Fetal Abdomen an Genitourinary System
1/24
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
25 Terms
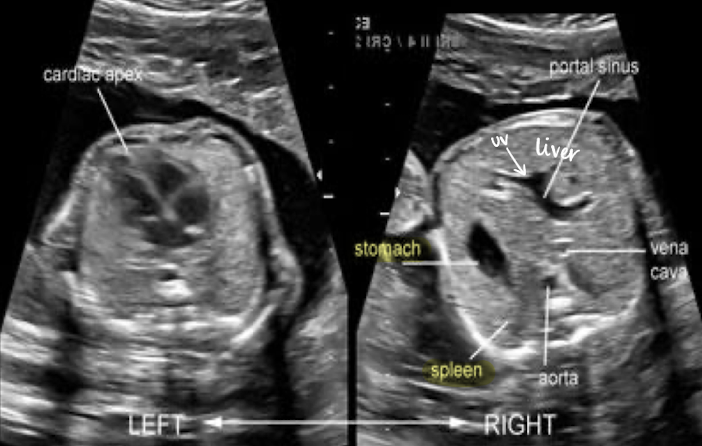
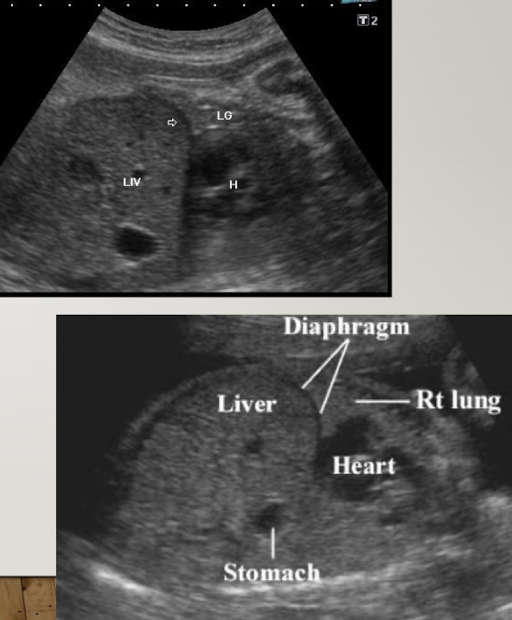
stomach
in LUQ
seen by 16w
amniotic, fluid-filled structure
if no fluid seen, evaluate 20-30 minutes
used as a marker for taking AC measurement
evaluating stomach
scanned in TRV plane (short axis)
anechoic (fluid-filled)
if stomach is empty, move on and come back later or have patient come back another day
can also image stomach and bladder together in LONG

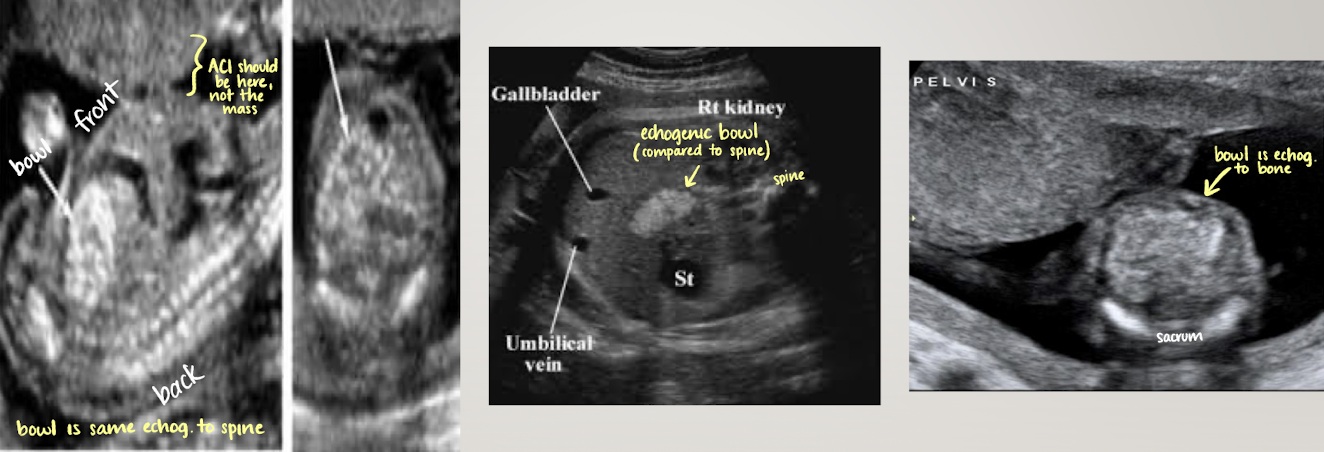
small bowel
mid-lower abdomen; centrally located echogenic areas inferior to liver
SONO: varies with menstrual age
mid gut herniation (<12wks)
early pregnancy=hypoechoic
late pregnancy=more echogenic
hyperechoic bowel is NOT normal
echogenicity should always be less than bone
may see peristalsis in 3rd trimester (normal)
abnormality?
