14. Surgical diseases of the oesophagus. Hiatal hernia. Esophageal feeding tubes.
1/78
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
79 Terms
What are the three parts of the oesophagus?
Cervical (lies to the left of the midline)
Thoracic (in mediastinum, between v. cava cranialis and aorta)
Abdominal (very short)
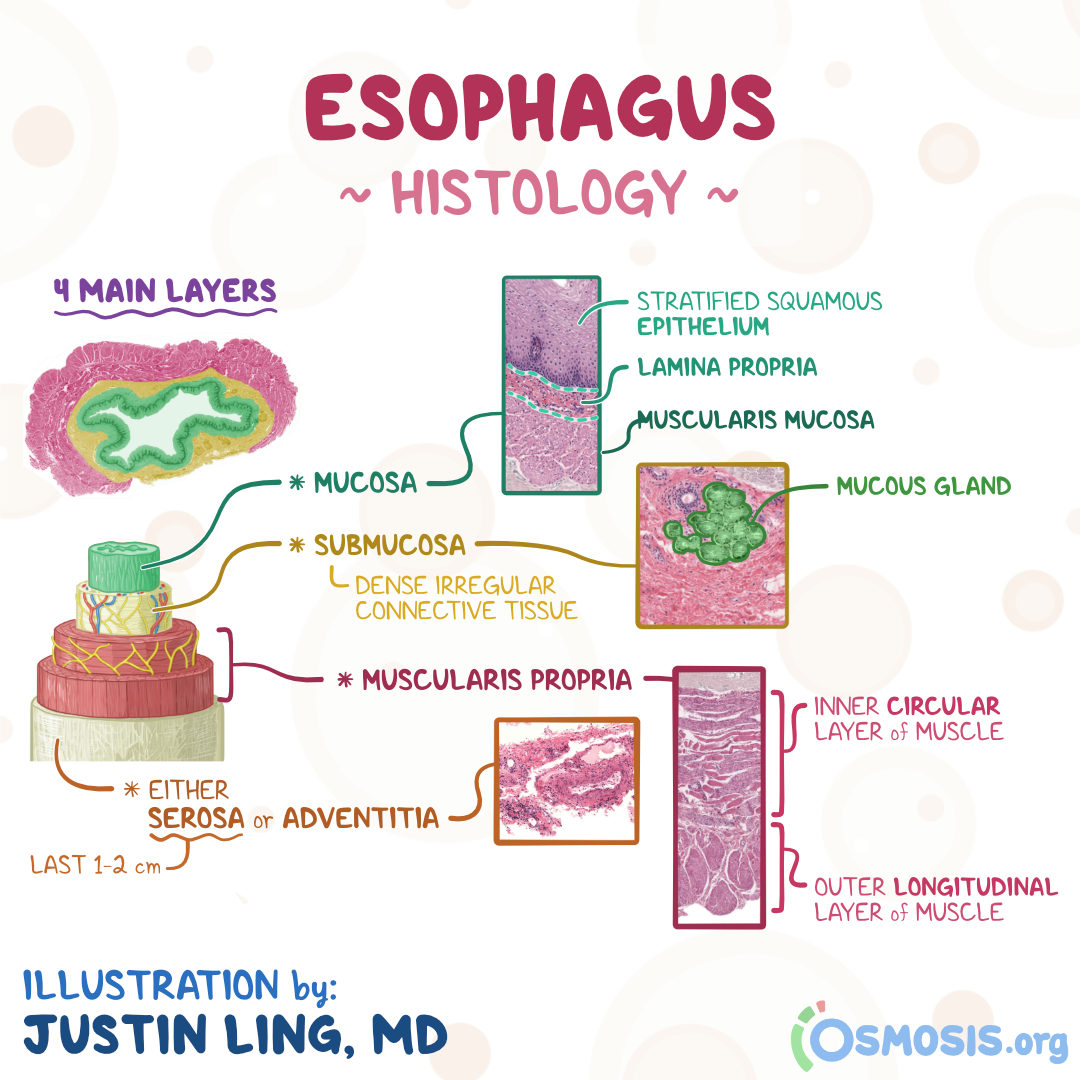
What are the four layers of the oesophagus?
