HEDC PAEDIATRIC DENTISTRY PERSPECTIVE
1/48
Earn XP
Description and Tags
history, examination, diagnosis, consent
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
49 Terms
outline paediatric challenges and considerations
think about why they have been referred
anxiety, past dental experience and cooperation (pre-cooperative VS cooperative)
completely new environment
child’s age and level of understanding and language
it may be a 3 or 4 way conversation if you have an interpreter and other family members present
outline communication and situational awareness in paediatric dentistry
first moments matter
use warm body language, soft tone, open expressions and smile
choose guiding phrases over questions that allow refusal
take time for gentle ice-breakers, nothing clinical for the first few minutes
situational awareness incl. time of yr e.g. ask about xmas plans, DOB close to holidays, uniforms, clothes
supporting child-centred care
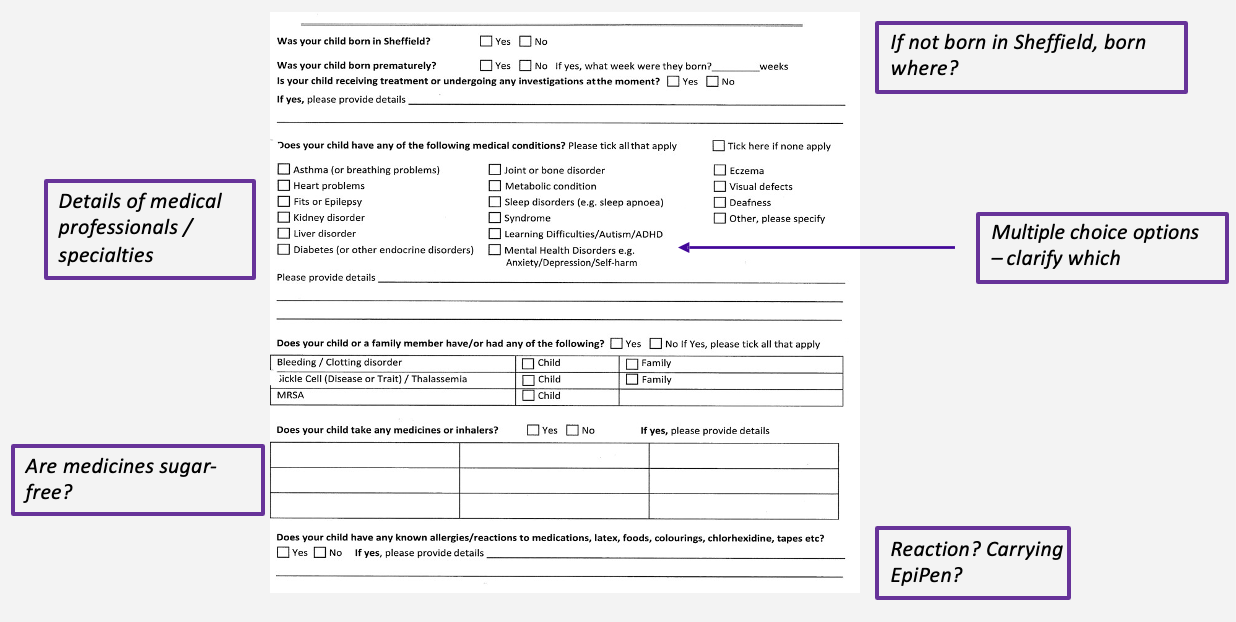
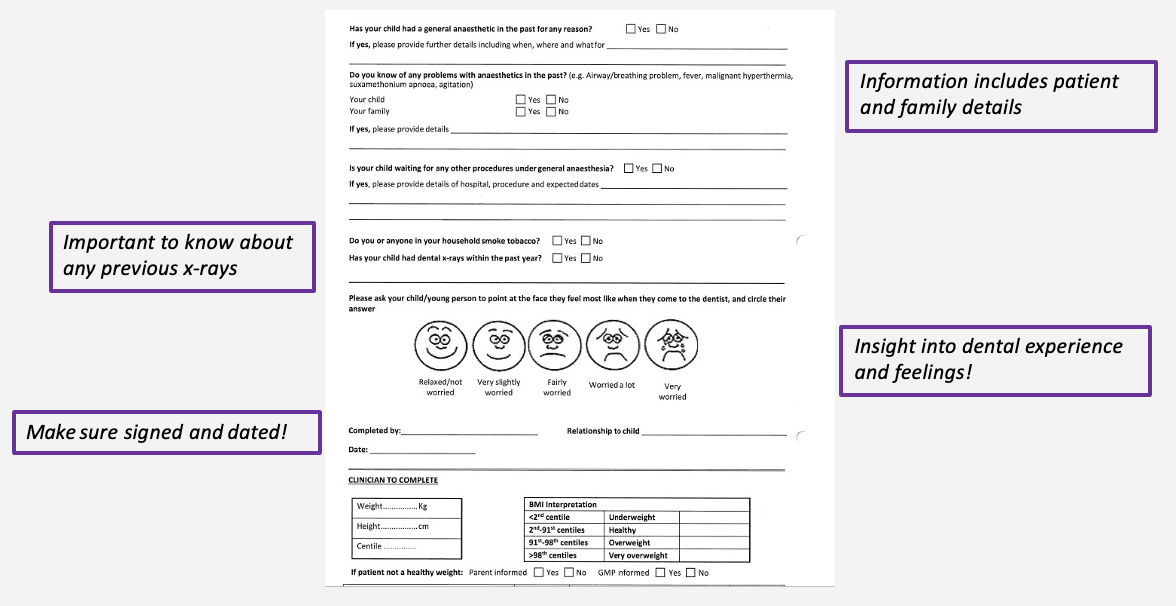
medical history forms
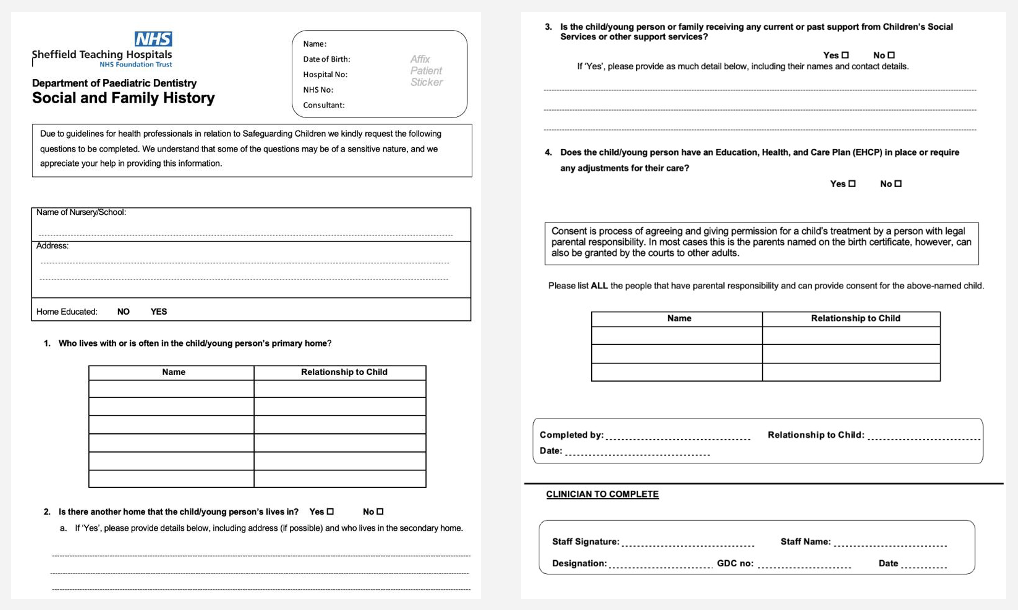
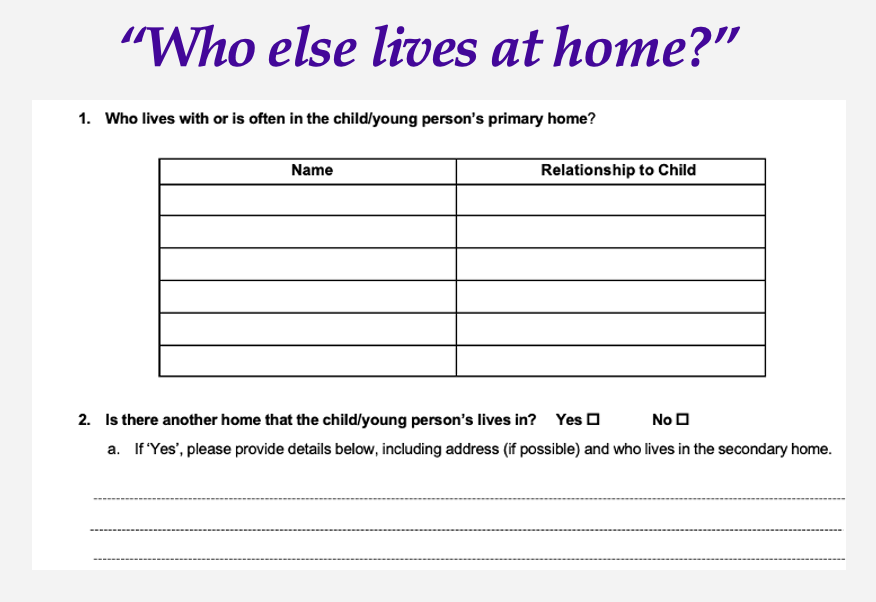
social and family history forms
education for children
if homeschooled, check with local authority
all children are entitled to an education under UN law
it is the legal responsibility of parents to ensure their children are receiving an appropriate full-time education
a record of a child’s school/ education provider is an important safeguarding check