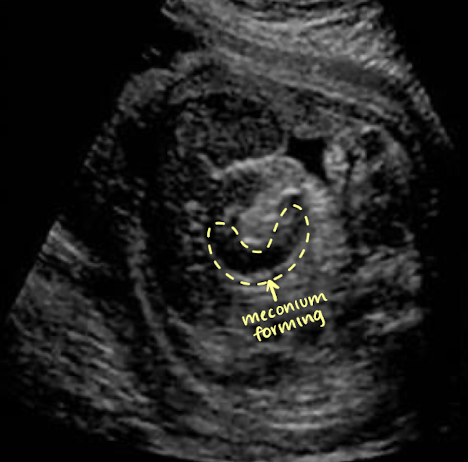
large bowel
seen after 22w (can discern between small and large)
more peripherally than small bowel
hypoechoic tubular structure (meconium)
meconium=baby stool
well-defined walls
haustral folds appear as thin linear echoes within lumen
liver
large compared to other abdominal organs
occupies upper right abdomen
left lobe is larger in utero
SONO:
homogeneous, moderate echogenicity
helpful for determining situs and obtaining AC measurement
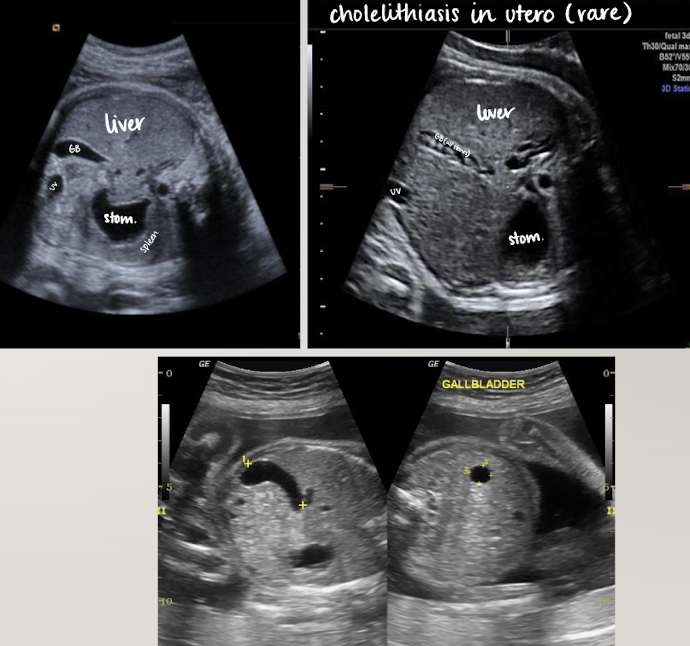
gallbladder
seen after 20 weeks
SONO: elongated anechoic structure in long-axis; circle in short-axis
in right abdomen near liver
more oval than intrahepatic umbilical vein
document presence
spleen
in LUQ
increases in size during gestation (biggest in 3rd trimester)
best images in TRV plane; to left of stomach
SONO:
homogeneous
similar echogenicity to kidney
less echogenic than liver

abdominal cord insertion (ACI)
becomes belly button after born
