lesson 1 cardiomyopathies
1/31
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
32 Terms
WHAT IS CARDIOMYOPATHY? Affects what ages’s of population? is there a cure for CM? what dysfuncyion is assocatied with CM? All CM will lead to what?
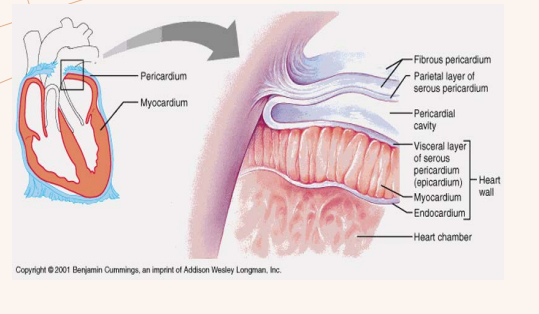
Disease of the heart muscle, specifically of the myocardium
Affects any age population
There is no cure but good treatments options available
Both systolic and diastolic dysfunction can be affected
All CM can lead to HF
what is the etiology (the cause of the disease) for cardiomopathy? and what its origin?
Idiopathic (without an identitiy, we dont know what caused it and not a result of another disease)
(there can be both genetic and nongetic origin)
Nongenetic Origin ( can from bio effections, automine disease, expsoure to toxins, pregrancy’s?) - secoundary causes
Familial Transmission, name 3
Autosomal Dominant
Autosomal Recessive
Sex linked
familial transmission:
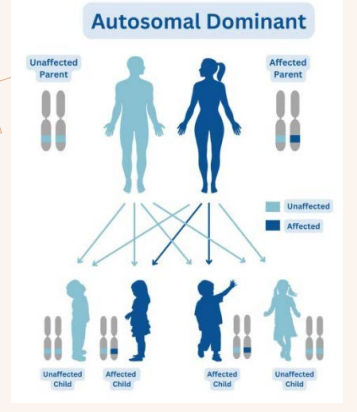
DEFINE AUTOSOMAL DOMINANT
An individual will only need to get an ………… …………from …………parent to ……….the ………..
what is the % chance of the child getting the ………
An individual will only need to get an abnormal gene from ONE parent to inherit the disease.
(50% chance of the child getting the gene)
familial transmission:
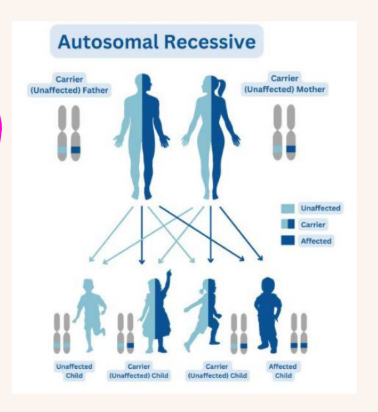
Define AUTOSOMAL RECESSIVE TRAIT
an individual born to who what? Has a what chance of getting the malfunctioning genes from ___ _______ and developing the disease?
An individual has a ___in ____ chance of inheriting one abnormal gene
An individual born to parents who BOTH carry an autosomal recessive disease
change (mutation) has a 1 in 4 chance of getting the malfunctioning genes from both
parents and developing the disease
An individual has a 2 in 4 chance of inheriting one abnormal gene
1 out of 4 children (25%)
→ can inherit BOTH abnormal genes
→ and have the disease2 out of 4 children (50%)
→ inherit only ONE abnormal gene
→ they are just carriers
→ they usually do NOT have the disease1 out of 4 children (25%)
→ inherit NO abnormal genes
→ completely normal
Describe the SEX LINKED : X-LINKED (DOMINANT) for the father?
The Father: (X+)(Y)
The father with the X+ will always give the disease to the daughters and never to the son
Describe the SEX LINKED : X-LINKED (DOMINANT) for the mother?
The Mother: (X+)(X)
The mother with the X+ will have a 50/50 chance for all children
50% chance she passes the normal X
50% chance she passes the abnormal X+
That means:
EACH child has a 50% chance of getting the abnormal gene.
BOTH sons and daughters each have a 50% chance of inheriting the abnormal X from the mother.
each pregnancy has a 50% probability.
what are the 4 WORLD HEALTH ORGANIZATION: WHO 1996 CLASSIFICATION?