post- COVID rise in no. of children being home-schooled
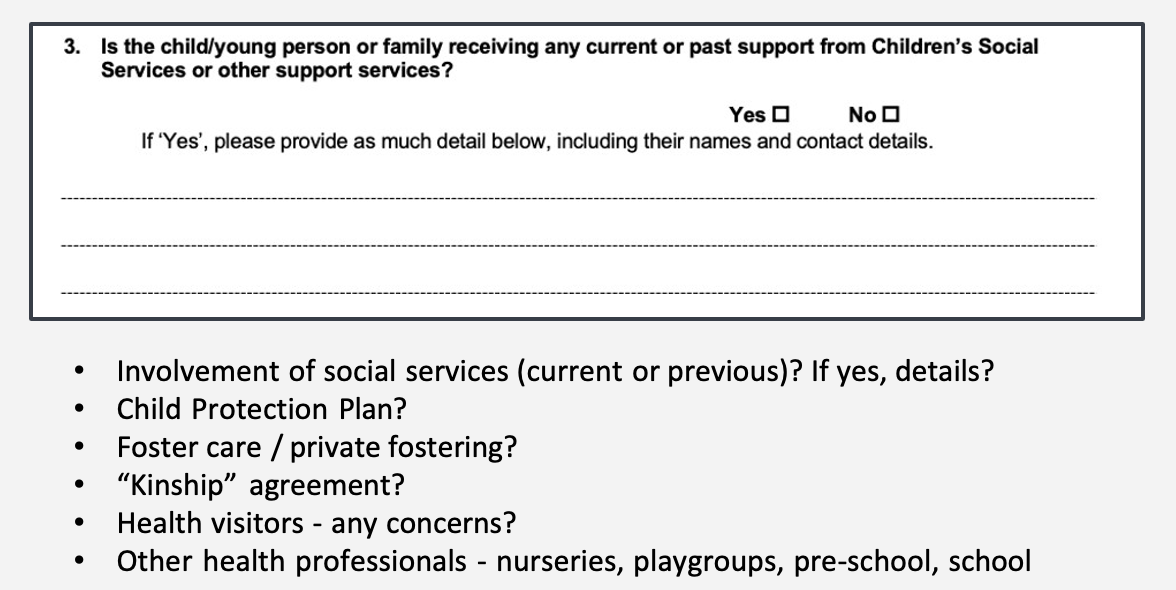
what is a kinship agreement
a family agreement not registered with social services e.g. if mother is not well the child will live with grandparents
family history: Children’s Social Services form
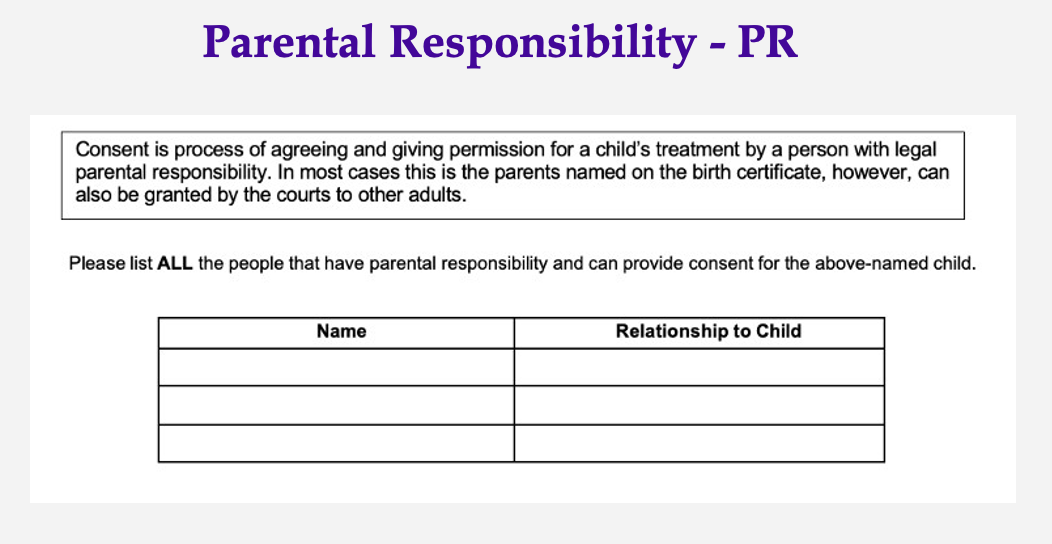
family history: parental responsibility form
dental history form
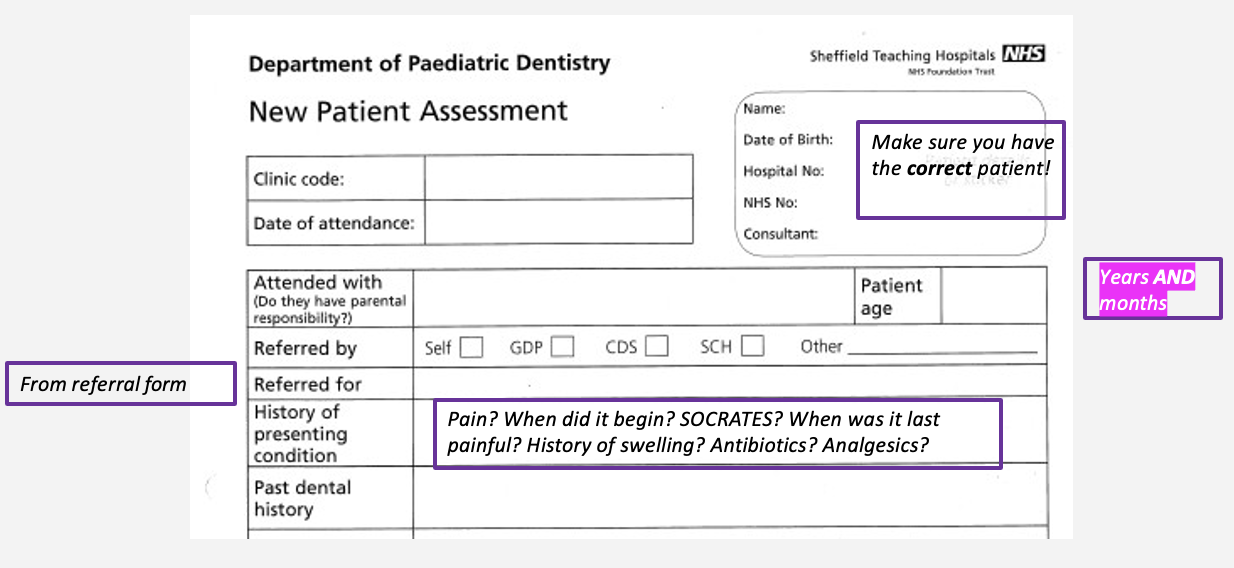
what else should you ask about pain history
is it affecting sleep, drinking/ eating
have they ever taken paracetamol or ibuprofen
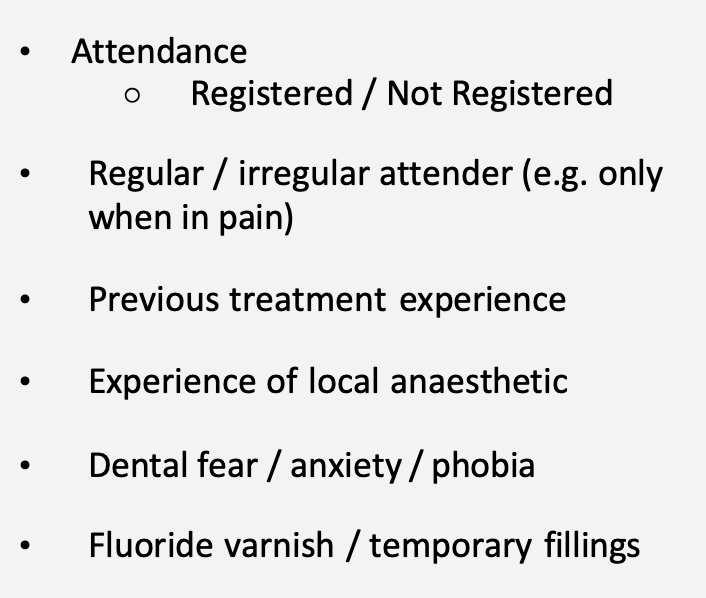
past dental history information
dental history form summary section
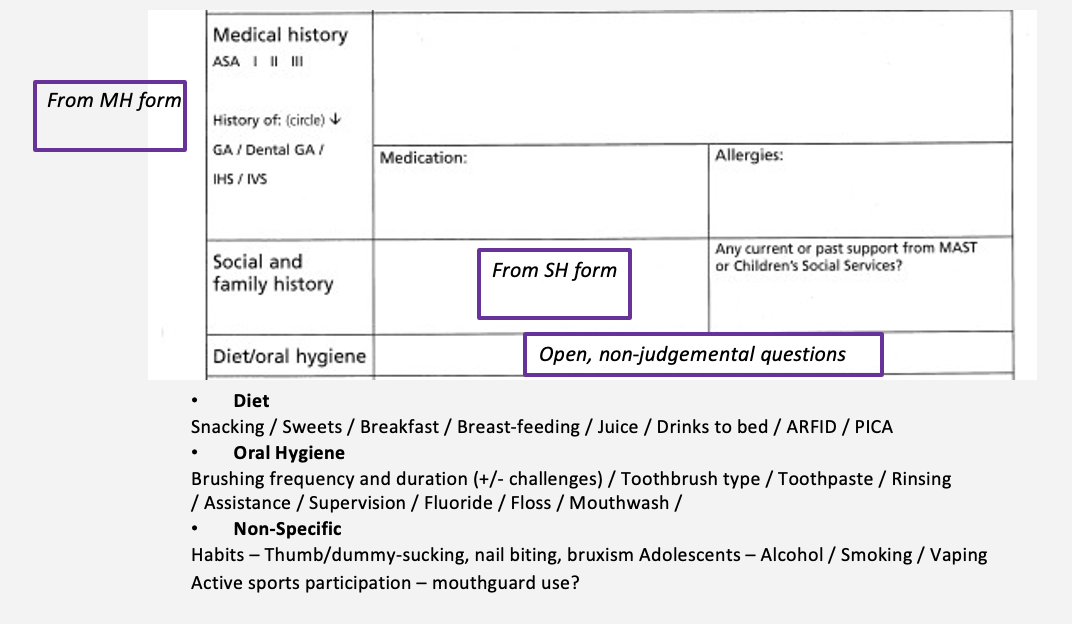
what is PICA