umbilical cord seen entering fetal abdomen just above level of bladder
UV courses to liver within falciform ligament
UAs course on either side of bladder
2VC can cause IUGR or is an indication of chromosomal abnormality
SONO:
image ACI with and without color Doppler
ensure smooth abdominal cord insertion (should be nothing “pooching” out)
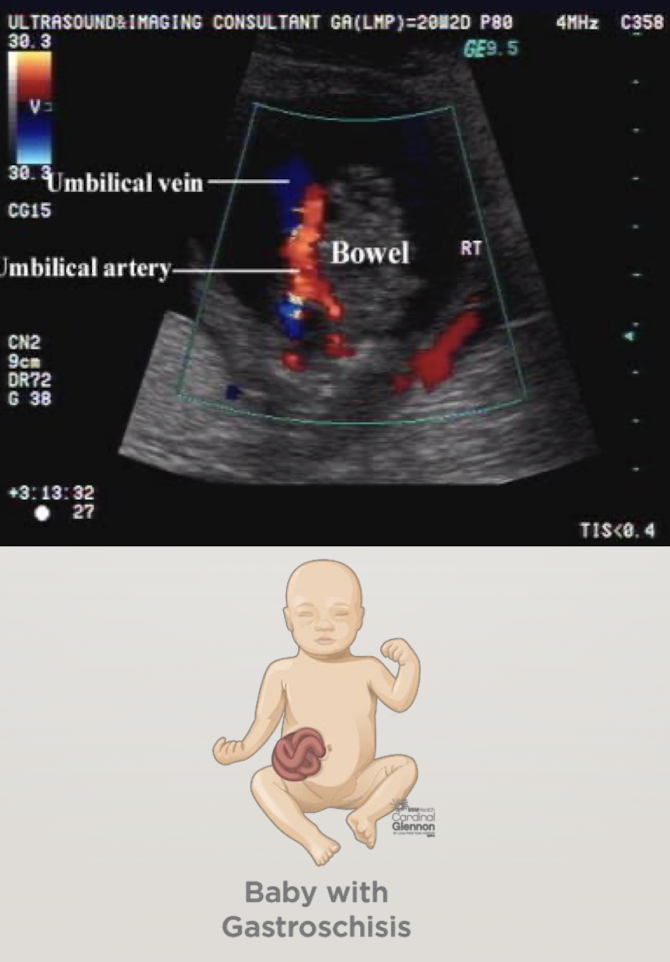
rule out gastroschisis and omphalocele

gastroschisis
“loose bowel pooching out—floating outside abdomen”
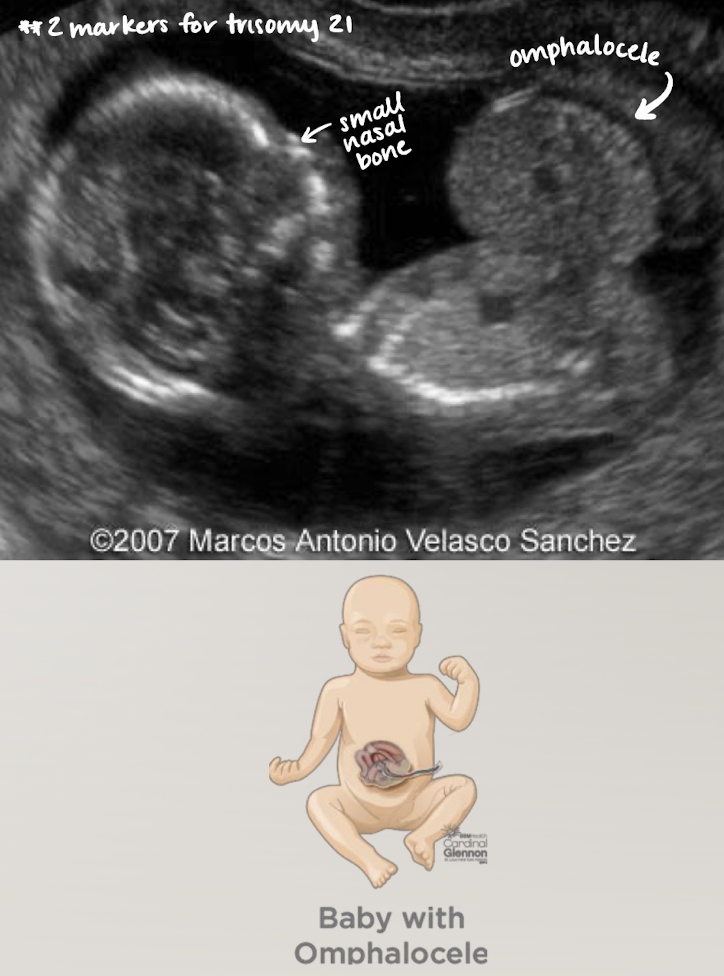
omphalocele
bowl or other organs come out, BUT difference is… it will be encased in a membrane
looks like a contained mass with smooth borders b/c of membrane
kidneys
kidneys form in pelvis and ascent into abdomen
urine formation around 11-2 weeks
excrete into amniotic cavity (component of amniotic fluid)
visible by 12-13wks
by 25wks distinction between renal cortex and sinus
must evaluate both kidneys
presence, number, position
size (is one bigger than the other?)