Mucosa, submucosa, muscularis, and adventitia. NO SEROSA
Which muscle layers are not incised during oesophageal surgery and why?
The inner circular muscle layers, to prevent damaging the submucosal blood supply.
What is bougienage?
Dilation of a stricture using a probe or dilator of gradually increasing diameter.
Which approaches require lateral thoracotomy?
Cranial thoracic and caudal oesophagus.
Where is the incision for lateral thoracotomy for access to the cranial thoracic oesophagus?
Choose an appropriate intercostal space according to radiographic location of the abnormality
How is a lateral thoracotomy closed?
Place thoracostomy tube 1-2 ICS caudally to incision, or remove air with catheter after rib apposition and muscle closure
Preplace 4-8 heavy monofilament absorbable sutures around ribs adjacent to incision
Use rib approximator/assistant to appose ribs while tying sutures
Suture serratus ventralis, scalaneus, and pectoralis muscles with simple continuous
Appose edges of latissimus dorsi muscle with simple continuous
Remove air
Close subcutaneous tissue routinely
Where is the incision for access to the oesophagus at the heart base?
4th or 5th intercostal space (dissect and retract azygos vein for adequate exposure)
What is the approach for cervical oesophagotomy?
Dorsal recumbency, midline cervical incision beginning at larynx and extending to manubrium.
What structures must be carefully avoided during cervical oesophagotomy?
Thyroid gland and carotid sheath (carotid artery, vagus nerve, and jugular vein).
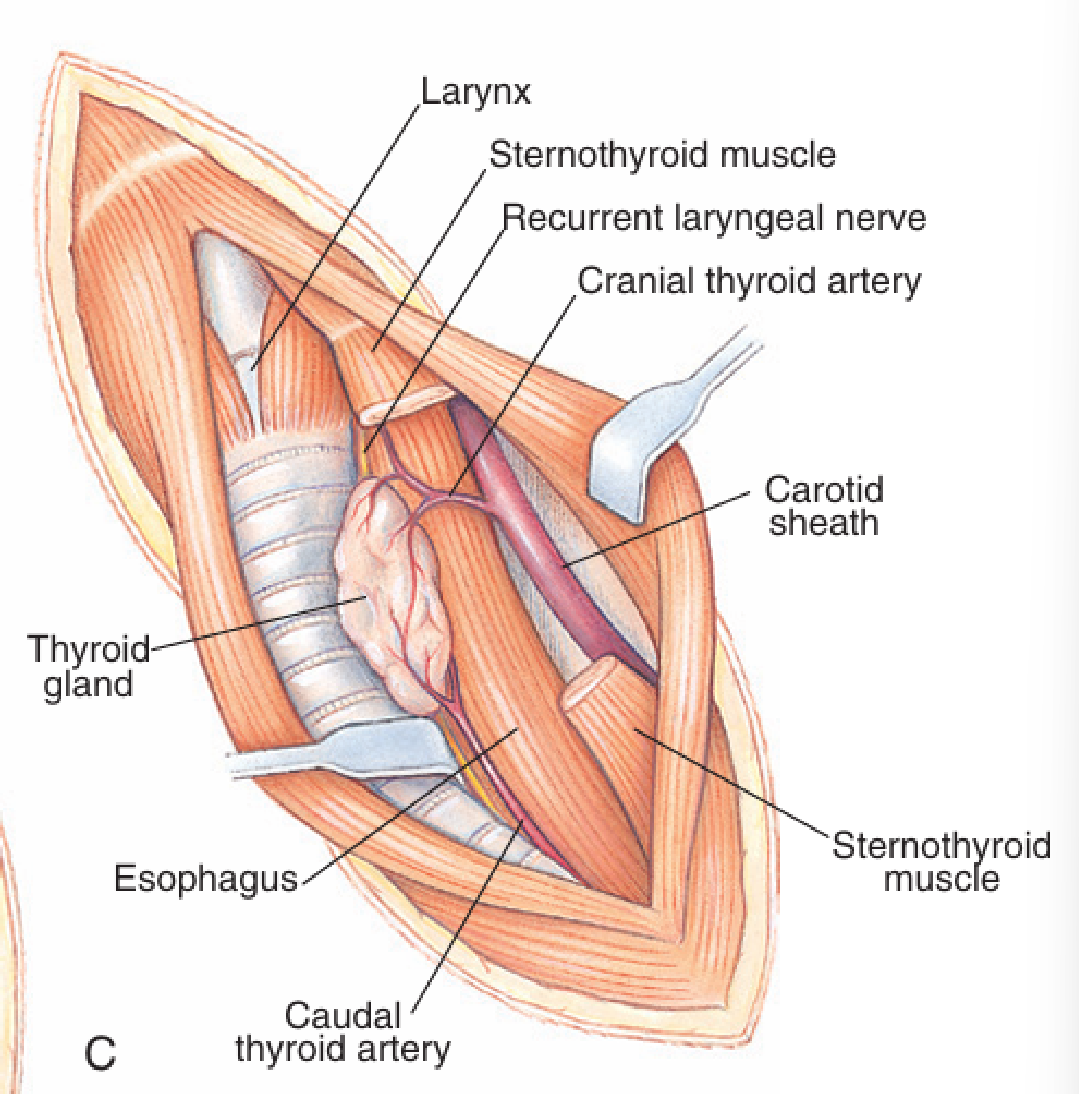
What is the procedure for cervical oesophagotomy?
Move trachea to the right.
Retract the paired sternohyoid and sternocephalicus muscles