eating non-food items of no nutritional value e.g. gravel, sand
examination of paediatric patients in the waiting room
general appearance - do they look well, cleaned, cared for?
body language
gait
hair/ nails/ hands/ skin
growth - appropriate for age?
unexplained injuries - ask
anxiety
“you’re a bit messy today, what have you been up to”
transitioning from history taking to examination
“let’s have a look at those lovely teeth”
if you think a child is pre-cooperative and you will only get one look, what should you do
get the tutor over for 2 pairs of eyes
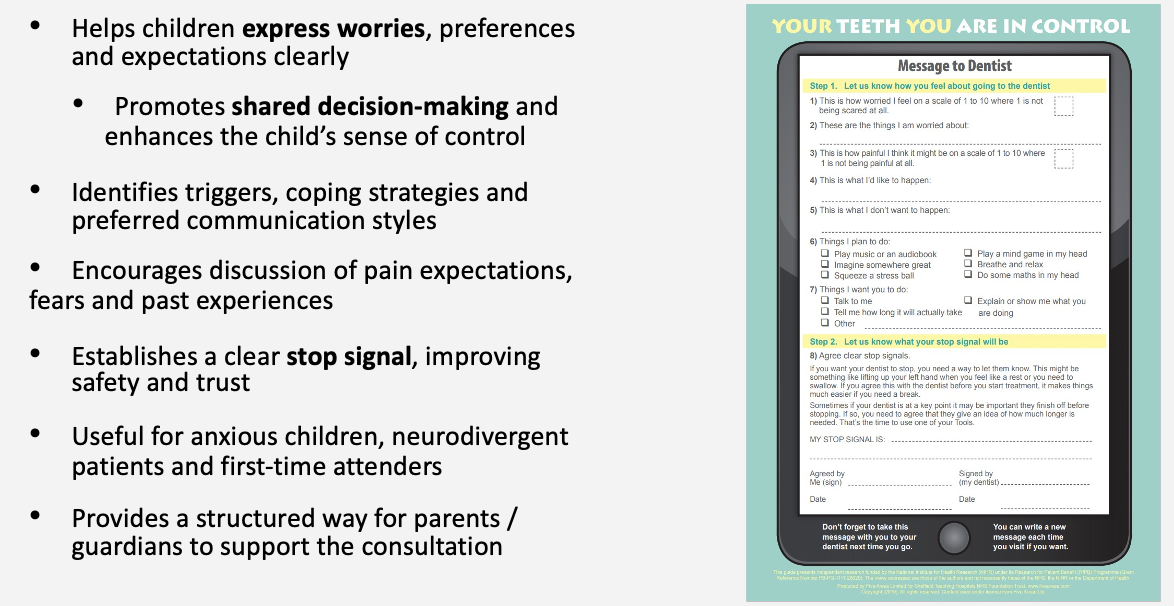
scene setting and support sheet

which instrument can be substituted in a paediatric patient
metal mirror » plastic mirror
childrenese
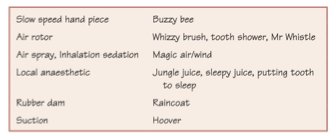