and name another 2
and please name for the 4 what AMERICAN HEART ASSOCIATION: AHA’S CLASSIFICATION OF
CARDIOMYOPATHY:
Dilated Cardiomyopathy
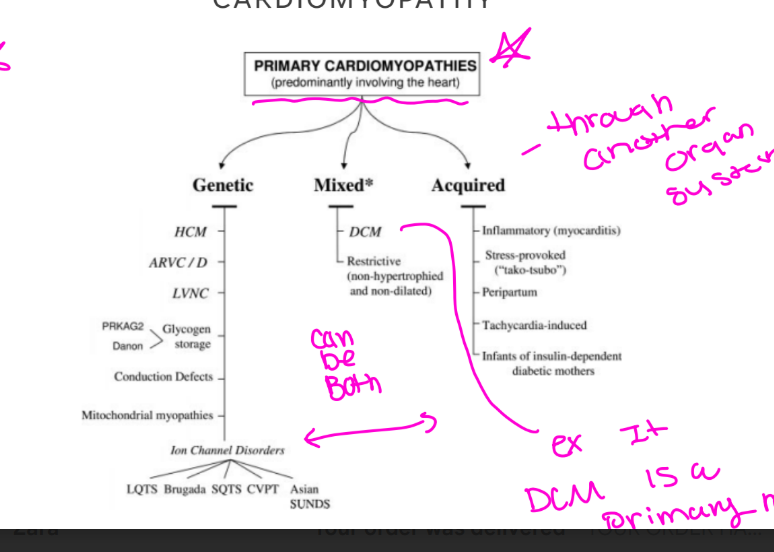
this is a primary cardiomyopathies (predominantly involving the heart) MIXED
Hypertrophic cardiomyopathy
this is a primary cardiomyopathies (predominantly involving the heart) GENETIC
Restrictive cardiomyopathy
this is a primary cardiomyopathies (predominantly involving the heart) MIXED (non-hyperthrophied and non - dilated)
Arrhythmogenic Right Ventricular Cardiomyopathy (ARVD/C)
this is a primary cardiomyopathies (predominantly involving the heart) GENETIC
5. Unclassified cardiomyopathy
6. Specific cardiomyopathy
Unclassified cardiomyopathy… name 4
• Fibroelastosis •
Noncompacted myocardium (LVNC) •
Systolic dysfunction with minimal dilatation •
Mitochondrial involvement
Specific cardiomyopathy….. name 10
Ischemic cardiomyopathy •
Valvular Cardiomyopathy •
Hypertensive cardiomyopathy •
Inflammatory/Infective Cardiomyopathy •
Metabolic Cardiomyopathy •
General system disease •
Muscular dystrophies •
Neuromuscular disorders •
Toxic •
Peripartal
AMERICAN HEART ASSOCIATION: AHA’S CLASSIFICATION OF
CARDIOMYOPATHY, how does it classifiy DCM?
Primary cardiomyopathies , Mixed (can be both genetic and acquired)
what are the HEMODYNAMICS IN CARDIOMYOPATHY?
The study of forces involved in the circulation of blood •
Systolic • Diastolic
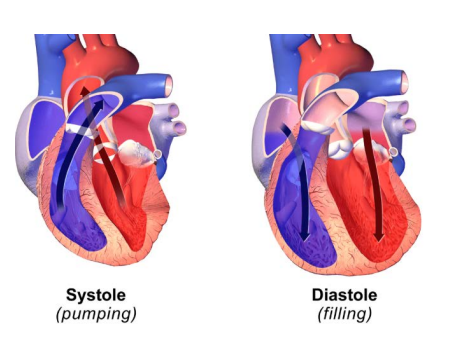
explain the HEMODYNAMICS: SYSTOLIC FUNCTION
• Contraction of the heart muscle •
Systole: The time the heart contracts
explain the HEMODYNAMICS: DIASTOLIC FUNCTION
Relaxation of the heart muscle •
Diastole: The period of relaxation of the heart muscle
explain preload
the degree that …………………….prior to
The degree that myocardial fiber is stretched prior to contraction
Preload, the ventricular wall tension at what cardiac cycle? And what is it Approximated by?
The ventricular wall tension at the end of diastole •
Approximated by the end-diastolic volume (EDV) or end-diastolic pressure (EDP)
This sentence is talking about preload. Your slide says preload is:
“the degree that myocardial fiber is stretched prior to contraction” and it is “approximated by the end-diastolic volume (EDV) or end-diastolic pressure (EDP).”
Here’s the simple version:
What is preload?
Preload basically means:
How full the ventricle is before it squeezes
or
How stretched the heart muscle is before contraction
Think of a Balloon
The more water you put into a balloon:
the more it stretches
The ventricle works similarly:
more blood filling it
= more stretch
= higher preload
What is End-Diastolic Volume (EDV)?
Diastole = filling phase of the heart.
So:
EDV = the amount of blood in the ventricle RIGHT BEFORE it contracts.
Bigger EDV:
more blood in ventricle
more stretch
more preload
What is End-Diastolic Pressure (EDP)?
As the ventricle fills with blood:
pressure inside rises
So:
EDP = pressure in the ventricle at the END of filling.
Higher EDP usually means:
the ventricle is fuller
or stiffer
and preload is higher
What does “approximated by” mean?
It means:
We cannot directly measure preload easily.
So doctors/sonographers use:
EDV
orEDP
to ESTIMATE preload.
Super Simple Memory Trick Preload =
“How much blood is in the ventricle before squeeze”
EDV =
“How much blood volume is there?”
EDP =
“How much pressure is there from filling?”
explain afterload
Resistance the ventricle must overcome to empty its contents
Afterload, Ventricular wall stress (pressure) that develops during what cardiac cycle?