Pack off oesophagus from the rest of the surgical field via moistened laparotomy swab OR simply place two stay sutures above & below (optionally on left & right)
Stab incision into oesophagus w/ scalpel blade & extend incision w/ scissors (on foreign body/caudally if trauma/necrosis)
Remove foreign body w/ forceps & examine oesophageal lumen for necrotic areas or perforation ⤍ treat if required
Suture oesophagus in 2 layers
1st layer: tunica mucosa & submucosa – simple interrupted (intra-luminal knot)
2nd layer: adventitia, muscularis & submucosa – simple interrupted (extra-luminal knot)
Sutures 2mm apart, following completion, check for leakage (saline but not performed in practise routinely)
Return trachea to normal position
Appose muscles & close incision using a simple continuous pattern
Appose subcutaneous tissue using a simple continuous pattern
Close skin using appositional suture pattern: simple continuous, simple interrupted, intradermal
What is the post-operative care after oesophagotomy?
IV fluids, nothing PO for 24-48 hours, water after 24 hours, soft food for 5-7 days, and antibiotics.
What are some complications of oesophagotomy?
Oesophagitis (due to gastric reflux, post-GA, or aspiration pneumonia)
Stricture formation (3-6 weeks post-op).
How are oesophageal disorders diagnosed?
X-ray with contrast (not barium if risk of rupture), fluoroscopy, endoscopy, CT, clinical signs, and history.
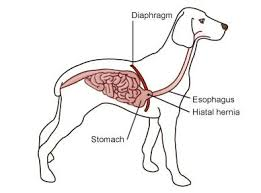
What is a hiatal hernia?
Protrusion of the abdominal oesophagus, gastro-oesophageal junction, and sometimes part of the stomach into the caudal mediastinum.
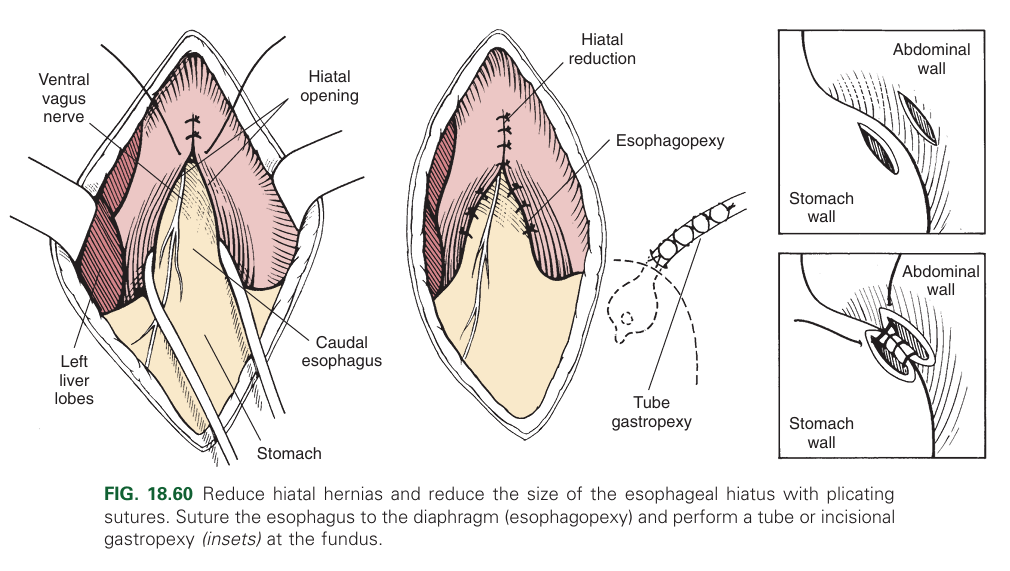
How is hiatal hernia treated?
