Myogenic nature of the heart
Cardiac muscle is myogenic: it can contract without external stimulation.
The heartbeat originates within the heart itself.
Sequence of Excitation in heart
Sino-atrial node (SAN) ("pacemaker") generates a wave of excitation in the right atrium.
Excitation spreads across both atria, causing atrial systole.
A non-conducting layer prevents excitation passing directly to the ventricles.
Excitation reaches the atrio-ventricular node (AVN).
The AVN delays the impulse briefly 0.1 seconds, allowing the ventricles to fill completely.
Excitation travels down the Bundle of His in the interventricular septum.
Excitation spreads through the Purkyne tissue (Purkinje fibres) from the apex upwards in ventricular walls
Ventricles contract (ventricular systole) from the bottom up, forcing blood into the arteries.
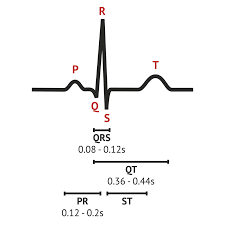
Normal ECG
P wave: Atrial depolarisation (atrial systole).
QRS complex: Ventricular depolarisation (ventricular systole).
T wave: Ventricular repolarisation (ventricular relaxation/diastole).
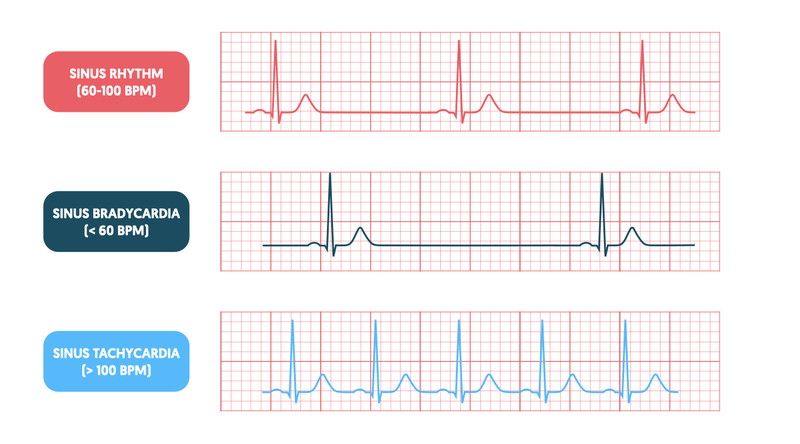
Tachycardia and brachycardia
Tachycardia:
Heart rate > 100 bpm.
ECG shows QRS complexes closer together.
Heart beats abnormally fast.
Brachycardia
Heart rate < 60 bpm.
ECG shows QRS complexes further apart.
Heart beats abnormally slowly.
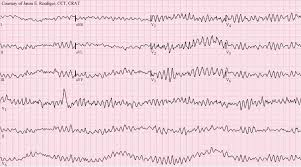
Fibrillation
Uncoordinated contraction of the heart muscle.
ECG appears irregular and chaotic.
Heart pumps blood less effectively.
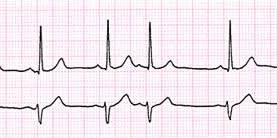
Ectopic Heartbeat
Extra heartbeat caused by excitation originating outside the SAN.
ECG shows an additional abnormal beat/wave between normal beats followed by long pause.
Often felt as a "missed" or "extra" heartbeat.
Oxygen Transport
Haemoglobin (Hb) in red blood cells binds oxygen reversibly (each of the 4 Fe2+ in each subunit binds to 1 oxygen molecule).
In the lungs (high O₂ concentration):
Hb + 4O₂ ⇌ Hb(O₂)₄ (oxyhaemoglobin)
In respiring tissues (low O₂ concentration):
Oxyhaemoglobin dissociates.
Oxygen is released for aerobic respiration.
Carbon dioxide transport
~85% as hydrogencarbonate ions (HCO₃⁻) in the plasma.
~10% bound to haemoglobin as carbaminohaemoglobin (HbCO₂).
~5% dissolved directly in plasma.
Haemoglobin at respiring tissues
Respiring tissues release CO2
Carbonic Anhydrase:
An enzyme inside red blood cells.
Catalyzes: CO₂ + H₂O ⇌ H₂CO₃
Speeds up the conversion of carbon dioxide and water into carbonic acid.
Formation of Hydrogencarbonate Ions:
Carbonic acid is unstable and dissociates: H₂CO₃ ⇌ H⁺ + HCO₃⁻
Hydrogencarbonate ions (HCO₃⁻) diffuse out RBC into plasma and carried down the concentration gradient
Haemoglobinic Acid:
The H⁺ produced does not remain free.
It binds to haemoglobin: Hb + H⁺ ⇌ HHb
Forms haemoglobinic acid (HHb).
Prevents large decreases in blood pH acts as buffer (removes H+ ions).
Also helps haemoglobin release O₂ (Bohr effect) as HHb has a different shape to Hb so O2 affinity lowers.
Chloride Shift:
HCO₃⁻ diffuse from the red blood cell and enters the plasma.
This would make the red blood cell too positive.
Therefore Cl⁻ ions move into the red blood cell and maintains electrical neutrality; down the electrochemical gradient
Haemoglobin at lungs tissues
Reverse Chloride Shift:
Hydrogencarbonate ions (HCO₃⁻) diffuse from the plasma back into the red blood cell.
This would make the red blood cell too negative.
