Lecture 7 - Bias and Confounding
1/34
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
35 Terms
What is bias?
Systematic error meaning multiple replications of the same study would reach the wrong answer on average
What does bias cause in epidemiological studies?
Lack of internal validity or incorrect assessment of the association between an exposure and the effect in target population
What is internal validity?
Extent to which the findings can be used in the assessment of the association between an exposure and the effect in target population
What is external validity?
Extent to which the findings can be used in generalisation between populations.
What is ‘Positive results’ bias?
Tendency to post or publish positive results rather than negative or inconclusive results.
What is ‘Hot Stuff’ bias?
Tendency to post and give attention to new, trending fields or topics.
What is selection bias?
Arises from procedures used to select study subjects and from factors which affect study participation
Results in relation between exposure and disease being different for those who participate in the study and those eligible for inclusion
Types of selection bias include…
Inappropriate definition of eligible population
Lack of accuracy of sampling frame
E.g. non-random sampling
Uneven diagnoses in target population
Bias during study implementation
E.g. losses to follow-up, non-response
How can selection bias be minimised?
Choose study population with extreme care
Should represent target population
Maximise take-up and follow-up among those invited to participate
If possible, compare characteristics of study population with those of persons who did not respond or withdrew
What is information bias?
Arises during data collection
Variables are inaccurately measured, recorded or classified
Focus on misclassification bias
Bias in classifying exposure or outcome
What is observer bias?
Interviewers' knowledge may influence the structure of questions and the manner of presentation which may influence responses
Researcher’s expectations, opinions and interpretation impact on the results
What is recall bias?
Those with a particular outcome or exposure may remember events more clearly
May also amplify their recollections
What is reporting bias?
Participants might give answers they perceive to be of interest to the investigators
What is Hawthorne effect?
People act differently if they know they are being watched
What is detection bias?
If greater effort is given to diagnosing disease in an exposed group than in an unexposed group
What is Protopathic bias?
Exposure is influenced by early (subclinical) stages of disease
E.g. drug is prescribed for early stage of disease that has not yet been diagnosed
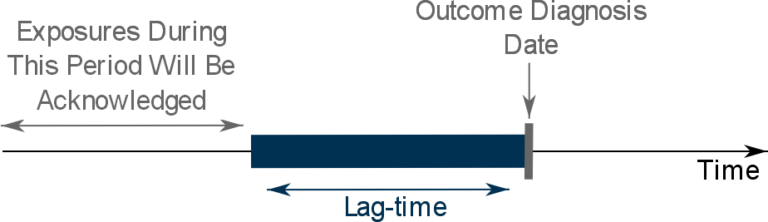
How can protopathic bias be minimised?
Either:
Calculate two odds ratios. One including cases who were prescribed the drug in response to early symptoms AND one excluding this group
Apply a lag-time into the exposure definition. Any exposures which occur during the lag time will be ignored.
What can be done to minimise information bias?
Blinding
Use standardised definitions of disease and exposure
Use standardised data collection instruments and ensure training and quality control
Maximise response to questionnaires
Validate information using independent sources
What is ‘mistaken identity’ bias?
In some trials strategies meant to alter patient behaviour may instead alter clinician behaviour
What is cognitive dissonance bias?
Belief in a given mechanism may increase rather than decrease in face of contradictory evidence
What is significance bias?
Statistical vs clinical significance
How can analysis bias be dealt with?
State hypothesis to be tested in advance
Follow analysis plan
How can interpretation bias be dealt with?
Treat all interpretations with caution
Look for evidence from systematic reviews
What is confounding?
‘A confusion of effects’
The effect of an external factor is mistaken for or mixed with the effect of the exposure under investigation
Such a factor is called a confounding factor
What are examples of confounding factors?
Number of storks nesting and numbers of babies born at around the same time
Seasonality
Low birth weight and father’s smoking
Mother’s smoking
Children sleeping with light on and myopia in later life
Children who read a lot
What is a confounding factor?