collecting system dilation (??hydro)
appearance (echogenicity; compared to liver and spleen)
**if hydro seen, measure renal pelvis (AP) in TRV plane
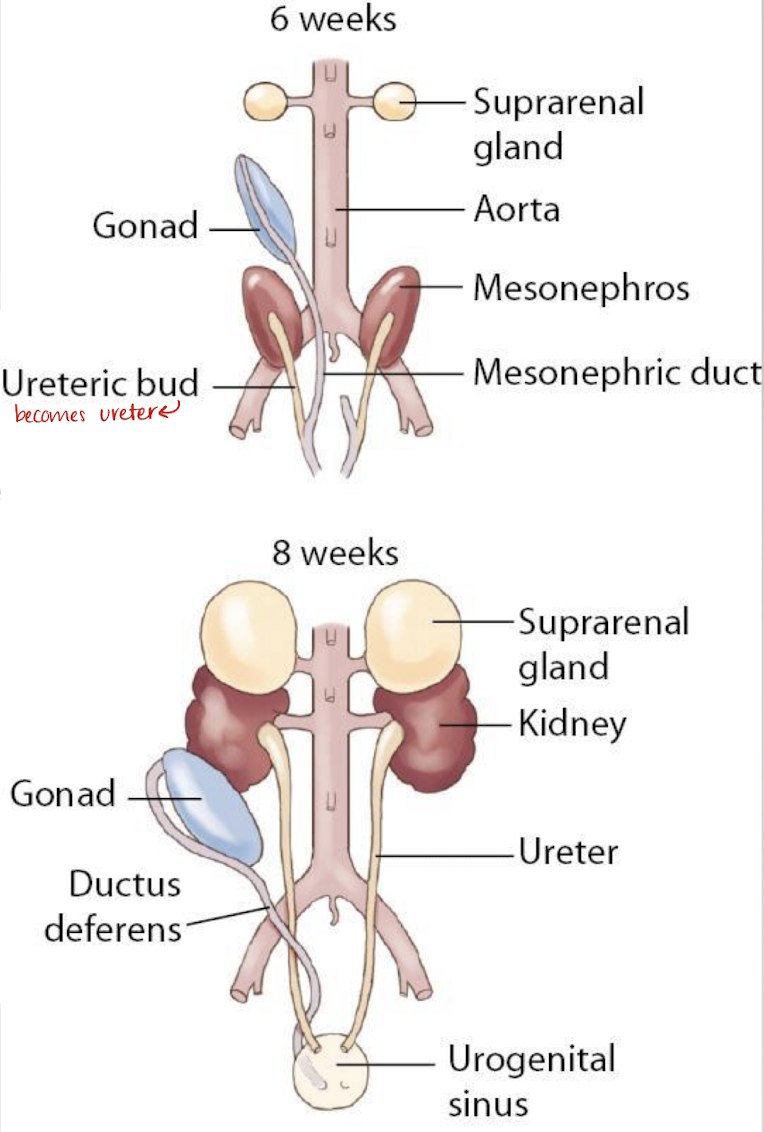
kidneys develop from what 3 excretory organs in embryo?