Diaphragmatic hiatal reduction
Left side gastropexy (most important)
Diaphragmatic plication (flattening of the diaphragm).
What are examples of other oesophageal disorders?
Obstruction
Oesophageal muscular weakness
Megaoesophagus
Oesophagitis
Oesophageal foreign bodies
Stenosis/stricture
Neoplasia
Tracheoesophageal fistula
What are some causes of oesophageal obstruction?
Congenital (persistent right aortic arch)
Acquired (foreign bodies, strictures/stenosis, neoplasia).
What are some causes of oesophageal muscular weakness?
Congenital (idiopathic, achalasia)
Acquired (myasthenia, hyperadrenocorticism, severe oesophagitis, gastro-oesophageal reflux, myopathies, Spirocerca lupi, botulism/tetanus, lead poisoning, canine distemper, chemicals, and iatrogenic causes like doxycycline, clindamycin, and NSAIDs).
What is megaoesophagus?
Dilation of the oesophagus and loss of motility → food and liquid accumulation.
How is megaoesophagus treated?
Feeding in an upright position, and prokinetics.

What are some causes of oesophagitis?
Infectious agents (Spirocerca lupi)
Non-infectious causes (foreign bodies, gastric reflux, certain drugs, cancer, and caustic substances).
What are the clinical signs of oesophageal foreign bodies?
Regurgitation immediately after eating, difficulty swallowing, dyspnoea and hypersalivation.
How are oesophageal foreign bodies diagnosed?
History, X-ray with contrast, endoscopy, and palpation.
How are oesophageal foreign bodies treated?
Endoscopic removal via the mouth if not sharp or pushing into the stomach for surgical removal.
What are some causes of stenosis?
Functional (spastic, oesophagitis)
Mechanical
Compressive (enlarged lymph nodes, haematoma).
What are some causes of tracheo-oesophageal fistula?
Congenital (e.g., in Cairn Terriers)
Acquired (penetration by a foreign body).
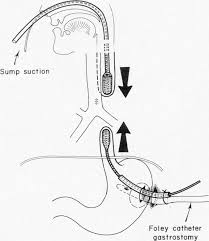
What are the types of feeding tubes?