non-pharmacological behaviour support techniques
tell-show-do
enhancing control
positive reinforcement
distraction
modelling
voice control
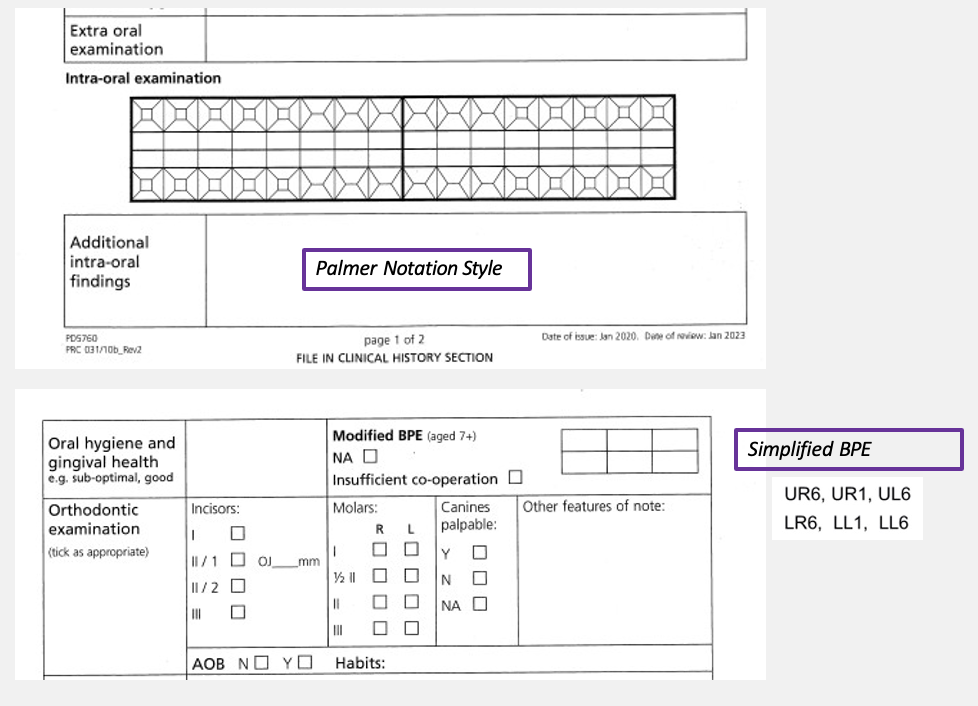
outline the simplified/ modified BPE
UR6
UR1
UL6
LR6
LL1
LL6
examination form
outline paediatric extra-oral examination
general appearance
skull and facial bones
swelling, lymphadenopathy
soft tissues
asymmetries/ facial dysmorphia
—
full extra oral exam is not necessary e.g. lymph nodes, TMJ unless they have been referred for it
what should you watch out for in children when examining them
head lice
important note for intra-oral examination
gentle air from 3in1
outline soft tissue intra-oral examination
tongue, FOM, palate, throat, buccal mucosa, lips