pronephros
mesonephros
metanephros
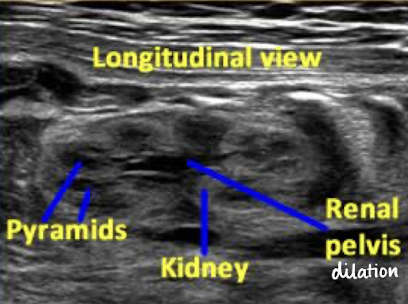
SONO: kidneys
homogeneous cortex
hypoechoic pyramids
anechoic collecting system

imaging the kidneys (TRV, SAG, coronal)
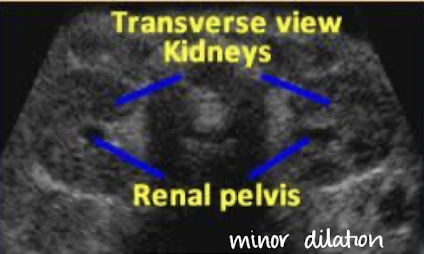
transverse (easiest plane)
kidneys visualized on either side of spine
measure AP diameter of renal pelvis
sagittal
long axis of kidney
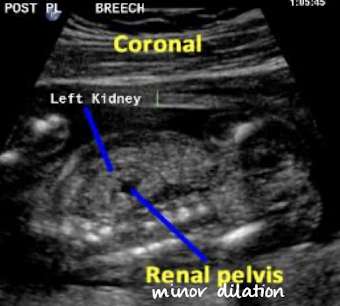
coronal
demonstrates a longer axis image of both kidneys
**always throw color Doppler on

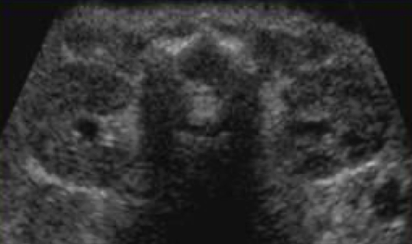