Orogastric
Nasogastric
Oesophageal
Gastrostomy
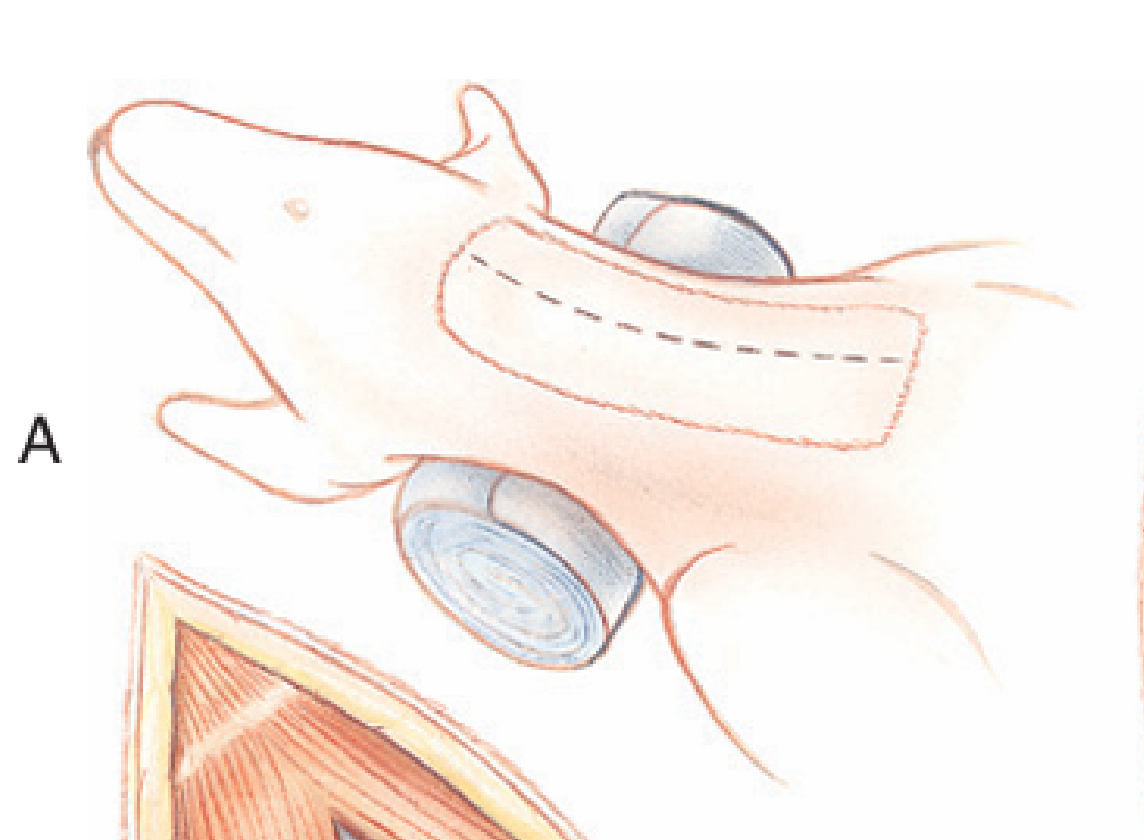
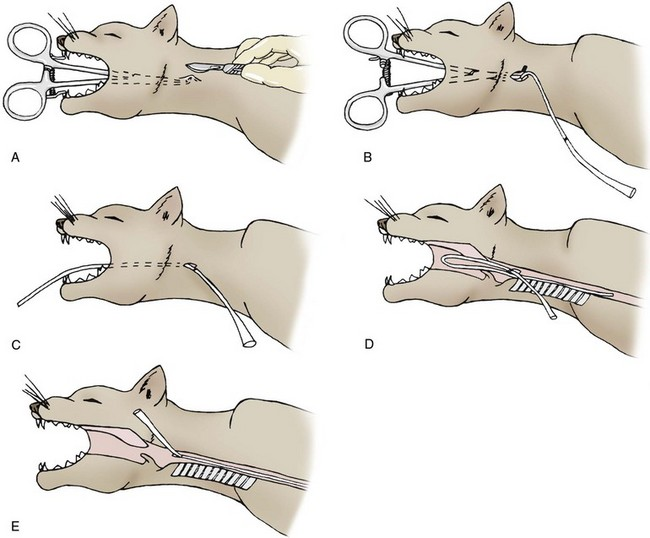
What is the method for inserting an oesophageal feeding tube?
Measure feeding tube from insertion point (mid cervical region) to level of 7th-8th ICS and mark it
Enlarge/make lateral opening/cut end of tube at oblique angle to encourage smoother flow of blended diet
Place curved tip of Rochester-Carmalt forceps through oral cavity into the oesophagus to the level of the left mid-cervical region (half way between mandible and shoulder)
Palpate the tip through the cervical skin, make a small incision and push forceps through oesophageal wall, sub cut and skin
Grab tube with forceps and pull out through the oral cavity
Redirect tube into the oesophagus, confirming placement by location of premarked area
Secure the tube to the cervical skin with a Chinese finger trap suture, loosely bandage the area and cap the end of the tube
How are animals fed through an oesophageal tube?
Small amounts of liquid food, followed by water