gingival condition - plaque index, BPE
oral cleanliness - fair, good, sub-optimal
pathology - ulceration, colour change, swelling
frenal attachment - high FA may lead to diastema
high FA = closer to lower arch
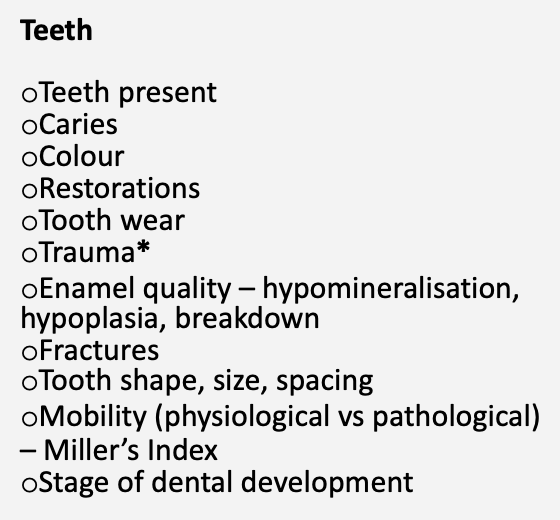
intra-oral examination: teeth
intra-oral examination: trauma
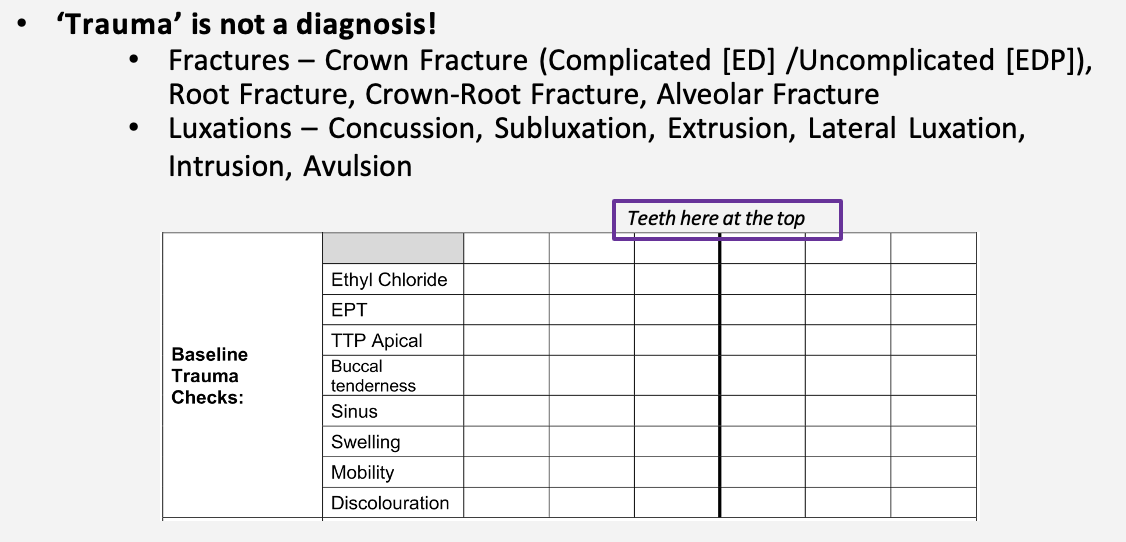
what does the tenderness of the buccal sulcus tell you about
root fracture
intra-oral examination: occlusion/ orthondontics
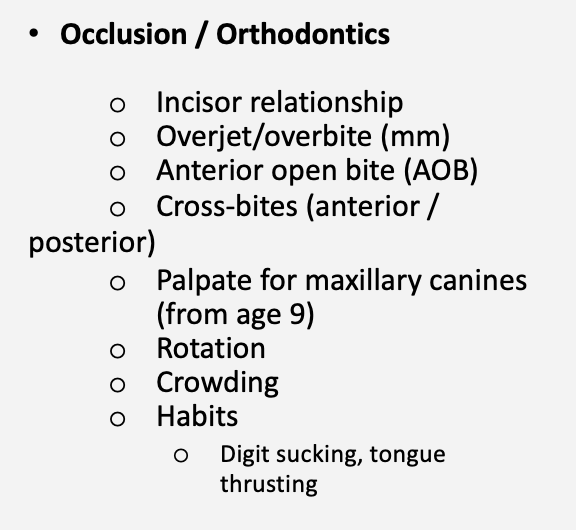
what to do if you encounter an AOB
measure AOB overjet
note down anything over 6mm
radiographic investigation
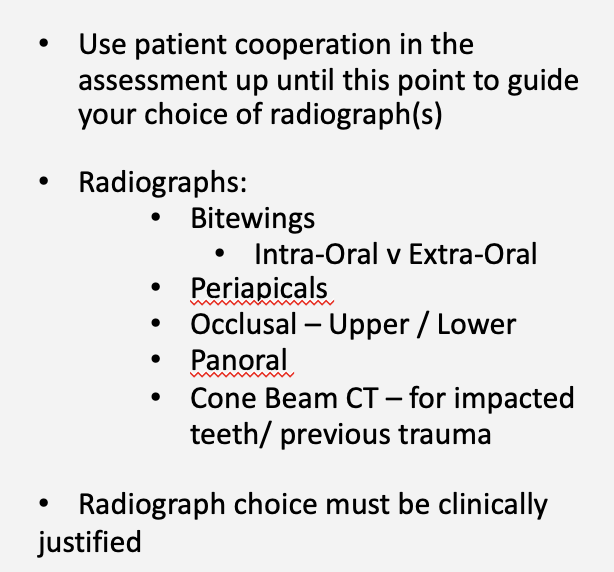
patient cooperation and choice of radiograph
good cooperation = intraoral radiograph