what plane was this taken in?
transverse

what plane was this taken in?
coronal
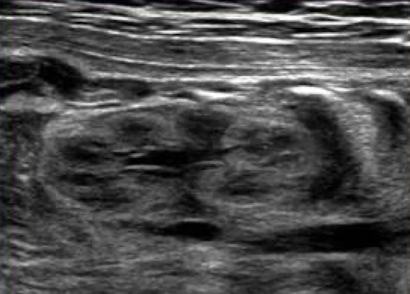
what plane was this taken in?
longitudinal
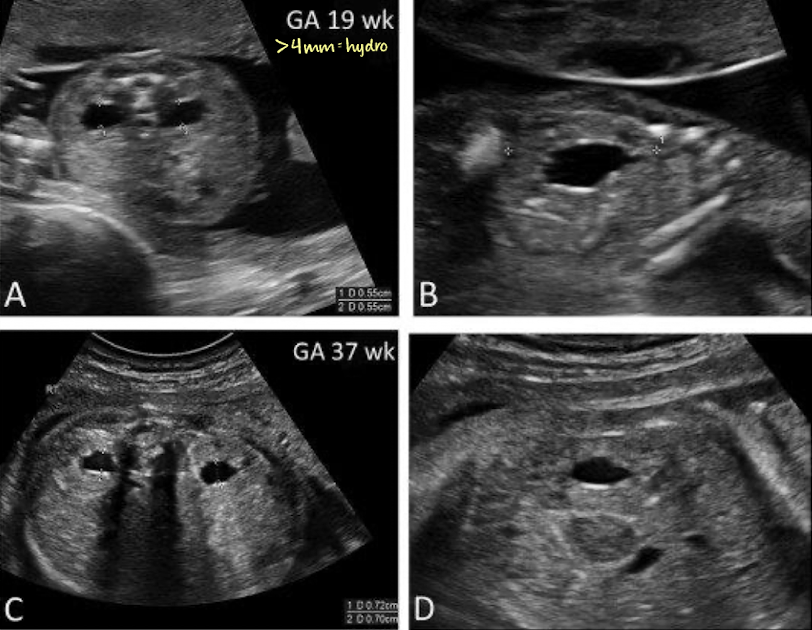
mild pyelectasis (dilation) vs. hydronephrosis in utero
before 27w = >4mm is abnormal
after 27w = >7mm is abnormal
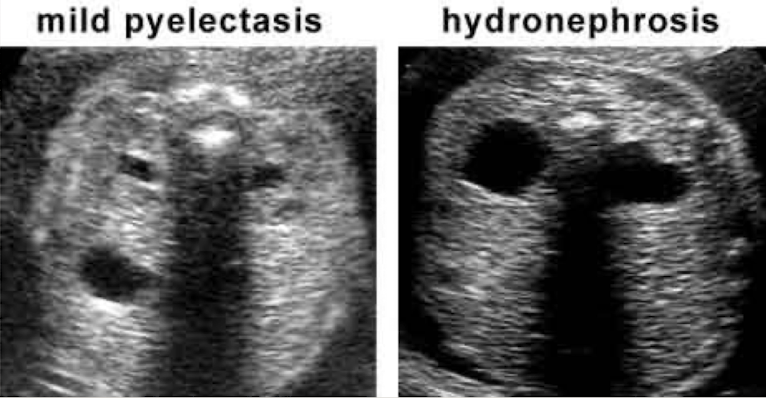
renal pelvis measurement for hydro
>4mm = hydro

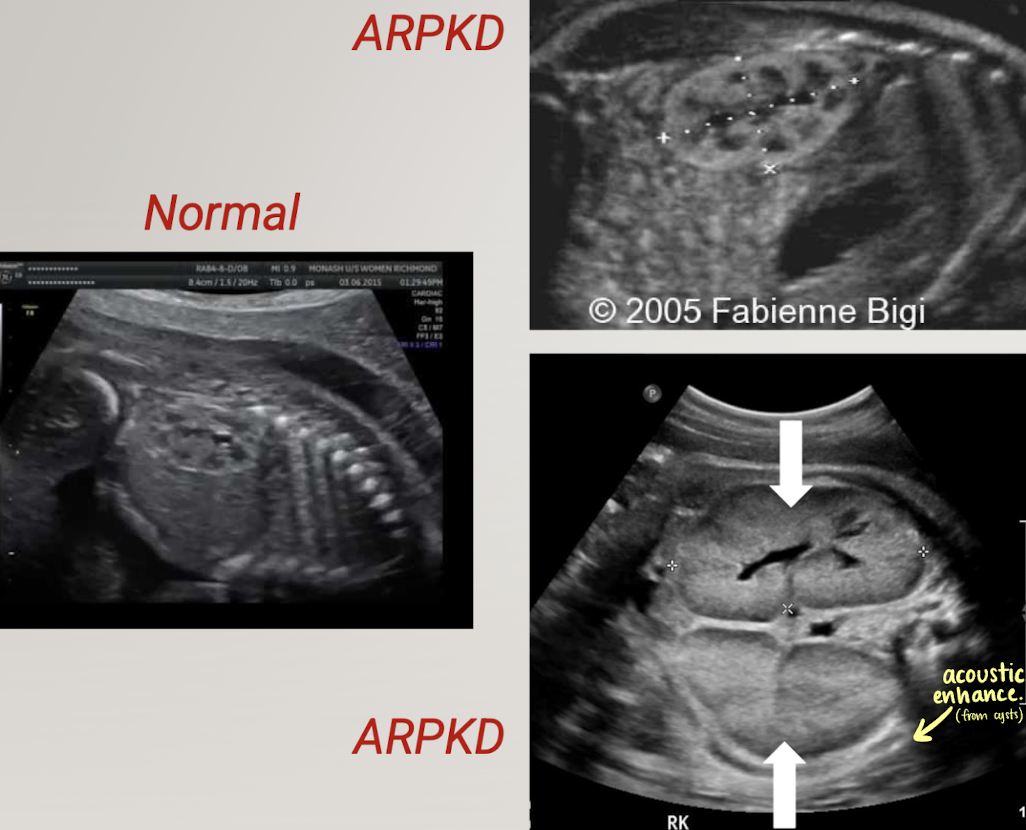
what is the pathology?