Ventricular wall stress (pressure) that develops during systolic ejection
define Stroke Volume and the equation
Stroke Volume – the volume of blood pumped by the left ventricle of the heart in one contraction
• SV= EDV – ESV
define cardiac output and the equation
Cardiac Output- the volume of blood that is pumped by the heart each minute • CO = SV x HR
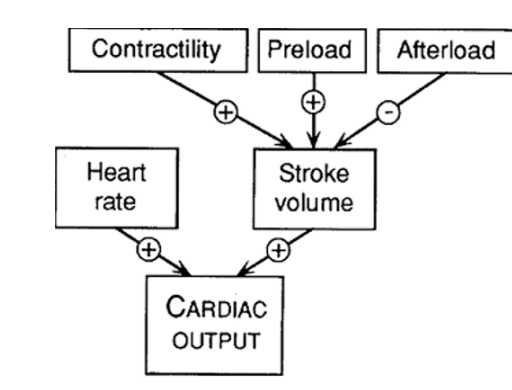
define contactility
Force generated by the myocardium when muscle fibers shorten
When contractility increases what happens with cardiac output?
When contractility increases, cardiac output increases
When contractility decreases, what happens with cardiac output?
When contractility decreases, cardiac output decreases
define HEART FAILURE and the affects it causes to the heart?
The inability of the heart to meet the metabolic demands of the body
Via systolic or diastolic dysfunction, and a decrease in CO
can you explain the steps for the Cardiac Performance?
what are the 4 PRIMARY CARDIOMYOPATHIES?
Dilated Cardiomyopathy
Hypertrophic Cardiomyopathy
Restrictive Cardiomyopathy
Arrhythmogenic Right Ventricular Cardiomyopathy
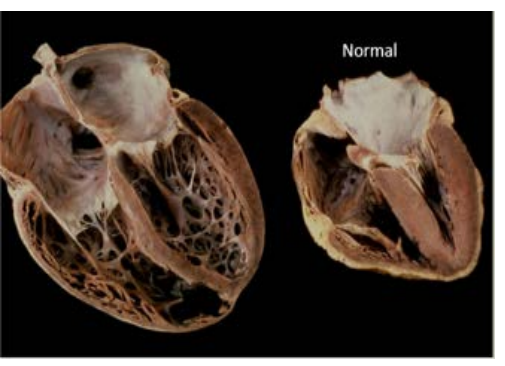
what is DILATED CARDIOMYOPATHY? what does it cause?
Dilation of the LV or RV
Causes systolic dysfunction and dilated ventricle
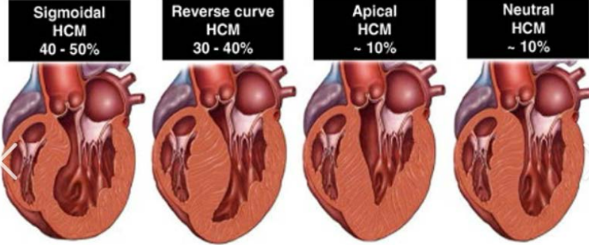
HYPERTROPHIC CARDIOMYOPATHY, what is it? (hint its disproportionate/abnormal….)
what dysfunction is this?
can be what or non?
what is the etiology of this? name 2
Disproportionate/abnormal hypertrophy of the LV and RV •
Diastolic Dysfunction •
Can be obstructive or non obstructive •
Idiopathic hypertrophic subaortic stenosis via muscular subaortic stenosis
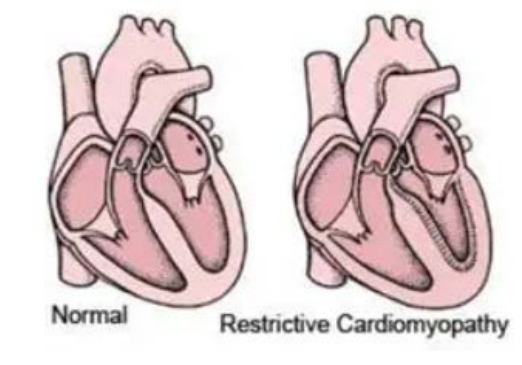
RESTRICITVE CARDIOMYOPATHY, define what this is ?
what does it restricts ?
what dysfunction is this?
Endomyocardial scarring affecting the LV and or the RV •
Restricts ventricular diastolic filling •
Marked diastolic dysfunction
(walls become stiff - not thick, have a hard time relaxig and filling ) (grade 3 diastolic dysfinction with restrictve CM)
(common to have a big atria on both the right and left side)
ARRHYTHMOGENIC (ARVD/C) CARDIOMYOPATHY, define what this is & resulting in what two things and what dysfunction?
Fibrofatty replacement of RV tissue resulting in wall thinning and aneurysm formation
RV dilatation and dysfunction
what is ECHO’S ROLE IN CARDIOMYOPATHY? Name 5
Identify in patient’s history •
History and signs and symptoms •
Family history •
Identify on echo •
Identify what needs to be focused on in a complete echocardiogram for certain cardiomyopathy
what does MOGES stand for?