sort of cooperative/ pre-cooperative = extraoral style bitewings
can you see caries on a radiograph
NO - you can only see a radiolucency consistent with caries
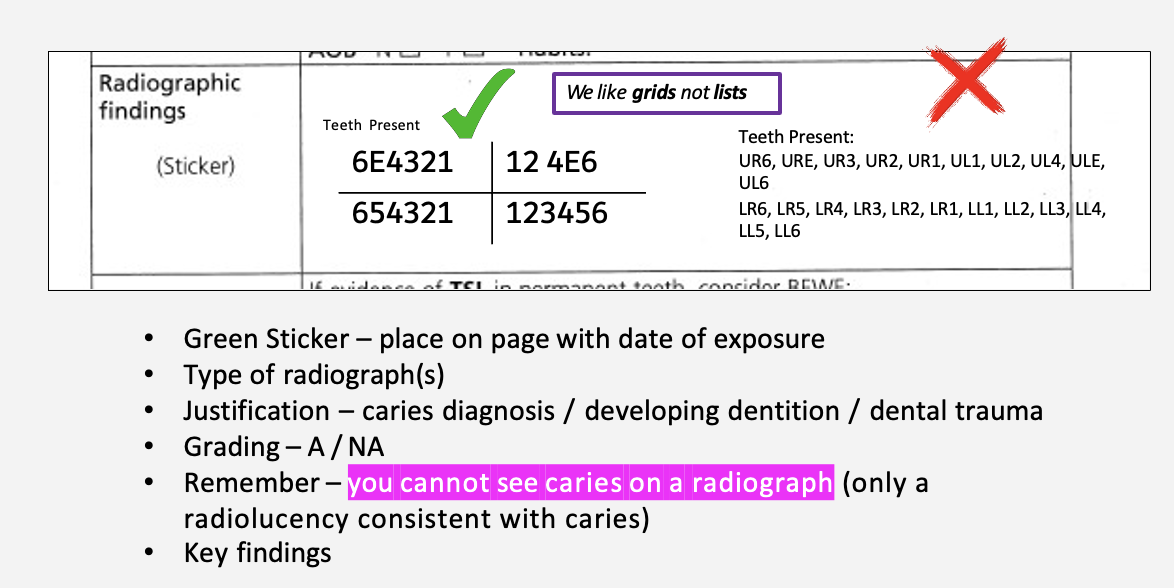
radiographic reporting
outline special investigations
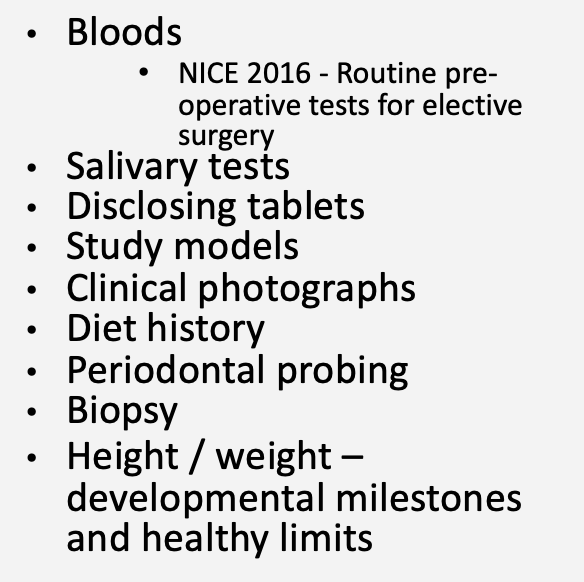
risk assessment
how many carious teeth does it take to be considered ‘high caries risk’
it takes 1 carious tooth to be at a high risk of caries
risk assessment form
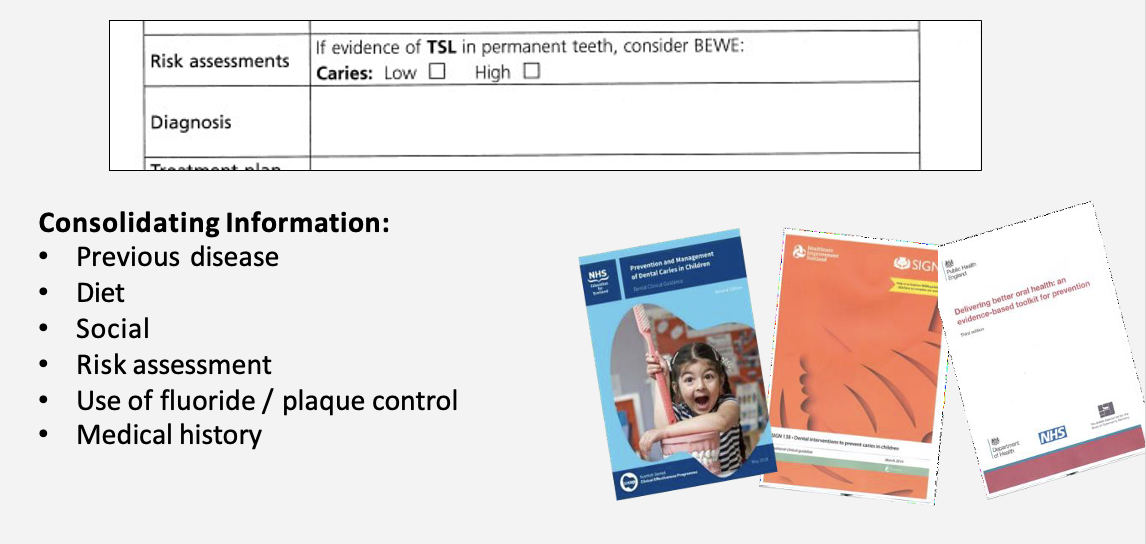
diagnosis form
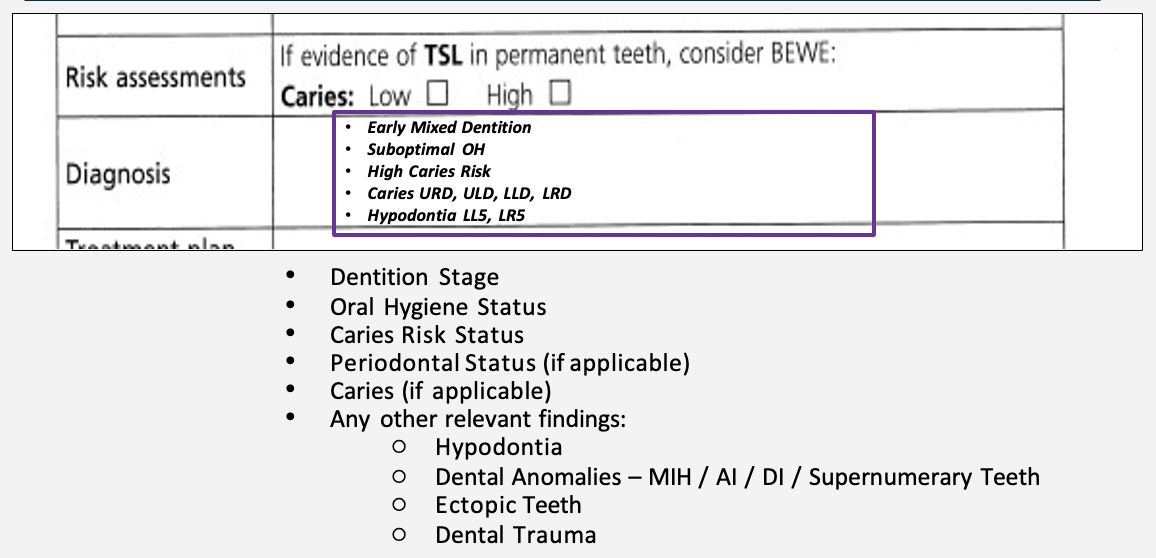
diagnosis and treatment planning
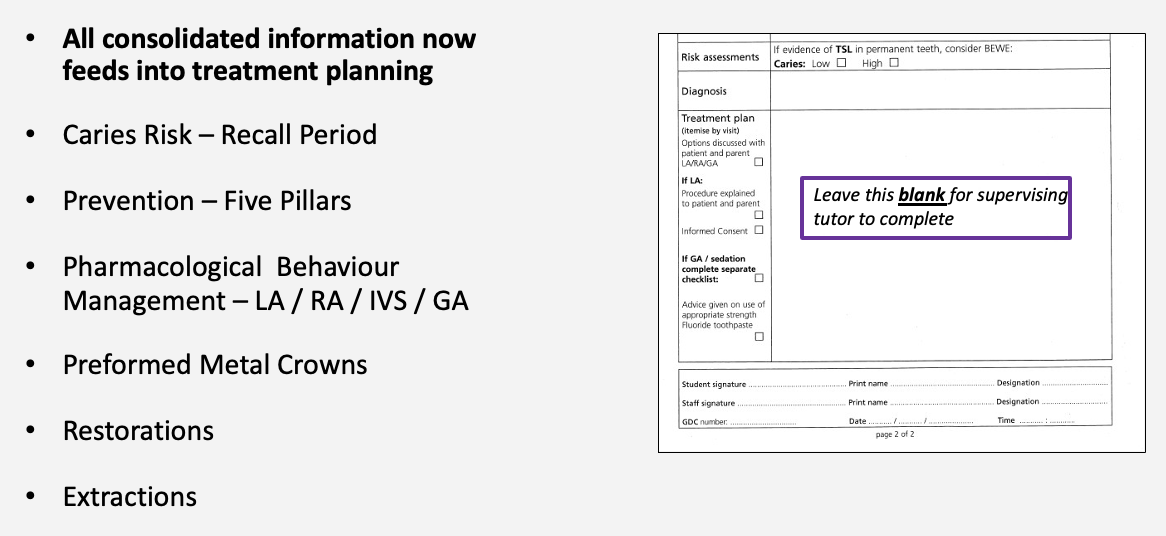
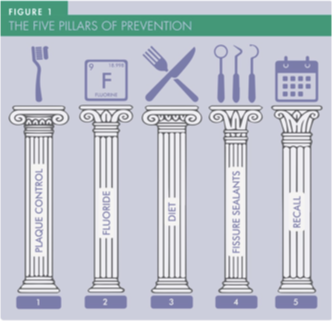
what are the five pillars of prevention
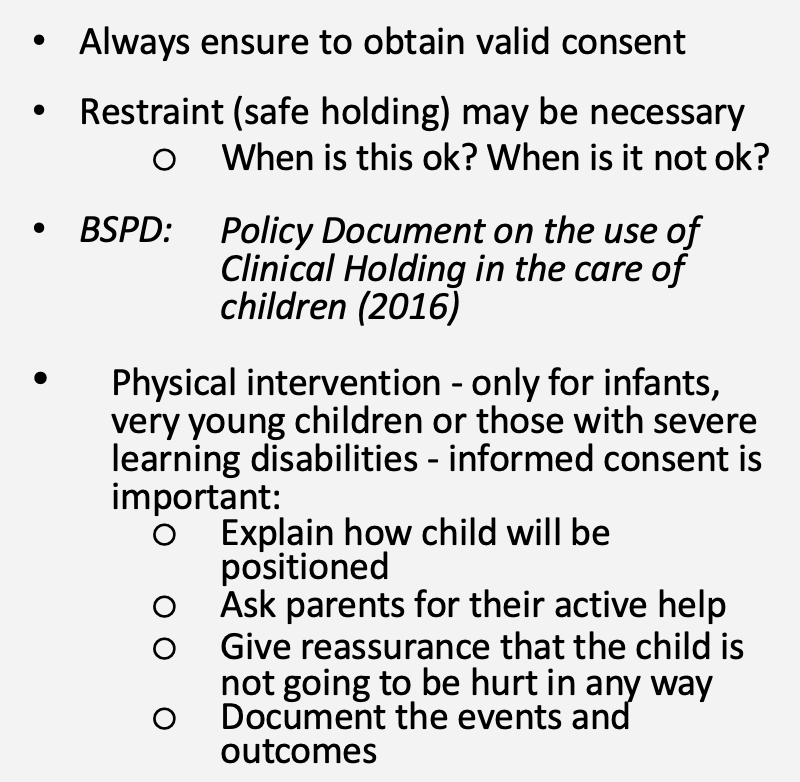