A is the exposure of interest and B is the disease or outcome being studied
C is an extraneous factor which confounds the relationship between A and B
C is a confounder which causes A and B
Can create a distorted association between A and B
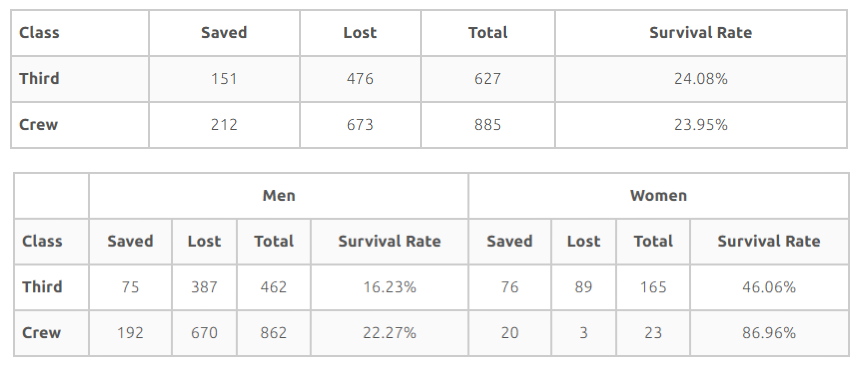
What is Simpson’s paradox?
Correlation present within different groups may disappear or even be reversed when the groups are combined
Titanic survivors
Among males and females, the crew had a higher survival rate than 3rd class passengers
However, because female survival rate was higher than males and because most the crew was male, the differences between crew and 3rd class passengers disappears when male and female data is combined
How can confounding be controlled for in the study design?
Restriction
E.g. exclude smokers
Matching
Select persons to minimise correlations with confounders
Match controls and cases
Randomisation
How can confounding be controlled for in analysis?
Stratification
Make comparisons within specific levels of confounders
E.g. gender, age group
Standardisation
Why can adjusting for confounding when its not present be bad?
Example:
Both risk factor A and disease B are related to C but A and B are NOT related
C is called a collider
E.g. genetic factor (A) and diabetes (B) may be unrelated but both may be related to heart disease (C)
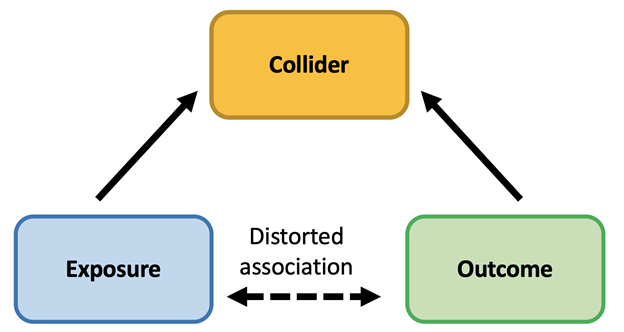
Adjusting for C would induce a spurious correlation between A and B
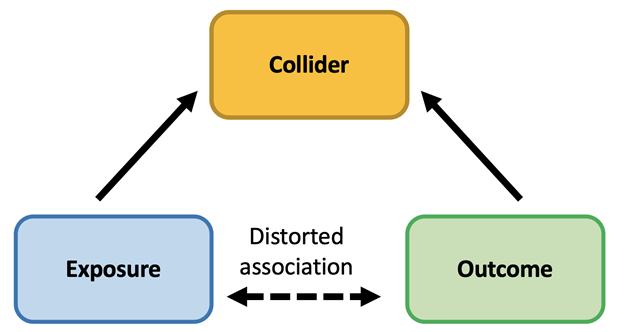
What is a collider when dealing with confounding?
A risk factor (C) which is related to exposure and outcome (A and B) BUT the exposure and outcome (A and B) are not related to one another.
A and B are both associated with C
What are intermediate variables?
If factor A affects the risk of disease C solely by modifying another factor B.
B is the intermediate variable
How can controlling for confounding mask relationships due to intermediate variables?
If factor A affects the risk of disease C solely by modifying another factor B, then adjusting for B would mask the relationship between A and C
E.g. if a factor increases the risk of heart disease by increasing blood pressure, then the impact would be obscured if you adjusted for blood pressure
What is the low birth weight paradox?
Children of smoking mothers are more likely to be of low birth weight
LBW children have higher infant mortality rate than others
BUT
LBW children born to smoking mothers have a lower infant mortality rate than LBW children of non-smoking mothers
What is the explanation of the low birth weight paradox?
Smoking is harmful in that it contributes to low birth weight which results in higher mortality than normal birth weight
HOWEVER
Other causes of low birth weight are generally more harmful than smoking resulting in increased mortality rate