ARPKD (autosomal recessive polycystic kidney disease)
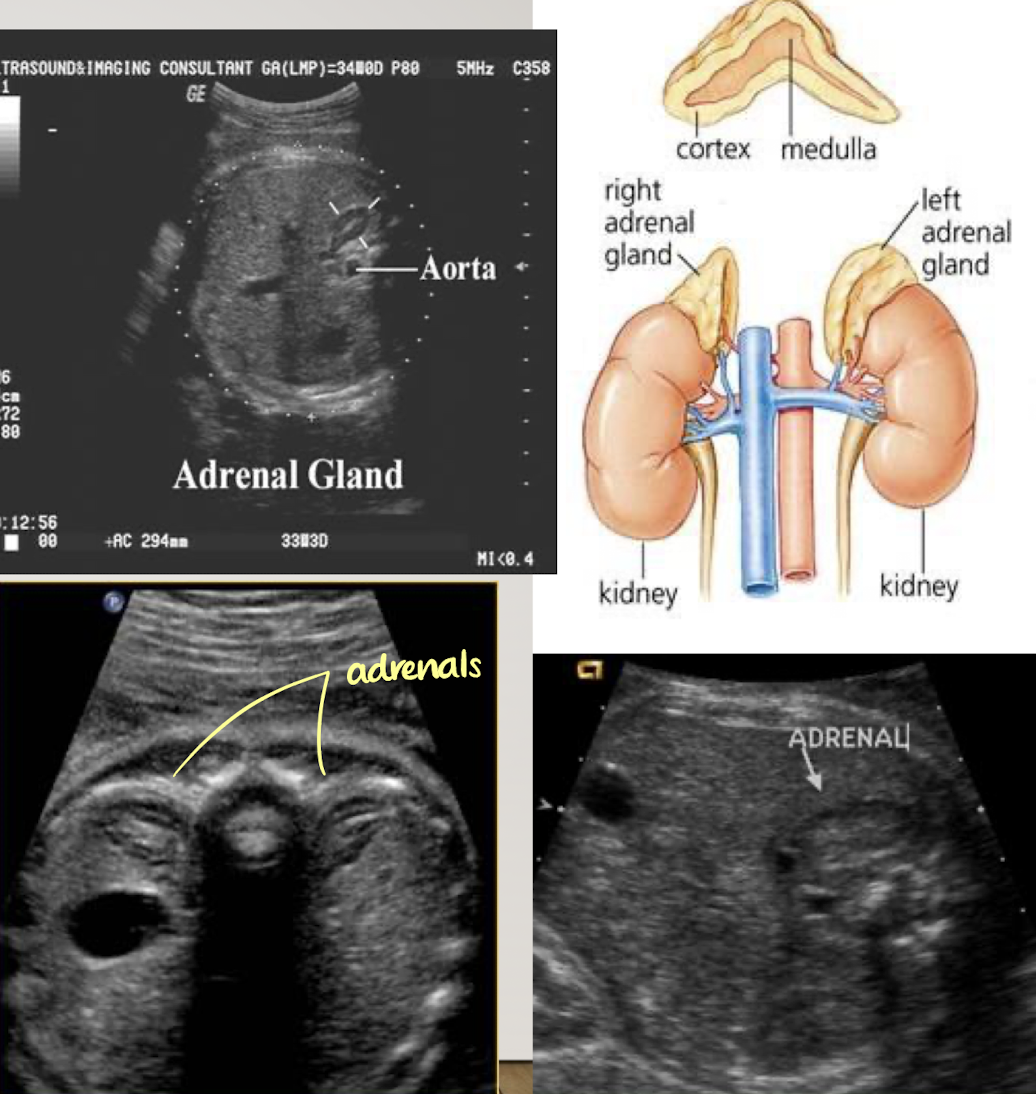
adrenals
adrenal glands can be prominent in fetus and neonate
located medially and superior to fetal kidneys
SONO:
best seen in TRV
superior pole of kidneys
hypoechoic cortex
echogenic medulla
bladder
distended bladder should be seen by 13wks
empties and fills at least once every 30 minutes
if not identified on exam; exam must be repeated within 24 hours
empty bladder is an indication of abnormality
SONO:
anechoic (fluid-filled)
document in LONG and TRV

genitalia
sexual characteristics develop between 9-12 weeks
fetal testes produce androgens that cause masculinization of external genitalia (baby start as a girl)
fetal external genitalia can be definitively identified with US after 18wks
SONO: genitalia (male vs. female)
male
both scrotum and penis identified
“turtle sign”
female
vulva/labia lips identified
“three-line sign”
“hamburger sign”