consent for children and young people
basic principles of paediatric consent
the consent form should itemise specific items of treatment and state whether primary or permanent teeth are involved
on occasion, definitive plans may depend on a further examination and radiographs under general anaesthetic if the patient is unable to manage an examination on clinic
input of child is encouraged where appropriate
in what situations may parental consent be null
parental consent may not be possible in an emergency or where parents disagree with life-saving treatment for their child
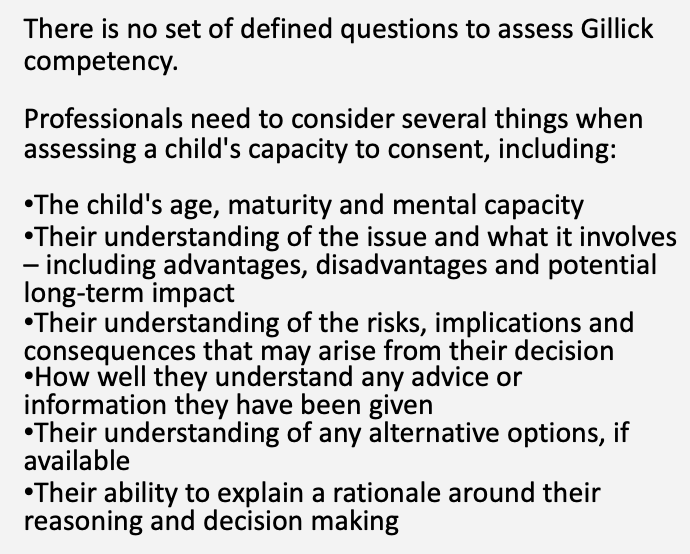
a young person may give their own consent if considered what
Gillick Competent
assessing Gillick Competence