Therefore Cl⁻ ions diffuse out of the red blood cell and into the plasma, maintaining electrical neutrality.
Reverse Haemoglobinic Acid:
Oxygen binds to haemoglobin, reducing its affinity for H⁺ ions.
Haemoglobinic acid dissociates:
HHb ⇌ Hb + H⁺
Hydrogen ions are released from haemoglobin.
Reverse Formation of Hydrogencarbonate Ions:
The released H⁺ combines with HCO₃⁻:
H⁺ + HCO₃⁻ ⇌ H₂CO₃
Carbonic acid is reformed inside the red blood cell.
Reverse Carbonic Anhydrase:
Carbonic anhydrase catalyses:
H₂CO₃ ⇌ CO₂ + H₂O
Speeds up the breakdown of carbonic acid into carbon dioxide and water.
Oxygen Affinity
Oxygen Affinity
The tendency of haemoglobin to bind oxygen.
High affinity = haemoglobin loads O₂ easily.
Low affinity = haemoglobin releases O₂ easily.
Cooperative binding
Haemoglobin consists of 4 polypeptide subunits, each with a haem group that can bind one O₂ molecule.
The first O₂ molecule is difficult to bind because haemoglobin initially has a low affinity for oxygen.
Binding of the first O₂ causes a change in haemoglobin's tertiary structure (conformational change).
This increases the affinity of the remaining subunits, making the second and third O₂ molecules easier to bind.
By the time the fourth O₂ molecule binds, few binding sites remain available, so binding becomes less easy than for the second and third O₂ molecules.
This changing affinity during oxygen loading produces the sigmoid (S-shaped) oxygen dissociation curve.
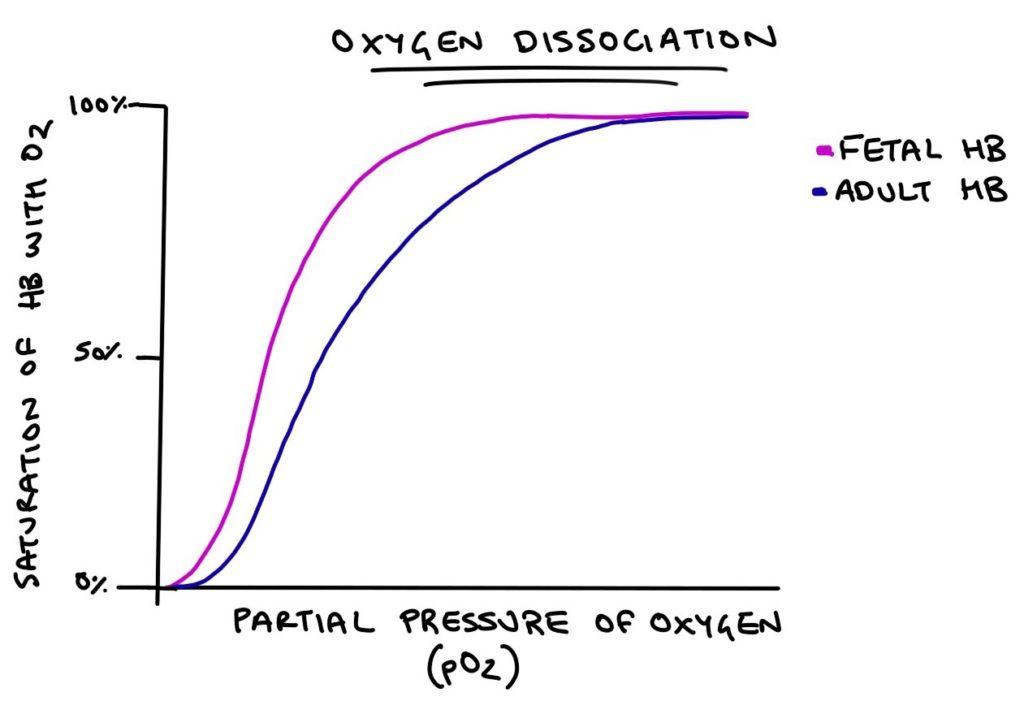
Oxygen Dissociation Curves
Relationship between:
Partial pressure of oxygen (pO₂) on the x-axis.
Percentage saturation of haemoglobin on the y-axis.
Shape of the Curve
Low pO₂: low saturation (few O₂ molecules bound).
Middle section: steep increase due to cooperative binding.
High pO₂: plateaus as haemoglobin becomes fully saturated.
Adult vs Fetal Haemoglobin
Fetal Haemoglobin
Curve is shifted left of adult haemoglobin.
Has a higher affinity for oxygen.
Loads O₂ at lower pO₂ values.
Allows fetal haemoglobin to remove oxygen from the mother's blood across the placenta.
Adult Haemoglobin
Lower affinity than fetal haemoglobin.
Releases oxygen more readily to tissues.
Bohr Effect
Respiring tissues produce CO₂.
CO₂ enters red blood cells and produces H⁺ ions, lowering pH.
H⁺ binds to haemoglobin, reducing its affinity for O₂ as changes it tertirary shape.
Oxyhaemoglobin dissociates more readily.
More O₂ is released to respiring tissues.
High CO₂ concentration → right shift of the dissociation curve.
Lower O₂ affinity.
More O₂ unloaded at a given pO₂.
Low CO₂ concentration (lungs) → left shift of the dissociation curve.
Higher O₂ affinity.
More O₂ loaded at a given pO₂.